
Abstract
Objectives
Community health centres are the main form of provision of primary care in China. There are three models: government managed, hospital managed and private. Our aim was to describe and compare primary care under the three ownership models.
Methods
Four aspects of primary care were studied: services, organization, financing and human resources. Interviews were undertaken with 60 managerial and professional staff in 13 community health centres in the Pearl River Delta region in 2010. Three community health centres were selected in the capital city and two were selected from each of the other five cities. Thematic framework analysis was conducted.
Results
Government-managed community health centres received the largest public funding, followed by hospital-managed community health centres, while private community health centres received the least. Private community health centres were the smallest in scale and provided lower quality public health services compared with the other two models. Patient out-of-pocket costs accounted for the majority of the revenue in all models of community health centres despite improved government funding for preventive services. General challenges such as the shortage of public funding, the exclusion of migrants in the funding for preventive services, low capacity in human resources and the separation of clinical and preventive care in community health centres were identified in all three models of community health centres.
Conclusions
The ownership and management of a community health centre greatly influence the service it provides. Private community health centres are in a disadvantaged position to deliver high quality clinical and preventive care.
Introduction
Primary care providers in China include community health centres (CHCs) in urban areas and township hospitals and village clinics in rural areas. 1 Until 1978 there was strong primary care known as the barefoot doctor system. 2 Over the last three decades government funding for health care has fallen together with a shift from primary care to hospitals. 3 The absence of a referral system gives patients the free choice of choosing providers. Currently, public hospitals provide the majority of ambulatory visits, 4 limiting access and increasing costs. 5 Life expectancy and the infant mortality rate have fallen behind what might be expected from the rapid economic gains seen in the last three decades.6,7 As a response to widespread discontent regarding poor access and high costs, the government launched a comprehensive health reform plan in 2009 to re-establish government roles in providing public goods. The plan aimed to invest RMB 850 billion (US$ 135 billion) to develop a more accessible, affordable and equitable health care system. 5 One of the cornerstones of the plan was to strengthen primary care facilities: CHC in urban areas and township hospitals in rural areas. 8 CHCs have been established since 1997 from a variety of sources, including local hospitals and clinics. By 2011, 32,812 CHCs existed. 9 CHCs have a multiprofessional team including doctors, nurses, public health specialists and traditional Chinese medicine doctors. They provide clinical and preventive care to residents in a defined area. Doctors working in the CHCs have often previously worked as specialists. They normally register as general practitioners (GPs) in addition to their original specialty after receiving 3–12 months training in family medicine.
Since 2009, the government has invested in a package covering elderly care, chronic disease management, health education, immunization, maternal and child care, mental health care, and communicable disease prevention and reporting. Funding, which is per capita based, is provided by the local government to the CHCs. Clinical care provided in the CHC is normally covered by a combination of health insurance and out-of-pocket payments.
Three models of CHCs exist: government managed (GCHCs) are owned and managed by local governments; hospital managed (HCHCs) are owned and administered by public (holding) hospitals; privately managed (PCHCs), owned by private business and located mostly in south and west China where local government does not have sufficient investment in primary care. 10
CHCs in the Pearl River Delta region
This region, located in southern China next to Hong Kong and Macau, includes six cities: Guangzhou, Shenzhen, Dongguan, Foshan, Zhongshan and Zhuhai. The total population is over 50 million and it is the most economically dynamic region in China with over 18 million internal migrants in its manufacturing workshops. The six cities had better health indicators than the national average (infant mortality rates 2–4% compared to 12.1% of China) and 5–8 doctors per 1000 compared to four of China in 2010. 11
The region contains all three types of CHC. Government CHCs staffed by former employees of public hospitals with catchment populations of 30–50,000. All GCHCs are expected to focus their services on public interest and report directly to the township government. There are two types of hospital CHCs reflecting the relationship with the holding hospital: Type 1 in which the holding hospital is a township hospital covering a population around 200,000; Type 2 in which CHCs are outreach clinics run by the holding public hospital and covering a population of 30–50,000. Private CHCs have largely disappeared from the region due to increased government investment in primary care. They were previously public clinics bought by private business.
Although a few studies have described the evolution of CHCs in China,1,12 little attention has been paid to the influence of ownership in their development. Our aim was to describe and compare the structure of each model (services, organization, financing, human resources) and consider to what extent these aspects have been influenced by ownership and what are the strengths, weaknesses and challenges facing CHCs.
Methods
Two CHCs were selected representing the most prevalent model in each cities: GCHCs in Dongguan; HCHCs in Foshan, Zhongshan, Shenzhen and Guangzhou and PCHCs in Zhuhai and Guangzhou. One extra CHC was selected in Guangzhou, the capital city of the province, where two models of CHCs coexisted.
Number of interview respondents in the six cities of the Pearl River Delta region, China.
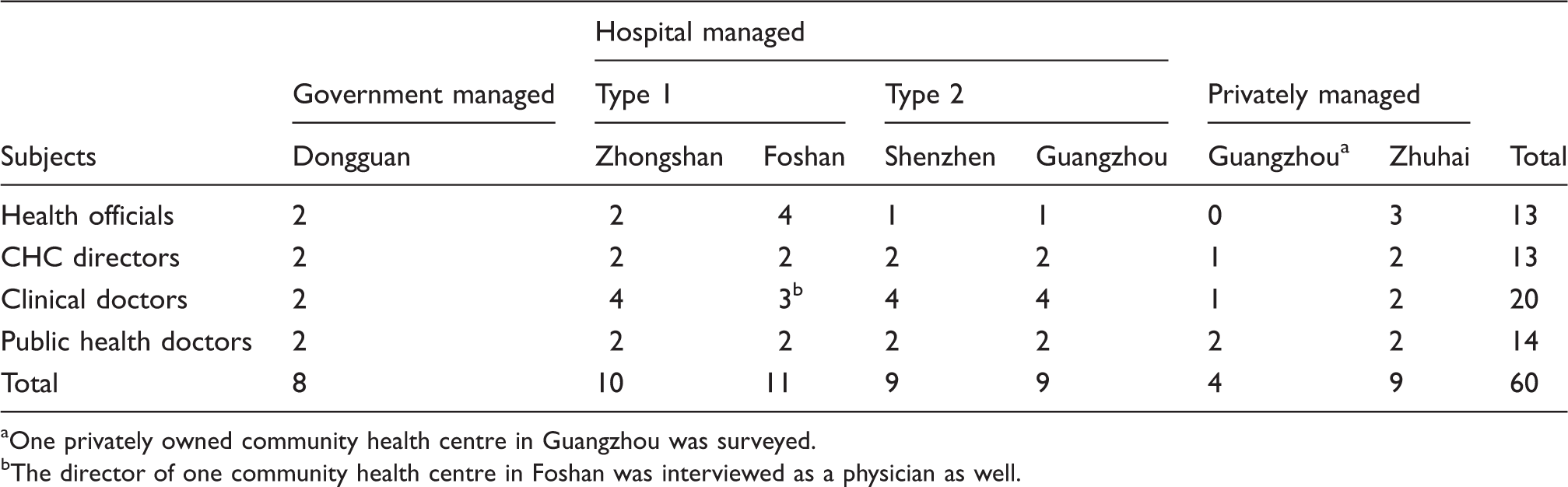
One privately owned community health centre in Guangzhou was surveyed.
The director of one community health centre in Foshan was interviewed as a physician as well.
Results
Interviews were conducted with 13 health officials, 13 CHC directors, 20 clinical doctors and 14 public health doctors or nurses. Institutional information was collected from all 13 CHCs (as shown in the online appendix).
Services
Organizational features and service provision in each type of community health centre (CHC).
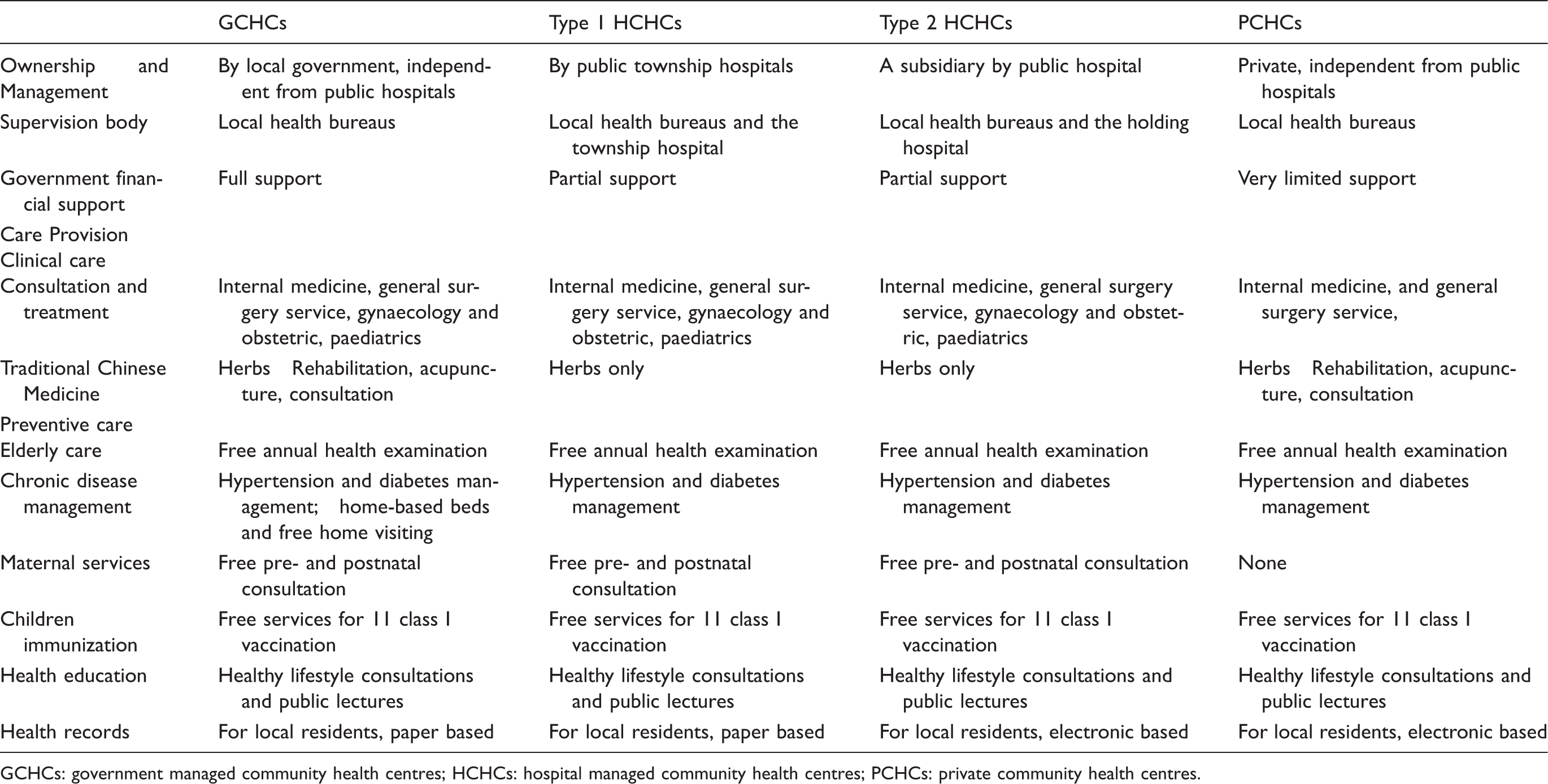
GCHCs: government managed community health centres; HCHCs: hospital managed community health centres; PCHCs: private community health centres.
In terms of the preventive care, all CHCs provided free pre- and postnatal consultancies for mothers except private CHCs in Zhuhai where such care was provided in the public hospitals. Child immunization under the government public health package is free for both local and migrant residents. However, immunizing migrant children is a big challenge. A CHC doctor commented that, ‘migrants do not understand the importance of immunisation for kids. They do not come [to the clinic] for immunisation. Some also changed their homes and mobile numbers so it is hard to find them’. Private CHCs were even more reluctant to provide immunizations due to limited government funding.
Organization
Government CHCs had a closer relationship with the local health bureau than other models of CHCs. In Dongguan, an inter-governmental committee for primary care had been established to discuss strategic coordination among different government agencies including the bureaus of health, finance, personnel and social insurance, and the township government. The health bureau and township government provided funding to CHCs and evaluated their performance on an annual basis. Based on the evaluation, the best CHCs were given an extra 10% of government funding and the worst were deducted 10%.
Hospital CHCs had weaker linkages with the health bureaus compared to the government CHCs. As one health official noted, ‘the holding hospital is a bridge. The Bureau gives funds to the hospital and then the hospital transfers funds to the CHCs. Little we can do if the hospital does not transfer the fund’. In Shenzhen, community health departments have been established in the holding hospitals to ensure CHCs receive public health funds.
Not surprisingly, the private CHCs reported the weakest linkages with the health bureaus due to the low level of public funding they received. Private CHC directors commented that ‘the health bureau provided much smaller funds to us for public health services because some of service is provided by public agencies’. In public CHCs, failure to pass the annual evaluation often led to a period of suspension of operation.
Government CHCs and public hospitals are separate organizations though the latter are required to provide technical guidance and training to CHCs. Patients that need specialist care were referred by CHCs to public hospitals but no hospitals refer back discharged patients who need primary care.
In hospital CHCs, the holding hospitals played an important financial and administrative role including appointing directors and staff, and supervising clinical and public health care. In Type 1 hospital CHCs, the hospitals covered the full costs including salaries. While in Type 2 hospital CHCs, the holding hospitals provided only limited financial support and CHCs had to generate their own revenues. The CHC directors reported that the holding hospital normally blocked the health bureau’s funds for public health services. ‘Government money [for CHCs] is given to our holding hospital. We do not know the exact amount the government provides [for CHCs]. [Therefore], there is no incentive for us to provide better public health care’, said a CHC director in Shenzhen.
A very weak link existed between the public hospitals and the private CHCs, as the trust between them was low. In certain areas such as acute care, the public hospital was in competition with the private CHCs.
Financing
Government investment, health insurance reimbursement and out-of-pocket payments were the three major sources of CHCs’ revenue. Government paid for the establishment of government CHCs, the package of public health services and the routine operation of CHCs. In contrast, for other models of CHC, government only paid for public health services. Thus, the share of government funding accounted for nearly half of revenues in government CHCs but only 5% in hospital CHCs and less than 1% in private CHCs.
The government provided per capita-based funds for the public health package, ranging from RMB 30–40 (USD 5–7). The package also covered migrants who have had a contracted job for six months or longer.
Government health insurance was a major source of revenue for many CHCs. Type 2 hospital CHCs had the highest contributions (nearly 33%), followed by government CHCs (25%), Type 1 hospital CHCs (10%) and private CHCs (less than 1%). Private CHCs were only recently covered by the government health insurance scheme, mostly for migrants without private health insurance. Only a small proportion of migrants who had long-term contracts were insured but their copayment was higher and benefits were lower compared with local residents.
Use of primary care was promoted in health insurance schemes. For example, the copayment rates were lower in CHCs (30–50%) compared with that in hospitals (40–60% of outpatient costs). In cities like Dongguan, patients had to seek care in CHCs before going to hospitals. Those who were referred to hospitals would be covered for 70% of their outpatient costs, while those who presented to hospitals had to pay all costs out of pocket. This rule applied to insured migrants only in Shenzhen.
Out-of-pocket payments still accounted for the majority of revenue in all CHCs. Hospital CHCs received over 60% and private CHCs 80% of their income from out-of-pocket payments compared with only 40% in government CHCs. The contributions of out-of-pocket payments had remained stable from 2008 to 2010.
Human resources
Government CHCs and Type 1 hospital CHCs had larger workforces as they were township hospitals, while Type 2 hospital CHCs and private CHCs were smaller because they operated as outreach clinics. The responsibilities of public health doctors, who graduated from the public health stream of medical schools, are to provide health education, disease management and case reporting. The majority of doctors, including public health doctors, in CHCs had only three years medical education at college level or below, indicating a limited education. More staff in the government CHCs and hospital CHCs had higher education, nearly 33% had five years university education of medicine compared with less than 10% in private CHCs.
All CHCs reported a separation of clinical and public health care, with the latter provided by public health staff. Providing chronic disease management in patients’ homes was a huge burden due to the large number of patients. We cannot meet the targets of chronic disease management. For example, 23% of our community residents of 35 years or older have hypertension, which translates to over 6,000 hypertensive patients. The health bureau requires follow-ups with every patient on a quarterly basis. We cannot visit patient homes with current human resources,
Public organizations are allocated staff by the government who receive a secured position and benefits. Hospitals often receive smaller quotas than required so extra hands are hired without a quota. A position outside the quota means insecurity, lower salary and less opportunity for promotion. Government CHCs had most of their staff within quotas, while in hospital CHCs, most nurses and junior doctors were not within a quota. Hospitals tended to give their quotas to senior doctors working in clinical departments rather than to staff in the CHCs.
All CHC staff were paid a salary plus a performance-based bonus. Salaries accounted for half the total pay, which is set according to the profession and years of service. On average, staff outside quotas received 50% less than those within quotas at the same level. Bonuses were similar between staff within or without quotas. Bonuses accounted for half the total payment and were based on personal workload and the department profits. In hospital CHCs, bonuses were calculated at the hospital level first and then distributed to the CHC level. In hospital CHCs and private CHCs, doctors’ bonuses were based on the profits the doctor brought to the CHC, such as drugs and medical examinations the doctor prescribed. In general, doctors working in private CHCs earned less than their peers in public CHCs.
Doctors and nurses in government CHCs and hospital CHCs reported receiving more external training opportunities than their peers in private CHCs. One clinical doctor said, I have been here (a PCHC) for three years but did not participate in any external training. There was once a national workshop, but the boss said we do not have any money to support such activities. I am very disappointed.
All CHC directors reported a high staff turnover. Nurses had a higher turnover rate than doctors because nurses were often without quotas and received less pay. One director of a government CHC commented that, ‘we have four to five staff asking for leave every year because of low pay and less opportunities for career advancement’. A hospital CHC director reported that, ‘most of our staff would like to work in hospitals instead of CHCs. We had an experience of recruiting for the same position four times within a year because three nurses came and left’.
Professional development was another barrier to CHC staff. The career promotion trajectory is not clear for primary care doctors. It is very difficult for a doctor to be promoted as a consultant physician because CHCs do not have any senior titles. Our staff with senior titles got them from hospitals before coming here,
Discussion
Main findings
Government CHCs received the largest amount of government funding that included the initial set-up, routine operation, training and the package for public health services, while hospital CHCs received government funds for all the above except routine operation. Private CHCs only received government funds for part of the package of public health services. As a result, local governments played a bigger role in financing and supervising the government CHCs, a lesser role in the hospital CHCs and a relatively weak role in the private CHCs, despite the government encouraging private business to operate CHCs. 15 In general, compared with private CHCs, employees of other models of CHC were better educated, participated in more refresher training and were better paid.10,12
Hospital CHCs had greater clinical capacity because they were directly managed by public hospitals, and patients normally perceived they provided a higher quality of services. 16 On the other hand, they were dependent on public hospitals which generated their income from patient charges, 17 so hospital CHCs were required to make a profit for their holding hospitals and focused on clinical care rather than public health services. 18
Compared with public CHCs, private CHCs received the least government support, were poorly staffed and provided a lower quality of care.10,16,18–20
Key challenges for primary care
The goal in China is to establish an equitable primary care-based system. 15 Family doctors in CHCs are expected to act as gatekeepers providing comprehensive and continuous care. This policy is influenced by primary care in the UK, Australia and Canada where population health indicators have improved and social inequity has been reduced.21,22 However, several key challenges need to be addressed to achieve this goal.
First there is insufficient public funding for CHCs which has not increased much since 2009.23,24 CHCs still rely heavily on patient copayments. 25 Funding has been improved in government CHCs but not much in hospital CHCs. The situation is the worst in private CHCs which are for-profit organizations and do not receive much public funding. International experience has shown that for-profit primary care organizations perform poorly compared with non-profit ones, 26 thus there is a need to encourage hospital CHCs and private CHCs to become non-profit CHCs.
The second challenge is the weak capacity of GPs who earn much less than their peers in public hospitals, a common phenomenon in developing countries. 2 A five-year university training programme has been recently introduced for GPs in China. 27 However, most doctors working in CHCs have only received short-term in-service training in primary care. 1 Furthermore, CHC staff have less opportunity for career development because family medicine is not regarded as a speciality in China. These issues need to be addressed by providing training programmes both for current CHC staff and new graduates. The government is promoting a standard three-year residency programme for medical graduates to become GPs, which will raise standards to that of doctors in hospitals. 28 Consequently, GPs should receive comparable salaries to other doctors at the same levels.
The third challenge is how to meet the needs of the underserved in the community, especially migrants and the elderly. This calls for better coordination between policies in primary care and other public programmes. Migrants tend to use more primary care due to the relatively low costs in CHCs.29,30 However, health insurance schemes only cover a small proportion of migrants with limited benefits, which prevented them using primary care services. 31 Another much needed reform is to curb the profit-driven activities of public hospitals. 3
The fourth challenge is the separation of clinical and preventive care in CHCs. 32 Health records, mostly electronic now, are not properly used and not updated by GPs in their consultations. Another drawback is that many services in the public health package rely heavily on process rather than outcome measures. For example, annual health examinations and quarterly hypertension follow-ups seldom check the impact on health.
Limitations
Several limitations have to be borne in mind. The study purposefully selected a small number of CHCs, thus results cannot be generalized to each model of CHC in China. Only views of providers and administrators of primary care were collected, with no attempt to find out about patients’ views of different models of CHCs.
Footnotes
Declaration of Conflicting Interests
The authors have no competing financial, professional or personal interests that might have influenced the performance or presentation of the work described in this manuscript and the organizations will not finance the publication of this manuscript.
Research ethics
Ethical approval was obtained from the Survey and Behaviour Research Ethics Committee of The Chinese University of Hong Kong, Hong Kong (Ref No. TB106179). Written informed consent forms were collected from all interviewees and participating community health centres.
Funding
We thank the local staff in the six cities, students from the Chinese University of Hong Kong who participated in the data collection, the Bauhinia Foundation Research Centre, Hong Kong (Ref No. 7050162) for funding and the Research Grants Committee, Hong Kong (Ref No. CUHK 4002-SPPR-10). The funding bodies played no role in the study’s design, data collection, analysis or preparation of the manuscript.