
Abstract
Objective
To evaluate patient experiences with a remote Colon Capsule Endoscopy (CCE) service delivered through the 5G-SUCCEEDS initiative, utilizing the InteliGI Smartbox for home-based diagnostics with remote clinical supervision.
Methods
This mixed-methods service evaluation involved 25 patients referred from primary care with low-to-intermediate colorectal cancer risk, or under post-polypectomy surveillance. Patients received a Smartbox with CCE equipment, including a capsule, receiver belt, and a tablet for remote videoconferencing with clinical staff. Data on patient experience, confidence, and satisfaction were collected through surveys and semi-structured interviews. Twenty-two participants returned the questionnaire, and eight completed semi-structured interviews. The Nonadoption, Abandonment, Scale-up, Spread, and Sustainability (NASSS) framework was used for thematic analysis.
Results
Analysis of the technology showed that most patients rated the Smartbox as user-friendly, with bowel preparation noted as the most challenging aspect. Analysis of the value proposition of the innovation showed that most patients expressed satisfaction with remote CCE. Videoconferencing was essential for ensuring correct equipment setup and providing patient reassurance. Patients valued the convenience of performing the procedure at home, with most able to continue their daily activities. Analysis of the adopter system found that most patients reported that they did not need any assistance from a family member or a nurse while doing the procedure.
Conclusion
This study indicates the patient acceptance of home-delivered CCE through the 5G-SUCCEEDS initiative. The results suggest that remote CCE, supported by 5G technology and the InteliGI Smartbox (or alternative), offers a viable and patient-centred alternative to in-clinic colonscopy procedures.
Introduction
Evaluation of patients with lower GI symptoms (low-intermediate risk group) represents significant pressure for colonoscopy services. The COVID-19 pandemic, and the resulting elective care recovery, has placed significant pressure on healthcare systems. 1 The aerosol generating potential of endoscopy led to multiple gastroenterology and endoscopy clinical societies suggesting immediate cessation of all but emergency colonoscopy during the peak phase of the pandemic, putting colonoscopy capacity under greater stress and reducing the rates of colorectal cancer diagnosis.1–4
To reduce potential diagnostic delays, the accuracy and role of colon capsule endoscopy (CCE) as a non-invasive diagnostic test is being increasingly recognised.5,6 In centres with availability, the European Society of Gastrointestinal Endoscopy and European Society of Gastrointestinal and Abdominal Radiology suggest that CCE may be considered in patients with ‘non-alarm' symptoms as an alternative to colonoscopy, although further evidence is needed. 7 In the English National Health Service (NHS), a national pilot has recently been completed to evaluate CCE as a first-line diagnostic test for patients with a positive faecal immunochemical test (FIT).8,9
As well as the burden on healthcare systems, patients have also reported finding the colonoscopy procedure uncomfortable. Difficulties encountered by patients included anxiety, the anticipation of pain, and feelings of embarrassment and vulnerability. 10 CCE allows for colonic assessment by eliminating the need for instrument insertion, gas insufflation or sedation along with associated pain. In CCE, after laxative bowel cleansing, patients swallow an ingestible pill-like capsule containing miniature cameras that travels through the gut providing full images of the bowel. The imaging data is sent to a data receiver which the patient wears on a belt.
At present, in settings performing CCE, patients are required to attend a clinic location, usually attended by one healthcare professional. In the clinic, patients are fitted with the receiver belt and a healthcare professional supervises oral administration of the disposable capsule. University Hospitals Coventry and Warwickshire NHS Trust (UHCW), a teaching hospital in England, has conducted a small-scale feasibility study of a home delivery service with patient self-administration of CCE,
11
facilitated by 5G technology and the widespread use and proliferation of videoconferencing in people’s day-to-day life, work and healthcare since the COVID 19 pandemic.
12
Called 5G-SUCCEEDS ( The InteliGI smartbox.
The primary objective of the 5G SUCCEEDS feasibility study of 25 participants was to assess the feasibility of home delivery of CCE service.
11
This paper reports on the patient experience and acceptability of undertaking CCE at home with a focus on: • Patient perspective - levels of confidence, satisfaction, convenience, and experience of the service. • Patient acceptability and preferences. • Emerging learning to inform other deployments of CCE home delivery service.
Methods
Baseline characteristics.
Twenty five patient participants were recruited to the feasibility study. As part of the recruitment and consent process, participants were offered a choice between colonoscopy and CCE. Participants were informed that CCE is a diagnostic procedure, that polyps cannot be removed during CCE, and that follow-up colonoscopy might be required if the examination was incomplete or pathology was detected.
All 25 participants of the 5G SUCCEEDS study were asked to complete a paper survey, given to them with the InteliGI Smartbox and returned along with the Smartbox following completion of the CCE procedure (see online supplemental table 1). A convenience sample of patients (based on time and resources) were approached by their clinician by telephone to invite them to participate in an interview. Patient information sheets were supplied to participants and participants provided verbal consent to a written consent form that was read to them over the telephone. If consent was given, an appropriate interview time was agreed with an evaluator. Questionnaires were completed immediately after the CCE procedure and returned with the equipment the following day, whereas interviews were conducted weeks to months later, after participants had been informed of their CCE results.
Interviews were conducted and recorded either via telephone or Microsoft Teams, depending on patient preference. Interviews lasted between 21 and 50 min. One participant requested that their partner listen in to the interview to assist with participant recall, the other interviews were conducted one-to-one with the interviewer. Patients were interviewed once between 1 and 7 months (following approval of the patient experience sub-study by the Research Ethics Committee) after their CCE procedure by a female independent evaluator, (C. Conway, PhD) commissioned from an NHS consultancy to capture patient experience. The evaluator was unknown to the patients prior to being consented by their clinician. Semi-structured interviews were conducted using a topic guide based on the topic guide used by Bond et al., 13 and adapted to consider the differences in the services being evaluated (online supplement).
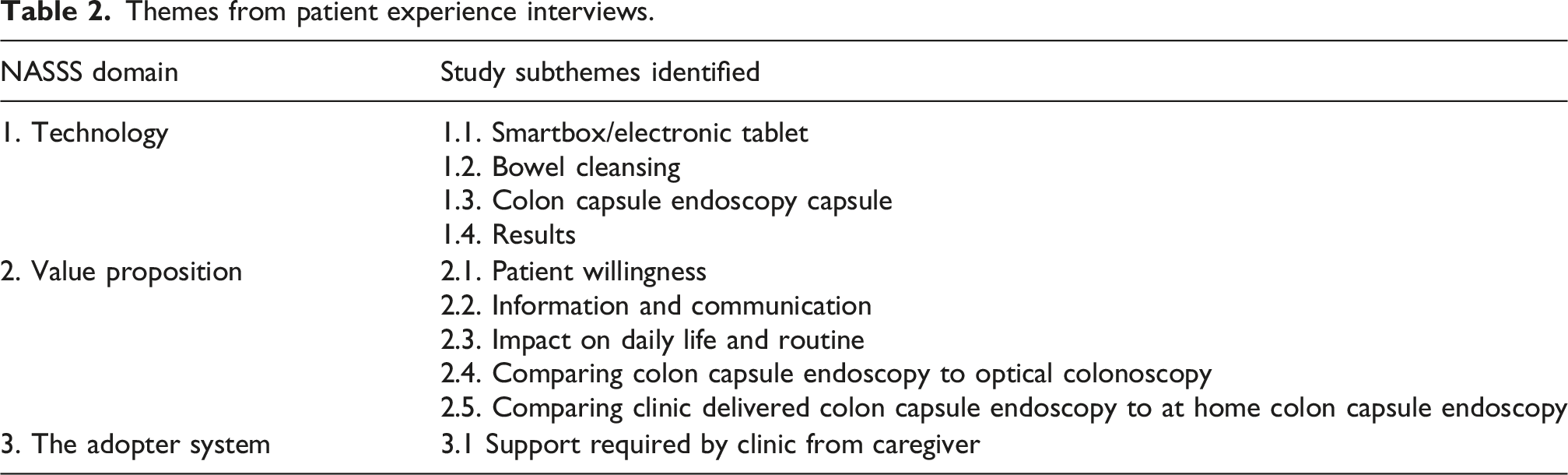
Interview recordings were transcribed and imported into a qualitative data management and analysis software package (NVivo 14, Lumivero). The evaluator reviewed transcripts for accuracy before analysis. No transcripts or analysis were returned to participants for comment. The evaluator used the same thematic coding strategy as Bond et al., 13 whereby the nonadoption, abandonment, scale-up, spread, and sustainability (NASSS) framework’s constructs 14 were used as a priori themes for organising and coding the data. The NASSS framework allows exploration of the data in the following domains: condition or illness, technology, value proposition (perceived value of service), adopter system (comprising professional staff, patients, and lay caregivers), organisation, wider (institutional and societal) context, and interaction and mutual adaptation between all these domains over time. 14 Transcripts were also coded inductively with subthemes identified and created in NVivo.
Results
Respondents and response rate
Between December 2022 and September 2023, a total of 25 patients participated in the 5G-SUCCEEDS study. Following CCE, 18 out of 25 participants (72%) required further investigation, due to the discovery of polyps (n = 10, 56%), or an incomplete CCE exam (n = 8, 44%). Completeness of the CCE examination was defined as achieving a comprehensive video recording of the colon and rectum with adequate cleansing.
Of the 25 patients who received the CCE home delivery, 22 (88%) participants returned the questionnaire with the CCE equipment. Reasons for not returning the questionnaire are not known. Eight patients (32%) participated in semi-structured interviews with an independent evaluator. Two patients that consented to participate in an interview dropped out before they were interviewed due to being too busy to identify a suitable interview time. The summary of the findings presented in this paper includes responses from both the completed surveys and the semi-structured interviews to understand patient experiences and acceptability of CCE home delivery. Out of the eight participants in the semi-structured interviews, half (n = 4, 50%) had previously had a colonoscopy before they participated in the study and five participants (63%) went on to have an additional colonoscopy procedure (Online Supplemental Table 2). Overall, 25 patients participated in the study; 22 returned the questionnaire and eight completed semi-structured interviews. Of the total cohort, seven patients were cleared following CCE, ten had polyps detected, and eight had an incomplete CCE examination requiring further investigation.
Analytic framework
Themes from patient experience interviews.
Technology
InteliGI Smartbox/electronic tablet
InteliGI Smartboxes (Figure 1) were sent by courier to the patient’s home address. Deliveries were scheduled to arrive at the end of the working day and collection for mornings before working hours, with patients describing this as well-organised and convenient. Eighty-two percent of respondents rated the Smartbox as extremely easy (n = 11) or easy (n = 8) to use. Patients received a phone call from a nurse/clinician the same evening to go through the Smartbox, bowel prep and the procedure. Patients found this contact helpful and reassuring.
Along with the bowel preparations, recorder belt and colon capsule, the Smartbox contained an electronic tablet to enable a nurse from Corporate Health International (CHI; the Smartbox producers) and the UHCW clinician to videoconference with the patient the day of the CCE procedure. This visual contact was to ensure that the patient was able to swallow the capsule and to check the belt and recorder and other equipment were set up and worn correctly. Patients described the videoconference call with the clinicians as ‘essential’ to ensure that clinicians could view how the patients had set up the belt and holster and to provide confidence and reassurance to swallow the capsule with 64% of patients describing the video instruction as extremely clear (n = 14) and 32% (n = 7) describing it as very clear.
Bowel cleansing
Seventy-seven percent of respondents reported the use of bowel prep to be very easy (n = 10) or easy (n = 7). However, in interview, patients described the bowel cleansing as the worst part of the procedure. All the patients described the CCE bowel prep/boosters as having an unpleasant flavour, and some struggled with the volume of liquid that they needed to swallow. Many patients however described it as a ‘means to an end’ and were prepared through the information they were given, having experienced previous similar procedures (colonoscopy), and through conversations with friends and family. However, patients that went on to have a colonoscopy described the preparation for colonoscopy as being less arduous.
15
Patients reported being glad to be at home and close to toileting facilities during the bowel cleansing. You're a lot more comfortable in your own space and your own bathroom and stuff like that, rather than, you know, being in a medical room with a toilet at the side…In hospital, I always feel someone's waiting outside until you're ready, you know, whereas you can sort of go, you know, that things happen at your own pace really. [Patient interview #1]
CCE capsule
Most patients talked about the capsule being bigger than they thought it would be and being daunted about swallowing it. The capsule’s flashing light also put off a couple of patients. However, patients were surprised by how easy it was to swallow with all participants reporting the capsule being extremely easy (n = 15) or easy (n = 7) to swallow.
Most of the respondents reported no discomfort at all during the process (55%, n = 12). Others reported that they experienced some discomfort (scores of 1 (n = 8) or 2 (n = 2) on a scale of 0-5). It is unknown which aspect of the procedure was the cause of this discomfort. However, we know from the interview data, the bowel cleansing was the aspect patients described as being the most difficult, with patients describing the capsule as easy to swallow, the belt as unobtrusive and with no patients reporting any pain or discomfort passing the capsule.
One of the patients described not knowing when they had passed the capsule with two others saying they only knew because of the flashing light on the capsule. Two patients described being worried about the potential for the capsule to get stuck but were reassured by clinicians. Some patients reported the continuing fasting, during the capsule passage, as being difficult.
Results of CCE
Following the CCE, 18 out of 25 participants underwent further testing, while 7 participants (28%) did not require additional examinations. Out of the sample of patients that were interviewed, five of the patients went on to have a colonoscopy either because polyps were identified or because of an incomplete exam (n = 2). Completeness of the CCE examination was defined as achieving a comprehensive video recording of the colon and rectum with adequate cleansing.
Patients were given information about how long it would take to receive their results. Out of the eight patients interviewed, three patients described a negative experience with getting their results either due to mixed communication on whether follow-up treatment was required; insufficient explanation about why follow-up investigations were required; or results taking longer to come than previously communicated.
Two of the patients interviewed (20%) expressed a lack of confidence in the efficacy of CCE to detect issues within the colon/bowel. The lack of confidence for one of these patients appeared to be centred around the misapprehension that the technology was also being trialled in this pilot, not just the mode of delivery.
Value proposition
Acceptability and satisfaction
Patients reported overall being either very satisfied (n = 15 (68%)) or satisfied (n = 7 (32%)) with the remote CCE procedure. Patients described viewing the CCE at home as an ‘easy’ option, avoiding the potential discomfort and invasiveness of a colonoscopy, and performing the entire procedure in the comfort of their own home rather than having to go to a hospital/clinic.
Most patients reported they would be very likely (n = 12 (55%)) or likely (n = 6 (27%)) to have remote CCE if clinically indicated in future. Three patients (14%) reported they were neither likely nor unlikely and one patient (4%) said they were unlikely. Six out of the eight patients interviewed would choose CCE home delivery again if they required an investigative diagnostic procedure and would recommend the service to family and friends, even though four of these patients did go on to require a colonoscopy due to failure of the colon capsule to capture all the data needed (n = 1 (of these six patients)) or removal of polyps. One of the other two patients would choose CCE over a colonoscopy but would prefer clinic-delivered CCE due to perceived safety reasons. The final patient would choose a colonoscopy – for this patient the CCE procedure failed (the colon capsule did not pass through in time) and the patient struggled with the bowel prep. I suppose I was a bit apprehensive about what actually was gonna happen, apprehension rather than, sort of, the fear you have when you go into hospital. I think it was nice, thinking I’m going to be at home, and I can just carry on with whatever I’m doing, so that was quite comforting. – [Patient interview #6]
Information and communication
As this procedure was self-administered, levels of confidence in undertaking the procedure were important. Several points of anxiety prior to the procedure were identified; not being able to swallow the capsule; setting up the equipment wrongly; the capsule passing too quickly/too slowly; questions during the procedure/error messages from the belt. However, the information and communication provided before and during the procedure alleviated these anxieties. There were three different points of communication with clinical staff: (1) initial phone call by nurse specialist after receiving the Smartbox, (2) teleconference with nurse specialist and doctor to set up belt and holster and to swallow the colon capsule (3) nurse specialist available to call/text while the capsule transited the digestive tract.
Patients were very positive about the information and the communication they received. With the level of communication provided, patients, in general, felt confident in doing the procedure at home and found the contact they had with clinical staff to be reassuring. The teleconference with clinicians during the procedure was viewed as essential to ensure that the equipment (especially the belt and holster) had been set up properly, to provide reassurance about swallowing the capsule, and to address any concerns/questions patients had about the procedure and what to expect. Those interviewed that did contact the nurse specialist found this helpful and reassuring.
Impact on daily life and routine
The majority of patients reported that they managed to continue with daily activities while having the capsule endoscopy (n = 19 (86%)). The patients that were interviewed had all taken time off work or ensured they did not have to leave the house for the day of the CCE, describing needing to be near toileting facilities. However, while at home, for most people, the procedure did not interfere with them doing other activities in their home/garden. A few of the patients felt, in retrospect, they may have been able to do their job if they had chosen to once the laxative had finished. However, most described how they would not have felt comfortable leaving their home. Those that went on to have a colonoscopy described the colonoscopy as taking a full day outside of their home environment where they would not be able to get on with their routines.
Comparing CCE to optical colonoscopy
Some patients described ‘dreading’ the prospect of having a colonoscopy and a CCE being a less intrusive option, easier to perform, and in the comfort of your own home. Patients also described losing more time with colonoscopy because of the sedation involved and having less freedom to do as they choose in a hospital environment.
Comparing clinic delivery of CCE with at-home CCE
Patients talked about the convenience and comfort of doing the entire procedure in their own home and close to their toilet facilities, as well as not having to travel (especially if suffering with other health problems), the anxiety of going to hospital, parking and associated costs. One patient said they probably would prefer (if required in the future) to take the colon capsule in a clinic rather than at home. They described they would feel safer at a clinic in case something went wrong.
The adopter system
Part of the NASSS framework looks at ‘the adopter system’ i.e., the staff, patients, and caregivers who will deliver/receive the technology. While Bond et al., 13 did not code any data to the adopter system theme, theirs was a clinic -managed service delivery model which did not place as much responsibility on patients for their own care (or require specific support from a family member or friend). The home-delivery service for CCE was self-administered (albeit with telehealth/videoconferencing support from a clinical team) and patients participating in the pilot required a person with them on the day of the procedure who was able and willing to help in case the patient choked while swallowing the colon capsule. This required more from patients and caregivers than the clinic-managed service.
The majority of patients (n = 18 (82%)) reported that they did not need any assistance from a family member or a nurse while doing the procedure. In the interviews, we probed patients about the support they had at home and whether they felt it was needed. None of the patients interviewed experienced any difficulty swallowing the colon capsule. One of the patients interviewed was not able to have anybody physically supporting them at home but would have been able to telephone their partner, a nurse, if needed. The other seven patients did not describe any difficulties in finding somebody willing to be with them during the procedure. Of these seven patients, four said that the support at home was not needed whereas the other three did require that support but for different reasons; one patient needed help to get through the bowel prep; one patient needed help to fit the belt and holster correctly; one patient needed moral support to swallow the capsule.
Discussion
Findings from a survey and interviews with 25 patients were that the home delivery and self-administration of the CCE procedure was acceptable, and for most, preferable to both a colonoscopy and clinic-delivered CCE. Benefits included convenience and comfort of being in their own home and close to their toilet facilities, avoiding any anxiety associated with attending a hospital setting, and the greater convenience and reduced costs of not having to travel, Most patients reported they would be very likely (n = 12 (55%)) or likely (n = 6 (27%)) to have remote CCE if clinically indicated in future. In the 5G-SUCCEEDS study, a high proportion of patients (n = 18, 72%) went on to require further investigations either because the CCE was of insufficient quality (poor bowel preparation) or because positive findings demanded a therapeutic procedure. 11 The conversion rate into a colonoscopy pathway is not static between different studies, and clinicians acknowledge that this could be as low as 28%. 11 A previous meta-analysis of patient preference had found that tolerance of both CCE and colonoscopy was high and that while patient preference before having either procedure favoured CCE, the preference for colonoscopy is much higher after the procedure, indicating that the expectations for colonoscopy may be much worse than the actual experience. 16 The authors suggest that if the tolerance is very high for both, the risk of two examinations following a positive CCE could be considered too high. 16 We probed this in the interviews with participants that required further investigations. Of those interviewed, only one participant who had experienced a colonoscopy after CCE would choose a colonoscopy as a first choice if indicated in the future. The other four would still choose at-home CCE if there was the possibility they could avoid colonoscopy, demonstrating a high patient preference for at home CCE over a colonoscopy for investigative procedures. Patient experience and acceptability should be interpreted within the broader diagnostic pathway, particularly where follow-up colonoscopy is required following incomplete examinations or detection of pathology.
While most respondents reported the bowel preparation to be either very easy (n = 10) or easy (n = 7) to use, like Bond et al., 13 the interview findings revealed negative experiences with the bowel preparation for CCE. Most patients viewed the bowel prep as an unpleasant procedure but a means to an end. Any improvements that could be made to the taste of the preparations, or to reduce the volume, would improve patient experience of the bowel prep.
Patients felt confident carrying out the procedure in their home but identified that visual confirmation from clinicians (via teleconference) was essential during the procedure to ensure that the belt and recorder were set up properly, something that patients reported they might struggle with, or feel anxious about, on their own. Improvements to simplify the appearance and wearability of the belt and data receiver might reduce the necessity for clinical contact for larger scale-up in the future. All the patients found the electronic tablet device simple to use, even those that did not have any previous experience of teleconferencing. To participate in the 5G SUCCEEDS pilot, patients were required to have a minimum of 3G coverage in their home and be IT literate. The interviews with patients suggested that the level of IT literacy required was minimal, and future roll-out expansions may want to test this latter requirement.
No patients reported any issue swallowing the capsule, even though the capsule was larger than they expected. Five out of the eight patients interviewed said that support of a person with them was not needed. The reported number of capsule aspirations for capsule endoscopy is very low. 17 For future roll-out and scale-up, consideration might be given to the necessity of having a support person, to enable the procedure for people without access to support. Any removal of this eligibility requirement would have to consider the risks of capsule aspiration.
Once the capsule had been swallowed patients felt able to get on with activities of their choosing, wearing the belt did not particularly interfere with them going about their routines. However, where applicable, patients had taken some off work and the day of the procedure and almost all patients did not leave their home, wanting to be close to toilet facilities. Many felt in retrospect that they might have been able to work but a larger study would be needed to elucidate any potential benefits on patients’ ability to continue to work while receiving home delivery of CCE.
The unlimited (all hours) access to contact a specialist nurse was appreciated and used. Future roll-out will need to consider the level and provision of remote clinical support that can be provided if the service were to be scaled up, in the context of what is currently provided for clinic-managed delivery of CCE.
Receiving results was an area where patient expectation was not always met, with one patient experiencing mixed communication about whether a follow-up colonoscopy was required, and another being informed they needed a follow-up colonoscopy without explanation. Two patients expressed lacking confidence in the technology to detect problems in use. There may be scope to develop protocols/guidance in reporting the results of CCE where these are not already in existence with consideration to including information on the efficacy of CCE as this may offer reassurance to those patients. This should be balanced against the environmental impact of such investigations in line with the NHS Greener plan. 18 While cost-effectiveness and willingness-to-pay were not assessed in this study, perceived convenience and value were important themes and may inform future economic evaluations of home-delivered diagnostic services.
Limitations
The study’s small sample size and single-centre design limits the generalizability of the findings. Demographic characteristics and digital literacy were not analysed within this patient experience sub-study, limiting assessment of differential experiences. Reliance on self-reported data might introduce response biases. Although the patients that took part in the study were positive about the experience and articulated a preference for remote CCE over traditional colonoscopy procedure, this sub-study has not explored the reasons that patients might have decided not to take part in the 5G-SUCCEEDS study.
Supplemental material
Supplemental material - Patient reported outcomes of home diagnostics with colon capsule endoscopy – results from the 5G-SUCCEEDS study
Supplemental material for Patient reported outcomes of home diagnostics with colon capsule endoscopy – results from the 5G-SUCCEEDS study by Cassie Conway, Gohar Jalayeri Nia, Chander Shakher and Ramesh P Arasaradnam in Journal of Health Services Research & Policy
Footnotes
Ethical considerations
This study was approved by the Health Research Authority (HRA) and Health and Care Research Wales (IRS number:311685). This study was conducted in accordance with Good Clinical Practice and the Declaration of Helsinki. All participants provided written informed consent.
Author Contributions
Cassie Conway and Gohar Jalayeri Nia are joint first co-authors.
Cassie Conway contributed to study coordination, data collection, project administration and manuscript preparation.
Gohar Jalayeri Nia contributed to study design, patient recruitment, delivery of the colon capsule endoscopy pathway, drafting and revision of the manuscript.
Chander Shakher contributed to clinical oversight, and critical manuscript review.
Ramesh P Arasaradnam contributed to study conception, supervision, interpretation of findings and critical revision of the manuscript.
All authors reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data available upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.