
Abstract
Objectives
Research suggests that better feedback from quality and safety indicators leads to enhanced capability of clinicians and departments to improve care and change behaviour. The aim of the current study was to investigate the characteristics of feedback perceived by clinicians to be of most value.
Methods
Data were collected using a survey designed as part of a wider evaluation of a data feedback initiative in anaesthesia. Eighty-nine consultant anaesthetists from two English NHS acute Trusts completed the survey. Multiple linear regression with hierarchical variable entry was used to investigate which characteristics of feedback predict its perceived usefulness for monitoring variation and improving care.
Results
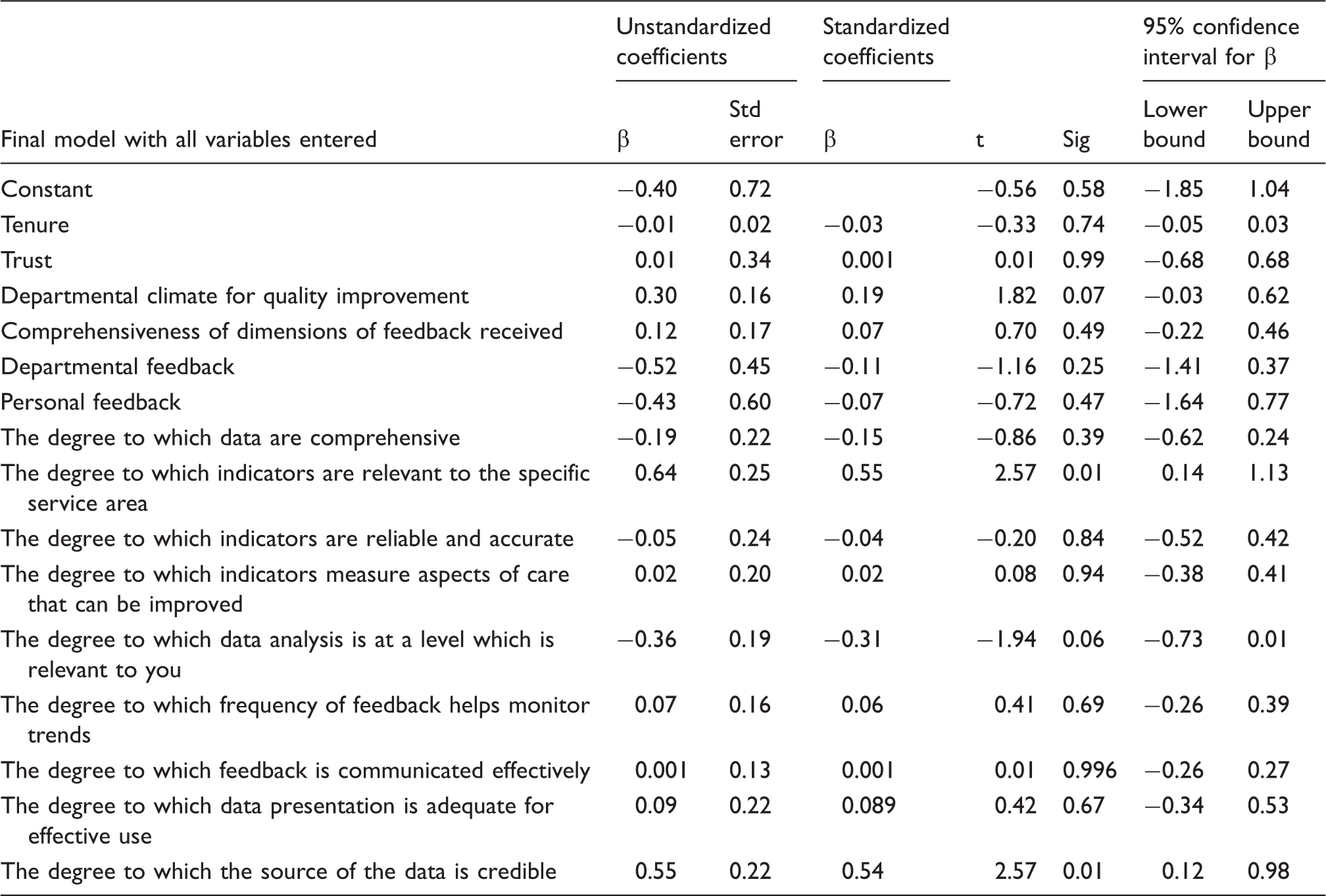
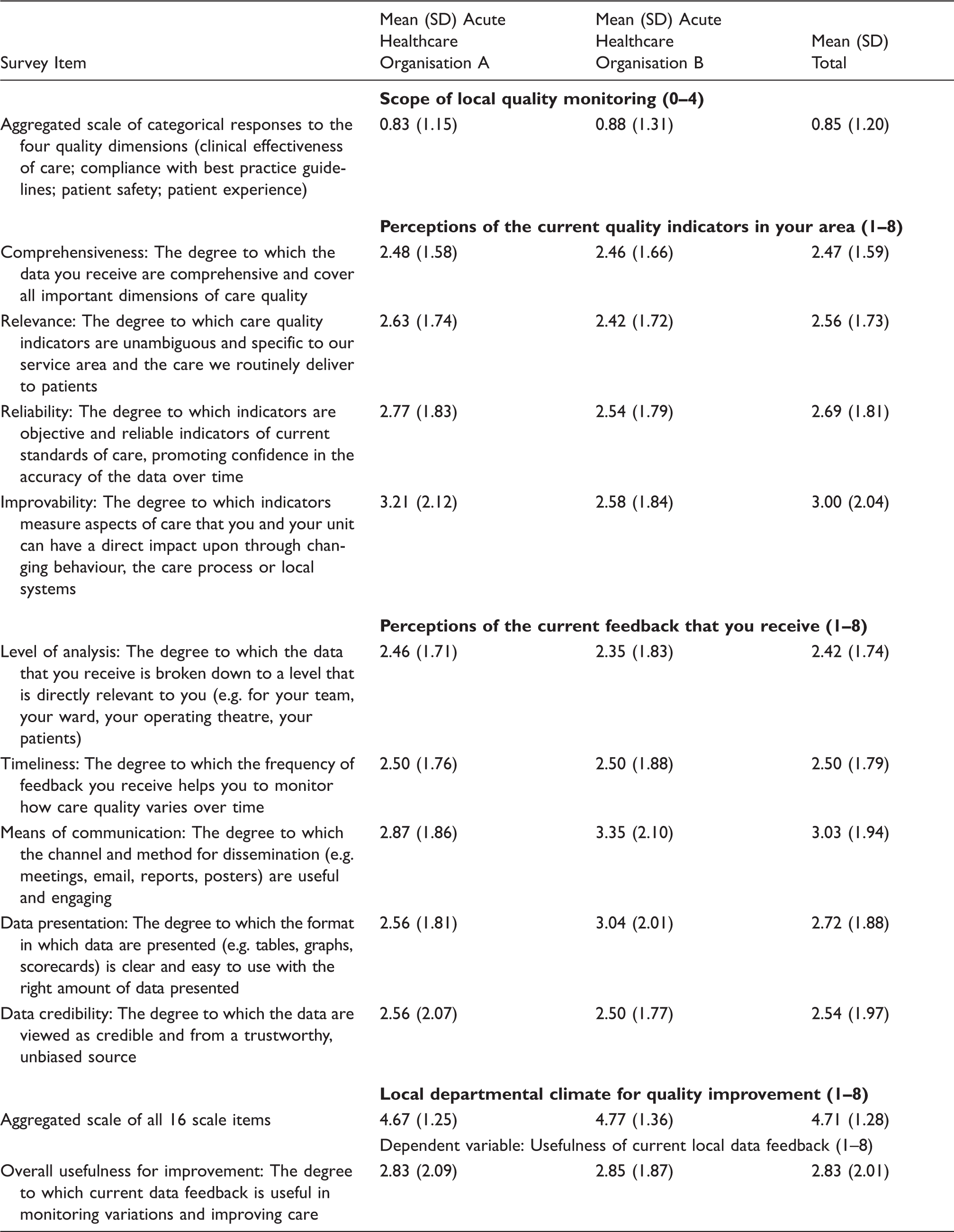
The final model demonstrated that the relevance of the quality indicators to the specific service area (β = 0.64, p = 0.01) and the credibility of the data as coming from a trustworthy, unbiased source (β = 0.55, p = 0.01) were the significant predictors, having controlled for all other covariates.
Conclusion
For clinicians to engage with effective quality monitoring and feedback, the perceived local relevance of indicators and trust in the credibility of the resulting data are paramount.
Introduction
The Francis Report called for information that is accessible and useable by all, allowing for effective comparison of performance by individuals, services and organizations. 1 Effective monitoring and feedback from quality indicators makes variations visible to health care professionals and can potentially support timely remedial action.
In the UK, clinician revalidation has been introduced as a mechanism to uphold and improve practice through continuous professional development. 2 Supporting professional development requires effective design of quality monitoring systems capable of delivering accurate, timely and useful feedback to clinicians based upon valid and reliable quality indicators. 3
A recent systematic review demonstrated that performance feedback to clinicians has a positive impact on behaviour and outcomes, resulting in small to moderate positive effects. 4 Such effects have been observed in terms of reduction of mortality rates and improved compliance with guidelines, amongst other outcomes.5,6 Tailoring feedback to the specific clinical setting has been shown to have a positive influence on its effectiveness along with ensuring those issuing the feedback are perceived as experts.4,7–10 High intensity and frequency of feedback improves outcomes along with sustained monitoring.7,10–13 A number of strategies have been identified to support the effectiveness of feedback, including providing recipients with information on specific areas for improvement, action planning and educational components.4,7,8,10–12 It has been suggested that the departmental context in which feedback is administered may be important.14,15
Little systematic research exists, however, to guide development of quality monitoring and feedback mechanisms that clinicians themselves regard as effective.3,16 One study of this type used a qualitative methodology and identified a number of characteristics for effective feedback, according to clinical and administrative staff. They included: the perceived validity and credibility of the data; their source and timeliness; the way units are benchmarked and the avoidance of individual profiling that could be misconstrued as punitive. 17 Other relevant studies focussed on evaluating existing approaches to feedback from the perspective of clinicians. These include multisource feedback18–21 and benchmarked feedback of patient reported outcome measures. 22
Existing approaches are more concerned with evaluation of audit and feedback interventions with limited attention to what makes specific interventions successful. Greater research effort needs to be devoted to understanding the underlying mechanisms through which feedback is effective. 23 Identifying the characteristics of feedback perceived by clinicians to be of most value may go some way in commenting on the ingredients required to produce the most desirable effects from audit and feedback as a quality improvement tool.
In anaesthetic services, intraoperative process data and recovery room quality indicators such as core temperature, patient reported pain, nausea, and quality of recovery may serve as the basis for feedback.17,24,25 The challenges of developing sensitive and reliable quality indicators and patient satisfaction measures in this clinical area are well documented.2,24,26,27 There is currently considerable specialty interest in developing national standardized guidance for perioperative quality monitoring and reporting in anaesthesia. 28
Currently, anaesthetists rarely receive continuous, systematic feedback on anaesthetic quality to support professional behaviour change and service improvement.17,24 Given the likelihood that feedback mechanisms are linked to organizational and departmental quality assurance, perceptions of feedback are likely to vary as a function of tenure, organizational context, and local unit climate for quality improvement. The role of the level of feedback, its intensity and more specific design characteristics may additionally influence perceived utility. Given the limited evidence as to the important characteristics of feedback from a clinician's perspective, the aim of the current study is to investigate which characteristics are of most value. We use baseline data collected in the evaluation of an initiative for anaesthetists to explore the role of a range of demographic, contextual, and design characteristics in predicting anaesthetists’ perceptions of utility of data feedback.
Methods
Study design
A cross-sectional survey design was used with data collected at a single time point.
Participants and data collection
Two UK NHS organizations with large perioperative service departments were selected as the basis for the study sample. These sites were chosen because research leads based at both sites were collaborators on a programme to develop perioperative quality indicators as part of a national initiative in the UK. 28
Data were collected from consultant anaesthetists prior to any local development of quality monitoring programmes.
Research measures
The survey measure was developed by a multidisciplinary research team working at the primary study site (Organization A). Initial survey items were developed based upon literature review of emerging theory in the area of data feedback for quality improvement. Questions were designed to quantify specific characteristics that have been identified as important, e.g. relevance, validity, reliability and applicability. 3 The approach taken was that anaesthetists should evaluate outcome measures against their potential to lead to improvements in standards of care and benchmarking. 2
Iterations of the survey items were discussed and refined by three consultant anaesthetists and a social sciences researcher with experience in survey design. The survey was piloted using a cognitive walkthrough technique with two additional consultant anaesthetists in which presentation, item interpretation and wording were clarified through a structured interview in which participant interpretations and responses to the survey items were verbalized and discussed with the researchers. Survey items were refined based upon the results from this exercise.
The survey measure comprised four items assessing the comprehensiveness of local quality monitoring, i.e. whether clinicians received regular quantitative feedback on a number of quality dimensions. These items were summed into a scale representing comprehensiveness of monitoring for the purposes of the regression analysis. The level of care that the feedback focused upon (i.e. care at the departmental/individual level) was then assessed.
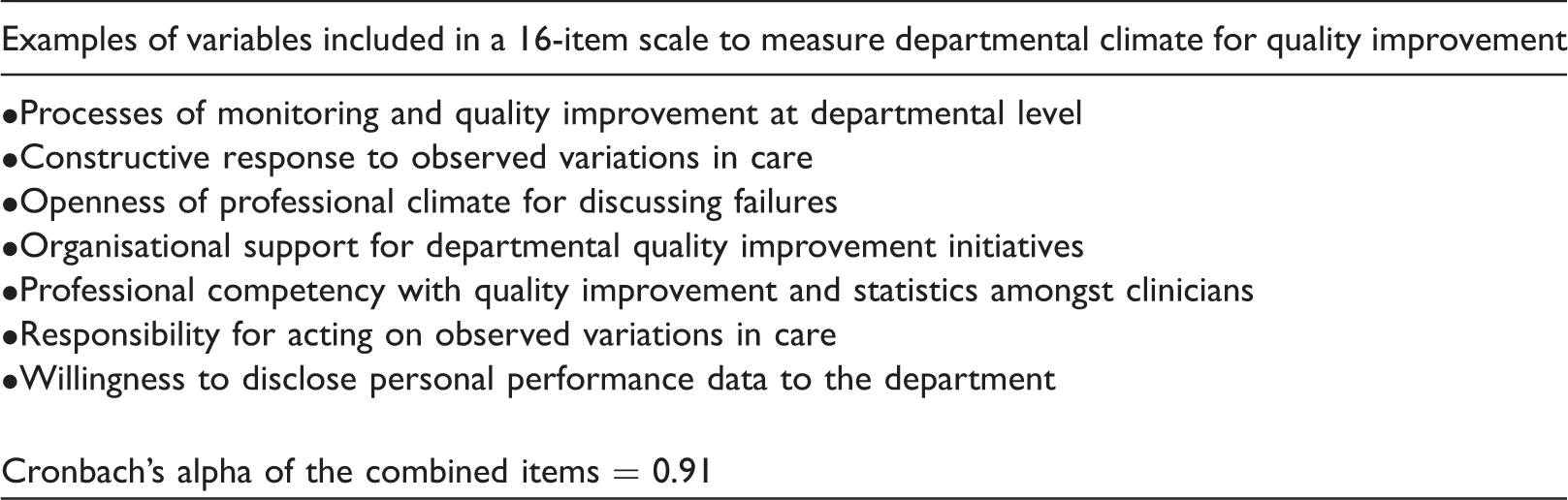
Departmental climate for quality improvement.
Statistical analysis
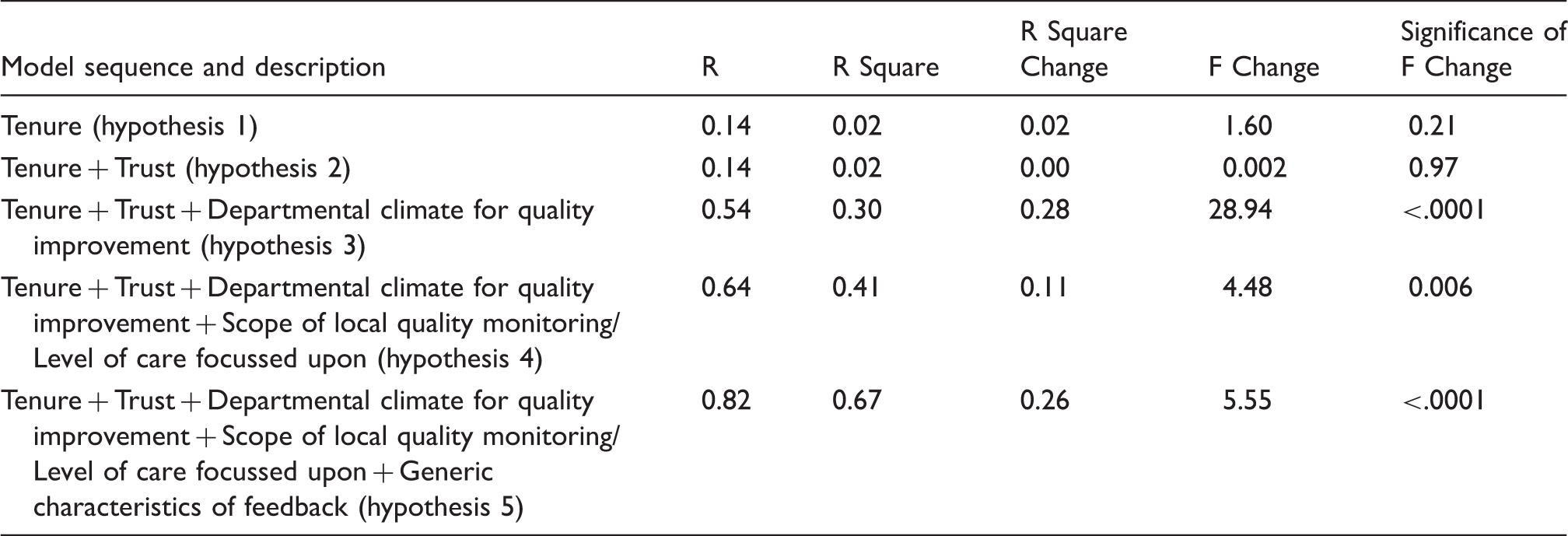
Multiple linear regression analysis with hierarchical variable entry was performed. The following hypotheses were tested using hierarchical entry of specific predictors in steps. For details of the predictors that were entered to test each hypothesis please refer to Table 4 in the ‘Results’ section.
Hypothesis 1: Length of time since qualification (tenure) will influence perception of the degree to which current local data feedback is useful for monitoring variation and improving care in anaesthesia. Hypothesis 2: Organizational membership will influence perception of the degree to which current local data feedback is useful for monitoring variation and improving care in anaesthesia. Hypothesis 3: The reported local departmental climate for quality improvement will influence perception of the degree to which current local data feedback is useful for monitoring variation and improving care in anaesthesia. Hypothesis 4: The reported scope of local quality monitoring will influence perception of the degree to which current local data feedback is useful for monitoring variation and improving care in anaesthesia. Hypothesis 5: The design characteristics of feedback will influence perception of the degree to which current local data feedback is useful for monitoring variation and improving care in anaesthesia.
The statistical significance of the additional proportion of variance in the dependent measure accounted for by each successive entry of variables was assessed in order to establish the role of each specific hypothesized predictor, having controlled for previously entered factors. 29 Forced entry regression was selected as the most appropriate method, as preexisting research findings and theory (outlined earlier) are available to support the order of causal and temporal priority amongst the independent variables.
Results
Descriptives
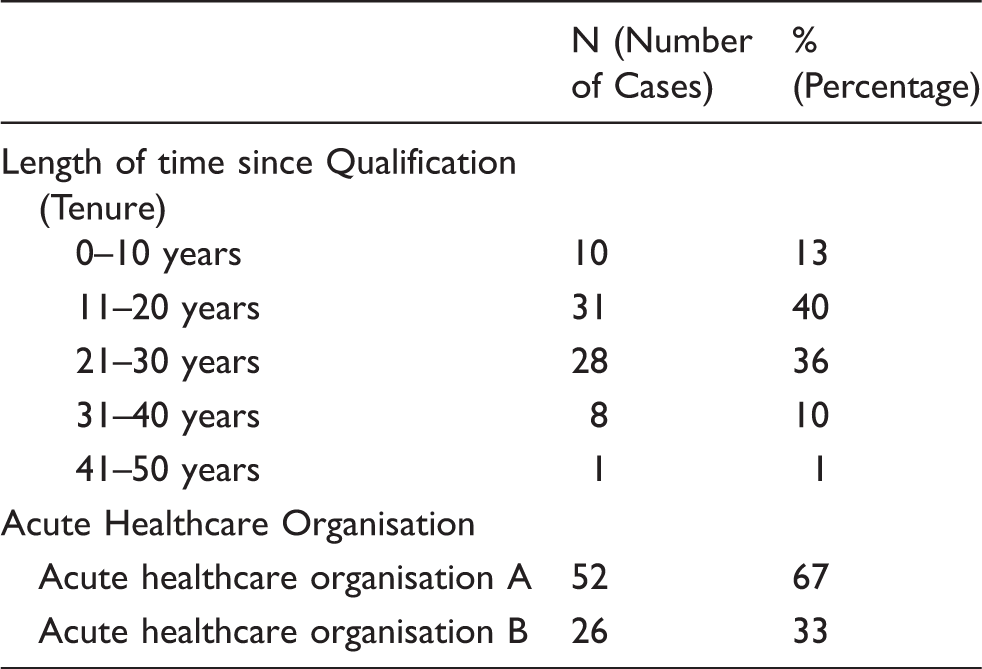
Eighty-nine respondents from two acute healthcare organizations participated in the study. This represents a response rate of 59% (70% for Organization A and 48% for Organization B). Eighty-two (92.1%) participants were consultants, six (6.7%) were trainees and one (1.1%) was nonconsultant faculty. Anaesthetists included were from a mixture of specialties typical of a large, urban, academic teaching hospital. Following exclusion due to missing data, 78 survey responses were included in the regression analysis.
Respondents’ characteristics: descriptive information about the clinicians that were included in the analysis.
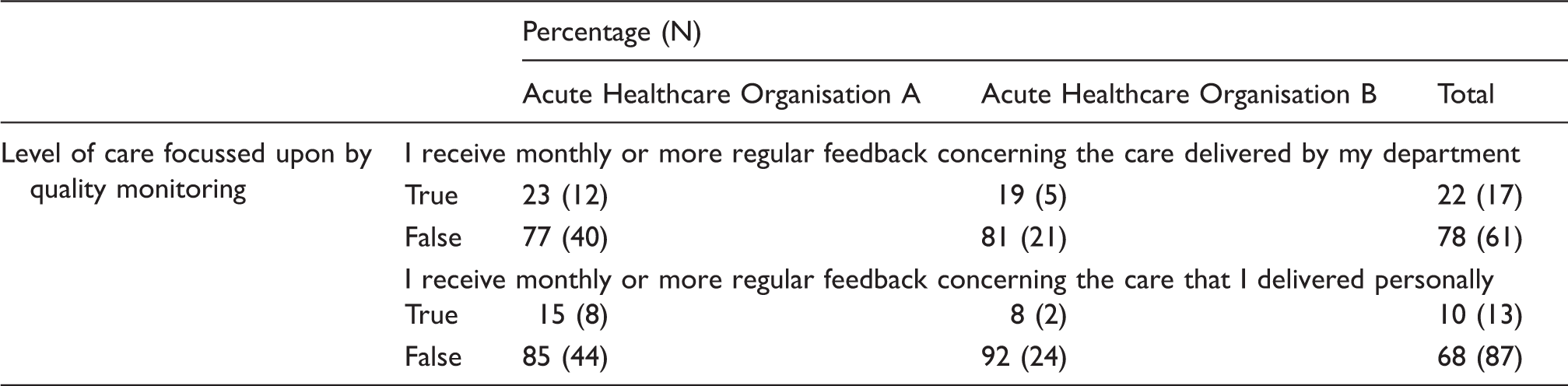
Descriptive statistics of survey items: percentage responses to categorical variables, with number of responses shown in brackets, split by acute healthcare organisation.
Descriptive statistics of survey items: mean responses to scale variables, with standard deviation shown in brackets, split by acute healthcare organisation.
Regression analysis
Model summary: overview of statistics illustrating model fit for each of the five study hypotheses.
Coefficients: model parameters for final fitted model with all variables entered.
Discussion
This study aimed to investigate the characteristics of feedback that are perceived by clinicians to be of most value.
Neither tenure nor organizational membership significantly influenced perceptions of usefulness, demonstrating that there were no significant differences in perceptions of current local feedback attributable to professional experience or due to location at either study site. Variations in perceptions of local departmental climate for quality improvement, however, was a significant predictor accounting for a large proportion of the variance in the dependent measure (27.5%). This finding is interesting as it suggests that without a supportive local context, providing information on variations in care may not result in improvement. It is additionally compatible with prior research, which suggests that having a local operating culture conducive to quality and safety improvement is an important contextual factor influencing the success of local initiatives.14,15,30
Both the scope of local quality monitoring and the level of feedback were significant predictors of perceived usefulness. This suggests that the more dimensions of care on which an individual receives feedback, the more useful information they have to interpret and from which to learn. Higher overall intensity of feedback has been shown to increase its effectiveness. 4 In our model, receiving feedback on care delivered by the individual practicing clinician was a strong positive predictor of perceived usefulness. This finding reinforces the notion that personal professional feedback is important in learning and improving practice.9,16
The final regression model investigated the role of feedback design characteristics, which were found collectively to explain a large proportion (26.4%) of the remaining variance in perceived usefulness, once all prior factors had been controlled for. As expected, the design of feedback is clearly the most important predictor of its utility. When all design characteristics were entered into the model simultaneously, only two factors were found to have a significant unique effect upon perceived usefulness of feedback. These were the relevance of the quality indicators to the specific service area and the credibility of the data as coming from a trustworthy, unbiased source.
Prior research has highlighted the importance of the perceived credibility of data from quality indicators and the extent to which it originates from a trusted source.3,4,9,31 Qualitative findings highlight the importance of investing time to establish the credibility of performance data and involving respected members of senior staff to achieve this. 17 Two systematic reviews support this concept further by identifying feedback provided by experts as being more effective.7,10
The local relevance of quality indicators has additionally been highlighted as an important characteristic of effective feedback. Two systematic reviews concluded that tailoring a feedback intervention to the local setting augmented its effectiveness.8,9 In anaesthesia, a recent national survey study in the UK has demonstrated that current practice in monitoring and feedback is focussed upon high-level perioperative outcomes, productivity, and efficiency indicators, rather than quality of care or patient experience measures. 28 The findings from the current study suggest these types of indicators may be perceived as less useful for quality improvement due to their limited local or clinical relevance.
Although the findings from this study add to our understanding of how to design better feedback from a clinician’s perspective, limitations mean the results should be treated with caution. The sample of respondents was relatively small and based on two organizations only. However, these organizations were both large hospitals and overall response rate was good. It is possible that findings based upon teaching hospitals may reduce generalizability. However, it might conversely be argued that in the preliminary stages of research in this area, clinicians in an academic medical setting are likely to be practicing within a data-rich environment and therefore better able to rate utility. Survey measures are open to a number of respondent biases, though subjectivity may be considered a strength where an ‘end-user’ or ‘stakeholder’ perspective is required. Whilst perceived usefulness is not synonymous with effectiveness, it is likely to govern engagement and uptake of the results from quality monitoring programmes.
Our findings should serve as a basis for further research, which might usefully employ longitudinal investigation of the effects of feedback interventions with specific design and implementation characteristics. Such work might, for example, clarify the potentially reciprocal relationship between the development of quality monitoring processes and local departmental climate for open and effective use of performance data. Does a more supportive climate lead to enhanced feedback or vice versa? Our study suggests that where feedback is limited, the local climate is important in determining its usefulness.
Given current enthusiasm for using quality and safety monitoring to drive improvements in practice, there is surprisingly little evidence to inform development of effective feedback from quality indicators. The findings from this study suggest clinicians perceive a range of factors as important in determining the usefulness of feedback. Specifically, local departmental context and its support of quality improvement is an important determinant of how instrumental feedback from monitoring quality indicators is likely to be. Furthermore, feedback tailored to the personal professional practice of the individual clinician is an important predictor of usefulness. In terms of the feedback design characteristics clinicians value most, the perceived credibility of the data and the local relevance of the quality indicators are paramount.
Footnotes
Acknowledgements
The authors wish to thank Dr Mark Sacks, Dr Christopher Stonell and Dr Claire Moloney for their contributions to the development of the survey measure and data collection for this study. We additionally thank Ms Floor Aleva for her contributions to the broader research programme upon which this study is based.
Declaration of competing interests
The authors declare that there is no conflict of interest.
Funding
This work was supported by funding from the National Institute for Health Research (NIHR) Health Services and Delivery Research (HSDR) Programme (project number 11/1015/21), the Collaboration for Leadership in Applied Health Research and Care (CLAHRC), and the NIHR Imperial Patient Safety Translational Research Centre. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Ethics approval
This study was approved as a service development project.