
Abstract
Objectives
To review the evidence of the effects of centralization of cancer surgery on postoperative mortality.
Methods
We searched Medline, Embase, Cinahl, Cochrane and Scopus (up to November 2019) for studies that (i) assessed the effects of centralization of cancer surgery policies on in-hospital or 30-day mortality, or (ii) described changes in both postoperative mortality for a surgical intervention and degree of centralization using reduction in the number of hospitals or increases in the proportion of patients undergoing cancer surgery at high volume hospitals as proxy. PRISMA guidelines were followed. We estimated pooled odds ratios (OR) and conducted meta-regression to assess the relationship between degree of centralization and mortality.
Results
A total of 41 studies met our inclusion criteria of which 15 evaluated the effect of centralization policies on postoperative mortality after cancer surgery and 26 described concurrent changes in the degree of centralization and postoperative mortality. Policy evaluation studies mainly used before-after designs (n = 13) or interrupted time series analysis (n = 2), mainly focusing on pancreatic, oesophageal and gastric cancer. All but one showed some degree of reduction in postoperative mortality, with statistically significant effects demonstrated by six studies. The pooled odds ratio for centralization policy effect was 0.68 (95% Confidence interval: 0.54–0.85; I2 = 80%). Meta-regression analysis of the 26 descriptive studies found that an increase of the proportion of patients treated at high volume hospitals was associated with greater reduction in postoperative mortality.
Conclusions
Centralization of cancer surgery is associated with reduced postoperative mortality. However, existing evidence tends to be of low quality and estimates of the effect size are likely inflated. There is a need for prospective studies using more robust approaches, and for centralization efforts to be accompanied by well-designed evaluations of their effectiveness.
Introduction
Evidence points to a positive relationship between clinical outcomes following complex surgical interventions for cancer and a higher number of procedures. 1 Accordingly, there has been a trend towards centralizing the provision of surgical care for cancer patients into hospitals with high activity volumes.2–4 Much of the evidence derives from studies comparing outcomes among providers with different characteristics such as the degree of specialization, case volumes or teaching status.5–7 Such work does however provide little insight into the direction of causality of the volume-outcome relationship for cancer surgery. Such understanding requires the use of prospective study designs 8 that assess the effect of increasing the volume of procedures through centralizing surgery on surgical outcomes. This study aims to synthesize the published evidence on the impact of centralization of cancer surgery on postoperative mortality and to quantify the relationships using meta-analysis and meta-regression.
Methods
We conducted a systematic review following the PRISMA guidelines. 9 The review is registered with PROSPERO. 10
In- and exclusion criteria
Centralization can be driven by active policy intervention or occur spontaneously (or both), 11 with the latter typically without a clearly identifiable starting point because of gradual implementation of related strategies as a result of, for example, individual providers’ desire to become more specialized and/or a greater recognition among professional organizations of the potential benefits of centralization of procedures. Accordingly, we considered two principal types of primary research in our review. First, we considered studies that compared changes in outcomes for (any) cancer surgery before and after the implementation of polices, recommendations or guidance on centralization. In the following, we refer to these types of studies as ‘centralization policy evaluation studies’. Eligible studies had to report the point in time when a given policy, recommendation or guidance was issued and assess in-hospital or 30-day mortality following cancer surgery as the outcome measure. No restriction on study design was imposed. Second, we considered studies that described concurrent changes in (i) the degree of centralization for (any) cancer surgery, measured as reduction in the number of hospitals providing the surgical procedure of interest or an increase in the proportion of patients treated at high volume hospitals, and (ii) in-hospital or 30-day mortality following cancer surgery. We refer to these studies as ‘concurrent changes studies’. Studies that only compared outcomes between hospitals with different activity volumes were excluded, as were studies published in a language other than English. Studies that considered individual surgeons rather than hospitals as unit of observation were also excluded.
Search strategy
We searched the databases Medline, Embase, Cinahl, Cochrane and Scopus from inception to November 2019. The search strategy was conceived to be as broad as possible to reduce the risk of missing relevant studies, while keeping the overall number of records retrieved manageable. Figure A.1 in the Online Supplement shows the detailed search strategy. Reference lists of included studies were followed up to identify additional studies, and Google searches were also conducted for gray literature using combinations of key words (i.e. regionalization, centralization, cancer, surgery).
Study selection
Two authors (RG, FV) independently screened the abstracts of identified records for potential with full text review conducted of studies considered potentially eligible. Disagreements about study eligibility were rare and resolved through discussion among the study team.
Data extraction
The following information was collected from each study: study design, country, objective (i.e. the evaluation of the impact of a centralization policy or description of time trends in postoperative mortality after cancer surgery), the level of policy development (national, subnational), if any, and the year of its enactment, the level of its evaluation (national, subnational), years of first and last data point, number of hospitals providing cancer surgery at the first and last year data point, proportion of patients receiving surgery at high volume hospitals at the first and last data point, and number of patients receiving surgery and in-hospital or 30-day mortality rate following cancer surgery. Where relevant, we used the xyExtract software 12 for data extraction from graphics.
Risk of bias assessment
Risk of bias assessment of centralization policy evaluation studies used the Cochrane Effective Practice and Organisation of Care (EPOC) criteria for interrupted time series (ITS) studies. 13 Uncontrolled before-after studies were considered to be at high risk of bias: given the general trend towards better outcomes after surgery due to advances in surgery and patient care, this study design cannot take into account the effect of pre-intervention trends and likely overestimates the effect of centralization.
Principal data synthesis and analysis
The main characteristics and results of included studies were summarized in tabular format. For centralization policy evaluation studies, we calculated the odds ratio (OR) with 95% confidence intervals from data reported on the number of surgical interventions performed before and after policy implementation and on the corresponding mortality rate. Raw data were extracted from the text, tables or figures of each paper. For included studies that used interrupted time-series design 14 to assess immediate and delayed effects attributable to a given intervention, 15 , 16 we combined these two estimates into a single measure representing the overall intervention’s effect in the study under consideration.
For concurrent changes studies, we estimated the OR for the last and first mortality data point, i.e. the relative reduction (if any) of the mortality risk observed over the respective time periods considered in individual studies (see Online Supplement Tables A.1 and A.2 for further detail).
Meta-analysis and meta-regression
We first conducted a meta-analysis, estimating the pooled OR for the effect of centralization policies on in-hospital or 30-day mortality following cancer surgery using the random-effects model described by DerSimonian and Laird. 17 This method does not assume a single underlying (fixed) intervention effect but takes observed differences that cannot be explained by chance into account in the pooled estimate and its precision. Where several included studies evaluated the same centralization initiative (e.g., a national centralization policy) using the same study design, we only considered the study with the largest sample size. Where study designs differed, we only considered the study with the higher quality design in the quantitative analyses. This means we prioritized ITS design over before-after studies. We carried out sensitivity analysis to assess the stability of the pooled estimate. Heterogeneity was assessed with the I2 statistic; publication bias was assessed through visual inspection of funnel plots and using the Egger test. 18 We further conducted subgroup analyses according to the type of cancer surgery (pancreatic, gastric, and oesophageal cancer).
We compared the pooled results of centralization policy evaluation studies with those extracted from published meta-analyses of studies comparing outcomes after cancer surgery in high and low volume hospitals,19–24 which we identified from a recent umbrella review on the topic. 1
We then conducted a random-effects meta-regression to explore the relationship between changes in the degree of centralization and concurrent changes in mortality following cancer surgery (concurrent changes studies), using the natural logarithm of the OR (lnOR) as dependent variable and (i) the reduction in the number of hospitals and (ii) an increase in the proportion of patients undergoing surgery at high volume hospitals as proxy measures of the degree of centralization. Both variables were treated as continuous, with study duration (years) included as a covariate, based on the assumption that this variable was also related to the degree of change observed.
We used StatsDirect statistical software (version 3.2.8) 25 for the statistical analyses and Stata (version 16.0) for meta-regression. 26
Results
A total of 41 studies were included in the review, of which 15 evaluated centralization policies27–41 and 26 assessed concurrent changes in the degree of centralization and mortality outcomes following cancer surgery (see Figure A.2 in the Online Supplement).
Characteristics of studies evaluating centralization policies
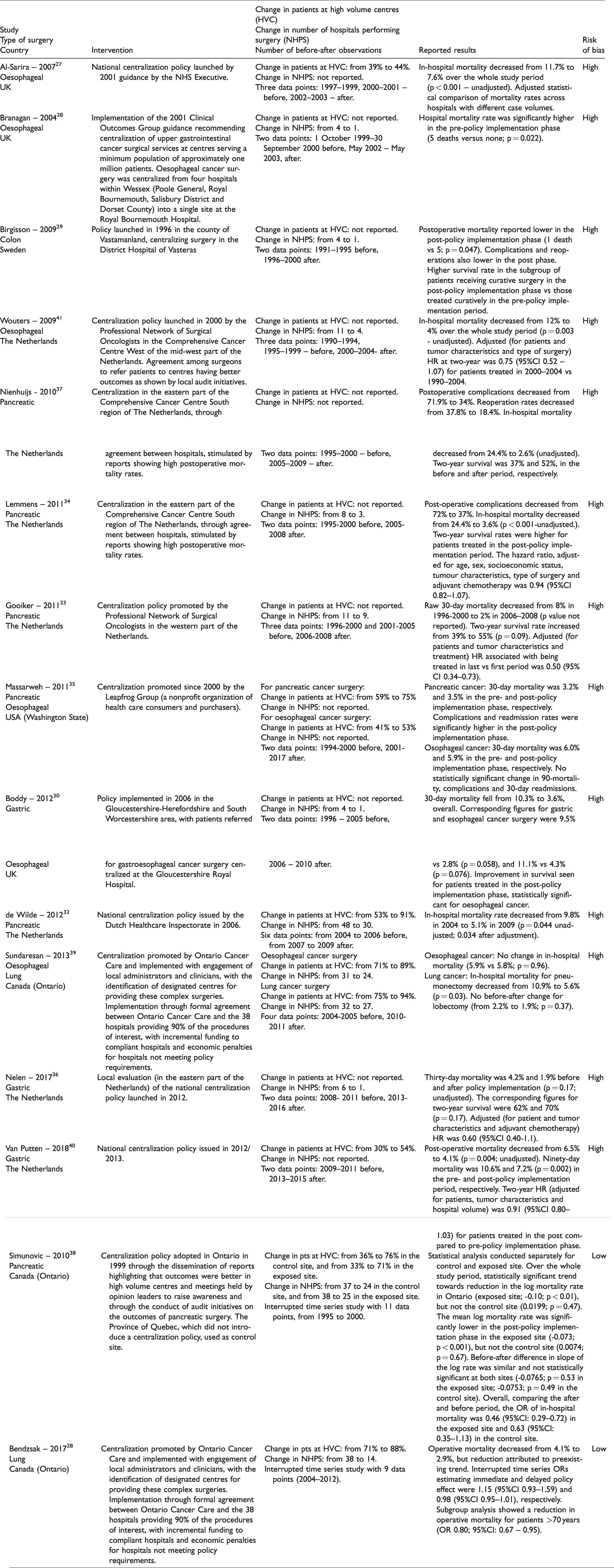
Table 1 summarizes the key characteristics of the 15 centralization policy evaluation studies. Of these, 13 used a before-after design without controls and two used ITS, 28 , 38 rated to be of good methodological quality (Table A.3, Online Supplement). The majority were set in European countries (UK, 27 , 30 , 31 Sweden, 29 the Netherlands32–34, 36 , 37 , 40 , 41 ) three in Ontario, Canada, 28 , 38 , 39 and one in the USA (State of Washington). 35 Six studies concerned surgery for pancreatic cancer,32–35, 37 , 38 five evaluated surgery for oesophageal cancer, 27 , 30 , 31 , 35 , 39 three focused on gastric cancer surgery, 30 , 36 , 40 two on lung cancer surgery 28 , 39 and one on colon cancer surgery. 29 Of the three Canadian studies, two evaluated the same policy for lung cancer surgery 28 , 39 while two Dutch studies focused on the same pancreatic cancer surgery policy. 34 , 37 Five studies evaluated policy impact at national level using administrative datasets, 27 , 28 , 35 , 38 , 39 with the remainder evaluating centralization initiatives at regional level, where volume-based referrals processes were adopted, often responding to national policy or guidance, through local consensus among providers. Studies often did not report well how the policy under review was actually implemented. Where this was documented, initiatives typically involved awareness raising of the benefits of centralizing cancer surgery through reports showing poorer surgical outcomes in patients treated at low volume hospitals 34 , 37 , 38 , 41 or the use of financial incentives to encourage centralization of surgery. 28 , 39
Key characteristics of 15 studies that evaluated the impact of centralization of cancer surgery policies on postoperative mortality.
Effect of centralization policies on post-operative mortality
Overall, 14 studies contributed to the meta-analysis, accounting for 16 observations: six for oesophageal, 27 , 30 , 31 , 35 , 39 , 41 five for pancreatic,32–35, 38 three for gastric, 30 , 36 , 40 and one each for lung 28 and colon cancer surgery 29 (see also Table A.1, Online Supplement). We did not consider the study by Nienhuijs et al., 37 which evaluated the same policy initiative as Lemmens et al. 34 but used a smaller sample of patients. Similarly, we excluded the study by Sundaresan et al. 39 which we considered to be of lower quality than the study by Bendzsak et al., 28 which evaluated the same lung cancer surgery centralization policy.
Of the 14 studies considered, eleven provided information on the effect of centralization policies on the number of hospitals offering the surgery of interest. We found a median relative reduction of 63% (range 18% to 83%), while the proportion of patients treated at high volume hospitals (information provided in six studies) increased by a median of 17% (range 5% to 38%).
Figure 1 shows the estimated odds ratios for the effect of centralization processes on postoperative mortality after cancer surgery. Studies varied greatly in terms of the precision of their estimates, with those evaluating centralization initiatives at the local level based on small sample sizes. Of the 16 observations included in the analysis, six showed statistically significant reductions in postoperative mortality following cancer surgery, 27 , 31 , 34 , 38 , 40 , 41 with an overall pooled estimate of 0.68 (95%CI: 0.54–0.85; I2 = 80%), equating to a 32% relative risk reduction. There was some evidence of publication bias (estimated slope from Egger’s test of 1.75 (p = 0.004); see also Online Supplement, Figure A.3).
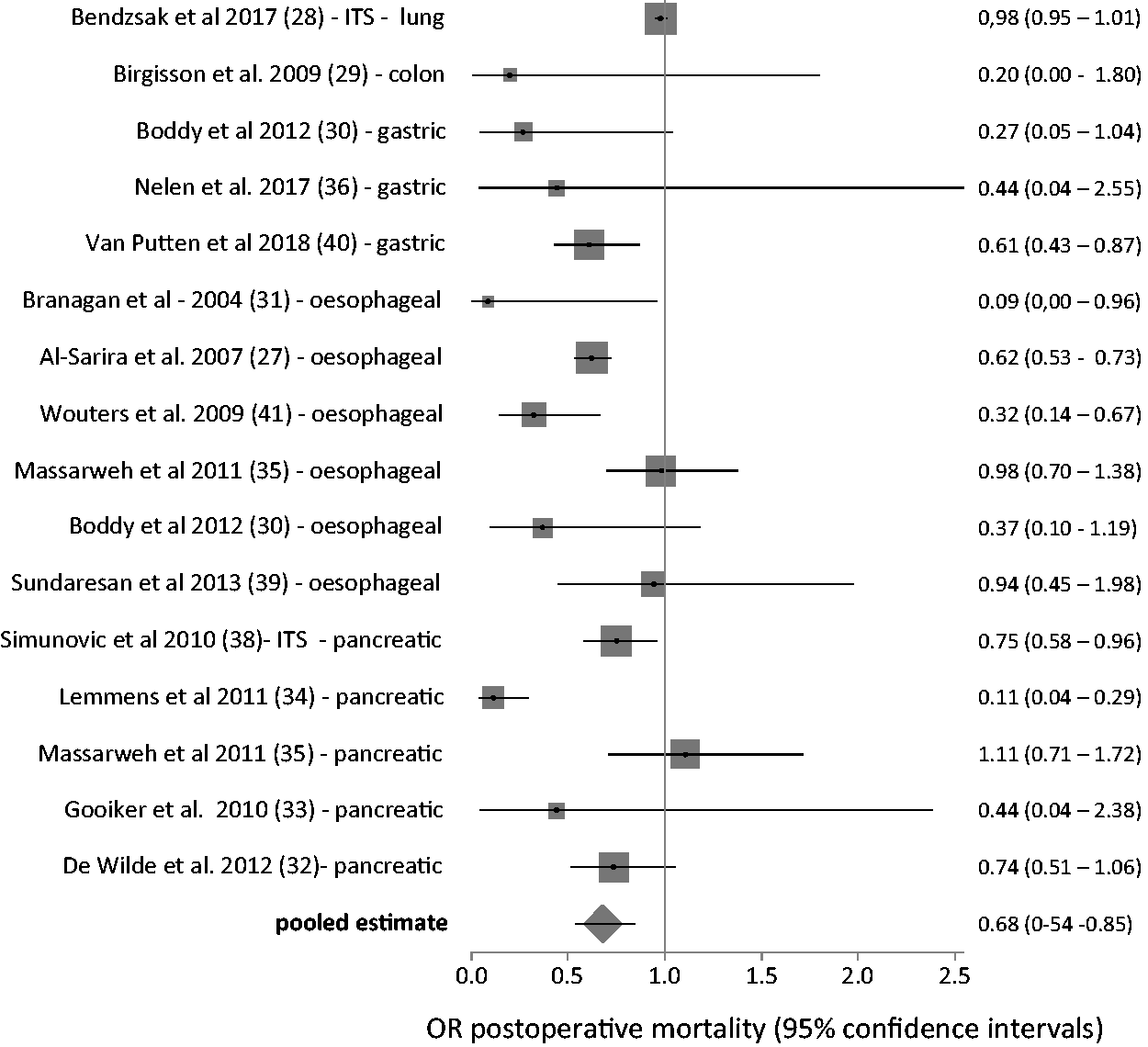
Forest plot of odds ratios (with 95%CI) from studies assessing the effect of centralization policies on postoperative mortality rate after cancer surgery.
We estimated pooled odds ratios for the subgroup of studies of pancreatic cancer, gastric cancer and oesophageal cancer surgery at 0.63 (95%CI: 0.39–1.01; I2 = 76%), 0.57 (95%CI: 0.42–0.79; I2=66%) and 0.63 (95%CI: 0.44–0.91; I2 = 64%), respectively. Figure 2 compares these estimates with those from published meta-analyses of studies comparing postoperative cancer surgery mortality at high and low volume hospitals.19–24 This suggests that, overall, our pooled estimates of the effect of centralization policies are, with one exception, consistently more conservative, with a relative reduction of the risk of postoperative death much lower than the benefit expected from comparing high and low volume hospitals.
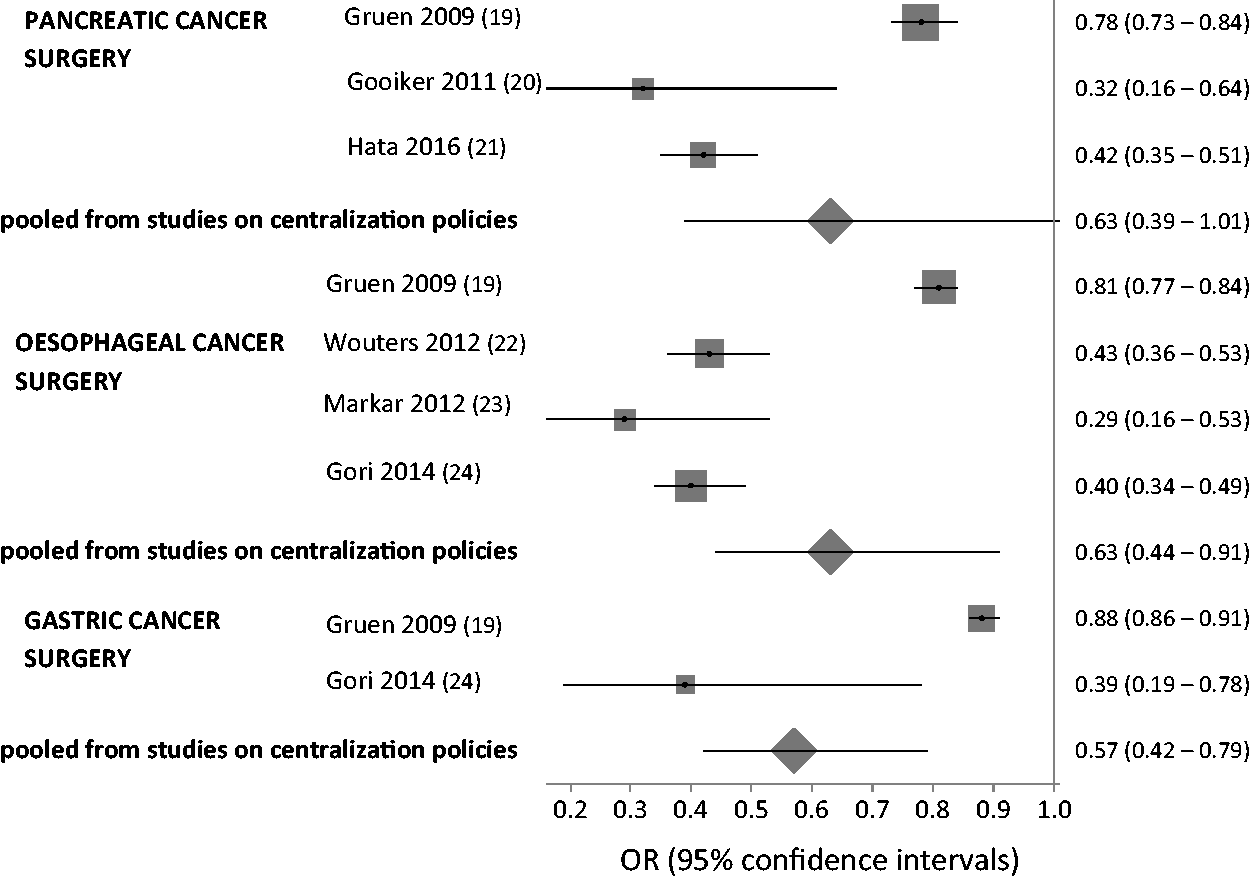
Forest plot comparing pooled estimates for postoperative mortality following centralization policies for cancer surgery with published estimates of meta-analyses of postoperative mortality following surgery at high versus low volume hospitals for pancreatic, esophageal, and gastric cancer.
Relationship between the degree of centralization and postoperative mortality
A total of 26 studies contributed 48 observations (Table 2) to the meta-regression analysis of the relationship between degree of centralization of cancer surgery and postoperative mortality.
Characteristics of 26 studies reporting concurrent changes in the degree of centralization of cancer surgery and in postoperative mortality.
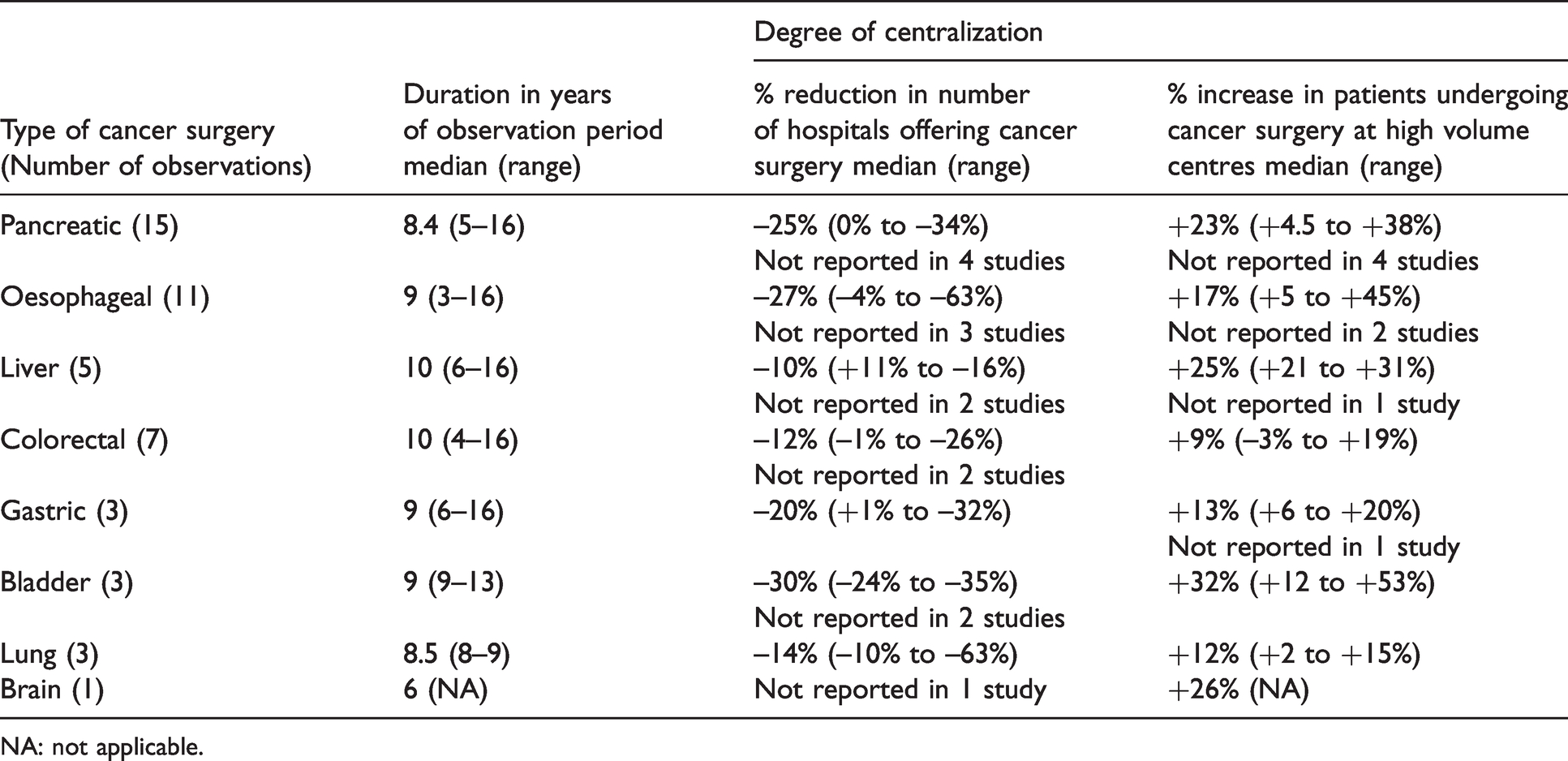
NA: not applicable.
Results of the random-effects meta-regression analysis of the relationship between the degree of centralization of cancer surgery and concurrent changes in postoperative mortality (expressed as natural logarithm of the pre-post odds ratio of postoperative mortality rates).

As shown in Table 3, both variables that we used as proxy for the degree of centralization achieved over an individual study’s time span had negative (and statistically significant) correlation coefficients, indicating that an increase in the degree of centralization was associated with a greater reduction in postoperative mortality. The second model which used the proportion of patients treated at high volume hospitals explained a greater proportion of the variation observed across studies in postoperative mortality reduction, as indicated by the R2 statistic. Inclusion of dummy variables for type of cancer surgery did not improve the model.
Figure 3 plots the findings of the meta-regression of the increase of the proportion of patients treated at high volume hospitals and the natural logarithm of the odds ratio. Assuming a baseline postoperative mortality risk of 5%, the estimated coefficients suggest that a 20% increase in the degree of centralization could account for a 2% reduction in the risk of postoperative death following surgery.
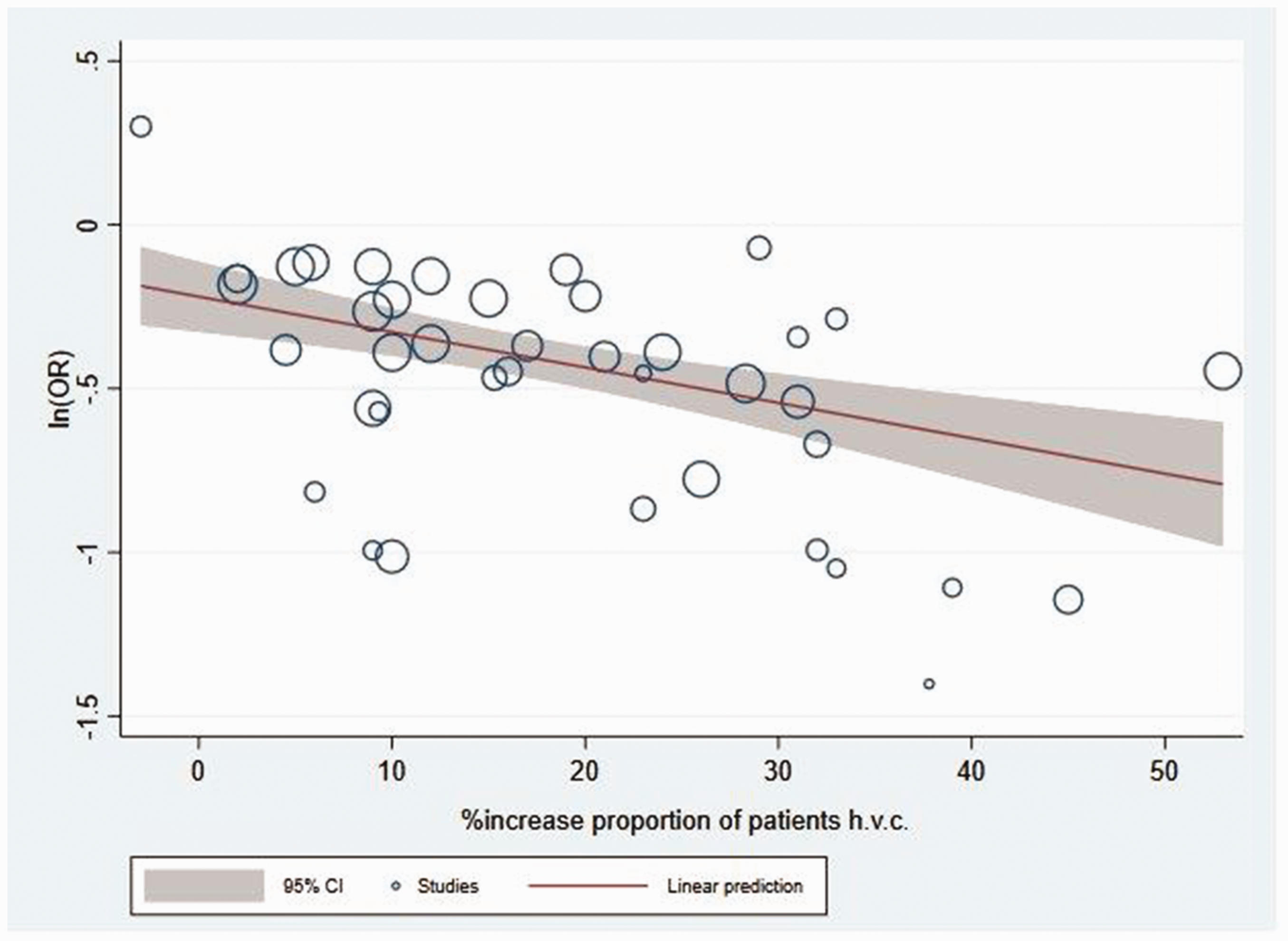
Bubble plot showing the relationship between increase of the proportion of patients receiving cancer surgery at high volume centers (hvc) and size of the reduction in postoperative mortality observed in each individual study (expressed as LnOR). The size of the bubbles is proportional to the precision of the study.
Discussion
To the best of our knowledge, this is the first systematic review of prospective studies of the impacts of centralization of cancer surgery on postoperative mortality. Overall, our findings support the benefit of centralization of cancer surgery, estimating a 32% relative reduction in the risk of postoperative death following the introduction of related policies. Furthermore, we estimated that a 20% increase in the degree of centralization can be linked to a 2% mortality reduction. This estimate is higher than the 1% reduction estimated in a recent study of centralization of surgery for pancreatic and oesophageal cancer. 42 We were unable to explore differential effects of different centralization approaches because of the small number of published studies.
Our findings draw, largely, on before-after studies without control, which means that our estimates likely overstate the ‘true’ impact of cancer surgery centralization. This is exemplified by two included studies evaluating the same cancer centralization strategy in Ontario, Canada, with Bendzsak et al. 28 using a more robust interrupted time series design unable to confirm the positive association found by Sundaresan et al. 39
However, while our pooled estimates of the relative risk reduction that may be attributed to centralization of surgery for gastric, oesophageal and pancreatic cancers may be inflated, they appear to be more conservative than estimates derived from meta-analyses of cross-sectional studies on the volume-outcome relationship for those cancers.20–24 There are many reasons why this could be the case. The most important being that centralization of surgery is often only one of the many factors that impact on cancer outcomes, along with general improvements in clinical and organizational management and in surgical techniques. Indeed, studies that sought to quantify the contribution of centralization to reducing postoperative mortality found that only about 50% of the observed effect could be attributed to centralization initiatives.43–45 This highlights the importance of the wider quality improvement context within which centralization efforts are embedded. This is illustrated in a comparative study of two Canadian provinces of which only one introduced formal centralization policies, and which found that while both provinces saw an increase in the number of patients seen at high-volume hospitals, a concurrent reduction in postoperative mortality only occurred where other quality improvement initiatives were implemented alongside centralization. 38
Strengths and limitations
Our systematic review of has a number of limitations. First, pooling estimates of effect from uncontrolled before-after studies is likely to reinforce biases of that study design but we deemed meta-analysis a useful approach to explore whether observed effects from longitudinal studies are comparable with those studying the volume-outcome relationship by means of cross-sectional designs. Furthermore, estimates from before-after studies tend to be biased in magnitude rather than in direction of effect and results from before-after studies included in our meta-analysis pointed consistently towards a mortality reduction linked to centralization efforts. Second, we used in-hospital or 30-day mortality following cancer surgery as short-term clinical outcomes as indicators of the actual performance of surgical interventions. However, centralization may impact on other relevant outcomes not considered in our review, such as disease-free survival, patient access to surgical care and costs. Third, we cannot exclude the possibility that our literature search missed some relevant studies. For example, we excluded studies published in languages other than English, although this limitation was previously shown not to affect the conclusions of meta-analyses. 46 We found evidence of publication bias, suggesting that smaller studies presenting negative results are missing, which could have influenced the results of our meta‐analysis. Finally, a small number of included studies focused on several types of cancer surgery, which added more observations to our analyses. However, we do not believe that this influenced our findings as observations related to different patient samples receiving different types of surgery should be independent of each other.
There is urgent need for more detailed data to help understand the benefits of developing centralization policies and of effective strategies for their adoption. In particular, there is a need for more reliable estimates of the expected benefits from such efforts, given the likely implementation challenges that relevant policies might face, such as provider resistance, along with associated costs and possible impacts on patient access to surgery. 3
Conclusions
Our review of prospective studies found evidence of beneficial effects of centralization of cancer surgery on postoperative mortality although our estimates are lower than those reported in cross-sectional volume-outcome studies of cancer surgery. Our review provides tentative evidence that centralization policies should be embedded into wider cancer quality improvement efforts to improve outcomes after surgery. There is urgent need for systematic evaluation of centralization policies for cancer surgery using robust study designs, alongside better reporting of the nature and scope of policies being implemented to inform policy development.
Supplemental Material
sj-pdf-1-hsr-10.1177_13558196211008942 - Supplemental material for The effects of centralizing cancer surgery on postoperative mortality: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-hsr-10.1177_13558196211008942 for The effects of centralizing cancer surgery on postoperative mortality: A systematic review and meta-analysis by Roberto Grilli, Federica Violi, Maria Chiara Bassi and Massimiliano Marino in Journal of Health Services Research & Policy
Footnotes
Acknowledgements
We are grateful to Prof Trevor Sheldon for comments and suggestions provided on an earlier version of the paper.
Declaration of conflicting interests
The author(s) declare(s) that there is no conflict of interest.
Ethics approval
Ethics approval was not required for this systematic review.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support to this project was entirely provided by the Azienda USL-IRCCS of Reggio Emilia.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.