
Abstract
The outbreak of coronavirus disease 2019 (COVID-19) has disrupted the global economy. Since containment measures directly limit mobility and social interactions, the pandemic has substantially affected the tourism sector. This work explores the effect of COVID-19 exposure on people’s travel intentions during the summer of 2020 use representative survey data for 3873 individuals collected in Spain, one of the countries with the highest infection and mortality rates. We define exposure to COVID-19 at two levels: (i) zonal, according to the degree of limitations imposed in the zone where the respondent lives, and (ii) individual, according to whether the individual has personally suffered from COVID-19 symptoms. We perform regression analysis and propensity score matching and also consider potential treatment heterogeneity. The results consistently show that those who were more severely affected by the pandemic exhibit a relatively higher willingness to travel.
Introduction
The outbreak of the severe acute respiratory coronavirus disease 2019 (COVID-19) has proved to be disruptive to the global economy. To contain its spread, travel restrictions, border closures, and even lockdown policies have been implemented in many regions. In countries such as Spain, Italy, and France, governments have adopted movement restrictions and forced the shutdown of many nonessential activities.
Predictably, the tourism and travel industry has been one of the sectors most affected by the pandemic. Due to its dependence on mobility and social interactions, containment measures and travel bans are particularly detrimental to this industry. Indeed, international tourism flows have been associated with the overall level of confirmed COVID-19 cases and deaths (Farzanegan et al., 2020). In addition to the temporary closure of hotels and restaurants during the peak phases of the pandemic, ongoing social distancing and crowd prevention are also expected to significantly reduce tourism demand in the medium term. Given this context, consumers’ responses to the fears and uncertainties related to the pandemic—especially concerning their willingness to travel—are relevant to policy.
An emerging body of research studies the consequences of the current pandemic for the travel, tourism, and hospitality industries (Assaf and Scuderi, 2020; Gil-Alana and Poza, 2020; Qiu et al., 2020; Sigala, 2020; Tsionas, 2020; Zenker and Kock, 2020). The preliminary evidence points to a significant drop in revenues, especially in tourism activities that involve confined public spaces like hotels or cruises (Sharma and Nicolau, 2020). In this regard, previous studies on the effects of health-related crises like Ebola, malaria, and avian flu show that tourists tend to avoid traveling to affected areas when their personal safety is threatened (Cahyanto et al., 2016; Novelli et al., 2018).
However, the current pandemic differs from previous health crises because of its worldwide extension. COVID-19 presents a nearly homogeneous shock for all potential destinations. Contrary to previous health crises, it could affect overall travel intentions rather than redistributing tourism flows among alternative destinations.
This work examines the effect of COVID-19 exposure on travel intentions for the summer of 2020. We consider two levels of exposure: (i) zonal, according to the movement restrictions imposed in the zone where the individual lives, and (ii) individual, according to whether the respondent has suffered from COVID-19 symptoms. On the one hand, we exploit the heterogeneity in restrictions across provinces in the de-escalation process that followed the lockdown in Spain. On the other hand, we study whether self-reported COVID-19 symptoms affect travel plans.
We use survey data from a representative sample of the Spanish population (3873 individuals) collected during the first week of June 2020. At that time, part of the country (40 provinces) was at “phase 2” of de-escalation. People in these provinces were subject to weaker restriction tiers; by contrast, the remaining 12 provinces were still in a previous stage due to their worse epidemiological situations (phase 1). These provinces were forbidden from carrying out several activities like practicing outdoor sport or going to the cinema, among others. This scenario could be seen as a natural experiment that allows us to assess how movement restrictions affect individuals’ willingness to travel over the summer period. Furthermore, the respondents are asked whether they had to contact health services because of having COVID-19 symptoms. Therefore, we examine whether individual exposure to COVID-19 affects travel intentions, controlling for sociodemographic characteristics, political orientation, and religious beliefs.
Our study is similar to that of Kourgiantakis et al. (2020), who study the impact of COVID-19 on holiday intentions on the island of Crete (Greece). In contrast to their descriptive evidence, we present a formal analysis using three methodologies: (i) regression analysis, (ii) propensity score matching (PSM), and (iii) a novel weighted estimator developed by Sloczynski (2020). Drawing on the program evaluation literature (Dehejia and Wahba, 2002; Heckman et al., 1998), we also address (i) the potential moderating effect of confounding factors like personal characteristics, (ii) nonrandom treatment assignment, and (iii) heterogeneous treatment effects.
We find clear and robust evidence that both inhabiting a zone with a worse epidemiological situation and having personally suffered COVID-19 symptoms increase the willingness to travel in the summer relative to controls for the same observation period (beginning of June 2020). This is confirmed by the three above-mentioned methodologies. We argue that these results reflect an intuitive dynamic: people who have been more exposed to the disease are relatively more in need of travel, escape, and relaxation after strict containment policies. Tourism travel has been shown to enhance people’s well-being through the emotional and hedonic components of traveling experiences, which, in turn, significantly influence behavioral intentions (Gilbert and Abdullah, 2004; Hosany and Gilbert, 2010; Sirgy et al., 2011). The results are thus in line with substantial evidence in the literature on tourism (e.g. de Bloom et al., 2017), travel medicine (e.g. Strauss-Blasche et al., 2005), and psychology (e.g. Etzion, 2003), showing that tourism can help people recover from bad experiences by relieving anxiety, stress, and burnout.
The remainder of the article is structured as follows. After this “Introduction” section, the second section reviews the related literature. The third section describes the data and presents some descriptive statistics. We also outline the lockdown that took place in Spain from March to May 2020 and the de-escalation phase. The fourth section explains the methodological framework. In the fifth section, we present the estimation results. Finally, the last section concludes with a summary of the findings, implications, and areas for future research.
Literature review
There is a growing body of literature on the short- and long-term consequences of COVID-19 on the tourism industry. These studies can be classified into four groups depending on their research purpose: (i) the economic and social costs of the pandemic on the travel and hospitality sectors (Baum and Hai, 2020; Gil-Alana and Poza, 2020; Qiu et al., 2020; Sharma and Nicolau, 2020; Sigala, 2020), (ii) potential changes in the tourism paradigm (Brouder, 2020; Gössling et al., 2020; Hall et al., 2020; Kock et al., 2020; Prideaux et al., 2020), (iii) recovery measures (Assaf and Scuderi, 2020; Tsionas, 2020), and (iv) tourists’ behavior and risk perceptions after COVID-19 (Gallego and Font, 2020; Kim and Lee, 2020; Kourgiantakis et al., 2020; Li et al., 2020; Neuburger and Egger, 2020; Wen et al., 2020).
This article lies within the last stream of the literature. We examine how exposure to COVID-19 affects traveling plans for the summer period immediately after the lockdown. On the one hand, those with higher exposure might be more afraid to travel, perceiving the risks of contagion to be greater away from home. On the other hand, higher exposure might instead increase the need for escape and, in turn, the willingness to travel.
Aversion to travel
Previous studies in tourism and psychology research show that people tend to avoid traveling after disease outbreaks if they perceive their personal well-being to be threatened (Chien et al., 2017; Novelli et al., 2018). According to the protection motivation theory developed by Rogers (1975), people adapt their behavior to protect themselves and are thus heavily dependent on subjective perceptions about risks. Relatedly, Wang et al. (2019) report a low level of adaptation among those who are excessively optimistic and do not realistically assess the risks of traveling. Furthermore, fear of traveling varies with individual and trip-related characteristics (Fennell, 2017) and cultural background (Seabra et al., 2013). Females tend to be more risk-averse during disease outbreaks (Park and Reisinger, 2020), and perceived risk is lower among repeat visitors to the affected destinations (Rittichainuwat and Chakraborty, 2009).
Lee et al. (2012) evaluate the impact of nonpharmaceutical interventions in the aftermath of the 2009 H1N1 influenza outbreak, including social distancing, monitoring personal health before and after the trip, and getting more information on travel intentions and desires. They find that perceptions about the disease do not constrain the desire for international travel, instead of causing travelers to engage in adaptative behavior to reduce the threat to acceptable levels. Cahyanto et al. (2016) analyze domestic travel avoidance within the United States after the outbreak of Ebola. They find that those with greater perceived risk levels are more likely to stop traveling, whereas a higher self-efficacy related to adhering to preventive measures moderates perceived susceptibility.
Preliminary evidence of the effects of COVID-19 on travel intentions points in the same direction: diseases reduce traveling intentions. Gallego and Font (2020) show that air passenger searches for future trips dropped by 30% in Europe and the Americas and by 50% in Asia. Using data from TripAdvisor forums, Uğur and Akbiyik (2020) find that travelers canceled or delayed their trips as news about the health crisis spread. Li et al. (2020) document a decline in intentions to use public transport and an increase in the willingness to travel by private car. The authors also show an increase in intentions to shorten or even postpone their holiday trips since the beginning of the pandemic, although travel resilience notably differs among sociodemographic groups. Neuburger and Egger (2020) find that risk perception and the willingness to change travel plans increased 2 weeks before and after the pandemic outbreak was confirmed. Kourgiantakis et al. (2020) report mixed evidence, with some people canceling their trips and others keeping their plans.
Therefore, social distancing to prevent infection may lead people to cancel or postpone their travel plans, especially to crowded destinations. From this perspective, those living in regions with high incidence rates or who have had symptoms compatible with COVID-19 might be more averse to travel. Nevertheless, another line of research points to a change in travel preferences rather than travel avoidance from mass tourism to so-called “slow tourism” (Wen et al., 2020) and “untact tourism” (Bae and Chang, 2020). Wen et al. (2005) examine Chinese travel patterns following the 2003 SARS outbreak, finding that people became more interested in outdoor activities and ecotourism.
Higher exposure as a push factor
Despite the issues discussed above, there are reasons to expect that higher COVID-19 exposure could increase travel intentions. Several studies show that traumatic events result in drops in subjective well-being and life satisfaction (Bucciol and Zarri, 2020; Clark et al., 2020; Metcalfe et al., 2011), causing anxiety and lower self-esteem (Bunce et al., 1995). The positive psychology literature and tourism research both show that traveling can help people overcome stressful situations and bad events. Etzion (2003) provides evidence that taking an annual vacation reduces stress and burnout. Similar findings are reported by Fritz and Sonnentag (2006). Strauss-Blasche et al. (2005) find that having time for one’s self, exercising, and socializing in a warm vacation climate facilitate recuperation from mental strain. Moreover, Chen et al. (2016) conclude that taking a leisure trip acts as a stress reliever.
Buckey and Westamay (2020) show that outdoor and nature recreation can produce substantial psychotherapeutic benefits. De Bloom et al. (2017) report that physical distance from home correlates with engagement in resource-providing activities that reduce worries. Interestingly, these authors find that holiday travel improves personal well-being more than spending free time at home. In the same line, studies by Howell and Hill (2009), Howell et al. (2012), and Guevara and Howell (2015) show that experiential purchases like traveling improve people’s well-being more than materialistic purchases through increased relatedness and decreased social comparison. We refer the reader to Chen and Petrick (2013) for a detailed review of this literature.
Ozamiz-Etxebarria et al. (2020) report that Spain’s severe lockdown has caused depression, anxiety, and stress in the population. The lockdown may have increased individuals’ need to escape and relax, and this effect may correspond with the degree of COVID-19 exposure. Caplin and Leahy (2001) introduce a psychological expected-utility model in which anticipatory feelings about the future affect current well-being. Similarly, Brunnermeier and Parker (2005) develop a model in which agents care about expected future utility flows, and optimistic or pessimistic views thus impact their current happiness. Under this framework, those in areas with less freedom or who have personally experienced the negative effects of COVID-19 symptoms might suffer a double utility loss if they also cancel their holiday plans. Holding optimistic expectations about the near future related to going on vacation might thus enhance their current happiness.
Furthermore, there is extensive evidence that consumers tend to be overconfident and overoptimistic when forming beliefs about the state of the world. This tends to lead them to underestimate potential risks (Grubb, 2015) and overestimate their control over outcomes (Van den Steen, 2004). The psychology literature shows that if the perceived severity and probability of a health problem is low, the likelihood of engaging in protective behavior is also low (Weinstein, 2000). In this regard, Welder-Smith et al. (2004) report that only 4% of Australian travelers to Asia, Africa, or South America seek vaccination before traveling. Moreover, in the context of a flood of news about the pandemic, people might become information-averse because of the stressful emotional volatility that these information flows create (Andries and Haddad, 2020; Golman et al., 2017). Accordingly, they might be inattentive to the true risks of traveling.
In the Spanish context, the differences in restrictions across provinces might cause those living in phase 1 provinces to be more willing to travel to second residences or to other areas with fewer movement restrictions. From this perspective, the greater willingness to travel among residents of the most-affected areas could also stem from stricter movement restrictions in their home provinces, which act as an incentive to travel.
Data
Database
The data come from the Special Barometer conducted by the Spanish Center for Sociological Research (Centro de Investigaciones Sociológicas, CIS) in June 2020. The CIS is a public organism in charge of collecting public opinion data for economic, sociological, and demographic research. Each month, the CIS surveys a representative sample of the adult (over 18 years of age) Spanish population to ascertain people’s voting intentions, opinions about current affairs, and primary concerns. Personal and sociodemographic characteristics are also gathered (see below).
In the June 2020 barometer, the survey included for the first time a set of questions about holiday plans for summer 2020, alongside questions concerning (i) personal exposure to COVID-19 and (ii) concern about the pandemic. This special release of the barometer allows us to examine the links between perceptions about the pandemic situation and travel intentions. Since it is the first time the CIS has inquired about holiday plans, we cannot compare travel intentions before and after the pandemic outbreak.
A total of 4258 individuals participated in the June 2020 barometer. However, due to missing values in some of the variables of interest, the final sample for our analysis consists of 3873 individuals. The sampling was done in 1416 municipalities in the 52 Spanish provinces. The sample weights provided by the survey are used in the analysis to make the data representative. Due to the required social distancing, all the surveys were conducted by telephone.
Descriptive statistics
The survey respondents are asked the following question about their travel intention: “Do you plan to go on holiday this summer?” The question includes domestic and international travel. About 28% of the sample report to be willing to travel during the summer. 1 Most of this group state that they plan to travel within the country (90.6%), in line with the results of Kourgiantakis et al. (2020) for Crete. The low frequency of people willing to travel abroad (n = 103) and the corresponding imbalance between the two groups preclude a formal analysis of the differences between traveling domestically versus internationally. Therefore, in our analysis, we only study generic travel intention without considering the destination type. Figure 1 maps the percentage of respondents that planned to travel by province (Nomenclature of Territorial Units for Statistics, level 3). The provinces in Basque Country and the provinces of Barcelona, La Rioja, Murcia, Zaragoza, and Madrid report the largest shares of respondents with summer travel plans.
Individuals are also asked about whether they have experienced symptoms compatible with COVID-19 (i.e. dry cough, fever, or difficulty breathing) with the following question: “Have you had to contact health services due to having symptoms related to coronavirus?” Around 7% experienced symptoms before June 2020. Figure 2 depicts this share by province. Toledo, Cuenca, Huelva, and La Rioja reported the highest prevalence of declared COVID-19 symptoms (between 15% and 20% of the sample).
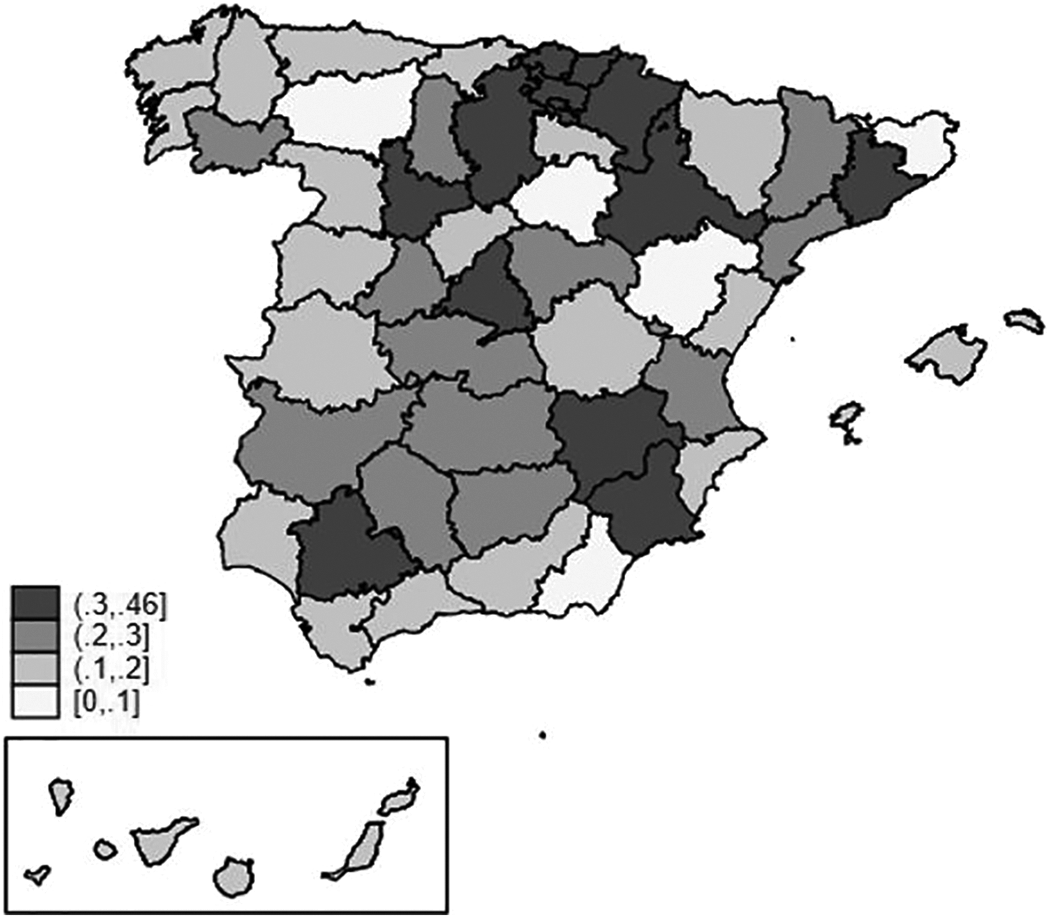
Travel intentions per province (%).
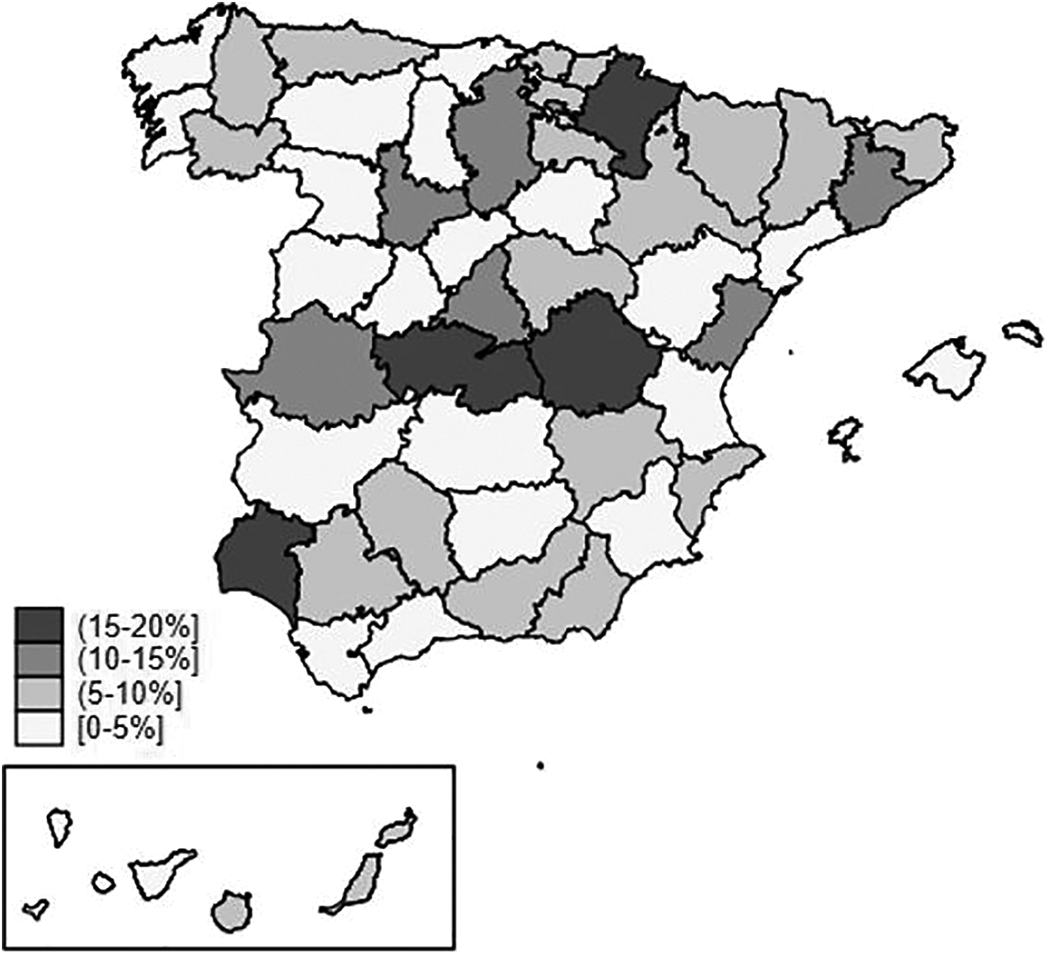
COVID-19 symptoms per province (%). COVID-19: coronavirus disease 2019.
The questionnaire also includes questions on sociodemographic characteristics, personal economic situation (as an indicator of income), political ideology, and religious beliefs. Table 1 presents summary statistics of the data. The average age of the respondents is 50 years old with 50.7% females and 18.9% active Catholics. The participants rate their personal economic situation as “moderate to good.” Most respondents place themselves near the center of the ideological scale with a slightly higher proportion of left-wing people. 2 The respondents’ households are composed of 2.7 members on average, with 54.2% married and 50.8% currently employed. About 26% of respondents are retired, with almost 5.1% being students and 4.5% being housekeepers (inactive). Concerning educational level, around 39.7% have high education, with a non-negligible 3.3% and 7.6% having no studies or only primary studies, respectively. Asked about their social class, most respondents place themselves in the upper middle (54.7%) or middle class (17.6%), with higher shares of working class (8.9%) and poor (7.4%) than upper class (5.9%). 3 Finally, when asked about the main problems in Spain at the time of the survey, 12.4% place the health pandemic situation in the first position.
Summary statistics (N = 3873).
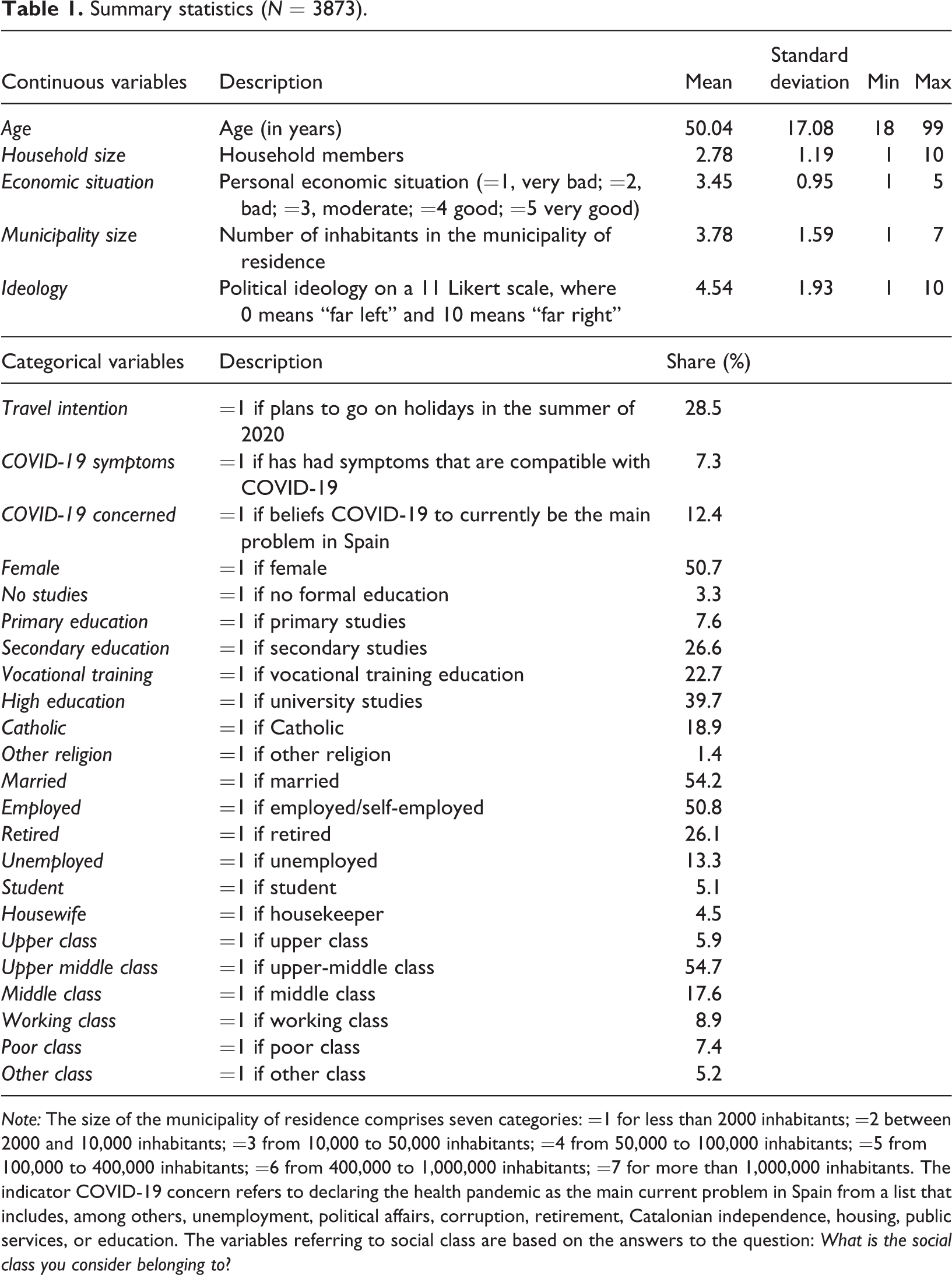
Note: The size of the municipality of residence comprises seven categories: =1 for less than 2000 inhabitants; =2 between 2000 and 10,000 inhabitants; =3 from 10,000 to 50,000 inhabitants; =4 from 50,000 to 100,000 inhabitants; =5 from 100,000 to 400,000 inhabitants; =6 from 400,000 to 1,000,000 inhabitants; =7 for more than 1,000,000 inhabitants. The indicator COVID-19 concern refers to declaring the health pandemic as the main current problem in Spain from a list that includes, among others, unemployment, political affairs, corruption, retirement, Catalonian independence, housing, public services, or education. The variables referring to social class are based on the answers to the question: What is the social class you consider belonging to?
Lockdown and the de-escalation phases in Spain
On March 15, 2020, the Spanish government declared a state of emergency (Estado de Alarma) to battle the COVID-19 propagation. 4 Due to the high risk of health system collapse and the increasing number of hospitalizations by mid-March, the government assumed all political authority and dictated an initial lockdown for 15 days (quarantine), similarly to the steps taken in other countries. The severe outbreak in Spain required a strict lockdown that lasted for almost 2 months. During the Easter period (the first two weeks of April), the government ordered a complete lockdown that impeded all nonessential economic activities and forced the population to stay home. Orea and Álvarez (2020) show that this decision effectively contained the spread of COVID-19.
To guarantee an appropriate transition to the so-called “new normal” and avoid new outbreaks, the state of emergency was extended six times and remained in force until June 21. By the end of April, the government passed a four-phase de-escalation plan. The government planned to return to normal life slowly and asymmetrically by regional areas, proceeding in periods of 2 weeks. Under this plan, the relaxation of restrictions and the recovery of free movement and social activities were gradual processes. Provinces moved to the next phase based on their epidemiological situation.
The data set was collected between June 1, 2020, and June 9, 2020. At that time, some provinces remained in phase 1 of the de-escalation plan, while the rest were already in phase 2. People living in areas in phase 2 were allowed to meet with up to 15 people, exercise at any time except during two periods reserved for children and the elderly, celebrate weddings, go to the cinema, and go to funerals, among other activities. By contrast, those at phase 1 were not allowed to carry out such activities.
Twelve provinces remained at phase 1 during the first week of June: Barcelona, Lleida, Madrid, León, Palencia, Burgos, Soria, Segovia, Ávila, Salamanca, Zamora, and Valladolid. 5 The remaining 40 provinces were in phase 2 (Figure 3). 6
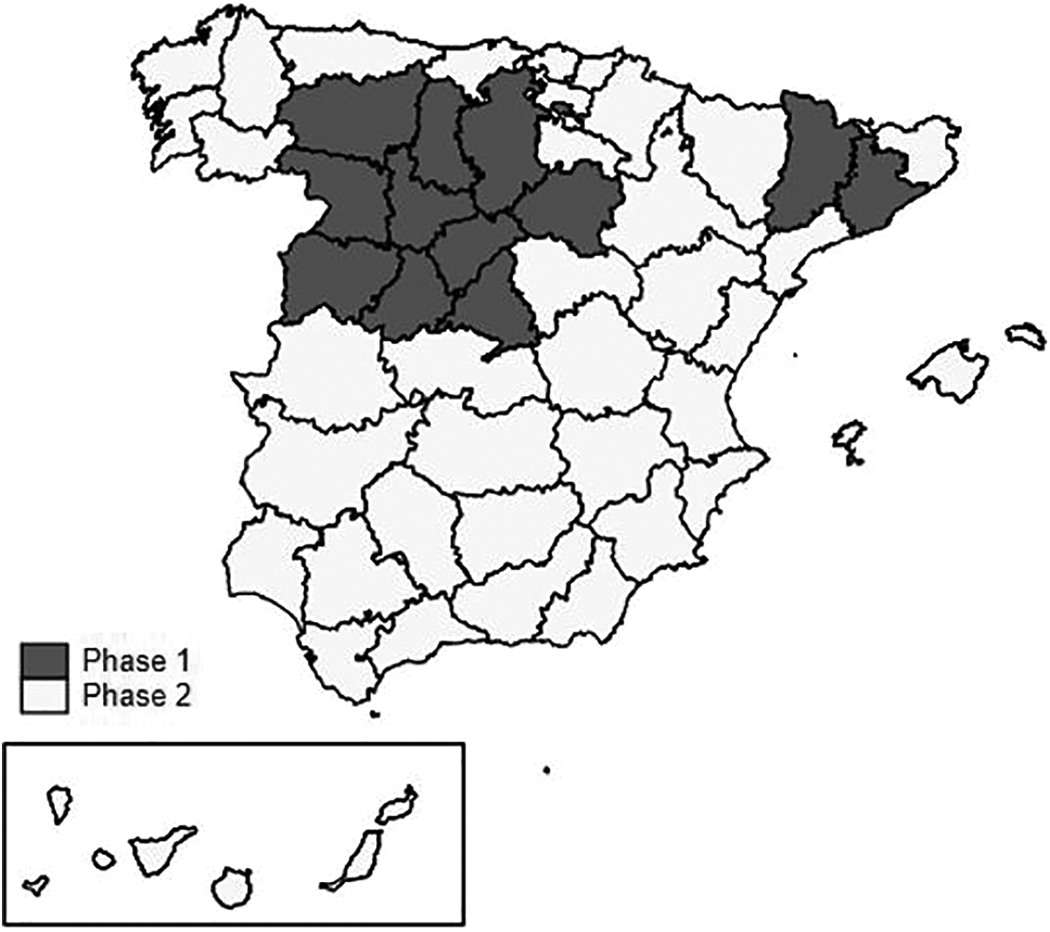
De-escalation phase by province.
Exploratory analysis
As a preliminary test, we compare the share of people that planned to go on holidays in the summer of 2020 with their province’s de-escalation phase. Similarly, we compare respondents’ travel intentions based on having had COVID-19 symptoms or not. Table 2 presents t-tests of the mean equality together with the sizes of the different subsamples. Interestingly, the share of people who plans to go on holidays is significantly greater among those at phase 1 at the time of the survey and among those who suffered COVID-19 symptoms. Therefore, those with more COVID-19 exposure were more likely to plan to go on holidays during the summer of 2020 relative to those with less exposure. This also applies when we compare the share of travel intentions between those who declared COVID-19 to be Spain’s primary problem with those who reported that other problems were more important. The differences are statistically significant in all three cases.
Travel intentions based on COVID-19 exposure and concern.
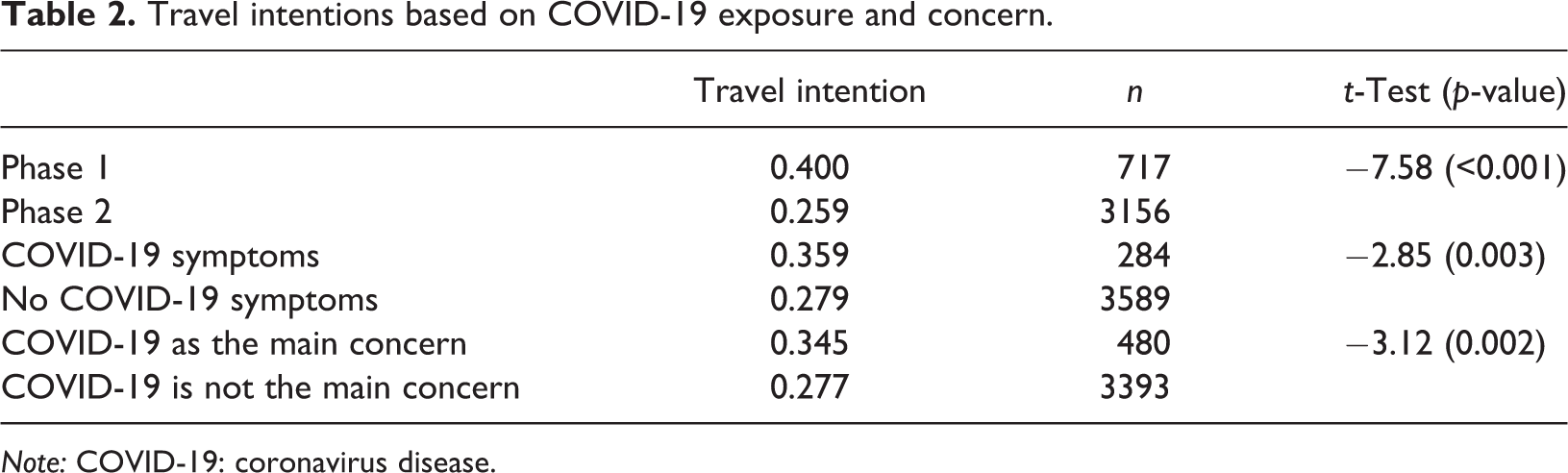
Note: COVID-19: coronavirus disease.
We should be cautious when interpreting these results since the differences in the means could partially reflect differences in the subsamples’ characteristics. Therefore, to ensure a more robust examination of the links between exposure to COVID-19 and travel intention, we perform a formal econometric analysis.
Methodology
As mentioned above, we aim to determine the effect of COVID-19 exposures at two levels: zonal and individual. Concerning the first level, the asymmetric de-escalation process among regions provides a natural experiment that allows us to analyze whether vacation plans, ceteris paribus, differ depending on the respondents’ de-escalation phase. Similarly, having suffered symptoms compatible with COVID-19 can be seen as an exogenous treatment that may have a causal impact on travel intentions.
Regression analysis
We initially propose the following linear probability model (LPM)

where α is a constant term; β and γ measure the effect of zonal and individual exposures, respectively; Xi is a vector of control variables; and
To control for other factors influencing the decision to go on holiday, Xi includes the following individual characteristics: gender (female), age, economic situation, household size, municipality size, educational level (vocational training and high education), civil status (married), labor situation (employed and unemployed), political ideology, religious beliefs (Catholic and other religion), and social class (upper class, upper middle class, and middle class). The standard errors are clustered at the province level to rule out potential confounding effects arising from correlation between units pertaining to the same regional area (Cameron and Miller, 2015).
The econometric evaluation of causal treatment effects in observational studies poses three main challenges. The first concerns the relationship between the potential outcome and the treatment since, in contrast to a randomized experiment, we cannot assume complete independence between them. The second refers to the so-called “overlapping” issue, which describes the possible heterogeneity between treated and untreated individuals; such heterogeneity makes the comparison (and hence the estimation of causal effects) unsuitable. Finally, the third relates to the fundamental problem of causal inference: a treatment’s impact on the outcome involves speculation about how the same individual would have performed if she had not received the treatment. To address these caveats, apart from standard regression analysis, we opt for PSM and a novel regression framework for treatment heterogeneity recently developed by Sloczynski (2020).
Propensity score matching
Adopting the Rubin potential outcomes notation (Rubin, 1974), for each unit i, for

Assuming that symptoms are exogenously given, the ATE of COVID-19 symptoms

where
The identification of treatment effects requires the assumption that the treatment assignment is randomly distributed across the sample. However, there could be selection bias so that the treatment likelihood depends on the characteristics of the respondents. For instance, elderly people could be more likely to suffer COVID-19 symptoms or those living in densely populated areas could be more likely to remain at phase 1. Although we control for these observables in the regression in equation (1), it could be the case that the ceteris paribus condition does not properly apply because of the reduced sample size of the treated units. Therefore, we assume conditional independence (i.e. selection on the observables) as follows


To better estimate treatment effects, we explore the potential dependence between the treatments and the outcome based on observable characteristics using PSM. Intuitively, we match treated and untreated individuals with the same characteristics (Xi) so that the latter act as counterfactuals for the former. In this way, PSM mimics randomized experiments using observational data (Rosenbaum and Rubin, 1983). We refer the reader to Imbens (2004) for an extensive review of the topic.
PSM proceeds in two steps. The first involves computing the scores (i.e. the probability of receiving the treatment conditioned on some covariates, denoted by p (X)). Subsequently, individuals are matched according to the similarity of their scores. For the first step, we run a Probit model. In the case of COVID-19 symptoms, we condition on all the variables included in X; for phase 1, we condition only on a subsample of covariates to ensure sufficient overlap. In the second step, we use two matching algorithms: (i) radius matching (Dehejia and Wahba, 2002) and (ii) kernel matching (Heckman et al., 1998). The radius matching algorithm matches the treated units only with controls whose propensity score falls within a predefined neighborhood. By contrast, the kernel matching algorithm matches the treated units with all the untreated units but assigns a lower weight to those whose scores keep away from those for the treated.
Importantly, it is necessary to restrict the algorithm’s potential matches to the common support. This means that, apart from having similar propensity scores, treated and untreated individuals must have enough overlap in their characteristics to make the comparison meaningful. Accordingly, after computing the scores, we apply the balance test (Imbens, 2004). The test clearly confirms that the mean propensity score is equivalent in the treated and untreated groups (available upon request).
Heterogeneous treatment effects
One important problem in policy evaluation is that only one outcome is observed for each individual. Regarding the impact of the de-escalation phase on travel intentions, doubts arise about whether the specific characteristics of the treated regions (e.g. size, wealth, degree of urbanization, political trust, and climate conditions) could play a role. Would the treatment effect be the same if the provinces at phase 2 were in phase 1 and vice versa? If so, our analysis could be biased. Furthermore, the estimates could be affected by a composition effect. The share of respondents in phase 1 (0.186) is notably lower than the share in phase 2 (0.814). 7 The regression coefficient β in equation (1) is a valid approximation of the treatment effect under randomization only if the treated and untreated groups are of similar size.
In light of the above, we also explore whether the treatment effect of movement restrictions on the travel intentions of those living in the treated provinces (ATT) differs from the counterfactual treatment effect for individuals living in the untreated provinces (ATU). In other words, we examine potential treatment heterogeneity for the de-escalation phase.
Sloczynski (2020) shows that under some conditions, the ordinary least squares (OLS) regression coefficient (β) derived from equation (1) is a convex combination of ATT and ATU, as the weights are inversely related to the proportion of observations in each group. Accordingly, the estimate converges to the ATT when few units are treated and to the ATU when most of the units are treated. In the case of phase 1, we have the following

where
Under treatment heterogeneity, the OLS coefficient could be biased. Sloczynski (2020) proves that the true ATE can be computed as follows
Results
Regression analysis
Table 3 presents the coefficient estimates from equation (1). The first column reports the estimates from an OLS regression. The second and third columns present the estimates and average marginal effects from a Probit model for comparison purposes. The effects are very similar. Hereafter, we will refer to the results from the LPM model because the linearity of phase 1 and COVID-19 symptoms on travel intention is better suited for the analysis that follows.
We find that living in a province at phase 1 increases the likelihood of going on vacation by 7.6 percentage points (hereafter pp), ceteris paribus. This finding holds for different specifications and control variables. 8 Therefore, stricter movement restrictions due to a worse epidemiological situation are associated with a higher intention to travel. We interpret this result as evidence that people who have suffered to a greater extent from the restrictions imposed to contain COVID-19 are more in need of travel. Accordingly, planning a holiday trip might act as a stress reliever that provides an opportunity for relaxation after strain, in line with the findings of Etzion (2003), Fritz and Sonnentag (2006), Chen et al. (2016), de Bloom et al. (2017), and Vidon and Rickly (2018).
Nonetheless, this finding does not preclude the possibility of a lower share of people who plans to go on vacation, compared to the prepandemic situation. That is, we do not infer that people are more willing to travel after the pandemic than they were before, but only that those who have suffered mobility restrictions for a longer period are relatively more likely to travel.
On the other hand, having suffered COVID-19 symptoms is not statistically significant at conventional levels in this setting (only at a 10% significance level). The imprecision in the estimate could be due to the low frequency of this variable in the data. We explore this in more detail later.
In line with Table 2, considering COVID-19 to be the current primary concern is significantly associated with planning to go on holiday (5.6 pp). This finding further supports our prior discussion: the higher the concern (and therefore, the expected anxiety and strain produced by the pandemic), the higher the willingness to go on vacation. Regarding the role of personal characteristics, we find that females are significantly less likely to report holiday travel plans. The opposite holds for married people. Traveling intentions are positively correlated with education level, municipality size, and being employed. This is consistent with previous evidence on the drivers of tourism participation (Alegre et al., 2013; Boto-García, 2020; Eugenio-Martín and Campos-Soria, 2010). Respondents’ self-reported economic situation is another significant predictor of the willingness to travel, possibly through its effects on budget constraints. Interestingly, self-identification as upper class or upper middle class is positively associated with traveling intention. By contrast, age, household size, political ideology, and religious beliefs are not statistically significant.
Coefficient estimates clustered standard errors at the province level in parentheses.
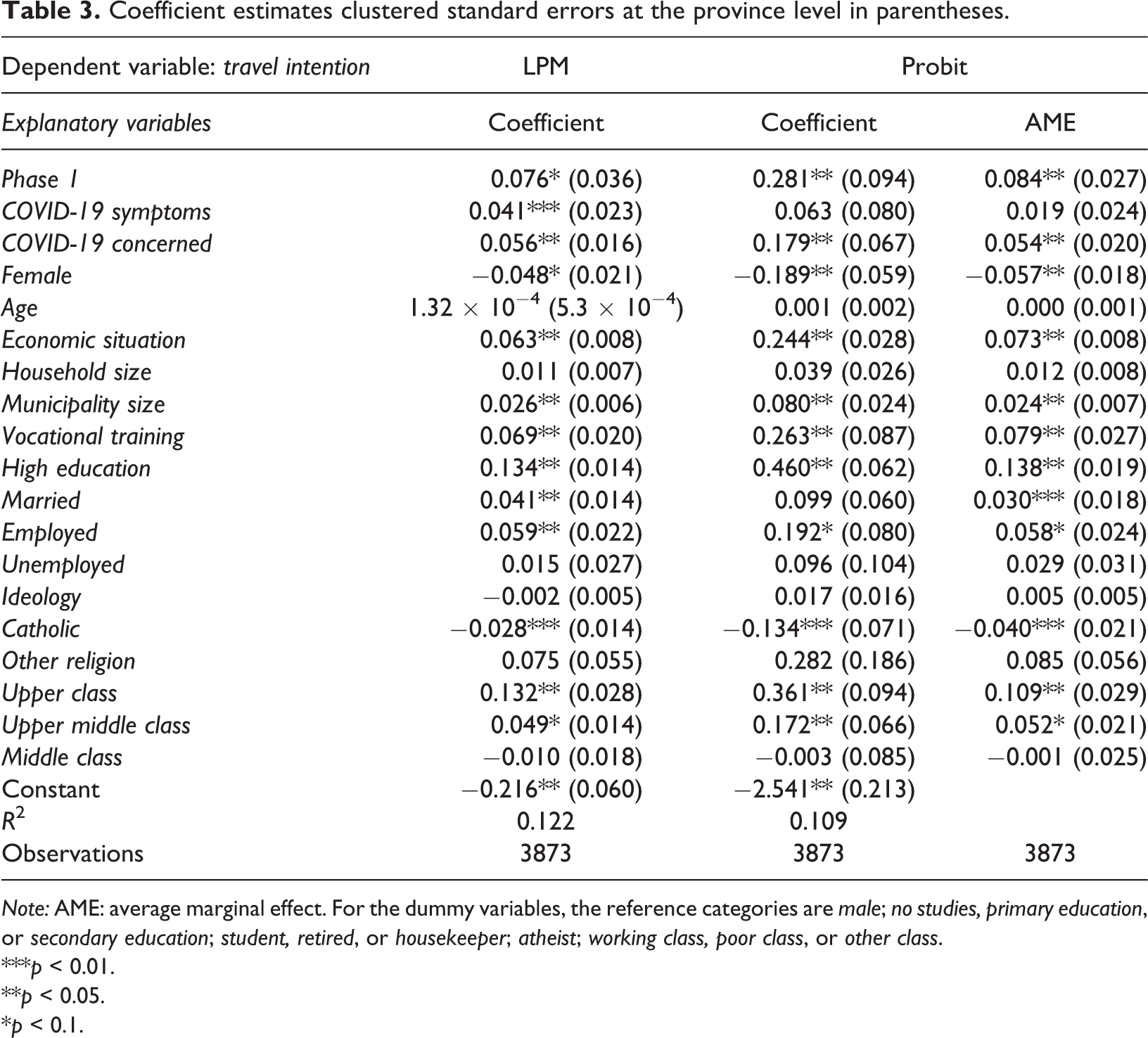
Note: AME: average marginal effect. For the dummy variables, the reference categories are male; no studies, primary education, or secondary education; student, retired, or housekeeper; atheist; working class, poor class, or other class.
***p < 0.01.
**p < 0.05.
*p < 0.1.
Propensity score matching
Table 4 presents the estimates of the average treatment effect on the treated (ATT) of phase 1 and COVID-19 symptoms obtained by applying PSM using the two different matching algorithms. We perform the estimates in Stata 16 using the modules outlined in Becker and Ichino (2002). In line with Table 3, the results indicate that living in an area subject to more severe restrictions (phase 1) increases travel intentions by around 7 pp. This alternative method provides further evidence of the positive causal effect of the de-escalation phase on vacation plans. Interestingly, having had COVID-19 symptoms increases the likelihood of going on vacation by around 8 pp. Contrary to the baseline regression analysis in Table 3, this effect is statistically significant and is larger than the estimate derived from the regression analysis.
Treatment effects on the treated using propensity score matching.
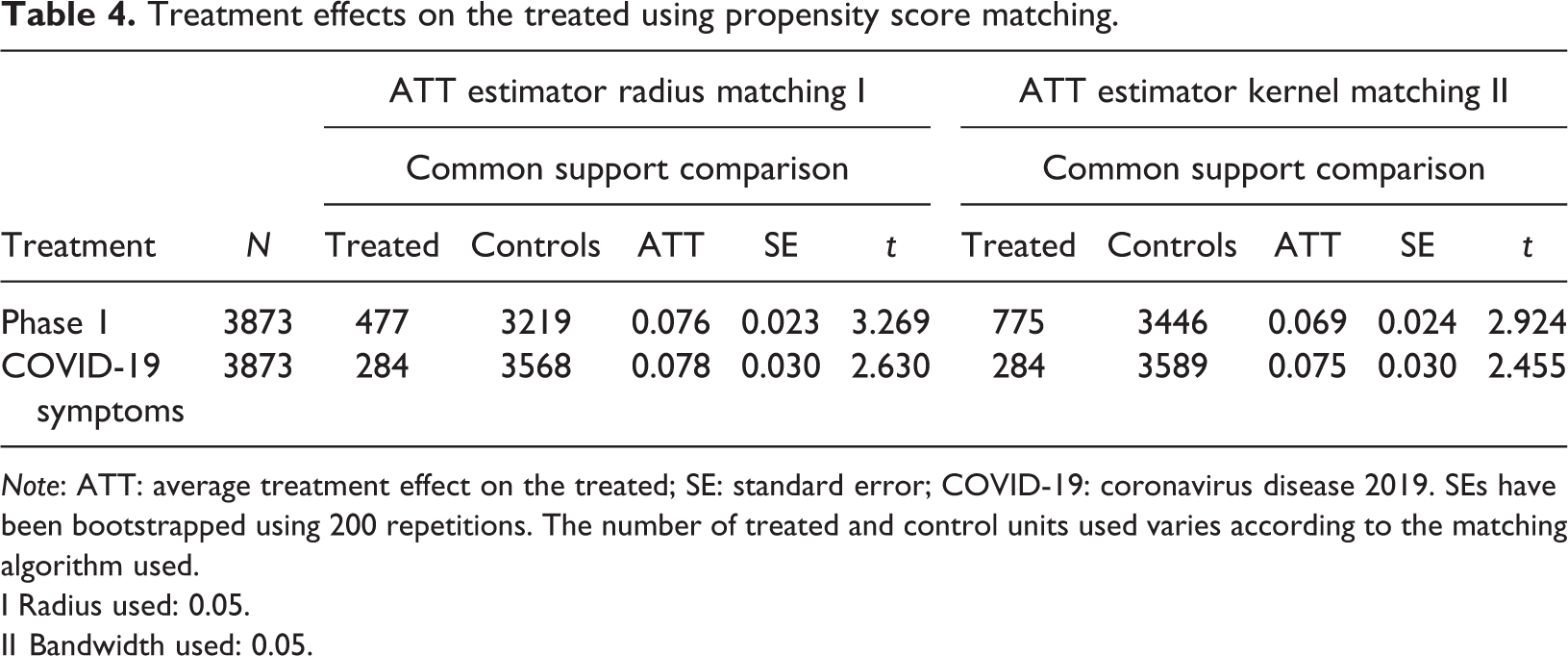
Note: ATT: average treatment effect on the treated; SE: standard error; COVID-19: coronavirus disease 2019. SEs have been bootstrapped using 200 repetitions. The number of treated and control units used varies according to the matching algorithm used.
I Radius used: 0.05.
II Bandwidth used: 0.05.
The differences in the magnitude of the effects across the LPM and the PSM method mainly reflect two factors. First, the two methodologies, athough similar, differ in how they compare treated and untreated units. Second, there is a technical difference between the ATE derived from the linear regression and the ATT units obtained from the PSM method; the latter measures the effect the treatment has on the actual treated units. These differences are discussed further in the following subsection.
Heterogeneous treatment effects
Table 5 presents the decomposition of the treatment effect following Sloczynski (2020). The estimates are derived after 1000 bootstrap repetitions. While the estimate of ATT is 8.5 pp, the ATU is estimated to be 5.7 pp. The OLS estimate (7.6 pp) is closer to 8.5 because of the lower proportion of treated units in the sample. Therefore, the OLS coefficient in Table 2 seems to overestimate the effect of the de-escalation phase on travel intentions. Specifically, the ATE is 6.2 pp. In other words, the effect of being in phase 1 appears to be slightly greater than it would have been had the provinces in phases 1 and 2 been reversed.
Treatment effect decomposition following Sloczynski (2020).
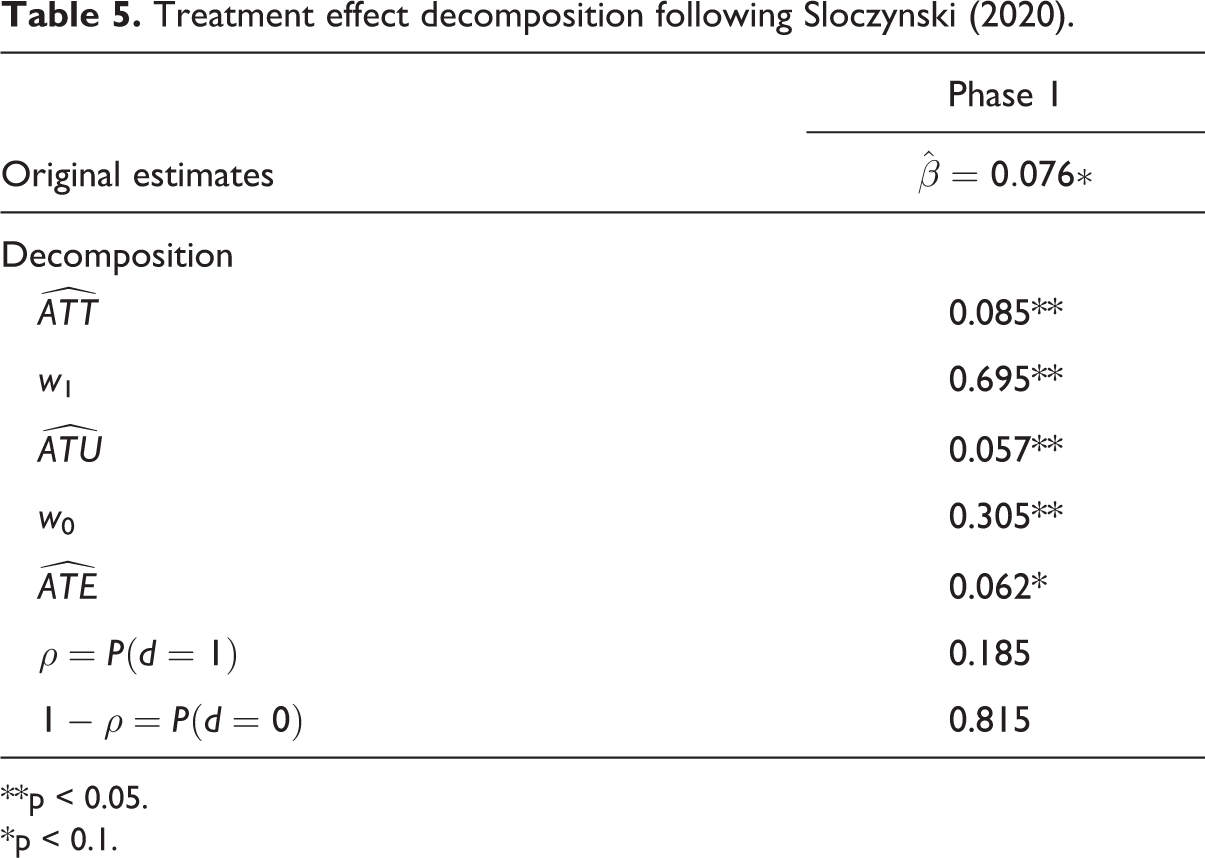
**p < 0.05.
*p < 0.1.
Conclusions
Summary of findings
This article analyzes how people’s travel intentions for the summer of 2020 were affected by exposure to COVID-19. We examine two types of exposure: (i) zonal exposure (the degree of movement restrictions in force in an individual’s province of residence) and (ii) individual exposure (an individual’s experience of COVID-19 symptoms). We use survey data for Spain, a country with some of the highest COVID-19 infection and mortality rates in the world, which underwent a severe lockdown for almost 2 months.
Standard regression analysis and PSM consistently show greater travel intention among those who have been more exposed to COVID-19, either personally or at the zonal level. Our results are in line with existing evidence in the tourism and psychology literature that shows that traveling enhances people’s well-being through emotional and hedonic components. Our findings suggest that tourism traveling can act as a stress reliever that helps people recover from bad events. As such, our estimates suggest that the positive emotions of sensation seeking and excitement produced by tourism can outweigh the potential risk of contagion associated with travel for some people. Concerning potential treatment heterogeneity, Sloczynski’s estimator shows that the effect of movement restrictions would be smaller if they were applied in the nontreated provinces, suggesting that the role of policy interventions tends to interrelate with specific regional characteristics.
Our analysis considers both treatment selection in observables and a set of sociodemographic characteristics as control variables. We find a greater willingness to go on vacation in the summer of 2020 among males, those who are highly concerned about the pandemic, and employed individuals. Furthermore, travel intentions are positively related to the size of the municipality of residence, education level, and perceived social class.
Practical and policy implications
This study contributes in several ways to the academic literature on health crises and tourism participation. From a practical standpoint, the article provides timely empirical evidence on the effect of exposure to COVID-19 on consumers’ willingness to travel. Despite the expected overall fall in tourism demand due to movement restrictions between countries and the reduction of disposable income, the people most exposed to COVID-19 exhibit a positive attitude toward traveling. This finding sends a positive message to the whole tourism ecosystem since it suggests that, given compliance with health and security protocols, traveling can act as an anxiety reliever. Since travel proves to be a basic need, tourism providers and public authorities should design tailor-made products to satisfy the need to travel while ensuring safety within so-called “untact tourism” (Bae and Chang, 2020). Our findings could help tourism organizations develop communication strategies that stress the benefits of traveling after COVID-19 while highlighting the necessity of complying with health protocols.
Limitations and future research
This study is not without limitations. First, the cross-sectional nature of the dataset does not allow us to assess the dynamics of the willingness to travel throughout the lockdown period. If this survey structure persists, it would be interesting to make a longitudinal comparison of people’s travel intentions as the pandemic evolves. Similarly, we lack comparable data on travel plans for the summer of 2019. As such, the fact that those who have been more exposed to the disease are relatively more willing to travel does not exclude the possibility of a decrease in the share of people who plans to go on vacation. Future research should extend our study by quantifying the expected drop in tourism demand caused by the health crisis compared to pre-COVID-19 levels. Third, the article investigates the willingness to travel rather than actual travel behavior. Future studies should examine whether the pandemic has affected the actual decision to travel. Relatedly, future research should also explore whether the pandemic has changed travel habits in terms of the choice of destination, accommodation, and mode of transport.
Supplemental material
Supplemental Material, sj-pdf-1-teu-10.1177_1354816621996554 - Exposure to COVID-19 and travel intentions: Evidence from Spain
Supplemental Material, sj-pdf-1-teu-10.1177_1354816621996554 for Exposure to COVID-19 and travel intentions: Evidence from Spain by David Boto-García and Veronica Leoni in Tourism Economics
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.