
Abstract
Objectives
To examine the types of choices available to patients in the English NHS when being referred for acute hospital care in the light of the divergence of patient choice policy in the four countries of the UK.
Methods
Case studies of eight local health economies in England, Scotland, Northern Ireland and Wales (two in each country); 125 semi-structured interviews with staff in acute services providers, purchasers and general practitioners (GPs).
Results
GPs and providers in England both had a clear understanding of the choice of provider policy and the right of patients to choose a provider. Other referral choices potentially available to patients in all four countries were date and time of appointment, site and specialist. In practice, the availability of these choices differed between and within countries and was shaped by factors beyond choice policy, such as the number of providers in an area. There were similarities between the four countries in the way choices were offered to patients, namely lack of clarity about the options available, limited discussion of choices between referrers and patients, and tension between offering choice and managing waiting lists.
Conclusions
There are challenges in implementing pro-choice policy in health care systems where it has not traditionally existed. Differences between England and the other countries of the UK were limited in the way choice was offered to patients. A cultural shift is needed to ensure that patients are fully informed by GPs of the choices available to them.
Introduction
Patient choice has multiple meanings, and this is a source of ambiguity. 1 Patient choice can be considered in relation to patient empowerment, which ranges from patient involvement in shared treatment decisions to participation in deliberative processes. 2 Patient choice can also refer to consumer choices within a market or quasi-market, which function to encourage competition between the providers of services. 3 Such choices may vary markedly in their scope and include choice regarding what care patients receive, where they are treated, who they are treated by and when they are seen.
In recent years, patient choice and provider competition have been introduced in many industrialized countries. 4,5 Of particular note is the introduction of patient choice of service provider in Beveridge-type single-payer, tax-financed systems such as England, New Zealand, Italy, Spain and the Nordic countries. 4,6 The success of these policies is dependent on the system changes which make choices available to patients, changes in booking systems, information to support choices and a cultural shift on the part of managers and professionals to facilitate choice. 7 –10
The NHS systems in each of the four jurisdictions of the UK share many similarities, both structural, as reflected in the tax-based funding system, and in policy direction, for instance in a shared emphasis on reducing waiting times. However, the devolution of powers to the Scottish Parliament and the Welsh and Northern Irish Assemblies in 1999 has resulted in four distinct policy trajectories shaping the planning and provision of health care. 11
Patient choice is a high profile policy in the English NHS. This has entailed system wide reform, led by the New Labour Governments of 1997–2010, and continued by the current Conservative-Liberal Democrat coalition government. Choice of appointment time and date was introduced in 2000, 11 followed by the development of ‘choice of provider’, 12 giving patients the chance to ask their general practitioner (GP) to refer them to their preferred acute services provider. Patient choice of provider was introduced in limited form in 2006 when patients were given the choice of five providers, including one from the independent sector, and expanded in 2008 to allow patients needing elective hospital care to choose from any accredited public or independent sector provider in England. This policy has been explicitly linked with the encouragement of competition between providers and has been developed in tandem with Payment by Results, a national tariff under which providers are paid according to the number of procedures they carry out; and an increasing plurality of organizations providing for the NHS, with growing involvement of independent for-profit and not-for-profit providers. 13,14
Whilst patient choice of provider and the development of the choice agenda for individual patients is an ongoing priority in England, 15 choice is not a prominent policy stream in the NHS systems of Scotland, Northern Ireland and Wales. Policy makers in these countries have been disinclined to replicate the English policies by widening the choice of provider, and in particular have rejected the use of the market and competition. 16 Nevertheless, all three systems have promoted policies of service improvement and responsiveness 17 and this has meant that certain de facto opportunities for individual choice have emerged. All three countries have encouraged providers to introduce booking systems which inter alia allow patients some choice over the time and date of their first outpatient appointment. 18 –20 Furthermore, all three countries have made the offer of treatment at an alternative provider for patients exceeding treatment waiting times. 21 –23
Our aim was to take advantage of policy differences between jurisdictions to compare patients’ choices when referred to providers. This allows an examination of the changes that have resulted from explicitly pro-choice policy in England. It focuses on choice of hospital, choice of practitioner and choice of appointment time. No attempt is made to discuss shared decision making or choices about treatment, although these are also important policy themes. The data reported relate to one element of a study of the construction and implementation of patient choice in the four countries of the UK. 24
Methods
The fieldwork was conducted between April 2008 and September 2009. The study focused on two sites in each country, consisting of local providers of acute hospital services, the purchasers of these services and the individuals responsible for making referrals to acute services. At each site, general practices were selected: two per site in England; and one per site in Northern Ireland, Scotland and Wales. The study focused on two high-volume surgical specialties, Ear Nose and Throat (ENT) and Orthopaedics.
Numbers of interviewees by country, organisation and role.
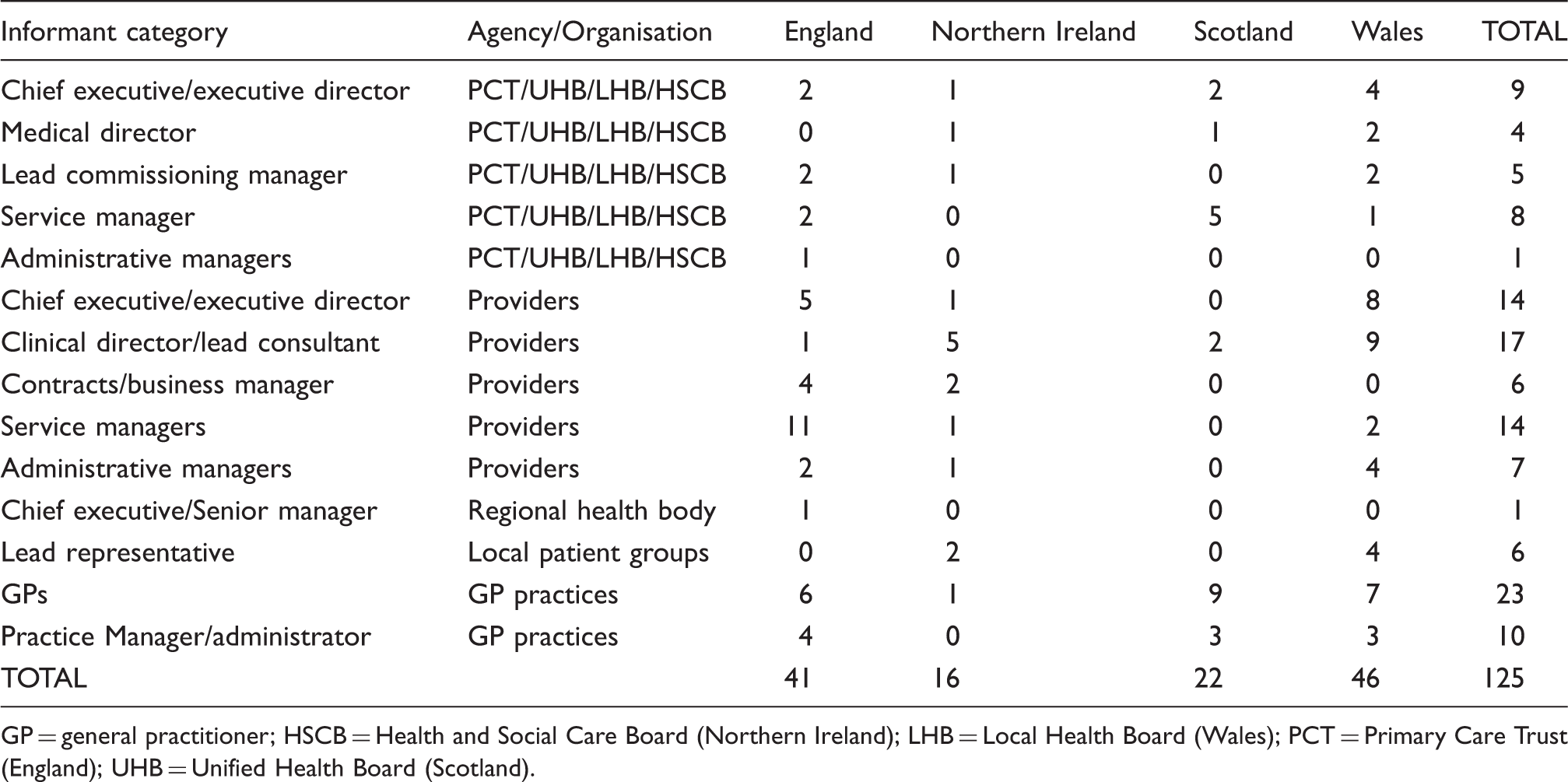
GP = general practitioner; HSCB = Health and Social Care Board (Northern Ireland); LHB = Local Health Board (Wales); PCT = Primary Care Trust (England); UHB = Unified Health Board (Scotland).
Most interviews were conducted face-to-face at the interviewee’s place of work with the rest conducted by telephone. The interviews used a semi-structured guide which is available. 24
The topic guide was developed from the research questions to identify organizations’ responsibilities for patient choice, their understanding of the choices which existed in the referral pathway, the systems in place to deliver these choices and the impact that referral choices were perceived to have on the organisation and the delivery of health services. Each interview was partially transcribed into a pre-agreed checklist of subject areas, based upon the topic guide. One interview from each country was transcribed and read by at least two team members, together with an accompanying partially transcribed summary in order to compare inter-rater reliability. Discordant interpretations were discussed between raters with the aim of resolving differences and agreeing a protocol for subsequent analysis. This resulted in a refinement of the categories to be included in the data summary, and an agreement to probe interviewees more deeply about the mechanics of the referral process, such as local rules regarding referrals made to named specialists. Comparisons were drawn between and within themes, case studies and organisational types.
Results
Types of choices available to patients
A comparison of choices and referral systems across the UK (as at 2009).
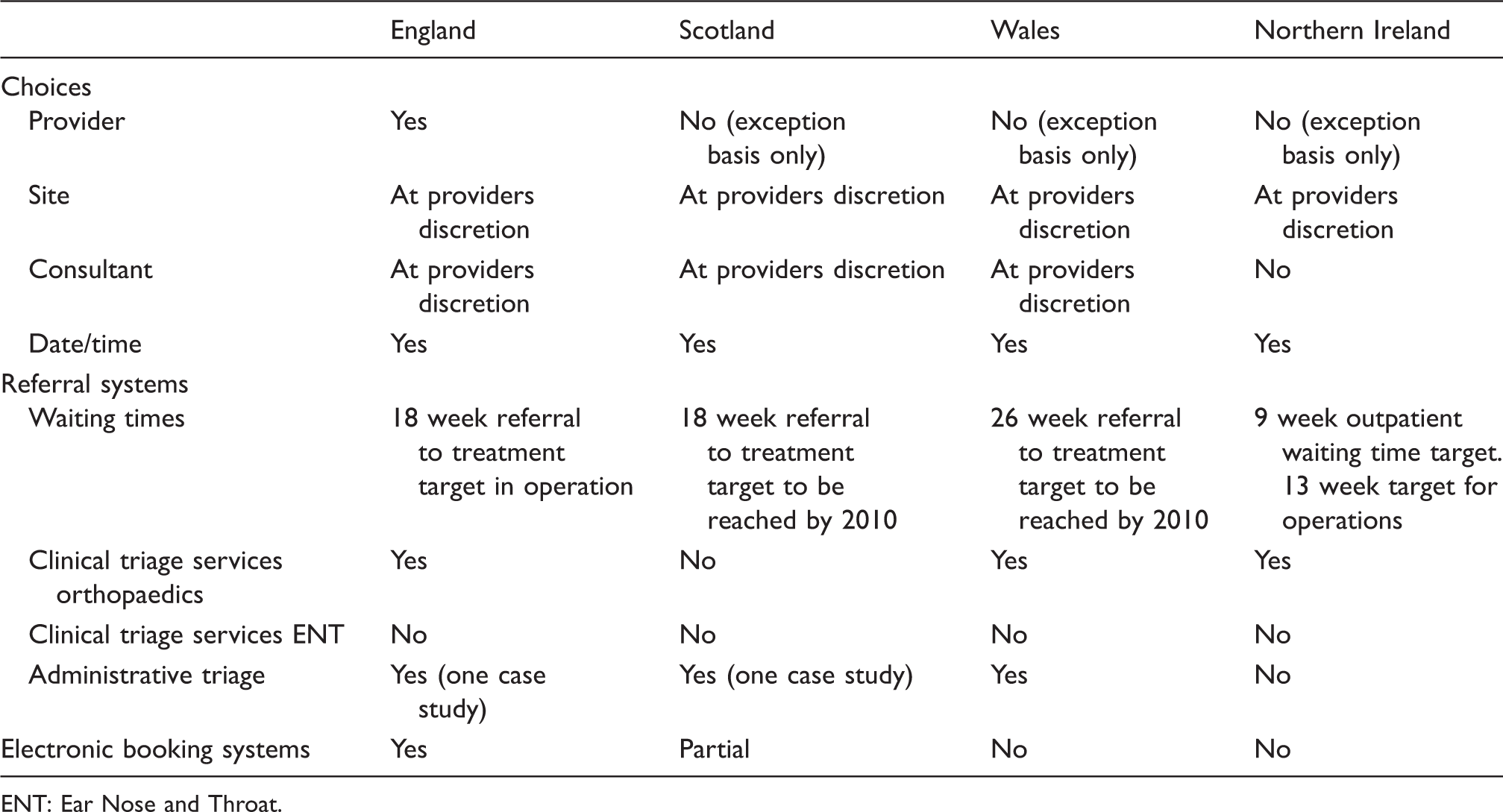
ENT: Ear Nose and Throat.
Choice of provider
There was a clear difference between England and the other countries in the availability of choice of provider. In England, patients had a choice of any provider, although in practice patients were only given the opportunity to select from a limited list of local providers. There was no national system to facilitate choice of provider in Scotland, Wales or Northern Ireland and opinions differed regarding the extent to which this choice was available.
Some interviewees in Wales and Scotland, and to a much lesser extent Northern Ireland, pointed out that patients had a potential choice of provider, albeit in a much more limited form than that available in England. In Wales, patients could be referred to any local provider with whom the local purchaser had a contract. An important distinction emerged between choice of provider and choice of site. For example, in Scotland patients could be referred to any site in the local NHS Board area, while in Wales they might go to one of several sites covered by a single NHS Trust. It was common for providers in all four countries to encompass more than one hospital and so, in effect, whilst patients in Scotland, Wales and Northern Ireland were not able to choose their provider, they might be given the choice between a number of sites managed by a provider. In all three countries, patients could be referred further afield on an exceptional basis. However, these options were reported by interviewees to be largely theoretical, with the vast majority of patients being referred to the local provider.
A number of factors beyond the lack of a policy of provider choice were cited in relation to the lack of choice in Scotland, Wales and Northern Ireland. In the main these related to issues of lack of access caused by geography and population distribution. In Northern Ireland, choice of provider was reported to be impractical due to the small size of the population and the limited number of providers that could be justified. Interestingly, the impact of geography on the availability of choice was also raised at one English site which offered more limited patient choice of provider because it was on the coast.
Choice of specialist
Choice of specialist (consultant) was reported to be available at the discretion of providers in England, Scotland and Wales but not Northern Ireland. In all cases, the reason for limiting patient choice of specialist was reported to be the need to reduce or control waiting times. GPs were encouraged to make generic referrals to teams, rather than to a named specialist (although it was also reported that GPs often ignored these requests). Paradoxically perhaps, the ‘Choose and Book’ electronic booking system in England, which was designed to make choice more easily available to patients, was reported by both GPs and providers to be used to limit choices by excluding choice of specialist from the menu of options.
Choice of date and time of appointment
Choice of date and time of appointment was available to patients when they were referred to a provider in all four countries. All four NHS systems had issued guidance to providers, outlining two associated methods of administering referrals (‘partial’ booking and ‘full’ booking) to offer choice of date and time of appointment to patients. In a full booking system, the patient was given an opportunity to agree a date within a working day of the decision to accept the referral. In a partial booking system, the patient was contacted four to six weeks before attendance/admission was due to agree a date and time. These systems entailed patients contacting the provider to make their appointments. If patients failed to do so, they could be discharged to the care of their GP, or if they rejected two ‘reasonable offers’ of appointment times, their waiting time could be restarted so that they went to the bottom of the list. Our data suggest that these systems functioned as a mechanism for managing waiting times for providers and were utilized primarily for this purpose, rather than to deliver choices to patients.
Management of choice along the referral pathway
Whilst the focus of the study was on the choices available to patients during referral, our data also highlighted the cross national similarities in the systems which had been put in place to manage the referral pathway.
In all countries, we found examples of clinical triage of orthopaedic referrals which aimed to ensure that patients were seen in the most appropriate clinical setting (e.g. acute orthopaedics, physiotherapy or rheumatology, etc). The nature of triage services varied greatly even within case study areas. Some were run by commissioners, some by providers, some used administrative triage based on the content of referral letters and some necessitated additional appointments with clinicians. In Scotland, Wales and Northern Ireland, these triage services were not seen as enhancing choice, even though they might provide opportunities for the expression of patient preferences. In England, it was apparent that the varied nature of these services meant that they affected choices in different ways. For example, where referrals were triaged within secondary care, GPs and patients were still free to choose the provider, but where an intermediate service performed the triage, there was a potential impact on GP and patient choice of provider as it was the triage service, not the GP, that was responsible for the onward referral of the patient to the hospital. Staff in one such orthopaedic triage service felt strongly that their role was to offer choice of provider to patients. However, they were hampered in doing so as they did not have access to the electronic booking system. Interestingly, whilst these services had a potential impact on choice of provider, the GPs interviewed did not feel that triage of referrals restricted choices. This may be connected to our finding that some GPs tended to bypass the orthopaedic triage service if they felt this was clinically appropriate.
Referrers’ communication of choices to patients
Interviewees’ understanding of the availability of choices was often confused and differed within sites. For example, in one Scottish site, GPs gave opposing accounts of referral options, including whether referrals could be made to named specialists and whether clinics were accepting referrals or not. A common area of confusion concerned referral pathways through intermediate clinical or administrative triage services, specifically whether pathways were mandatory or optional, and, indeed, in some cases, there was uncertainty about the triage services in existence. In Northern Ireland, GPs at one site were largely unaware that patients could choose to bypass the orthopaedic triage service.
In England, GPs and providers had a clear understanding that choice of provider should be made available to patients who were being referred. The majority of English GPs interviewed were clear that they did offer choice of provider to patients, not least because at the time of the study, the number of referrals made through the electronic choice menu was monitored, and, in some cases, was linked to discretionary payments to practices. However, in spite of guidance and the electronic booking system, some English GPs were still confused about the referral choices which were available and how to access them. For example, where choice of specialist was thought to be available, some GPs reported that this choice was either not available or could only be made if they knew how to navigate the clinic choices in the electronic system.
Interviews with staff across all four countries suggested that the offer of choice, or full explanation of options, tended to depend on how far patients themselves raised the issue. GPs in Scotland, Wales and Northern Ireland reported that discussion of individual patient options tended not to take place unless initiated by the patient. The nature of these discussions was unsurprising, given the lack of choice of provider policy in the three countries. Referrers in Scotland and Wales often appeared to feel strongly that patients wanted to be referred locally, citing the practicalities of treatment close to home, or, in the case of Wales, that patients were very keen to support their local hospital to ensure it remained viable.
From English GPs’ accounts, discussion of choice of provider with patients tended to be fairly limited. Despite the theoretical availability of any provider, practices appeared to suggest a limited range of options during the consultation, often consisting of five local providers. Although some GPs mentioned the time taken to discuss choices with patients, the content of the choice discussion was a bigger factor in limiting discussion in consultations, with GPs reporting that patients were confused by and not interested in choice.
A further inhibitor of in-depth discussions between GPs and patients about potential providers was a lack of knowledge about the available providers. The view of some GPs was that they only had knowledge of local providers and were not able to advise about other providers, which were ‘just a name in a box’.
Discussion
Whilst the explicit promotion of patient choice in English policy would suggest greater possibilities for choice compared with Scotland, Wales and Northern Ireland, in practice differences were more nuanced. Only in England was choice linked to encouraging competition between providers. However, a concern with responsiveness in the other countries meant that providers still took account of patient preferences. All four countries had some degree of choice of provider.
Choice in England appeared more limited than policy would suggest, as referrers reported offering patients a choice of five, rather than any provider. GPs’ reluctance to offer a free choice and their reported unfamiliarity with distant providers may be due to the staged roll out of policy in England, in which choice of any provider was a recent development at the start of the study. In Scotland, Wales and Northern Ireland, the choices available were much more limited than the ostensibly free choice available to patients in England, although patients might still have some influence over where they were treated. However, whilst choice of provider was limited, choice of site was potentially available to patients in all four countries.
The feasibility of choice of provider is limited by certain immutable factors including the size of the country and the geographic distribution of the population affecting the number of accessible providers, factors which were reported to make choice of provider impractical in much of Scotland, Wales and Northern Ireland. These issues also appeared to limit the availability of choice of provider for patients in parts of England and are perhaps indicative of a tension between the number of providers needed to offer reasonable choice and the limits of tax funded systems to provide excess capacity. It would be reasonable to expect that these issues would not to be so pertinent in relation to urban populations within the four countries, but GPs also cited patients’ perceived desire to use services close to home as a further limiting factor.
There were strong similarities in the referral pathways across the four countries in terms of the use of triage services and the booking mechanisms offering choice of time and date of appointment to patients. The impact of triage services on patient choice of provider varied depending on the structure of the service in question. Only in England were these services considered in relation to the possibilities they presented for offering choices to patients. However, at the time of the study, choice policy in England with its focus on referral from GP direct to providers, largely ignored the more diverse referral pathways which often existed.
Choice of date and time of appointment was similar across all four countries. Unlike other types of choice which were often seen as limited by issues of capacity, the system used to deliver choice of date and time of appointment was acknowledged to be a very successful tool for capacity management. This perhaps explains the use of similar approaches and is indicative of the prominence of waiting time targets in all four countries.
Referrers’ understanding of referral options for patients was at times confused in all four countries. Whilst most GPs in England were clear about the choice of provider available to patients, those in all four countries were uncertain about other aspects of referral which had an impact on choice, in particular choice of specialist and the status of recommended referral pathways. It was perhaps surprising that this confusion existed in England, where referral options had been formalized in the Choose and Book electronic menu. Difficulties navigating the booking system itself could have an impact on GPs’ understanding of available options. This suggests that patients’ experience of choice in all four countries depended to some extent (less so in England) on the GPs’ knowledge. Our data suggest that GPs were not always compliant with the rules or guidance regarding referrals, sometimes for instance choosing to refer to a named specialist rather than a generic team or to bypass recommended referral pathways.
Much research examining the implementation of patient choice policy in England has focused on the ambivalence of clinicians, 8 particularly GPs, towards the policy. We found that the conversations English GPs reported having with patients about choices were not markedly different from referral conversations in Scotland, Wales and Northern Ireland. Referrers in all countries reported that they were largely steered by their perceptions of what was in the patient’s interest when exploring choice of provider, and in the main they felt that patients’ appetites for choice of provider was small, even in England. Whatever the reasons for the restricted nature of choice conversations, according to GPs, the result was a fairly reactive offering of choice to patients across all four countries.
We did not find sharp differences between England and the other three countries. One explanation may be that choice of provider policy in England was still bedding down at the time. Free choice of any provider had only been recently introduced and it may take time for policies affecting doctor–patient interaction to be implemented. This is supported by survey data in England suggesting that patients’ recall of being offered a choice of provider in England was rising steadily in the period from 2006 to 2010. 25
Since 2009, the direction of travel of patient choice policies in England, Scotland, Wales and Northern Ireland has continued. Scotland, Wales and Northern Ireland have increased their focus on organisational integration and collaboration rather than provider competition, and achieving patient involvement in care decisions through care pathway planning rather than individual patient choice. The coalition government has retained patient choice in England and extended it by ensuring that choice of specialist-led team is offered. It has also relaxed the performance management of waiting times. This, together with policies favouring a greater variety of providers, and increased patient experience of being given choice of provider, may give providers in England the opportunity and incentive to offer more choice in the future and thus accentuate the difference between England and the rest of the UK.
The study illustrates the challenges of implementing policies that extend patient choice in health care systems where it has not traditionally existed. Overall a longer term cultural shift on the part of GPs is required, in all four countries, if patients are to be made fully aware of the choices available to them.
Footnotes
Acknowledgements
We thank the members of the team which conducted the patient choice research: Vikki Entwistle (University of Dundee), Andrew Thompson (University of Edinburgh), Lindsay Prior (Queens University Belfast), Alison Powell (St Andrews University) and Huw Davies (St Andrews University).
Funding
This project was funded by the National Institute for Health Research Service Delivery and Organisation (NIHR SDO) programme (project number 08/1718/147). The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the NIHR Health Services and Delivery Research Programme (formerly SDO), NIHR, NHS or the Department of Health.