
Abstract
Background:
To date, real-world applications of the 2024 McDonald criteria have been limited to non-Asian cohorts, with a lack of data from Asian populations.
Objectives and Methods:
We evaluate the 2024 and 2017 McDonald criteria at disease onset in a large multicenter Korean multiple sclerosis (MS) cohort to assess differences in criteria fulfillment and time to diagnosis.
Results:
In 306 individuals with MS, we compared the 2024 and 2017 McDonald criteria at disease onset. Under the 2024 criteria, all participants fulfilled diagnostic criteria at initial evaluation, whereas 90.5% (277/306) met the 2017 criteria. Among 22 participants with clinically isolated syndrome who fulfilled the 2024 criteria earlier than the 2017 criteria, the median time to diagnosis was reduced by 5 months. This difference was primarily attributable to the inclusion of optic nerve involvement as an additional dissemination in space site.
Conclusion:
These findings suggest that the 2024 McDonald criteria facilitate earlier MS diagnosis in real-world practice.
Keywords
Introduction
The 2024 McDonald criteria aim to enable earlier and more accurate diagnosis of multiple sclerosis (MS), thereby supporting timely clinical management. 1 Major revisions include recognition of the optic nerve (ON) as a fifth dissemination in space (DIS) location, with dissemination in time (DIT) no longer required in selected circumstances. The criteria also incorporate para-clinical markers including MRI-based central vein sign (CVS), paramagnetic rim lesions (PRLs), and cerebrospinal fluid kappa-free light chain index (CSF-KFLCi) as an alternative to CSF-specific oligoclonal bands (CSF-OCB) to enhance diagnostic confidence. Radiologically isolated syndrome (RIS) can also fulfill diagnostic criteria.
To date, real-world applications of the 2024 McDonald criteria have been limited to non-Asian cohorts,2–5 and data from Asian populations remain absent. Accordingly, we applied the 2024 and 2017 criteria at disease onset in a large multicenter Korean MS cohort to assess differences in criteria fulfillment and time to diagnosis.1,6
Methods
From 2006 to 2025, we retrospectively identified Korean participants with MS with disease onset between 15 and 60 years of age at four referral hospitals. The analysis included those whose diagnosis was confirmed by experienced neurologists during a median 7-year follow-up. 6 Eligible individuals had an initial brain MRI performed within 3 months of symptom onset at their first-ever clinical event (for clinically isolated syndrome (CIS)) or an index MRI (for RIS), a disease duration of at least 2 years, and sufficient clinical and para-clinical data to allow application of both the 2017 and 2024 McDonald criteria.1,6 Individuals with insufficient data or alternative diagnoses were excluded (Supplementary-Figure-1).
MRI was performed on 1.5- or 3.0-T scanners and included brain fluid-attenuated inversion recovery and/or T2-weighted sequences, with post-gadolinium T1-weighted imaging. Gadolinium-enhanced brain MRI was available in 96% of participants. CSF-OCB using isoelectric focusing and CSF-KFLCi measured by nephelometry were available in 80% and 28%, respectively. 7 Spinal MRI was available in 80%, and ON assessment using visual evoked potentials and/or orbit MRI was available in 56%. Advanced MRI markers, CVS and PRLs, could not be evaluated because they were not collected at disease onset in this retrospective cohort. 1
We compared the 2024 and 2017 criteria at disease onset to quantify differences in criteria fulfillment and time from onset to diagnosis.1,6 In addition, among individuals diagnosed earlier using 2024 criteria, we analyzed which aspects of the revised diagnostic criteria contributed to these differences.
The dataset was anonymized, approved by the IRBs at each participating center, and informed consent was waived.
Results
In total, 306 eligible individuals with MS were analyzed. The median age at onset was 29 years, and 70% (213/306) of the cohort were female.
When the 2024 criteria were applied at disease onset, all 306 participants (100%) fulfilled the diagnostic criteria, of whom 277 (90.5%) also met 2017 criteria (Figure 1). Under 2024 criteria, 294 had relapsing MS, 5 had progressive MS, and 7 were classified as RIS. Of these, 272/294 with relapsing MS and all 5 with progressive MS met 2017 criteria, whereas none of the 7 with RIS did. Overall, 29 additional participants (9.5%) met 2024 criteria compared with 2017 criteria. These differences were attributable to ON involvement newly recognized as a DIS location (n = 20), RIS (n = 7), fulfillment of DIS ⩾ 4 anatomical locations (n = 1), and combined ON involvement with DIS ⩾ 4 anatomical locations (n = 1). Under the 2024 criteria, 118 of 306 participants (38.6%) fulfilled DIS solely by involvement of ⩾4 anatomical locations, without additional diagnostic requirements.
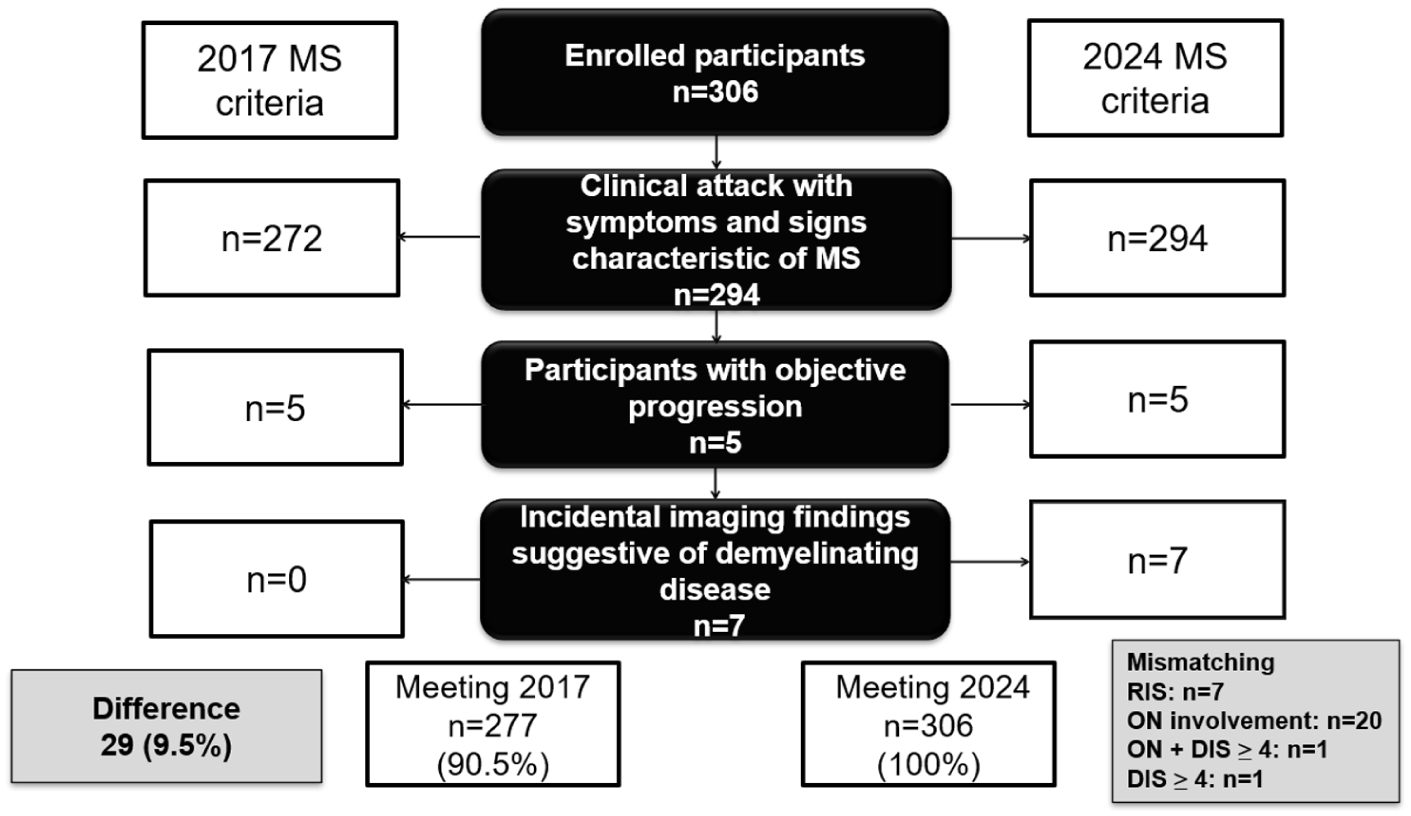
Application of the 2024 and 2017 McDonald criteria.
Among the 29 participants who fulfilled the 2024 criteria but not 2017 criteria, 7 individuals classified as RIS were excluded, as a comparable diagnostic time-point could not be defined. In the remaining 22 CIS participants, application of 2024 criteria led to earlier diagnosis at the initial clinical event compared with 2017 criteria, with a median reduction of 5 months. In the seven individuals with RIS, the median time to development of typical MS symptoms was 18 months.
Discussions
In a large multicenter Asian MS cohort, a higher proportion of individuals met MS diagnostic criteria at baseline using the 2024 criteria than 2017 criteria (100% vs 90.5%). Among 22 CIS participants diagnosed earlier under 2024 than 2017 criteria, the median time-to-diagnosis was reduced by 5 months, supporting earlier identification of MS in routine clinical practice.
The higher proportion diagnosed under the 2024 criteria in the current cohort is comparable to prior evaluations in different populations. In the Australian (n = 163), Croatian (n = 118), Egyptian (n = 197), and UK (n = 274) cohorts, the 2024 criteria identified an additional 6.7%, 8.5%, 13.7%, and 17.5% of participants, respectively, compared with 2017 criteria.2–5 The diagnostic gain in our cohort (29/306, 9.5%) falls within this reported range. The 5-month reduction in time to diagnosis was confined to CIS participants diagnosed earlier under 2024 criteria in this study; although recent studies reported a 44-day or 0.1-month reduction in the overall cohort, comparison is limited because all individuals in our cohort fulfilled 2024 criteria at baseline.4,5
Pivotal change contributing to 20 additional diagnoses (6.5%) in our cohort compared with 2017 criteria is the inclusion of ON as a fifth DIS topography, with comparable gains reported in the non-Asian (1%–7.2%) cohorts.3–5 Reclassification of RIS also contributed to additional diagnoses; all seven RIS individuals in our cohort developed typical MS symptoms within a median of 1.5 years, supporting the potential clinical relevance of earlier identification under 2024 criteria, although confirmation in larger RIS cohorts is warranted. Another modification allows diagnosis based on involvement of ⩾4 anatomical locations without requiring DIT; in current cohort, this criterion contributed to only two additional cases. When applied to the entire cohort rather than only newly diagnosed individuals, 38.6% (118/306) met DIS in ⩾4 anatomical locations, comparable to the proportions reported in non-Asian cohorts (38%–44%),2–4 indicating a consistent mechanism that may facilitate earlier diagnosis.
This study has several limitations. As this analysis was conducted in an MS-confirmed cohort and did not include the full spectrum of individuals undergoing evaluation for suspected MS or alternative diagnoses, evaluation of diagnostic specificity or misclassification risk under the revised criteria was not possible. Para-clinical data, such as optical coherence tomography, CVS and PRL, and CSF markers, could not be fully investigated. The retrospective design, including heterogeneity and variable availability of diagnostic assessments, may have introduced unintentional selection bias and influenced estimation of the impact of the 2024 criteria. Future prospective studies including broader clinical spectra and advanced para-clinical marker assessment are needed to further clarify the clinical implications of applying the 2024 criteria.
Supplemental Material
sj-tif-1-msj-10.1177_13524585261462503 – Supplemental material for Application of the 2024 and 2017 McDonald criteria at disease onset in a multicenter Korean MS cohort
Supplemental material, sj-tif-1-msj-10.1177_13524585261462503 for Application of the 2024 and 2017 McDonald criteria at disease onset in a multicenter Korean MS cohort by Jae-Won Hyun, Ki Hoon Kim, Seung Woo Kim, Ha Young Shin, You-Ri Kang, Tai-Seung Nam, Woojun Kim, Su-Hyun Kim and Ho Jin Kim in Multiple Sclerosis Journal
Footnotes
Author contributions
J-W.H. and H.J.K. had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. All the authors contributed to the acquisition, analysis, interpretation of the data. All the authors drafting of the manuscript and critically revised it for important intellectual content.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: H.J.W. has received a grant from the National Cancer Center and consultancy fee from Merck. K.S.W., K.Y.R., N.T.S., K.W. report no financial disclosure. K.K.H. received consultancy or speaker fee from Merck, GPH Korea, Neurophet, and Tanabe Pharma Korea. S.H.Y. has received a grant from the National Research Foundation of Korea and research support from Hanmi, Myung In Pharm, and Yuhan; honoraria/consulting fees from Alexion, Astellas, AstraZeneca, Biogen, Daewoong Pharmaceutical, Eisai, Euroimmun, GC Pharma, Genuv, Genzyme, Handok Pharmaceutical, Janssen, Johnson & Johnson, Merck Serono, Mitsubishi Tanabe Pharma, Roche, Samsung Bioepis, Sanofi, and UCB. K.S.H. has lectured, consulted, and received honoraria from AstraZeneca, Merck Serono, Sanofi, Mitsubishi Tanabe Pharma, and Roche and received a grant from the National Cancer Center. K.H.J. received a grant from the Korea-US Collaborative Research Project and the National Research Foundation of Korea; received research support from AprilBio, Eisai, Good T cells and UCB; received consultancy/speaker fees from Alexion, Altos Biologics, AstraZeneca, Biogen, Daewoong Pharmaceutical, Eisai, GC Pharma, Kaigene, MDimune, Merck, Mitsubishi Tanabe Pharma, Roche, Samsung Bioepis, and Sanofi; is a co-editor for the Multiple Sclerosis Journal and an associated editor for the Journal of Clinical Neurology.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Anonymized data not described within this article can be made available on the appropriate request from any qualified researcher.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.