
Abstract
Background:
People with multiple sclerosis (PwMS) frequently experience invisible symptoms, including cognitive impairment, fatigue, depression, anxiety, and psychosocial factors such as stigma, which can substantially affect social role participation (SRP). These factors are often under-recognized in clinical care despite their functional impact.
Objective:
To examine the unique contributions of invisible MS-related symptoms to SRP after accounting for demographic characteristics and objective cognitive performance.
Methods:
A cross-sectional sample of 434 PwMS was recruited from a large outpatient neurology clinic specializing in MS care. The sample was predominantly female (75%), largely white (85%), and middle-aged (M = 51.0, SD = 11.7), with mild-to-moderate disability. Participants completed a computerized cognitive battery and validated patient-reported outcome measures assessing disease impact, mood, fatigue, stigma, and SRP. Hierarchical regression models evaluated the variance explained by demographics, cognitive performance, and patient-reported symptoms.
Results:
Demographic variables were not significant predictors of SRP. Cognitive performance accounted for 13.3% of the variance. Adding patient-reported outcomes increased explained variance to 70.6%. Depression, disease impact, fatigue, and executive functioning remained significant predictors, whereas stigma did not.
Conclusions:
Patient-reported symptom burden showed strong associations with SRP and explained more variance than demographic factors and most cognitive measures, while executive functioning also contributed independently.
Keywords
Introduction
Multiple sclerosis (MS) is a chronic neuroinflammatory and neurodegenerative disease characterized by demyelination, axonal injury, and disruptions in large-scale neural networks that give rise to heterogeneous symptom patterns. 1 Traditional clinical evaluation frameworks, including the widely used Expanded Disability Status Scale, 2 have historically emphasized visible and quantifiable neurological manifestations such as gait impairment, sensory loss, spasticity, and visual disturbances. While invaluable for monitoring disease progression and treatment response, these visible symptoms capture only a segment of the multidimensional burden experienced by people with multiple sclerosis (PwMS). Over the past two decades, empirical studies have increasingly demonstrated that many of the most disabling and personally impactful symptoms of MS are not readily observable to clinicians, family members, or employers. These invisible symptoms (i.e. cognitive impairment (CI), fatigue, depression, anxiety, and stigma) are often episodic, internal, and context-dependent, making them challenging to detect and insufficiently addressed in standard care, which is especially relevant for neurologists, neuropsychologists, MS clinicians, and researchers involved in MS management.3,4
CI in MS, which affects processing speed, executive function, memory, and attention,1,5 can impair the ability to plan, organize, multitask, and sustain complex social interactions. These cognitive skills are foundational for fulfilling everyday interpersonal, occupational, and community roles. Notably, even subtle deficits can interfere with performance in environments that require rapid information processing or divided attention. Fatigue, another hallmark invisible symptom, is consistently rated among the most debilitating features of MS and manifests in physical, cognitive, and psychosocial dimensions.6,7 Many PwMS describe fatigue as unpredictable, overwhelming, and profoundly limiting, leading to constrained participation in employment, recreation, and family responsibilities. Mood disorders, particularly depression and anxiety, occur at higher rates in MS than in the general population and are associated with poorer adjustment, accelerated disability progression, and diminished engagement in meaningful activities.8–10 Stigma, whether enacted by others or internalized, compounds these challenges by influencing identity, self-concept, and social behavior.11–13
Social role participation (SRP) has emerged as a central determinant of health, functioning, and psychological well-being. Rooted in models of disability and social integration, SRP reflects an individual’s perceived ability to engage in valued roles across interpersonal, occupational, familial, and community domains.14,15 These roles contribute to autonomy, purpose, self-efficacy, and relational connectedness, all of which are essential components of quality of life.16,17 In MS, diminished participation is associated with decreased employment, heightened social isolation, reduced emotional well-being, and lower life satisfaction.18–20 However, despite strong conceptual importance, SRP remains understudied relative to physical disability or performance-based outcomes.
Prior research has identified associations between individual invisible symptoms and SRP, but few studies have examined these symptoms simultaneously within a comprehensive, multidimensional analytic framework. Most existing work has focused on singular outcomes (such as work participation, mobility, or daily functioning) or has evaluated symptoms in isolation rather than as interacting components of a symptom cluster. Research on symptom clusters in MS suggests that invisible symptoms frequently co-occur, interact, and produce compounded effects on functioning.21,22 Thus, a multidimensional approach is necessary to understand how these symptoms jointly influence SRP. SRP offers a functional lens for examining the cumulative impact of invisible symptoms on daily life, making it both clinically meaningful and theoretically significant.
The present study aimed to quantify the relative contributions of invisible symptoms (CI, fatigue, depression, anxiety, and stigma) to SRP after controlling for demographic variables and objective cognitive performance. Invisible symptoms were intentionally prioritized due to their high prevalence, substantial functional impact, and frequent under-recognition. Visible disability was intentionally excluded from the regression models to isolate the incremental contribution of invisible symptoms. The Patient Determined Disease Steps (PDDS) was retained for descriptive characterization but was excluded from multivariable analyses due to conceptual overlap with the Multiple Sclerosis Impact Scale (MSIS)-29. Although symptom clusters are conceptually important in MS, the present study focused on estimating the independent contributions of each symptom domain using hierarchical regression. Interaction effects among symptoms were not modeled in the current analysis but represent an important direction for future research. Executive functioning was of particular interest given its central role in planning, organization, social cognition, and goal-directed behavior, all of which are critical for effective participation in social and occupational roles. Consistent with prior literature, we hypothesized that (1) invisible symptoms would strongly correlate with SRP and (2) depression, fatigue, and executive dysfunction would retain independent predictive value in multivariable models.
Methods
Participants and procedures
The study included 434 adults with neurologist-confirmed MS who were consecutively recruited from a large outpatient neurology clinic specializing in the care of individuals with MS. Consecutive recruitment minimized selection bias and permitted inclusion of a broad range of symptom severities and demographic backgrounds. Inclusion criteria were age ⩾18 years, established MS diagnosis, and English proficiency sufficient to complete assessments. Exclusion criteria removed individuals experiencing acute relapse, severe sensory or CI that could compromise data validity, or acute psychiatric or medical instability based on clinician judgment during routine clinical evaluation.
The NYU Langone Institutional Review Board approved the current study. Participants completed cognitive assessments followed by patient-reported outcomes (PROs) during routine clinic visits. Cognitive measures were administered first to minimize potential confounding effects of fatigue or mood on performance. All data were de-identified prior to analysis. This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies.
Measures
Cognitive assessment
Cognitive performance was measured using the NeuroTrax cognitive assessment battery (CAB), a computerized tool that generates standardized indices across multiple domains, including memory, executive functioning, processing speed, visuospatial ability, attention, verbal skills, and motor functioning.23,24 The global cognitive score represents an aggregate measure of overall functioning. The CAB has demonstrated high reliability, strong associations with conventional neuropsychological tests, and sensitivity to MS-related changes in brain structure.25,26
PROs
Disease impact was assessed using the MSIS-29 (range = 0–100, higher scores indicating greater impact). 27 Mood symptoms were measured using the Hospital Anxiety and Depression Scale (HADS), with separate anxiety (HADS-A) and depression (HADS-D) subscales (range = 0–21 each; scores ⩾8 indicating possible clinical symptoms). 28 Fatigue was assessed using the Modified Fatigue Impact Scale (MFIS; range = 0–84), including physical, cognitive, and psychosocial subscales. 6 Stigma was measured using the Stigma Scale for Chronic Illness (SSCI-8; range = 8–40). 12 SRP was assessed using the Patient-Reported Outcomes Measurement Information System (PROMIS) Ability to Participate in Social Roles and Activities short form (T-score metric; mean = 50, SD = 10, higher scores indicating better participation).14,15
Statistical analysis
Descriptive statistics characterized the sample. The Pearson correlations assessed associations among demographics, cognitive indices, PROs, and SRP. Hierarchical regression quantified incremental variance in SRP. Assumptions for linear regression were evaluated prior to analysis, including linearity, normality of residuals, and homoscedasticity. Sample size was adequate based on established recommendations for multivariable regression. Multicollinearity was assessed using variance inflation factors (VIFs), with values <5 indicating acceptable independence among predictors. Block 1 included demographics (age, sex, race, and education). Block 2 added CAB domain scores. Block 3 added PROs (HADS-A, HADS-D, MSIS-29, MFIS subscales, SSCI-8). This structure aligned with theoretical expectations: demographics reflect baseline influences; cognitive performance reflects objective functioning; and PROs reflect invisible symptom burden. Although mediation models may elucidate pathways among variables, hierarchical regression was appropriate for isolating unique contributions given the study’s goals.
Results
Sample characteristics and correlations
The sample (N = 434) was predominantly female (75%), largely white (85%), and middle-aged (M = 51.0, SD = 11.7; range = 20–87). The remaining participants identified as black, Hispanic, Asian, or other racial/ethnic groups (see Table 1). Clinical disability, measured via the PDDS, indicated mostly mild-to-moderate impairment (median = 2). Most participants (84%) were receiving disease-modifying therapies, and approximately half were employed.
Patient demographics.
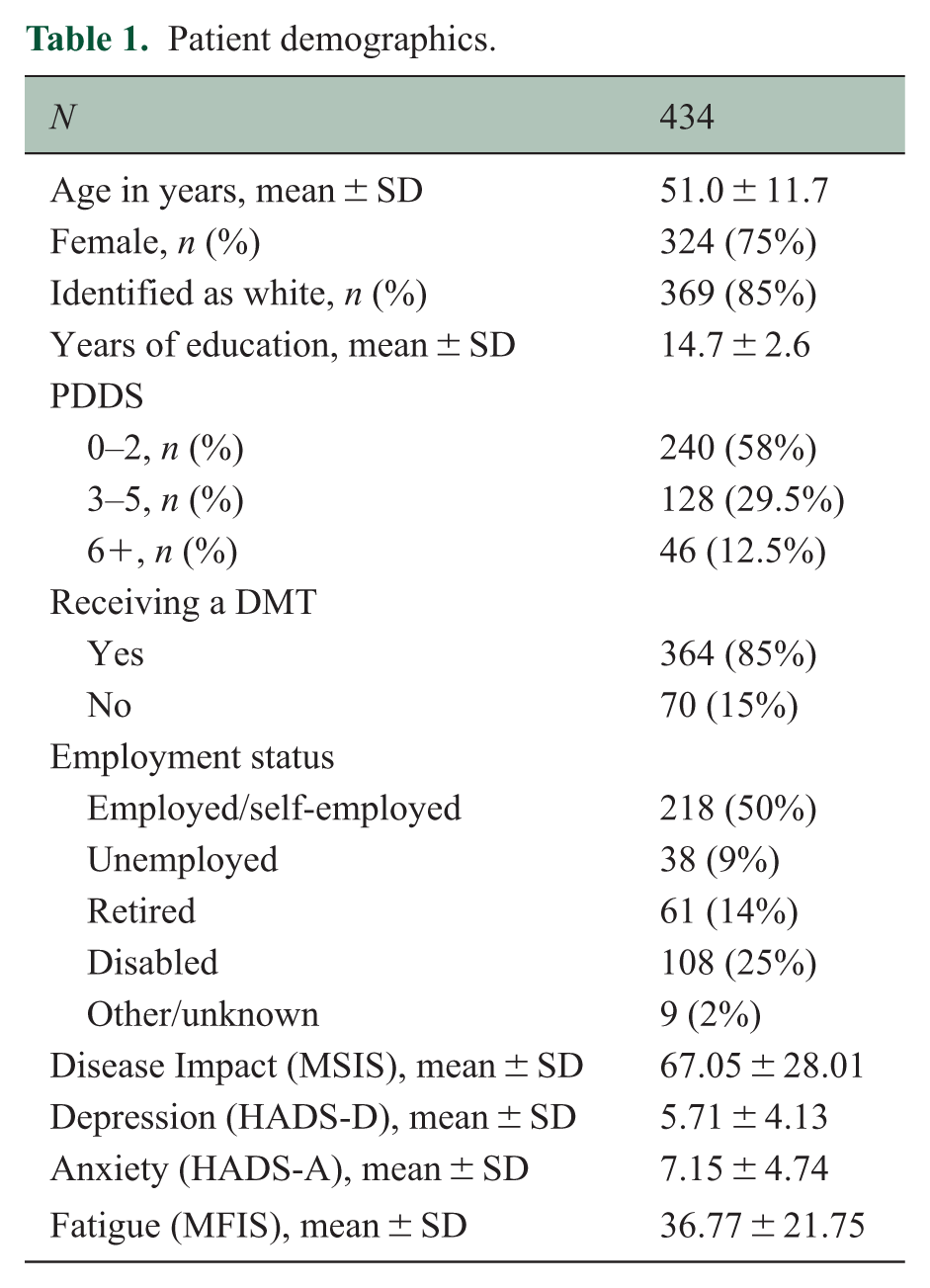
Participants demonstrated cognitive profiles consistent with commonly reported cognitive patterns in MS, with processing speed and executive function showing the greatest variability.29,30 Demographic variables showed minimal association with SRP, although education demonstrated a weak positive correlation (Table 2). Cognitive performance exhibited modest associations with SRP, particularly for executive functioning, processing speed, and motor accuracy (Table 3). In contrast, PROs, including depression, disease impact, physical fatigue, psychosocial fatigue, and stigma, showed strong negative correlations with SRP, indicating a substantial influence of invisible symptom burden on participation (Table 4).
Pearson correlations between demographic variables and SRP.
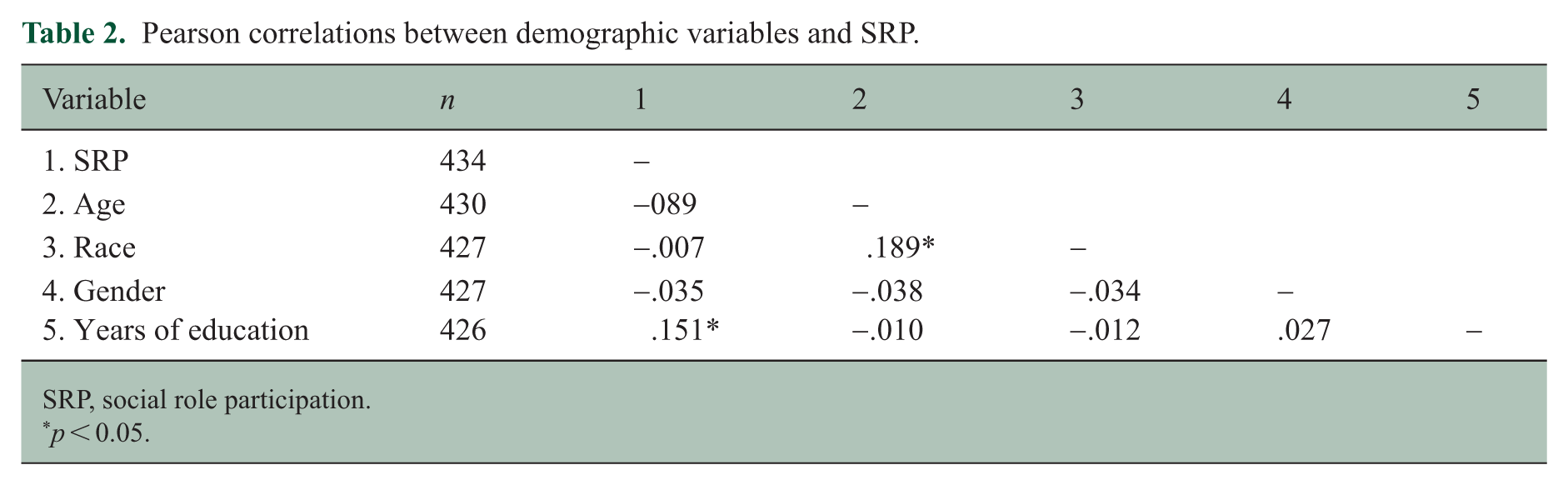
SRP, social role participation.
p < 0.05.
Pearson correlations between CAB scores and SRP.
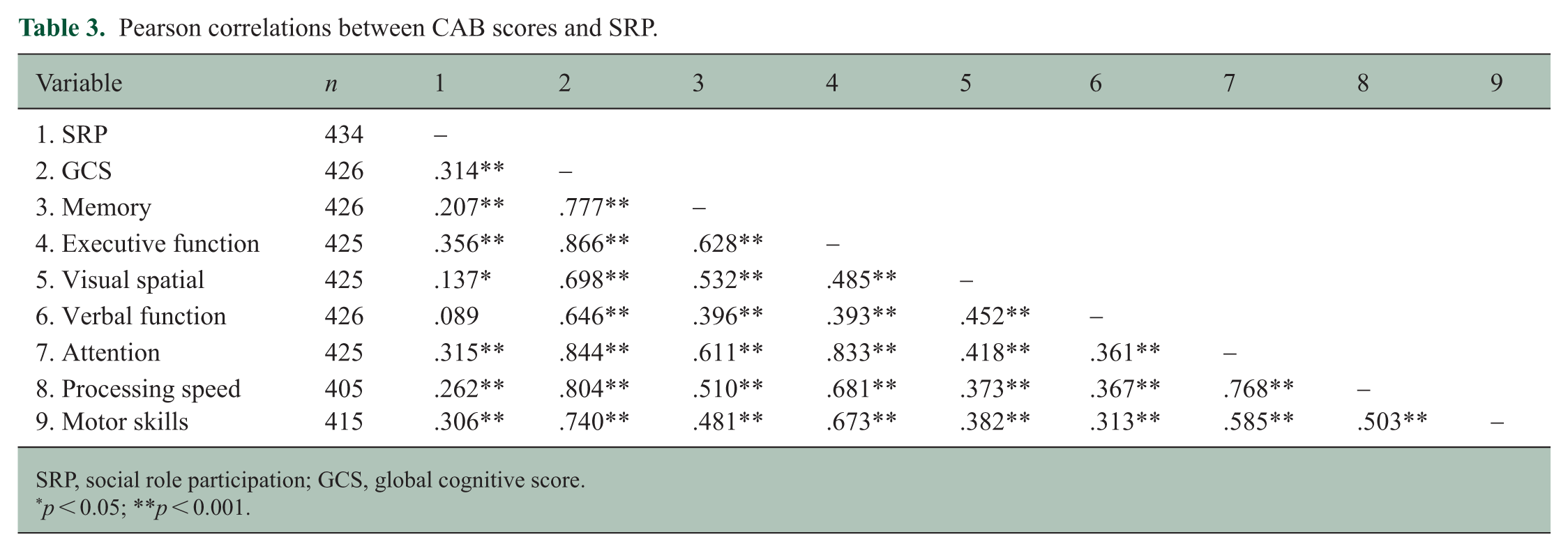
SRP, social role participation; GCS, global cognitive score.
p < 0.05; **p < 0.001.
Pearson correlations between patient-reported outcomes and SRP.
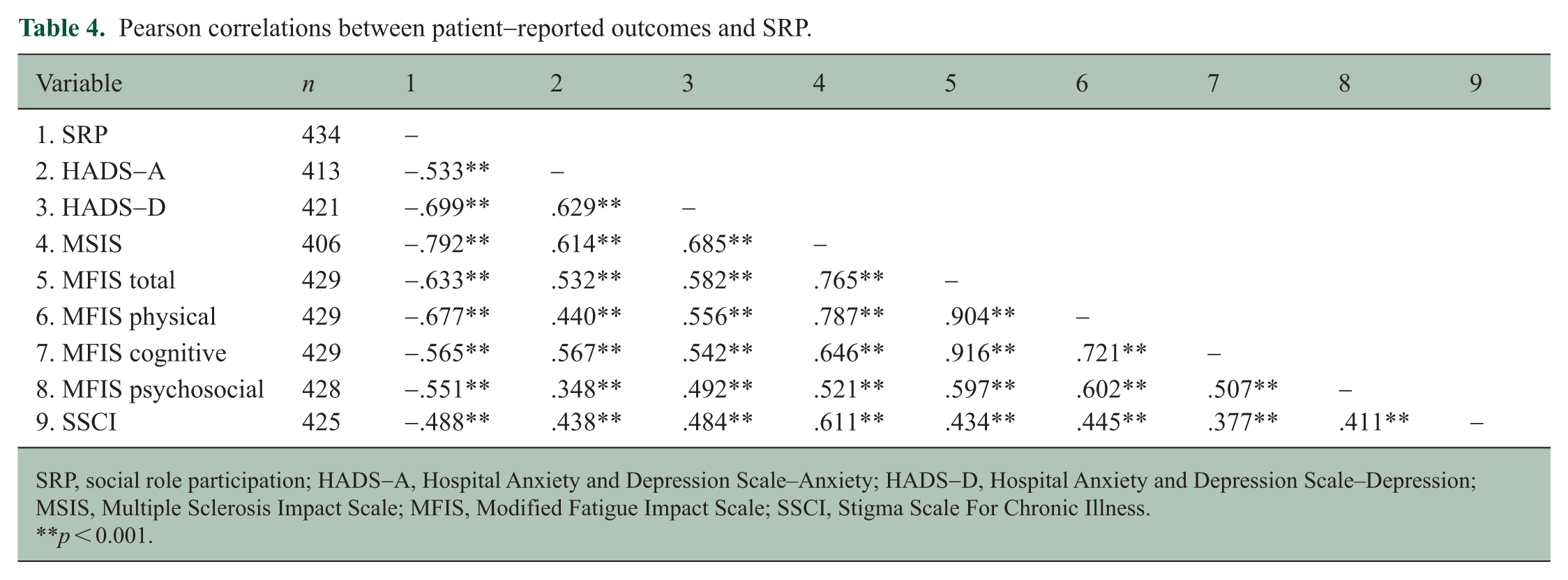
SRP, social role participation; HADS-A, Hospital Anxiety and Depression Scale–Anxiety; HADS-D, Hospital Anxiety and Depression Scale–Depression; MSIS, Multiple Sclerosis Impact Scale; MFIS, Modified Fatigue Impact Scale; SSCI, Stigma Scale For Chronic Illness.
p < 0.001.
Hierarchical regression
Demographic factors explained a slight variance in SRP. Adding cognitive performance increased the explained variance to 13.3%, with executive functioning, processing speed, and motor skills contributing independently. PROs substantially increased explained variance to 70.6%. Depression, disease impact, physical fatigue, psychosocial fatigue, and executive function remained significant predictors (Table 5). Anxiety, cognitive fatigue, and stigma fell out of significance, suggesting overlapping variance with stronger predictors.
Hierarchical regression results examining predictors of SRP.
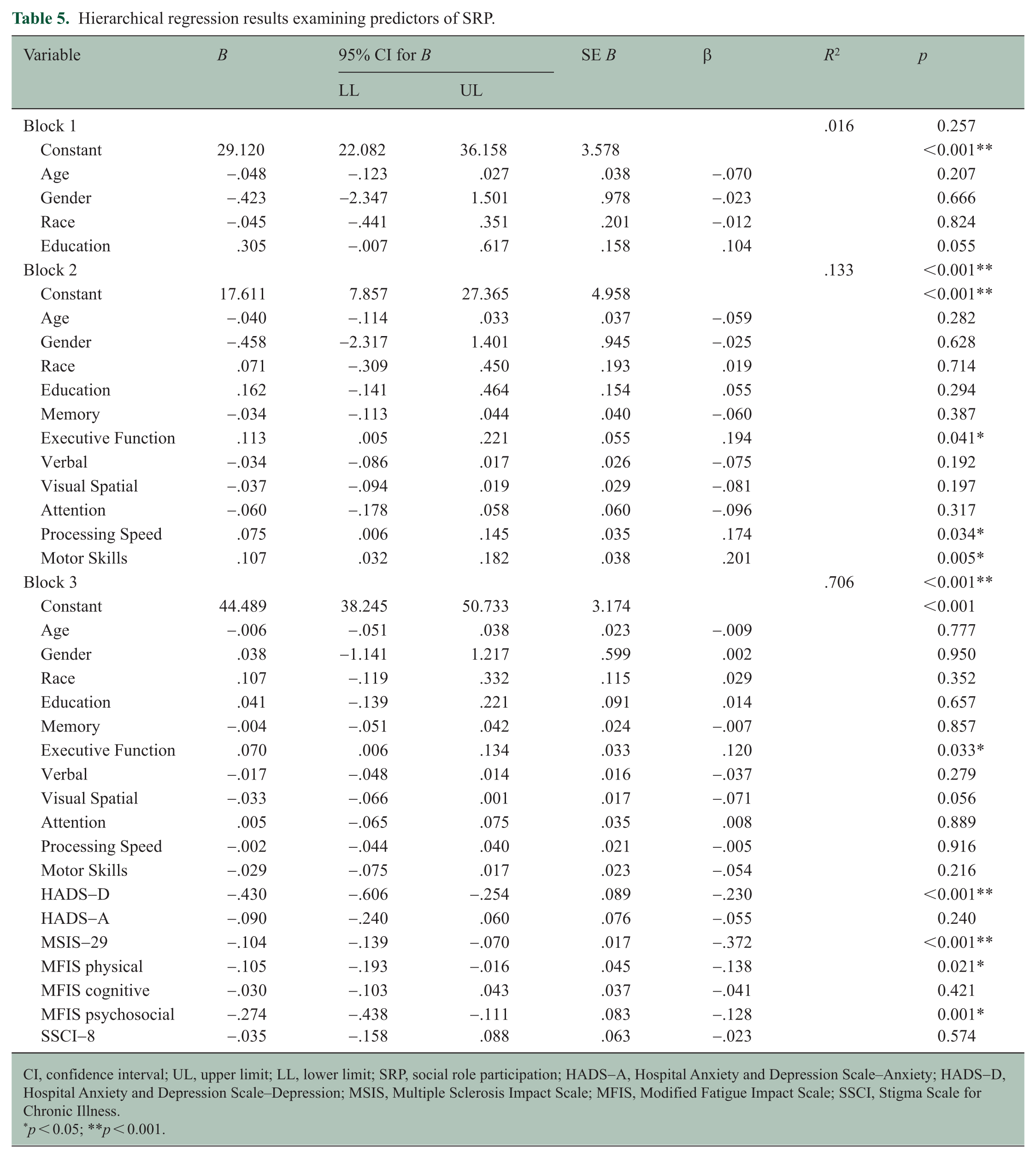
CI, confidence interval; UL, upper limit; LL, lower limit; SRP, social role participation; HADS-A, Hospital Anxiety and Depression Scale–Anxiety; HADS-D, Hospital Anxiety and Depression Scale–Depression; MSIS, Multiple Sclerosis Impact Scale; MFIS, Modified Fatigue Impact Scale; SSCI, Stigma Scale for Chronic Illness.
p < 0.05; **p < 0.001.
Discussion
Patient-reported invisible symptoms showed the strongest associations with SRP in PwMS, far surpassing demographic characteristics and objective cognitive performance. Among the predictors examined, depression showed the strongest unique association with SRP, consistent with literature linking depressive symptoms to reduced activity, interpersonal withdrawal, and diminished psychological resilience.8,10 Fatigue (particularly physical and psychosocial fatigue) played a substantial role, aligning with studies showing that fatigue constrains daily functioning, social fulfillment, and quality of life.7,18 Disease impact also exerted a strong independent influence, suggesting that global illness appraisal shapes perceived capability and engagement.
Executive function retained independent predictive value even after accounting for PROs, underscoring its role in planning, problem-solving, social communication, and role management.29,30 Although stigma correlated with SRP, it did not retain significance in multivariable modeling, suggesting its influence may operate through mood or fatigue pathways, consistent with qualitative findings describing stigma-driven withdrawal and internalized negativity.11,13 Notably, executive functioning remained a significant predictor even when modeled alongside depression, indicating that objective cognitive processes contribute independently to participation outcomes rather than being fully explained by mood-related factors.
Viewed across analytic models, these findings clarify how invisible symptoms collectively shape SRP by demonstrating their substantial explanatory power within a multidimensional model that incorporates both objective cognitive metrics and validated PROs. It is also plausible that depression exerts indirect effects on SRP through its influence on cognitive performance, particularly executive functioning, consistent with longitudinal evidence linking depressive symptoms to cognitive changes in MS. The implications are practical, not theoretical. These findings have direct clinical relevance and underscore the need for systematic screening and treatment of depression and fatigue, as well as targeted cognitive interventions focused on executive functioning, to support daily functioning and participation among PwMS. Routine screening for depression and fatigue using brief validated tools (e.g. HADS, MFIS) should be integrated into standard MS care. In addition, cognitive screening with emphasis on executive functioning may help identify patients at risk for participation restrictions. Interventions may include cognitive rehabilitation targeting executive skills, behavioral activation or psychotherapy for depression, and energy conservation or fatigue management programs. A multidimensional assessment approach may better inform individualized treatment planning aimed at preserving social and occupational engagement.
Limitations and future directions
This single-center design limits generalizability, although standardized assessment enhances internal consistency. Incorporating clinician-rated mobility measures, such as the Expanded Disability Status Scale (EDSS), in future work would enable direct comparison of the contributions of visible and invisible symptoms to SRP, complementing the current study’s intentional focus on invisible symptom burden. Although several PROs may exhibit conceptual overlap, each instrument is independently validated and captures essential components of MS symptomatology. The cross-sectional design precludes causal inference. Future research should incorporate longitudinal, mediation, and moderation models to highlight pathways through which invisible symptoms influence SRP and to integrate broader quality-of-life measures for contextualization.
Conclusion
Patient-reported invisible symptoms (particularly depression and fatigue) were strongly associated with SRP and accounted for substantial variance beyond demographic factors and most objective cognitive measures. This distinction is clinically relevant. The findings underscore the importance of comprehensive assessment strategies that extend beyond visible disability. Routine use of validated PROs, combined with targeted psychological, fatigue, and cognitive interventions, may meaningfully enhance everyday participation and overall quality of life for individuals living with MS.
Footnotes
Acknowledgements
The authors would like to thank the individuals with multiple sclerosis who participated in this study and the clinical staff who supported data collection. The authors also acknowledge the contributions of research and clinical personnel involved in assessment administration and data management.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: G.M.D. is an employee of NeuroTrax Corporation. The authors declared no other potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
This study was approved by the NYU Langone Institutional Review Board. All procedures involving human participants were conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments.
Consent to participate
Written informed consent to participate in the study was obtained from all participants prior to enrollment.
Consent for publication
Not applicable. This manuscript does not contain individual-level identifiable data, images, or videos requiring consent for publication.
Data availability
The data that support the findings of this study are not publicly available due to ethical and privacy considerations but are available from the corresponding author upon reasonable request and with appropriate institutional approvals.