
Abstract
This study is concerned with the negotiation of tall women's body height and perceived normativity in our Western society. The introduction aims to describe the role of the body in a cultural context and questions socially embedded norms regarding deviations. Medical procedures and possibilities are presented how body height can be determined already in childhood and how it can be influenced in case of deviations from the norm. Central to this is the procedure of prospective final height determination. Methodically, the Trajectory Equifinality Model (TEM) was used. A total of two persons were interviewed in a semi-structured interview. The participants consisted of a mother and her daughter, who is considered tall. Individual negotiation was found to be related to maternal body height. Counter narratives play a key role in the negotiation of this by attempting to compensate for a deficient characteristic with another idealized construct. The work showed that medical procedures create norms, while at the same time can support affected individuals in their self-negotiation.
Beauty ideals that have prevailed since time immemorial are often linked to genetic aspects and dispositions that are judged to be beautiful in the respective cultural circle or are considered a beauty norm for individuals. These ideals vary between cultures but normativity itself seems to be a universal phenomenon. But when do social norms begin to take effect in relation to physical ideals? And what happens when a genetically determined characteristic like body height can lead to exclusion within an entire system? Medical examinations in Western society serve to verify and ensure healthy child development and occupy a relevant position in the early detection of growth disorders. Nevertheless, a non-developmental pathological tall stature is often addressed and medical procedures to determine the final body height are proposed or further indications to inhibit growth by means of the orthopedic procedure of epiphysiodesis. Those ideals of beauty as well as its deviations, which become social representations have an immense influence on human well-being. The Trajectory Equifinality Model (TEM) as theoretical frame allows to assess these social representations and how they affect the individual. The influencing factors Societal Dominance and Societal Guidance reveal how the person concerned deals with this experienced normativity over the course of life and how this may have influenced the way that person develops.
In terms of the question of beauty, body and normativity, this study addresses norms of physical appearance and the associated perception of “tall” women. Disadvantages due to divergent societal concepts about body shapes and a non-normative appearance are still a reality today. Based on that, this paper will address the normativity of body height. How do women in the Western society experience “being tall”? To appeal to prevailing norms, the focus is on tall women’s personal negotiation with their body height. For this purpose, an interview was conducted with a mother and her daughter who speak about these societal influences of past and present life situations and offer a comprehensive perspective on life. The data was analyzed through the lens of the TEM to describe the life paths they took and to make visible the other, unchosen options. From the research, it emerged that Societal Dominance (e.g., gender stereotypes the woman should be smaller than the man) is a key societal that affects the female body perception. Similarly, it became clear that Societal Guidance is often based on a counter narrative. Say, you are a tall woman, then you can be a model (while catering to a different underlying beauty standard). As possible negotiation attempts and short-term acceptance counter narratives are used which are based on tolerated and supposedly advantageous social constructs which mostly aim at an improved functionality (you are tall, you can play basketball) or an ideal of beauty (you can become a model) in order to camouflage culturally deficient deviations without a sincere confrontation and a breaking of stigmas having to happen.
This paper aims to find out how “being tall” is being perceived by an intergenerational pair mother (Linda) and daughter (Marie) in our contemporary German society. Since the interviewees are mother and daughter, this provides the opportunity to examine their life courses from the prenatal stage to the present. Along with this, a developmental focus is necessary to grasp the tall picture, which is why her daughter is also interviewed and her BFPs of negotiating her self-perception are illustrated. The article focuses both on the individual experiences and challenges faced by a tall woman and mother herself and the impact on her daughter. The main point is to show that there is no right way in life, but options that sometimes seem invisible and first have to be brought out of hiding to the surface.
Prenatal normativity
As soon as a new life is born and grows in the womb, it is usually a very special experience for the expectant parents. In the process, a unique little human being is created in just 40 weeks of pregnancy, with each of these weeks of pregnancy representing a milestone. In our western society, we usually have the privilege of being accompanied by physicians and having examinations performed during this time. One of these examinations is the measurement of the body height of the fetus. This is supposed to provide information on whether a “normal” development of the unborn child is taking place (Gehl & Lechthaler, 2021). However, these examinations seem to be strongly tied to social normativities, which already take impact before birth, in that body height is linked to divisions into percentiles. In addition to being medically necessary, it is questionable whether this visual representation of “normal” and “deviant” also fuels the normative thinking of the expectant mother.
After birth and in the course of childhood, the measurement of body height continues to play a central role and is included in almost every standard examination. The bone age (also called skeletal maturity) is a measure for the development of the growing child. Again, the word “normal” is in focus here, because typically the bone age coincides with the chronological age. If it differs, it is possible to assess the child’s biological maturity using an objective procedure called prospective final sizing (Faust, 2011). Knowledge of bone age can be used to evaluate questions about developmental status and possible interference with growth, and to make predictions about expected body height (Faust, 2011). But why - apart from possible hereditary growth disorders - is it at all relevant for medical examinations to predict future body height? While such a procedure can provide information about whether a growing person is developing healthily, it also seems to be aimed at detecting deviations from the norm. It is particularly important to indicate the intrapersonal dialogues that are stirred up in the parent by these procedures. Suddenly, from a medical point of view, my child does not conform to the norm, which can lead to other life paths being taken and decisions being made or not. To address that in more detail, the methodology of the TEM is presented below.
TEM – a tree of real and imagined options in life
The TEM is a pre-factum focused method, that proves to be a suitable tool for this study due to its representation of possible and chosen life choices as well as their societal influences over the life span of an individual (Valsiner et al., 2009). Herein, the focus is on the search for the pre-factum and the real as well as possible trajectories. The event is thereby considered as human development united in irreversible time. Accordingly, the TEM aims at revealing processes of constructions in a trajectory of a system as they proceed. It is an essential principle that the method considers what has already happened, taking into account what could happen at the future step and what should happen. Underlying this process are both the individual and the social demands on the person itself. The aforementioned development has multiple paths, that is, trajectories, that lead to goal-like equivalent results, and can therefore be considered as multi-linear (Valsiner et al., 2009). Elementary to this is that the fundamental structure of TEM seeks and considers relevant the differentiation of past and future considering actual and potential trajectories (Valsiner, 2017). Concomitantly, this raises the question of why people do or do not choose one option or another in certain situations in their lives. The issue of “what if” and the potentially associated consequences on a personal and social level are crucial here.
To generate a deeper understanding of the TEM, it is necessary to understand the various steps and processes. For this purpose, the individual terms of the model will be explained in their fundamentals in order to apply them to this research and the life of the interviewee in the next step. It is noteworthy that TEM in its methodology helps to see not only the paths and options of the actor, but it also takes into account the continuity and agility of life, which would be invisible under the application of other methods. The focus is not only on the choices actually made, but also around those that were considered but not taken. This allows a deeper insight into the actor’s real and potential choices, with imagination being a key element, which is also influenced in its ideals by societal norms and values (Valsiner et al., 2009). Thereby key factors are Societal Dominance and Societal Guidance. These affect how tall women perceive and negotiate their own body height with themselves. Societal Dominance, for example, would be the norm set by our society, such as determining whether an unborn child’s body height complies with the norm. In this research, Societal Dominance is expressed through the examining physician, to name a few. Societal Guidance, on the other hand, could represent personal characteristics, such as contesting perceived normativity with humor and consciously lived individuality.
Bifurcation point
The Bifurcation point (BFP) represents a stylistic break in whose procedure the actor decides for one trajectory and against the other. In doing so, it offers the option to read between the lines and consider possible tensions between the individual’s potential options. Bifurcation point is a point for which there are alternative options (Figure 1). The Bifurcation - BFP.
Obligatory passage point
The concept of Obligatory passage point (OPP) was developed within the sociology of science by Latour in 1988 (Valsiner & Sato, 2015). Whereby, this describes an event that inevitably occurs considering exogenous and autochthonous influences. In the former, the OPP is determined by the external impacts, such as the environment. Thereby, the monthly period would represent the opposite for women, whereby this is biologically determined. Menstruation is an inevitable, biologically timed event that occurs during puberty for not all, but most women. In the course of life, the monthly period can change, such as when the female cycle finally fades after menopause. But it can also change due to external transitions, such as immense stress or during times of war.
At the same time, the seclusion of menstruation reflects another social normativity. Above all, the monthly period experienced by women represents fertility, life, and youth. Not least because of the biologically limited period, which temporally determines exactly that fertility and the passing on of new life. Being a woman is femininity, which also includes such described processes. It also seems to be constricting and also to create space for exclusivity and normativity. This is also pointed out by the so-called menstruation hut, which is still present today in countries such as India, despite being illegal.
At the same time, socially determined exogenous OPP’s should also be mentioned, such as the compulsory enrollment of children in school, with the process extending over several years (Valsiner & Sato, 2015).
Societal dominance
Societal Dominance (SD) represents both the social influences and the social power that affect a person’s decision-making. In addition, societal dominance inhibits personal choice in the direction of EFP. Here, “being tall” could represent exclusion. Social demands at certain stages of life include seemingly banal aspects, such as clothing, in order to feel like one belongs. “Being tall” in itself brings social dominance to the fore in that the person concerned deviates from the average in his or her visual appearance. And this not only from the size, but also by the fact that possibly not the same clothes can be worn due to the body height. In this case, the clothing and the external appearance in itself would clarify the social dominance and makes it more difficult, for example, to feel self-confident and to perceive one’s own body positively.
Societal guidance
Societal Guidance (SG) is to be understood as the antagonistic counterpart of Societal Dominance, working against its inhibition. This represents the support and encouragement, such as from close friends and family, to achieve EFP (Valsiner et al., 2009). Societal guidance, in the concept of Counter narratives, can additionally appear as a positively reinforcing lever, which can include people but also inherent traits, such as resilience, bravery, and humor.
Equifinality point
The equifinality point (EFP) is an intermediate point, as it is a place of temporary similarity and also a node for further development (Valsiner & Sato, 2015). Equifinality point is a goal-like end to which a person aspires (unconsciously or not) and which can be achieved through a variety of pathways.
Polarized EFP
The EFP is key to answering the research question and is determined based on it. In order to balance the implicit value system of the researcher, a complementary aspect is selected and set up as Polarized EFP (P-EFP). This is an imaginary point that is in contrast to the EFP. A girl may be immediately concerned as she grows. Her mother may also be concerned, such as Linda: “I always hoped for her that she would not grow above 1.85 m” (l. 167). Where the EFP outlines the approximately average range where growth stops.
Second EFP
Second-Equifinality point (S-EFP) is the next EFP that an actor perceives and pursues after the previous EFP. This can be illustrated by the fact that a girl, for example, reaches the first EFP with a height of 1.65 m and then starts doing everything in her power to look taller (which she cannot do), for example, by wearing high heels.
Irreversible time
Irreversible time flows like a river from an infinite past to an infinite future and never against its natural flow, i.e., backwards. It is based on a person’s experience and is therefore subjective (Valsiner et al., 2009). Even though this is the actual meaning for irreversible time, it must be said that in this particular case it is about a growth process. Growth takes time, is irreversible, and comes in time intervals, spurts or plateaus. An example of this would be a parent asking why their own child did not grow as much this year as they did last year.
In the cockpit of her own plane - Linda as the pilot
An overview regarding Linda’s life path using the TEM will be illustrated with the guidance of Figure 2. The focus of this research is primarily on women’s perceptions of body height. Linda takes an exciting position in this regard. Since she herself is considered a taller woman, it is conceivable that her experiences are also shaped by this. Nevertheless, she herself has already managed to fit into our society. As she enters motherhood, Linda also has to make decisions for her daughter and once again sees the societal hurdles regarding norms and body height for girls and women through a different lens. Based on this, the EFP can be determined as follows: being a loving mother who leads by example with her above average body height (especially for her daughter). The resulting S-EFP is to give her daughter self-confidence and to accept her as she is. The P-EFP was determined to be Linda’s daughter positively embracing her body and accepting herself as she is. Considering and incorporating the Societal Dominance and Societal Guidance, the following will assess whether certain trajectories and social influences, have steered or directed Linda away from the metaphorical highway toward EFP. Trajectory equifinality model: Tall girl you are beautiful.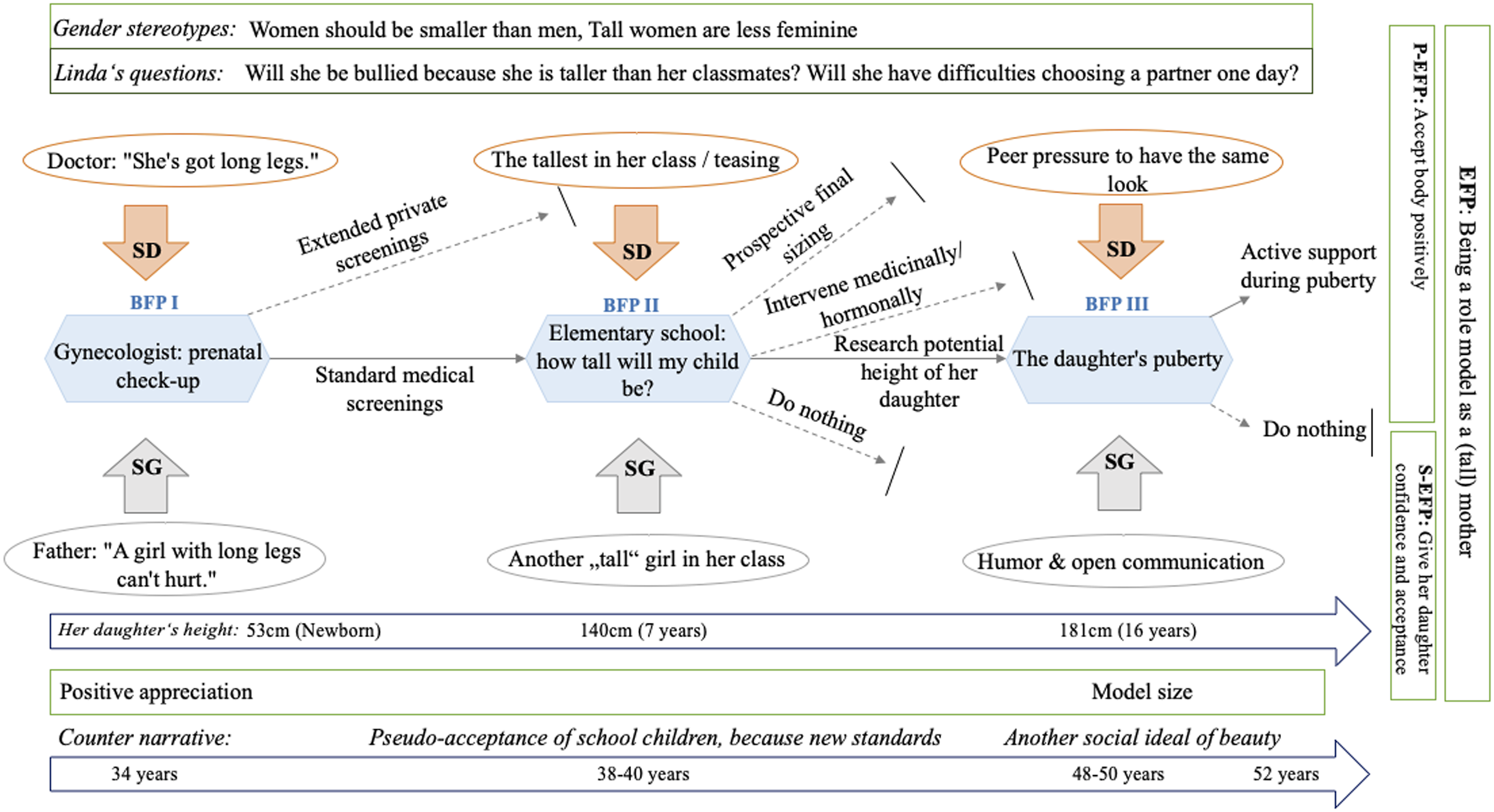
Entering pregnancy – “she was a wish child” - BFP I
Linda lived in the Netherlands during this period of her life, together with her then husband. Relatively “late” the two decided to have a child, which she herself described as a “wish child”. At the age of 34, Linda became pregnant and her journey into motherhood began. As a native German in the Netherlands, Linda found her pregnancy challenging because the health care system and prenatal screening were very different from those in Germany (l. 34). With this she referred to the hardly any examinations by a doctor. In view of the fact that Linda was approaching 35 and her ex-husband was 10 years older, she decided on her own initiative to have an ultrasound examination in the fifth month. During the ultrasound, the attending doctor was already commenting on the height of her unborn daughter, saying, “Oh she has some tall legs (l. 78–79).” Her alternative at that time was now to have further examinations. When asked how this realization of the option felt to her, Linda related that she was initially more amused by the doctor’s statement than concerned. Why should she? After all, her unborn daughter seemed healthy. In the end, she declined to have any further tests - she put it this way: I thought to myself with the father no matter, with 2 meters body height it was actually clear that our child will be rather taller (OPP I). We grinned and thought, well a girl with long legs can’t hurt (ll. 97–100). She seemed healthy and I didn’t feel comfortable just doing special investigations because of this comment (ll. 102–103).
Linda decided against further examinations, it should remain the last one before the, formulated by her, upcoming adventurous birth (l. 114). By this decision, she resisted the social requirement (SD) such as that she might be labeled as not being a good, caring mother, as she did not further address the attending physician’s comment. Had she had further testing done without a health need, it could have not only caused more stress in the pregnancy, but also confirmed what Linda once expressed as follows: In Holland, you don’t actually go to the doctor during pregnancy, only to the midwife. This is something quite natural and normal there. You basically only go to the doctor if something is wrong (ll. 55–58).
The casual remark of the attending medical practitioner (ll. 78–79) could have put her in a social tunnel from which she probably would not have found her way out so easily. At the very beginning of her motherhood, she would have followed the path of the norm. Accordingly, this alternative would have tended to push her away from the EFP. At the same time, her sense of humor and another ideal of beauty (having long legs as a woman) that is embedded in parts of our society could have led her to move toward EFP. Namely, being a mother who gives her daughter self-confidence with her taller than average body height, encourages and acts as a role model herself as a taller woman.
Growth and limits – BFP II
Five years passed and Linda’s daughter grew. Already in elementary school it was noticeable that she was the tallest in her class - as she still is today (OPP II). In elementary school, this deviation from the norm was not as conspicuous as Linda describes it here: Of course, she quickly realized that she was indeed the tallest of them all. But luckily there was another girl who was also very tall - I was incredibly grateful for that. And with a total of only 13 children in the class, the average height also increased somehow (ll. 292–296).
Based on this statement, it can be determined that the other taller girl in the class helped to curb exclusions and bullying because she was not the only taller girl standing out from the crowd after all. Therefore, the fact for more acceptance among the school children can be recorded as SG based on the fact that Linda’s daughter was no longer on her own and was less likely to “step out of line” on average due to the small class size. This also helped her towards S-EFP, namely giving her child self-confidence in her life journey and showing that there are other taller girls like her. Counter narrative is also interesting at this point; because: Acceptance of her body height in her social cohort, could only occur when a “peer” was added to the class system. A truly positive body image could only seem to be developed and did not come from Linda or her daughter themselves. It would be conceivable that on the part of the social subsystem as well as on the part of Linda and her daughter, one can speak of a so-called pseudo-acceptance of their own body height at primary school age.
It could be argued that Societal Dominance pushed Linda into the decision to document her daughter’s growth using a growth chart despite the classmate who was perceived to be more accepting of her daughter. In further conversation, Linda expressed that she observed how rapidly the growth was increasing and as a result, she became curious and began researching on the Internet about her daughter’s potential final body height. After I asked her what led her to do this, she responded as follows: [...] looked on the net times. Simply for me to see what there are actually for possibilities and how tall she becomes. So what is the ratio? Will she be as tall as her father or like me, or something in between? I was interested in the estimated value, because I have always secretly hoped for her that she will not exceed 1.85 m (ll. 164–168).
Social demands on women and their femininity in particular are washed to the surface here. Not only Linda, as a mother, but also her growing daughter seems to be exposed to these, even if not necessarily consciously. Accordingly, a societal ideal of women is aspired to, and it seems as if Linda is worried that her daughter will not be able to come close to it. But what is really behind Linda’s question of what body height her daughter will finally reach and whether she will crack the 1.85 m mark, although she is in perfect health and no physical impairments are to be expected due to her height? It is possible that Linda is confronted with two elementary thought structures that are based on gender stereotypes. One might be the idea that women should ideally be a little smaller than men. This, in turn, could fuel the question of whether Linda’s daughter might experience difficulty in choosing a mate, given her potential body height of over 1.85 m. A mother usually wishes only the best for her child, but at that moment when such a thought sprouts up in her, many experiences and deep-rooted attitudes seem to resonate, fueling her worries: I have a colleague who is 1.88 m and also very thin, maybe I’m still lagging behind the old, the man should be but best a little taller. Is not written anywhere, but the pressure is there [...] Equal taller is also ok, but if the woman is then so 1.90 m tall, that can also scare off many men (ll. 176–183). Very tall women also often have bad posture and the whole charisma is affected by it. They usually don’t wear high heels, but flat shoes like my colleague and are often bent over so that they don’t look even taller (ll. 185–188).
Linda’s inner voice of the so-called non-ideal becomes louder and louder: She herself associates a lot of negative attributes with women who do not fulfill a certain social and also homemade ideal because of their “too tall” body height. The way she describes her colleague’s appearance indicates that she herself is ambivalent about her thought structures, such as “the man should ideally be a little taller” (l. 180). On the other hand, she often emphasizes during the interview that it is “actually nonsense” (l. 180) to think this way. What is thrilling about this passage is that Linda (as a taller woman herself, mind you) has a crystal-clear picture in mind of what makes taller women and what they radiate. Linda exclusively refers to bad attributes here: a bad posture, difficulties in choosing clothes and shoes, which is accompanied by a negative visual impact on the overall external image. Last, she mentions a stooped, bent posture, indirectly claiming that women try to make themselves small because they are ashamed of their appearance. A mother who is so caught between her own ambivalences initially tries to ward off the thought with humor that her daughter might one day become so tall. But as her life progresses, Linda must confront reality and reframe her own ideals so that she can be the role model for her daughter that she wants to be (EFP).
Lastly, Linda reports that she experienced it as challenging to grow up so quickly at such an early age, as her daughter was often valued as older by strangers. Along with this, Linda feels that expectations for the child also increase: People tend to think the child is older because of the body height. You think she’s two years older, but no, she’s not. She was often overwhelmed because the expectations were being placed on her taller and that made her feel insecure (ll. 221–223).
Accordingly, in her daughter’s elementary school years, not only teasing was central, but also societal and Linda’s own ideals of how tall women appear, what they exude or just don’t exude. In addition, there is a new aspect: the misjudgment of her daughter’s age. This resulted in her being misunderstood or misrepresented early on, which may have affected her self-esteem on yet another level. Her support here in particular is a key point in cushioning her daughter with self-confidence and making her realize that people are not what they seem at first glance. This attitude could move her daughter toward the S-EFP, i.e., generating a positive body image and standing up for herself, even if she is perceived to be out of the norm with her body height. It is essential to note here that the EFP has been biologically determined (Linda’s daughter reaches a height of 1.80 m) and is not specifically defined by the individual. Here, it is important to mention that EFP is only indirectly biologically determined (Linda’s daughter reaches a body height of over 1.80 m) and is not specifically defined by the individual but rather by a societal ideal, which can lead to an internalization of this norm.
During her previously mentioned research on the Internet, she came across a medical procedure (prospective final height determination), which makes it possible to determine the final body height on the basis of the child’s left hand bone. It was at this point that Linda encountered her second BFP: to have her daughter’s final height determined, to possibly intervene with hormone administration to curb growth, to do nothing, or to simply learn about potential body height. But what inhibited her from choosing these trajectories and what at the same time moved her to choose the one she did? I have been thinking for a long time, wavering between options. On the one hand I thought it is as it is, on the other hand I hoped that she will not be taller than 185cm (ll. 199–200). I did not have it determined, it would have been hard for me to influence it. You can probably control the whole thing a bit with hormones. But imagine that the child has side effects just because you as a mother think that she could exceed a certain height (ll. 201–204).
In this regard, the expectations of being a good mother who acts in the best interest of her child (SG) were weighted more heavily for Linda than the perceived societal attitudes and negative attributions of taller women (SD). At the same time, this decision moves her closer toward her S-EFP of being a mother who loves her daughter and, as a taller woman herself, also a role model. In doing so, she encourages her daughter and keeps in mind that “different” or taller, respectively, does not equal bad, but can also have advantages (l.234). Nevertheless, a counter-narrative can be discovered here as well, in that Linda points out the advantages instead of conveying self-love and acceptance in a norm-free manner. By deciding against prospective final sizing and hormonal treatment, she prioritizes the well-being and health of her child, escapes societal pressure, and accepts her as she is. Positive accompaniment is given to her chosen trajectory of leaving it at informing that she does not feel exposed to the responsibility of possible side effects of the treatment.
Puberty: Help Mom! - Everyone is smaller than me – BFP III
Already in her mother’s womb, it was noticeable that Linda’s daughter would most likely grow taller than other emerging girls and women her age. For as long as she can remember, she has been the tallest in class, and that was not to change as puberty progressed. As is well known, life in this stage generally does not prove to be an easy breeze, as most teenagers face a number of changes and developmental processes. According to Linda’s descriptions, she faced her daughter with even additional underlying issues at this time: She definitely deviated from the norm with her body height [...] The norm is something very constricting and anyone who deviates from it is often bullied or ostracized and then of course she felt that in the form (ll. 275–279). The peer pressure is so high. All the girls have long hair, all the girls wear the same jeans, all have the same T-shirt [...] Everyone wants to have the same thing and anything that is different from that is not good at all. Then when you deviate with your body height [...] that torments her tremendously because she can’t change it (ll. 301–308). I don’t think you want to be an eye-catcher in your teens anyway, it’s all quickly embarrassing. And she stands out directly, was often ostracized because the others find it “weird” (l. 330) that she is taller than 180 cm at 16 (ll. 323–325).
In this phase of her daughter’s life, too, Linda reports on social exclusion and a prevailing non-tolerance, which they had to face again. In the analysis of BFP II, Linda describes how she perceives her work colleague, nailing down her shoes and choice of clothes, among other things. Hence, there also seems to be difficulty in literally “fitting in.” Perhaps at this stage of her life, when so much seems to revolve around appearances, it is not possible for her daughter to wear the same pants as other girls in her class. At this moment, we are moving on yet another level of the so called norm. Children and teenagers are often rejected or ridiculed by their peers if they seem to be just a little bit different. So, if in Linda’s daughter’s case, not only is her being tall an obvious flaw and cause for teasing, then additionally “not fitting” clothes and shoes as Societal Dominance could make her an unwanted eye-catcher and outsider. At this point, Linda tries to coax her daughter with the help of another counter-narrative by repeatedly telling her that she has a “model size” (l. 229). Probably unconsciously, she picks up on an opposing, socially anchored ideal of beauty: having long legs and a certain body height, which is often in demand in the fashion world and offers the option of postulating a size that deviates from the norm as something beautiful. While this leads to her daughter feeling better about herself and accepting herself and her body in a positive way (towards S-EFP), this growing self-acceptance is regulated by the variety of pseudo-concepts of beauty ideals. Here, Societal Dominance and Societal Guidance negotiate a personal solution. This is especially strengthened by the feeling given to a tall woman (and the woman herself).
Metamorphosis of a young life – Marie
Marie’s data analysis also proceeds according to the TEM. In the constellation as Linda’s daughter, she represents a young woman who is now 17 years old and who, contrary to medical recommendations, has not decided to have her final body height determined. After Linda has presented the maternal point of view on Marie’s trajectories of life regarding her body height, her own perception shall follow. Marie’s path can be divided into three elementary bifurcations (BFP’s) that accompany her process of negotiating her body height. Marie’s EFP can be defined as a continuous self-acceptance and the S-EFP is the refraining from overthinking whereby her P-EFP is to appreciate her own body as it is. These and other variables, such as Societal Dominance and Societal Guidance, will be presented in the form of a general overview in the following Figure 3. Metamorphosis: From a caterpillar to a butterfly.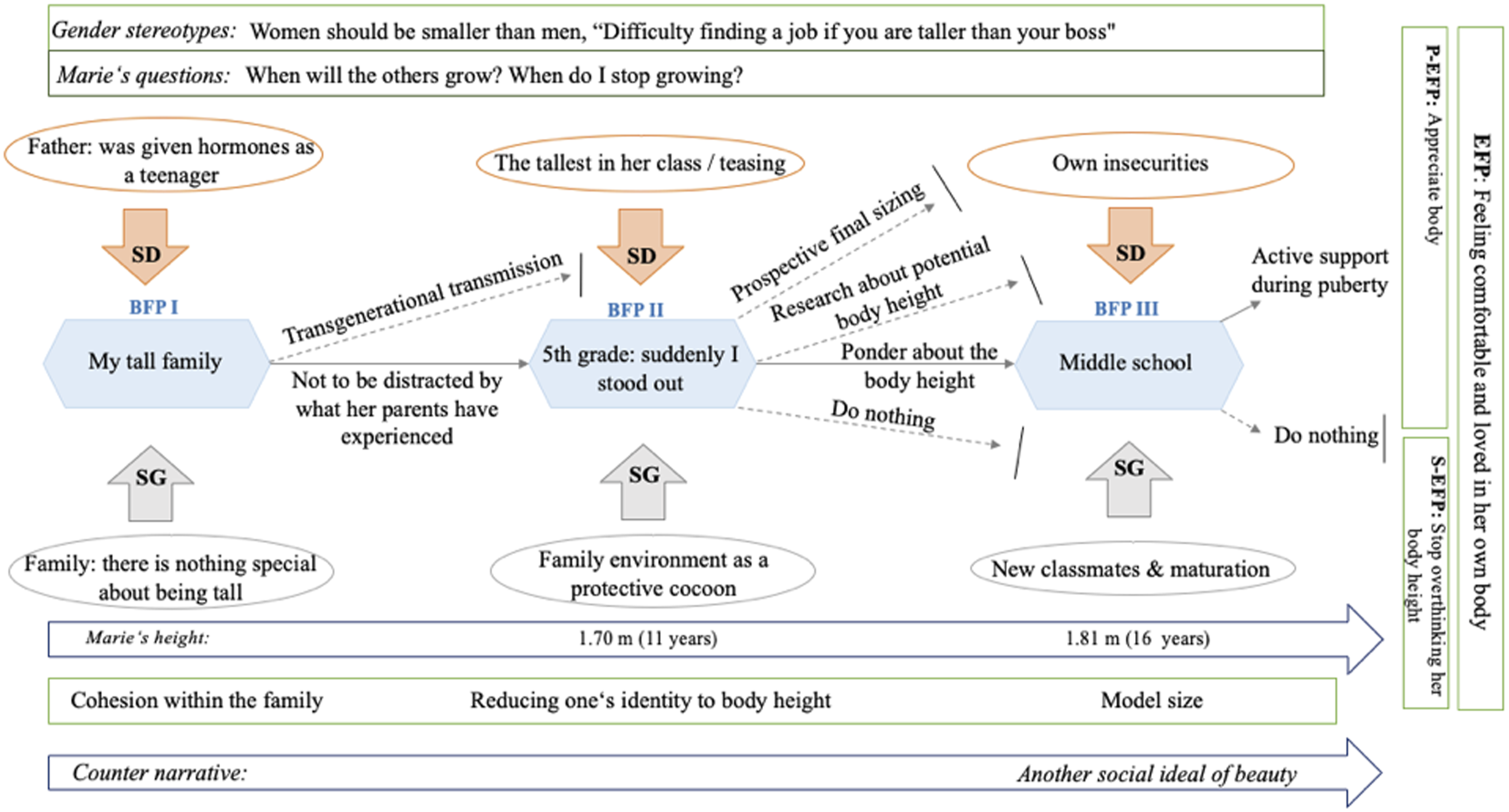
Before I was born - BFP I
Already at the beginning of the interview, Marie referred to the body height of both her parents. She emphasized that her mother, at 1.80 m, and her father, at 2 m, are above average (Marie, l. 11). Her father in particular came into focus. Because of his body height, he had to take growth-inhibiting hormones himself as a 16-year-old in order to curb his later expected body height (Marie, l. 13). Overall, according to Marie, most people in her family of origin are relatively “tall.” Therefore, it took time for her to see her body height as something she would have to negotiate with herself and be subject to some social normativities. While growing up, she became aware, among other experiences, through her father, that “being tall” could be associated with remarks on the part of the medical perspective: [...] my father is, after all, 2 m and he was always advised by the doctors at that time that he should under no circumstances seek a tall woman. Also so that the children would not become too tall (Marie, ll. 87–88).
Even if this statement refers to Marie’s father, it could have influenced her obliquely and bears the risk of a transgenerational transference of this external, medical conception, which could result in stigmatization. The medical professional’s remark here could be found to be so-called prenatal Societal Dominance, since Marie was not yet born at that time, but she is subsequently born into a world in which ideas about her, as her father’s child, already prevail. In the first BFP, Marie took the path of not letting herself be distracted by such comments and events that had already transpired on the part of her family, and of internalizing this normativity or even accepting the alleged transgenerational adoption. This is also actively affected by Societal Guidance, in that her family educates her about it while also teaching her that there is nothing wrong or abnormal about being taller than other people. [...] from my family’s side, it was always pretty normal. We were all tall, so it was never portrayed as something special. That’s why I only noticed it outside of home, because you have a lot of contact with other people (Marie, ll. 153–155).
Even at elementary school age, Marie’s thoughts, by her own admission, did not revolve around herself and her body height that much, although at the age of seven and a height of 1.40 m, she appeared somewhat taller than others her age. The perceived first point of exposure for her was at the beginning of fifth grade, when Marie realized that she was the tallest in her class. She states that her own perception of “being tall” came to her only belatedly, because she did not stand out in her family with her body height. Her family and in particular their internal handling of her body height can be seen as Societal Guidance. In this case, Marie’s family acts almost like a protective cocoon, giving her time to learn to accept herself as she is, as if in a kind of metamorphosis, and to have role models such as her mother Linda, who sets an example as a tall woman.
Marie the tall one - BFP II
The metaphorically described breakout from the cocoon also marks her first step towards BFP II (the decision to make a prospective final height determination, to leave it at Research of one’s own final height, to take no further action or to continue to ponder one’s own final body height) when Marie enters the fifth grade of a high school. At this time, Marie made another “real push” (Marie, l. 48) in terms of her body height and was perceptibly taller than her classmates.
In fifth grade, I truly noticed that I stood out from the crowd. And I’m just taller. I considered that to be silly and would have liked to be small and petite like all the other girls. Especially when it starts in middle school with boys, that’s when the wishes start to come up (Marie, ll. 52–55).
Noteworthy here is that Marie’s mother Linda also named standing out from the crowd as a strong influencing variable that can cause increased uncomfortable feelings and fuel intrapersonal negotiation at a certain stage in life. Marie’s self at the time also seems unhappy and almost ashamed about embodying a characteristic with her body height, which makes her stand out from other adolescents her age. The unwanted conspicuousness at the beginning of puberty can clearly be titled Societal Dominance. The entry into this physical development and exploration phase seems to be an essential BFP, which holds a lot of variables of Societal Dominance and Societal Guidance in store and paves the further path for possible chosen or not chosen but thoughtful trajectories of Marie. Her expressed desire to be small and petite like the other girls in her class (Marie, l. 53) seems understandable when it is considered that her standing out from a cohort of peers, initially regardless of whether boys or girls, is something for which Marie has also faced ridicule. For the first time, she views her body height as something negative through the influence of others. Her internalized need to be equal is also to be understood as Societal Dominance, as Marie stands in her own way and inhibits herself in the direction of her EFP. Moreover, that desire seems to go hand in hand with Western-anchored ideals of beauty, which are also related to certain visual gender stereotypes (the man should be taller than the woman, if I as a woman am taller than the boys in my class, I might not find a boyfriend). Despite the existing Societal Guidance in the form of her family, it seems that the social pressure in the school context due to bullying, own ideals and ideas regarding body height, general development processes and other female classmates is stronger than that counter-narrative. Above all, Marie was bothered by the fact that she was always categorized by others because of her physical appearance: [...] I was then put into one of those pigeonholes. I don’t know, one is the class clown, then there’s the prissy one, the nerdy one, and then there was me and I was Marie the tall one (Marie, ll. 62–64).
Behind this categorization by the class community given in this instance, there is also an externally imposed role and attribution of identity, based on an external characteristic. The question of one’s own adoption and internalization of this is to be seen critically. Marie also names other examples of compartmentalization of her classmates, which all refer to character traits, but not to directly visible or optical ones. This reduction to a certain, perceptible characteristic can also be seen as Societal Dominance, since Marie would like to break free of this construct at this moment and even, as previously described, harbored the desire to be small and petite. At the same time, a Societal Guidance could emerge from this Societal Dominance, since she titles herself as “the tall one” (Marie, l. 64) and possibly makes an external imposed role her self-perception, which in this case, does not necessarily have to be negative. It could even be an opportunity to see her body height as a part of her identity and to come one step closer to her EFP. Marie continues to talk about habits she had during her time in junior high school, which provides clues to her negotiation with her body height at that time: I always stood in a circle with other girls, and I remember very well that I always shifted my weight to one leg and then always pushed my hips out so that I would be one centimeter shorter, so that somehow it wouldn’t be so noticeable (Marie, ll. 136–139).
Marie experiences several fluid stages with herself in relation to her body height and constant growth even within this BFP. At home, her mother loves her as she is (Societal Guidance) and does not pay special attention to her height, since all family members tend to be “tall”. Contrary to this, Marie experiences a kind of bullying for the first time, a reduction because of that. She is made aware with the constantly repeated phrase “Marie the tall” and equally aware that her body height is a part of her, even if she finds it repulsive and not belonging at some moments. Here, the seemingly internalized Societal Dominance of the need to be equal develops into an emotion of shame, which Marie tries to hide by pushing her hip to the side. Interestingly, mechanisms can be observed which act like a catalyst. A series of social pressure as well as social support, which changes scenically, depending on the time of day and the environment, and which is partly internalized by Marie, then externalized again and again re-filtered. During this trial, the question of whether Marie should undergo a medical measurement to determine her final body height comes closer to her mind. After thinking about it for a while, Marie’s mother in particular decided against that option. However, Linda informed herself about the medical options for determining the final size and researched how tall her daughter could ultimately become. Marie, on the other hand, continued to ponder her final body height. Taking that trajectory was primarily related to the fact that Marie was under some social pressures at the time, fueled by the onset of puberty and the growth spurt and teasing of her classmates. Ultimately, she and Linda decided not to go through with it. Part of the influence in this regard was the fact that the other students were also developing and that the boys in Marie’s class in particular were growing taller (Marie, l. 249). Along with this, according to Marie, the comments and the pure reduction to her body height also decreased. This Societal Guidance (the “following” of others) in turn moves her towards her EFP’s and the S-EFP of not worrying excessively all the time seems to move a step closer. Marie states that for her there was a limit at which she would have retrospectively wished to have both a prospective final sizing and to accept a medical or hormonal indication. She refers to a personal limit of 1.90 m for her as a woman: Not that every 1.90 m woman is unhappy, but in everyday life one is then already restricted (Marie, l. 98). And with 1.81 m I don’t have something like that yet, but with 1.90 m something like that could certainly start (Marie, l. 197).
When questioned whether Marie would have wished in retrospect that a medical intervention had been made, she stated that she finds a body height for women of 1.90 m or more problematic. Here she draws particular attention to everyday things, such as making it harder to negotiate with oneself if, for example, the kitchen counter is always a little too small, the bed too short, and even the pants never fit in terms of length (Marie, ll. 195–196). A clearly definable Societal Dominance, which would have led Marie to take action against her growth, is due to everyday standards of life, being oriented to the mass and average height of people. This potentially perceptible human-created Societal Dominance seems to trigger something in Marie that would have caused her discomfort and leveled the choice of a differentiating path (option of prospective final size determination and hormonal indication, if necessary). What is impressive at this point is that Marie as an individual would have shown willingness to change in order to fit into a societal norm, even though she critically reflects on the home-made system.
School change - BFP III
The third station of Marie’s life path so far is primarily intended to shed more light on her trajectory after middle school, in which she underwent a change of school. In the further course, the BFP shall be taken up, how her current situation and the negotiation of her body height in her new environment. In middle school I stood out more and yes now I’m tall too, but it’s not as obvious anymore. But maybe it’s due to age. Children are mean and have no feeling for it. The older you get the more empathy there is also and more often think about whether you say something. In the past, what came from the outside was much more unfiltered (Marie, ll. 256–259).
It is evident from the excerpt that the teasing in particular, which she experienced at the beginning of fifth grade (see BFP II), has become blurred with the change of school and the accompanying increase in age. The school change itself, and the changing social environment, seems to represent a Societal Guidance factor at this point in her life. This influencing variable can be described in more detail, as it seems that the decision to switch schools had a positive impact on Marie, especially since she is now surrounded by new adolescents and they are already in the process of growing due to her age. She no longer protrudes from the class community to an uncomfortable extent (Marie, l. 256). It should be kept in mind that the new class situation itself could produce an improvement in well-being, since no one there knew anything about Marie’s time in fifth and sixth grade. Another component of Societal Guidance at this crossroads in her life is age. Marie describes that as she grew older, those around her, as well as herself, would be more reflective of what was said and things would no appear “unfiltered” (Marie, l. 259). Parallel, she attributes more empathy and consideration to her fellow human beings. It remains open whether this behavior, which she attributes as understanding, is to be equated with a sincere acceptance of her own person or whether this also partly reflects a social conformity on the part of the young people. This fusion of influences merges into Societal Guidance, which can be described as the maturing of the social environment. Furthermore, there consists a Societal Guidance which refers to a natural maturation process, which seems to be unstoppable and primarily pertains to the physical growth and further development of the classmates. Marie also underlines this observation with the following statement: It’s all receded and then when the body is also finished developing and you have the feeling that you’re not growing anymore, it’s also easier (Marie, l. 252).
She describes it as a sense of relief to notice that, for one, she no longer stands out so much in class and is the only “tall” person, and for another, Marie seems to be steadily worrying less about her body height as she notices that her body appears to be full-grown. This containment of worrying too much about her body height and how it compares to others can plainly be seen as a big step towards her S-EFP’s. It could be argued that this step towards her EFP could have been generated more quickly if Marie had known a few years earlier how tall she would become. The certainty in this regard could have been stated as Societal Guidance and would have possibly inhibited the uncertainty as a counterpart to the Societal Dominance that occurred. It could be speculated that in Marie’s case the negotiation of her own identity, which is interwoven with her body height, would have been easier for her if she had used medical measurement to determine her final height. My goal was always to be fine with it and to accept myself with my body height. And also not to worry so much all the time. I always thought about it way too much (Marie, ll. 241–243).
From her current life situation, Marie mentions that looking back on this process, it was always relevant for her to feel acceptance for herself and her body height. Along with this, she was also accompanied by the desire to experience love for herself and to brood less about those norms and “not fitting in” and possibly internalize this. A very long, courageous and persistent path, which according to the TEM’s will never be finished and will always come across new points of negotiation in the future. Connected with new influences of Societal Dominance as well as Societal Guidance, which could drive them in another, new stage of life in the direction of EFP or away from it.
How SD and SG are coordinated: Counter-narratives
On closer inspection, it becomes apparent that these two already elementary components of the TEM, have an additional function. Societal Dominance and Societal Guidance can counteract or reinforce the human-made norm. So-called counter narratives were discovered in this paper, which seem to give the two components a new dynamic. Counter narratives describe a kind of leverage, which for instance counteracts a weighty norm with another underlying concept created by a society itself. In the paper, one such could be explored right at the beginning, when Linda’s ex-husband responded to the doctor’s comment that his daughter had very long legs at the screening examination by saying that a girl with long legs couldn’t harm. What is interesting here is that by saying “long legs in women can do no harm” (SG), he relates it to the concept of femininity and beauty, neutralizing the doctor’s Societal Dominance of “your daughter is taller than the other girls and does not conform to the norm,” with another social ideal. This beauty ideal of long legs opposes the norm (women should not be so tall, her daughter is taller than average) and weakens it. The counter narrative functions not only as a lever but also as a regulator that can neutralize or reinforce both Societal Dominance and Societal Guidance in some ways. Counter narratives have multiple manifestations, but they can have different effects on Societal Dominance and Societal Guidance. Thus, they also create acceptance, which, must be viewed critically in the context of this study and tends to be classified as pseudo-acceptance. With regard to the Societal Dominance perceived by Linda, that other girls are significantly smaller than her daughter and that she even experiences bullying for this in elementary school, the statement “you have model height” can transform the body height as a negatively classified and genetically determined aspect into something positive and socially even recognized and admirable. Counter narratives seems to be stable over time, especially since it allows a long-term and sincere confrontation with cultural norm deviations to be socially circumvented. It could be argued that this can have an impact on those affected, as it makes honest self-acceptance more complicated. At first glance, the short-term categorization and the resort to other beauty constructs or functionalities give the impression of making a compliment to the person – yet, this is based on a biological component to which the woman is repeatedly reduced. In our Western society, we often try to find meaning and, above all, utility in the things we do. So when Linda’s daughter, because of her height, is asked to try a sport that is symbolic of height, a function seems to be sought for her body height - a sociocultural fit. Counter narratives are seen as based on socially embedded assumptions, stereotypes, and entrenched patterns. In the process, these prove to be enormously powerful and seem to have the ability to regulate, neutralize, undermine, and shatter both Societal Dominance and Societal Guidance.
Norms and genetics – compatible?
Norms have existed since time immemorial and are often passed on over generations in a culturally specific manner. The prevailing normativity and conception of what a woman should be and look like is also not only manifested in the course of life, but already in the womb. In doing so, our being that thinks and acts in norms encounters boundaries of something much bigger than us our genetics, our growth, our nature. This is also evident in this work through Linda’s and Marie’s contested trajectories, which were and are conditioned by societal influences, some of which are based on counter-narratives. Counter-narratives helped the mother-daughter pair to approach their EFPs, yet the question arises to what extent they are sincere and can be understood as enduring over time. Likewise, (gendered) stereotypes are perpetuated in this way. Accordingly, counter-narratives can reduce social pressure for a time, but break it up again at another point. An interface to be explored more deeply here could be the link to pediatric medicine, whereby it could be examined how the life paths of those affected and their families change should a medical indication, by means of hormone therapy or orthopedic minimally invasive surgery, be undertaken in early childhood.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.