
Abstract
Objectives:
Health care reforms often include provider diversification, including privatization, to increase competition and thereby health care quality and efficiency. Donabedian's organizational theory implies that the consequences will vary according to the providers' ownership. The aim was to examine how far that theory applies to changes in English NHS primary medical care (general practice) since 1998, and the consequences for patterns of service provision.
Methods:
Framework analysis whose categories and structure reflected Donabedian's theory and its implications, populated with data from a systematic review, administrative sources and press rapportage.
Results:
Two patterns of provider diversification occurred: 'native' diversification among existing providers and plural provision as providers with different types of ownership were introduced. Native diversification occurred through: extensive recruitment of salaried GPs; extending the range of services provided by general practices; introducing limited liability partnerships; establishing GPs with special clinical interests; and introducing a wider range of services for GPs to refer to. All of these had little apparent effect on competition between general practices. Plural provision involved: increased primary care provision by corporations; introducing GP-owned firms; establishing social enterprises (initially mostly out-of-hours cooperatives); and Primary Care Trusts taking over general practices. Plural provision was on a smaller scale than native diversification and appeared to go into reverse in 2011.
Conclusions:
Although the available data confirm the implications of Donabedian's theory, there are exceptions. Native diversification and plural provision policies differ in their implications for service development.
Keywords
Introduction
Of the theories which might implicitly underlie provider diversification policy, the most coherent, and one which provides an integrating framework for certain other narrower organizational theories (e.g. resource dependency theory gap, contingency theory), seems to be the one linking providers’ organizational structures, work processes and outcomes. 1 It assumes that an organization’s formal structure determines who the organization is accountable to and has authority to direct it; hence, whose goals and interests the organization pursues, and what goals. Ownership gives, indeed is, the power to decide these matters, including the power to delegate or sell these powers themselves. Since an organization adopts innovations compatible with its ‘values’, its goals determine its choice of the production processes which create its outputs and determine their quality, e.g. whether for-profit providers aim so strongly at minimizing costs as to engender ‘quality shirking’. 2 Many nuances qualify this schema. External capitalization or joint venture status complicates organizations’ ownership. Negotiations among stakeholders (e.g. professions) may modify organizational goals. Existing technologies and external resource dependencies (e.g. contracts with purchasers) constrain the choice of production process. Technical competence and resources determine how closely an organization’s outputs match its aims, have unforeseen side-effects and, in health care, impact upon health outcomes. Nevertheless, structure-process-outcome (S-P-O) theory implies that different ownership is a basis for explaining why health care providers develop distinct organizational structures, work processes and patterns of service provision, quality and costs.
It also implies a distinction between two different concepts of provider diversification: native diversification within a closed set of existing providers; and plural provision, introducing differently owned providers from outside the existing set. S-P-O theory predicts that the corresponding two policies will have different consequences for the development of provider competition, for the range of services offered, to whom (with equity implications) and at what quality and cost. Studies of the English National Health Service (NHS) mainly describe native diversification and its consequences, studies of the USA and Bismarckian systems those of plural provision.
Native diversification
Under native diversification, providers develop more elaborate organizational structures, strengthen their performance management, cost accounting and marketing, and develop a more entrepreneurial organizational culture. They develop and differentiate their services at the margins rather than altering their established core working practices and power relationships. Professional partnerships adopt hybrid organizational structures combining partners’ ownership and control with corporate-style support structures and managerial practices. 3
During 1997–2007, a period of simultaneous native diversification and plural provision, hospital waiting times for NHS patients fell without less equitable access. 4 Before 2002, some NHS hospitals did somewhat differentiate their prices but the introduction of uniform hospital tariffs ended this opportunity to observe how much price differentiation might eventually result. (The same applies to Germany.) During 1991–1998, competition between NHS providers had, with a few exceptions, little effect on service quality 5 but after 2004, non-price competition appeared to raise quality of care for certain groups (e.g. acute myocardial infarction in-patients). 6 Most such studies attribute these effects to competition (meaning reduced market concentration) without reporting what mechanisms, whether native diversification or other managerial changes within providers, produced them. Indeed, NHS hospitals often tacitly agree a division of labour with other nearby providers: not competition but collaboration bordering on collusion.
Native diversification depends upon existing providers having sufficient latitude and motivation to exploit the policy. Otherwise, a government intent upon introducing competition has to adopt a policy of provider pluralism, whether to demonstrate resolve in making existing providers contestable (‘to continue to lever change in the NHS’ 7 ) or to launch wide-scale privatization.
Pluralism
If ownership determines organizational goals and work processes, ownership differences between new providers are as important for the aforementioned consequences as their differences from existing providers. Corporations with shareholders typically aim to maximize shareholder value (dividends, share price) and consequently their market share. Clinician-owned partnerships typically aim to satisfy their owners’ income and professional interests in the range and quality of services provided, and sustain collegial working. 8 Co-operatives, charities and other not-for-profit organizations typically pursue normative policy or local objectives, such as supplying services that would not otherwise be available. They have to break even financially. Assuming that common regulations, professional norms, evidence-based medicine and purchaser requirements do not restrict the scope for provider differentiation too narrowly, 9 S-P-O theory implies that quality and costs will vary more than under native diversification. Models of care and ways of organizing providers’ work will appear that did not, indeed could not, develop under native diversification.
Empirical comparisons of for-profit and not-for-profit providers suggest somewhat different patterns of service development, although few studies distinguish ‘social enterprises’ (Community Interest Companies in England), professional and/or patient cooperatives (e.g. Group Health, USA), charities and other NGO or ‘third sector’ forms of ownership among not-for-profit providers. Analysis of American Hospital Association data for 1988–2000 10 found that for-profit organizations tended to offer relatively profitable services (e.g. diagnostic imaging, orthopaedics), public hospitals the opposite (e.g. emergency departments, burns services), with not-for-profit organizations often in between. The latter provided more care to uninsured patients. 11 In England, though, accusations that treatment centres (corporate providers of planned diagnostics and in-patient treatment, under contract to the NHS) ‘cherry-pick’ their cases appear unsubstantiated. 12
A systematic review 13 about US dialysis services found that for-profit had slightly (relative risk 1.02) higher mortality than not-for-profit providers. A review of studies with disparate quality indicators 11 found more favouring not-for-profit provision. Another 14 showed higher quality care in terms of staffing and pressure ulcer prevalence in not-for-profit nursing homes. In England, though, outcomes for cataract extraction, groin hernia repair, hip replacement, knee replacement and varicose vein surgery appear similar in treatment centres (corporate providers contracted to the NHS) and NHS hospitals.12,15 The Healthcare Commission (which until 2009 monitored the quality of NHS care) reported that patients rated their experience of care higher in treatment centres.
On balance, not-for-profit providers in North America charge lower prices than for-profits.11,16 US data for 1986–1994 suggested that all hospitals raised prices after mergers, but for-profit hospitals did so the most. Prices and administrative costs were higher in for-profit than not-for-profit and public hospitals, apparently because for-profit hospitals prioritized income maximization. 17 A systematic review 18 of studies comparing Canada and USA found few differences in one- and six-month mortality but higher prices in the USA, implying lower efficiency in the more corporately dominated system. Medical pay, lengths of stay and production costs (as opposed to prices to purchasers) were however lower in for-profit hospitals. 19 During 1980–2000, though, US for-profit and not-for-profit hospitals converged in terms of costs, 9 size, occupancy, case-mix and lengths of stay. The effects of ownership also depended on the degree of market concentration and, possibly, the presence of common purchasers and regulations.
Under plural provision, competition among German and US hospitals appeared to cause market concentration as losing competitors closed or merged (and similarly when commissioners compete, as in Germany and the Netherlands). Once consolidated, structures are difficult to unbundle. 20 Providers with large market shares set pricing and quality patterns for the health system as a whole. 11 Over 40% of US hospitals, predominantly not-for-profit ones, participated in mergers, acquisitions, joint ventures or partnerships during 1994–1996 alone. Not-for-profit hospitals took to imitating corporate pricing, managerial and merger strategies. Some converted to corporate status. However, increased market concentration and, therefore, treatment volumes per hospital have contributed to declining mortality for some high-risk cancer operations. Declines in mortality for other procedures are attributed to other factors. 21
The foregoing suggests three possible consequences of plural provision. When corporations find health care unprofitable and not-for-profit providers cannot break even, only native diversification can occur. Alternatively, corporations expecting profits may try to take market share from existing providers. However, the most likely scenario is that corporations provide the profitable services and not-for-profit organizations provide the rest. Overall, since the 1980s studies of plural provision have moved from finding little difference between for-profit and not-for-profit hospitals and nursing homes towards reporting specific implications of these ownership differences.
Objectives
This evidence gives reason to wonder whether plural provision of English NHS primary health care may have similar implications, raising questions as to what existing research shows regarding: the extent of native diversification and provider pluralism in NHS primary medical care since 2002; and the consequences for the range of services, their quality and cost. Compared with hospital services, there are few studies of provider diversification in primary care and, for the English NHS, no recent overview. Because many health systems follow similar policies, these questions are relevant beyond England.
Just counting providers or using, say, the Herfindahl-Hirschman Index cannot differentiate native diversification from plural provision. Qualitative criteria are required, respectively: existing providers develop more diverse roles and organizational structures; and providers with different kinds of legal personalities to existing providers enter the health system. Either change must be extensive enough to make old style providers contestable. So for hospitals the Department of Health eventually mandated one independent sector treatment centre per Primary Care Trust (PCT, which until 2012 commissioned hospital and community health services, and monitored general practice quality). An equivalent scale of plural primary care provision would be one corporate, co-operative or other non-partnership provider of mainstream primary medical care per PCT. For native diversification, the equivalent would be one GP partnership per PCT providing a different range of services or division of clinical labour than was previously standard.
Methods
To address these questions a framework analysis was used, whose categories and structure reflected the above theory, its implications and distinctions. It was populated with data from a systematic review, administrative sources and press rapportage.
Studies for this paper were initially selected from those found by a wider-ranging systematic review. Full details of the search and selection strategies are reported elsewhere. 8 Briefly, an initial scoping study of papers known to be relevant and their references was made to identify and select keywords. The keywords were used to search Medline, PubMed and Cinahl, ABI-Inform, Scopus and Web of Knowledge, yielding 2194 abstracts. Screening and selection began by independently coding a maximum-variety sample of 24 abstracts against headings reflecting S-P-O concepts and relationships, thereby testing coding reliability and, as necessary, consensually re-writing ambiguous coding criteria more specifically. Of the remaining abstracts, only 15% satisfied the first inclusion criterion, of reporting empirical studies (the rest were mainly a priori economic models or other normative pieces). Of the empirical studies, 69 satisfied the second inclusion criterion, relevance to at least one S-P-O category in an English primary care context since 1998.
Data were extracted from full text copies of these papers into a structured form whose headings matched S-P-O categories and sub-categories. Supplementary and more recent data were found by hand-searching Department of Health and NHS Information Centre websites for ‘grey’ publications and administrative data, and from professional press reports (e.g. Pulse, Medeconomics), tracing reports which had such origins back to their peer-reviewed sources. Relevant peer-reviewed journals (e.g. JHSRP, BMJ) appearing since the database searches were also hand-searched. The additional data were coded and extracted as described above.
The forms were then collated into one document of similar structure, providing an analytic framework. It collated the empirically reported links between provider ownership, other organizational structures, service delivery patterns (productive ‘process’) and, less often, service outputs and health outcomes. Showing these relationships required arranging the data chronologically, including time series (where available) of quantitative administrative data. This method of integration also exposed any disagreements, ambiguities or gaps among the selected studies. Patterns found across the populated framework revealed the character of native diversification and plural provision and, where reported, the consequences for work processes, service outputs and health outcomes. These patterns were then compared with the secondary literature noted above.
Results
Native diversification
Native diversification began from general practices. In 2002, 69% of them were professional partnerships co-owned by several GPs (mode: 4–5 GPs), typically but not always in equal shares. Single-handed GPs owned the remainder. Both types employed practice nurses, receptionists and occasionally other staff (e.g. physiotherapists, psychologists).
Under the 1998 Primary Care Act, Personal Medical Service (PMS) contracts permitted non-doctors to become partners in general practices (e.g. a pharmacist, nurse or manager joining several doctors). 8 Nurses (and theoretically other professionals) could now form partnerships, employing salaried GPs as necessary. Then non-doctors became the patient’s first point of NHS contact and gatekeeper to primary care doctors. There were probably fewer than 50 such practices, although still enough to be proof of concept. The provider signatory to a PMS contract was a general practice, not a named GP as before. A practice could therefore change its medical staff and ownership without necessarily jeopardising its NHS contract. In 2004, the new General Medical Services (NGMS) contract extended that arrangement to most other practices.
Distribution of general practice contract types, England 2001–2012.
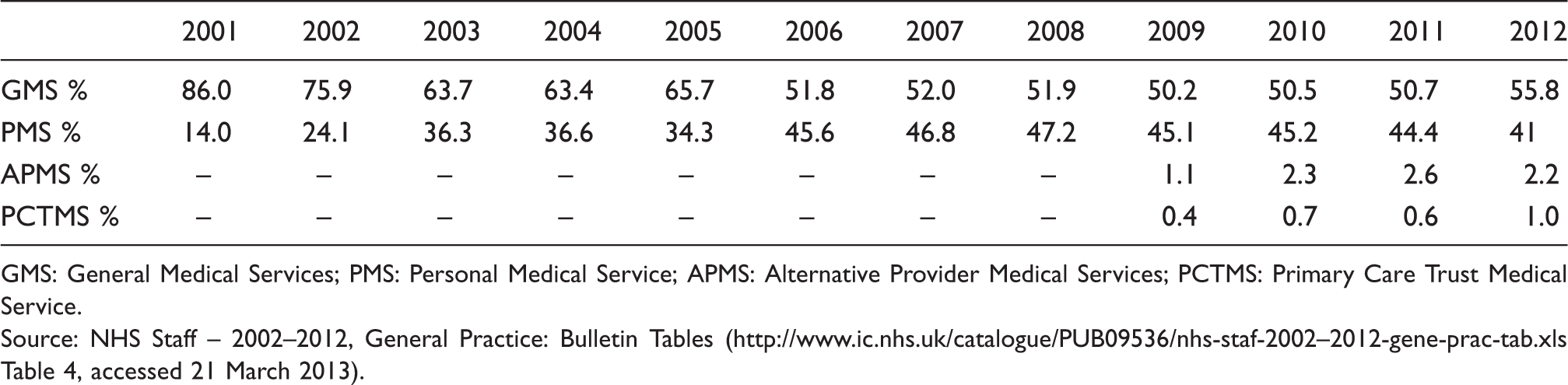
GMS: General Medical Services; PMS: Personal Medical Service; APMS: Alternative Provider Medical Services; PCTMS: Primary Care Trust Medical Service.
Source: NHS Staff – 2002–2012, General Practice: Bulletin Tables (http://www.ic.nhs.uk/catalogue/PUB09536/nhs-staf-2002–2012-gene-prac-tab.xls Table 4, accessed 21 March 2013).
Even among partner GPs, changes in GPs’ contracts made some lead GPs ‘chasers’ and other partners the ‘chased’ in pursuit of the new contract targets. 24 Non-medical staff numbers per GP remained stable at around 2.4 whole time equivalents but the composition shifted from administrative towards ‘direct patient care’ staff, the latter (which excludes nurses) rising from 3.2% to 8.7% of practice staff, including in some cases receptionists trained to do phlebotomy. 8 Nurses were increasingly employed to implement parts of the National Service Frameworks and other quality guidelines. Nevertheless, practice management required increasing effort, partly because mean practice size continued to increase (from 3.23 to 4.37 GPs between 2001 and 2011; approximately 49% of GPs worked in practices of six or more doctors by 2011). Clinical governance activities and the new contracts increased the requirements of PCTs for data from practices. Distinctions between professional and managerial cultures began to blur. 24
Legislation in 2010 allowed English general practices to become limited liability partnerships, ending the partners’ unlimited liability for each other’s debts. Total conversion figures are apparently not publicly available, although Virgin Care alone absorbed 25 such partnerships. 25 Theoretically, although it is still too early to tell, limited liability should facilitate investment in partnership-owned practices.
New structures also appeared to facilitate coordination between general practices. General practice membership of PCTs was mandatory, resulting in a network form of clinical governance through which lead GPs monitored other general practices’ implementation of nationally recommended quality standards and care pathways. Practice-based commissioning (partially reviving GP fund-holding that existed in the 1980s and 90s) meant that networks of general practices collectively commissioned community health services (as well as secondary care) and redesigned primary care pathways. Many Local Improvement Finance Trust projects (a primary care variant of the private finance initiative) were used to co-locate several general practices in one building, often with community health services, social work and minor surgery provision.
When local demography permitted, general practices expanded their services by replication. Some also developed follow-up services previously delivered by non-medical providers (e.g. pharmacies, health education departments). 8 Sixty-four per cent of the general practices in wave 8 of practice-based commissioning reported commissioning new services, although whether new meant larger volumes from existing providers, new providers of existing services or new kinds of services is unclear. PMS contracts permitted more flexible primary care provision than previously, including services for homeless people, refugees and drug users which would not otherwise be funded. Similarly, the 2004 NGMS contract accommodated three frameworks for commissioning Enhanced Services. Specialized PMS (SPMS) contracts allowed practices to concentrate on such services rather than the full range of primary medical services.
Additional services became available for GPs to refer to. Some GPs became GPs with Special Interests (GPSIs), specialising in particular topics (e.g. mental health) and accepting referrals from other GPs. Nurse-led practices were acceptable to patients but their productivity (e.g. consultation rates) was lower than in general medical practice 26 so the costs per patient were not necessarily lower. In 2003, a US insurer was invited to run pilot projects with nurse practitioners as case managers and some PCTs developed such schemes independently. 27 Without corporate involvement, nurse-led case management was then rolled out nationally as the Community Matron programme. The Improving Access to Psychological Therapies scheme provided assessment and low intensity treatments (e.g. cognitive behaviour therapy) delivered, mostly, by clinical psychologists. There were also fresh attempts to substitute primary for hospital care. Closer to Home schemes aimed to use specially trained practitioners with special interests and community based diagnostic services to help GPs substitute community for hospital care.
A conspicuous change in general practice during this period was closer compliance with quality standards. National Service Frameworks and NICE guidelines were already stimulating this trend before 2004, although more for the management of physical long-term conditions than for mental health. 28 The 2004 NGMS contract tied around 20% of practice income to compliance with the Quality and Outcomes Framework (QOF), resulting in increased activity. A census of salaried GPs found inconclusive evidence that their practices might have slightly higher QOF scores than other practices. 23 Salaried GPs spent less time on practice administration but more working out-of-hours and giving direct patient care, allowing more patients to be seen. They held shorter consultations than partner GPs, prescribed less but made the same number of hospital referrals. 29 However, the increased compliance with quality standards (and consequent increase in GP incomes) seems due to incentive payments and an increased exposure of their clinical practice to NHS managers rather than native diversification. Neither did native diversification obviously stimulate competition between general practices, partly because over-doctored areas remained few and partly because (judging by the professional press) the idea of competition – or perhaps competitors – was often uncongenial to GPs.
Plural provision
Three initiatives enlarged the scope for plural provision of NHS primary care. General practices could be awarded a Alternative Provider Medical Services (APMS) contract supplementing or replacing a GMS or PMS contract, a step often taken for small (mean APMS practice list size of 796 patients per GP versus 1570 for GMS practices in 2011) or hard-to-fill vacant practices. However, APMS contracts were awarded by competitive tendering which were open to third sector and public providers (local government, NHS Trusts), GP-led firms and corporations.
The Fairness in Primary Care Procurement programme provided practical support but no extra funds to help ‘under-doctored’ PCTs use APMS contracts to establish additional general practices. In 2007, a report by Lord Darzi proposed forming polyclinics in London. Following BMA opposition, partly because they feared corporations would be offered the work, the proposal was diluted into one for federated networks of existing general practices with a central hub providing a single point of access to general practice, community health services, walk-in clinics and (in some sites) out-posted hospital diagnostics and consultations. Darzi’s report also triggered the Equitable Access to Primary Medical Care programme which required – and funded – every PCT to let an APMS contract for a new GP-led health centre (‘Darzi-centres’ or ‘Darzi-clinics’) offering bookable and walk-in services to registered and unregistered patients. The 50 PCTs (nearly a third) with the fewest GPs could bid for up to three such health centres. GP partnerships ran most of the new clinics under both programmes but a minority were contracted to GP-owned firms or out-of-hours co-operatives. More widely, APMS supported the development of social enterprises, GP-owned firms and corporations. Alongside these, nationalized providers appeared but not GP-hospital joint enterprises or new, large NHS-owned polyclinics.
PCT Medical Services (PCTMS) contracts enabled PCTs in effect to nationalize vacant general practices. Often this happened when PCTs intervened to take over small practices or practices in difficulties, or when no available GP wanted to become a practice partner or owner when vacancies arose. The staff, GPs included, became salaried PCT employees, the GPs being line-managed by a PCT medical manager. The PCT rented or bought the practice buildings from the former owners. To attract GPs, PCTs managed these practices as if they were professional partnerships, leaving the doctors considerable autonomy. 8
Building upon experiments involving nurse prescribers and nurse practitioners, and imitating corporate examples, the NHS also introduced walk-in clinics (e.g. in railway stations) and a number of GP-run urgent care centres as alternatives to hospital A&E departments and general practices, although some were re-badged existing services. The limited data about them suggest large variation and no uniform improvement in cost and quality over A&E services. 30 Besides providing health advice over the internet and by phone, NHS Direct (subsequently remodelled as NHS111) triaged telephone requests for out-of-hours medical care and in places provided it. These too were NHS-owned services.
From 1990 to 2004, general practices had been responsible for out-of-hours medical cover for their patients. Some sub-contracted to corporate deputising services but most established GP cooperatives. GPs elected a board which employed non-voting staff (telephonists, drivers etc.) for non-medical work and sub-contracted GP members to provide sessional medical cover. The NGMS contract transferred default responsibility for providing out-of-hours services to PCTs, destroying many cooperatives as GPs opted out of out-of-hours work. Against this, some GPs formed organizations (often social enterprises) to screen hospital referrals, partly taking over GPs’ gatekeeper role, and supplying other commissioning support services. From 2009, some PCTs tried to induce their community health services staff to exercise their right to request that their service be converted into a social enterprise. A few (e.g. Central Surrey Health) succeeded but because NHS staff and GPs feared losing their NHS Pension Scheme membership, there was little incentive. 8 By 2009, other smaller social enterprises were running at least four general practices and six other clinics but their role in mainstream primary medical care was tiny.
Provision by limited companies originated partly from among GPs themselves. General practices had often set up parallel companies to circumvent regulatory restrictions on owning land, vehicles and pharmacies. An estimated 9% of GP income already came from private work. A few general practices and at least two large out-of-hours co-operatives converted to GP-owned firms. 8 As Clinical Commissioning Groups (CCGs: federations of general practices which took over PCTs’ commissioning functions in 2013) were being established, 36% of the GPs in GCC executive positions and 23% of CCG Board members were reported to have financial interests in for-profit providers, including out-of-hours and other primary medical care providers. 31 Twelve percent of GPs in CCG executive positions had links with voluntary or not-for-profit providers. Some corporations (e.g. Virgin Health, which later ceased doing so; Assura) and GP-owned firms formed joint ventures with general practices and/or out-of-hours co-operatives.
Percentage of general practice contracts placed with limited company providers, England 2009–2012.
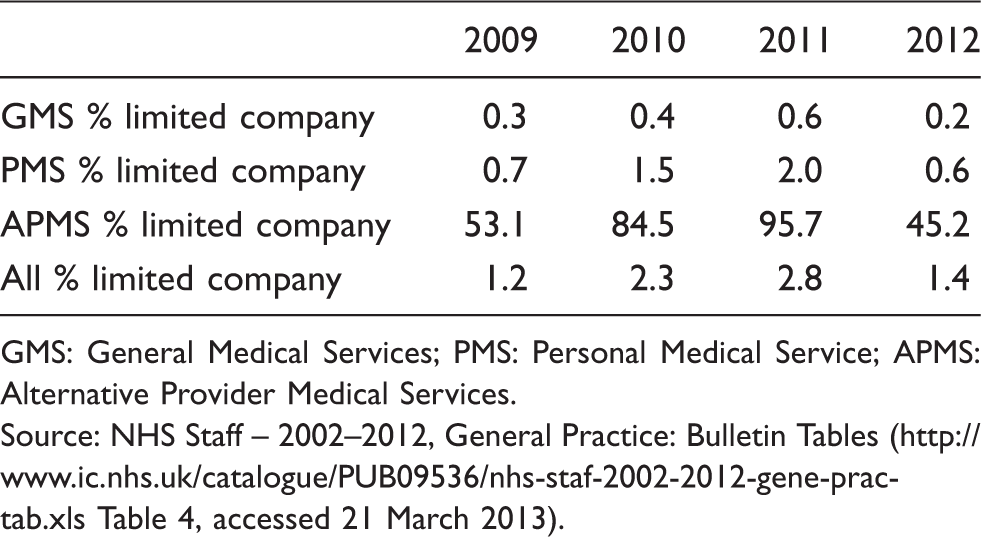
GMS: General Medical Services; PMS: Personal Medical Service; APMS: Alternative Provider Medical Services.
Source: NHS Staff – 2002–2012, General Practice: Bulletin Tables (http://www.ic.nhs.uk/catalogue/PUB09536/nhs-staf-2002-2012-gene-prac-tab.xls Table 4, accessed 21 March 2013).
Only 10 of the first 113 practices were corporate or run by GP-owned firms. 32 By April 2012, Aston HealthCare ran eight practices, Care UK 13 (and two walk-in centres), Intrahealth 25, The Practice 50 (various kinds of provider) and Harmoni 4 (since taken over by Care UK), as well as others. Two US corporations (UHE and Aetna) also won contracts. Some out-of-hours services were re-contracted to corporations (e.g. 23 Harmoni; one with Serco). Unsuccessful cooperatives argued that large infrastructures and financial reserves let corporations write the necessarily complex bids more easily and use predatory pricing to drive out existing providers. Corporations replied that their bids reflected efficiency and bidding experience. 8 However, limited company contracts halved in number from 2011 to 2012 (Table 2).
As a consequence of more plural provision, the range of primary care services has increased slightly. Cooperatives often supplemented their out-of-hours services, partly to benefit their member-GPs (e.g. locum cover, clinical education) and partly extending medical care (e.g. with walk-in clinics, palliative care). Re-analysing Primary Care Foundation data, though possibly disregarding catchment differences and that private providers often inherited problematic services, Pulse reported in April 2012 that not-for-profit out-of-hours services were cheapest and most likely to be rated good or very good by patients although private firms completed a higher proportion of urgent assessments within 20 min. In 2012, the Care Quality Commission (which now monitors the quality of NHS care) reported failures to meet quality and safety standards, and the National Audit Office investigated data manipulation, in Serco’s out-of-hours service in Cornwall. Evercare’s proprietary case management system was however popular with patients and staff but did not reduce unplanned hospital admissions. Increased case-finding may have outweighed any reduction in admissions for patients already known to the system. 27 Attempts in Derbyshire and London to let general practice contracts to corporations, and later the re-sale of such contracts, aroused public opposition. In June 2011, on the NHS choices website, patients rated general practices run by private firms lower than partnerships, and Darzi-clinics higher than conventional general practices but these were self-selected respondents not necessarily representative. Irrespective of ownership some Darzi-clinics were reportedly paid more per patient than conventional general practices but also provided a wider range of services. Darzi-clinics’ uneven success in recruiting patients led to about one in eight being closed to save costs, including clinics operated by private firms and cooperatives.
Discussion
Extensive native diversification of NHS primary medical care providers led mostly to services expanding and developing at the margins (larger practices, additional services for specific hard-to-reach care groups) rather than changing general practices’ core work processes. The latter seem to have changed more because of QOF incentives and the increased transparency of clinical practice than through provider competition, which native diversification did not stimulate much. Native diversification engendered a stratification among general practitioners.
Plural provision was more limited. Nationalization enabled the provision of services which were either unattractive, for example because of the locality, or hard for professional partnerships to provide (e.g. NHS Direct/111). By 2011, there was on average at least one limited company provider contract per PCT, so although 97% of contracts remained with GP partnerships, plural provision was not negligible. While plural provision intensified provider competition for contracts and stimulated the development of nurse-led case management, its other effects on general practice quality remained unclear. The limited evidence available suggests that its effects on out-of-hours service cost and quality may depend on whether the new providers are for-profit. The emergence of firms owning and/or managing numerous general practices represents increased provider concentration, though only modestly. It is not yet known whether the 2012 decrease in limited company contracts reflects corporate pessimism about the profitability of NHS primary care, disruptive reforms of NHS commissioning or other causes.
So far as they go, these findings about NHS primary medical services tend weakly to support elaborating S-P-O theory with accounts of a contrast between the effects of native diversification (extensive replication; service development and differentiation at the margin) and those of plural provision (larger quality and cost variations; provider concentration). The above evidence also hints at consequent differences in types of service, service quality and (more ambiguously) costs between the services of medical care providers in England based on their ownership. However, this association was only weak and remains under-researched.
Across the wide domain of primary care this paper considers only medicine. It would be worth researching whether NHS dentistry with its similarly organized providers, contracts and provider ownership policies shows any parallels. Neither do the above findings necessarily apply to Scotland, Wales and Northern Ireland, nor health systems in other countries where professional partnerships or single-handed doctors dominate primary care provision. Out-of-Hours co-operatives apart, plural provision of primary care is not long-established in the NHS. Published data still discriminate poorly between NHS-employed and partnership-employed salaried GPs. Freedom of Information requests elicit low response rates, considering their statutory basis.
Confusions between native diversification, plural provision, competition and privatization bedevil policy polemics and academic debate. It is simplistic to equate these four. Native diversification and plural provision may have different consequences. If so, provider ownership is not an irrelevant criterion for health care provider selection.
Footnotes
Acknowledgements
In part this article presents independent research commissioned by the National Institute for Health Research (NIHR) through the Service Delivery and Organisation programme. Jill Schofield, Susan Pickard, Bernard Dowling, Russell Mannion and Susan Child were co-researchers. The views expressed in this publication are those of the author, not necessarily those of the NHS, the NIHR or the Department of Health for England.
Declaration of conflicting interests
The author declares no conflict of interests.