
Abstract
Objectives
People with disabilities have worse health outcomes than people without disabilities, leading to a 10–20-year life expectancy gap. Health workers’ attitudes and lack of training are barriers to health care for people with disabilities, yet current training initiatives are unsystematic and limited to specific cadres or institutions. Countries that have adopted the UN Convention on the Rights of Persons with Disabilities likely have legal obligations to train health workers on disability. We sought to explore how this obligation is included in disability laws and policies in sub-Saharan Africa, as this is an important indication of activities to close the health gap for people with disabilities.
Methods
We searched the two available databases on disability laws: WHO MiNDBANK and UN websites for disability laws and policies for each country to systemically extract information across 11 domains.
Results
57 documents in English, French, and Portuguese from 31 countries were included. No relevant documents were found for 18 countries. Of the most recent document for each country, nearly half (n = 16, 52%) had no mention of disability training, while the remaining countries required or mandated it (n = 15; 49%, respectively). Most laws and policies had limited details, though more robust ones had information on budget allocation, competencies, and cadres included.
Conclusions
Therefore, several countries in sub-Saharan Africa include health worker training in disability laws, but more detailed policies could improve disability training initiatives.
Background
Globally, there are 1.3 billion people with disabilities. Estimates of disability prevalence in sub-Saharan Africa vary by context and age group, ranging from 6 to 7% amongst children across sub-Saharan Africa 1 to 10% amongst those five and older in the Western Cape, South Africa 2 and nearly 40% amongst older adults in Ghana. 3 Many people with disabilities experience barriers in accessing health care, 4 leading to a 10-20 year gap in life expectancy amongst this population. 5 Health worker attitudes, stigma, and poor training is frequently cited as one of the key barriers for people with disabilities to access healthcare,.6,7 Indeed, a systematic review of healthcare barriers for children with disabilities in sub-Saharan Africa and surveys in four African countries identified inadequate training and communication with health workers as a major barrier to delivering high quality health services for this population.8,9 While health worker training is not the only solution to improving health systems for people with disabilities 10 health worker training is seen by people with disabilities as viable solution for narrowing this gap 11 and is one of the 40 actions for health equity for persons with disabilities recommended by WHO. 12
Over the past two decades, international organisations and laws have also increasingly called for more disability training for health workers through global pledges and commitments. For example, Article 25(d) of the UN CRPD specifies health worker training as a means of improving health equity and quality of care for disabled people. 13 Regionally, the African Union has protected the rights of disabled people through the African Disability Protocol, which mandates several stipulations in regards to the right to health. Several clauses of Article 17 of the African Disability Protocol address stigma, discrimination, and health worker training, informing the importance of this topic in African countries’ disability laws. 14 Accordingly, several countries in sub-Saharan Africa include disability training in their national disability laws, committing to this central component of improving health for disabled people. National laws are essential to recognise these binding commitments and implement the guiding international conventions and regional protocols that countries sign onto. Countries, therefore, have a domestic and international legal obligation to deliver disability training for health workers by ratifying these treaties and protocols. However, there are limited examples of disability training for health workers in sub-Saharan Africa in the literature. 6
While there is an important distinction between laws and policies and implementation of training, laws and policies are nonetheless important to examine to understand the legal requirements that exist in countries. Legal requirements are more useful to examine than curricula, as the unsystematic approach to trainings mean there are no standardised curricula to asses. Focussing on laws therefore provides a more reliable and comparable basis for analysis across settings. Similarly, examining how national disability strategies have incorporated disability training can be insightful for how countries implement policy in practice and how individual governments have conceptualised their obligations under UN CRPD. To date, most analysis of disability laws has focused on how these laws support inclusive education for disabled children. 15 However, very little research has examined the right to health within these laws or determining countries’ obligations to deliver health worker training.
Methods
Using the READ approach 16 for document analysis, which involves systemically selecting and extracting data according to a framework, we examined the laws and policies of 49 countries in sub-Saharan Africa. The laws, policies, and strategies were sourced from two reference frames that have comprehensive records of existing disability laws: WHO MiNDBANK (More Inclusiveness Needed in Disability and Development) and UN Department of Economic and Social Affairs (UN DESA) webpages. Additionally, one author (TS), familiar with in-country contexts, provided documents for Zimbabwe that had not been updated on WHO MiNDBank. First, we searched for each country’s page on the WHO MiNDBank, 17 which includes countries’ national policies, strategies, and laws on mental health, substance abuse, disability, general health, human rights, and development. This database was then cross-referenced with the UN DESA Disability Strategies and Action Plans by Country webpage, 18 as well as their Disability Laws and Acts by Country webpage. 19 These existing databases provided a standardized way of accessing recorded laws, policies, and strategies, to reduce bias from using other search engines unsystematically or encountering potential language or geographic biases. There were no date or language restrictions applied. The databases did not provide date of updates, but since the databases were cross-referenced among available aggregated data sources, they were assumed to be up to date as of when they were searched (10 April 2026).
Each document was saved on the date of access and reviewed by two authors, including documents in French and Portuguese. An extraction framework was developed to count mentions of 11 specific aspects of training, including: (1) legal requirement (2) costs associated with delivering training, (3) length of training/time requirements, (4) competencies covered, (5) staging (e.g., when training is delivered in curricula), (6) training methods, (7) impairment type covered, (8) cadres involved in training, (9) benefits of completion, (10) objectives of training, and (11) methods of evaluation and monitoring. These categories were developed using the key elements of the trainings from a systematic review of interventions to train health workers about disability. 6 Data were then extracted for each aspect of the framework by one author and checked by a second author. An Excel-based extraction tool was used to summarise information and any disagreements were discussed by the authors. Finally, the extracted data were analysed by documents and by country (after selecting the most recent document) to infer trends in inclusion of disability training for health workers in disability laws, policies, and strategies. Documents were excluded if they pre-dated boarder changes (e.g., Sudan).
Results
Of the 49 countries included in the sample, 18 (37%) had no disability laws, policies, or strategies in any of the databases.17–19 In total, 57 documents were eligible for inclusion across 31 countries. Most countries had disability policies from post-UNCRPD implementation (i.e., 2006), while four had only documents from before 2000.20–23 Malawi and South Africa had the most documents at four each, while most other countries had a disability law only (Figure 1). Number of disability laws and policy documents by country.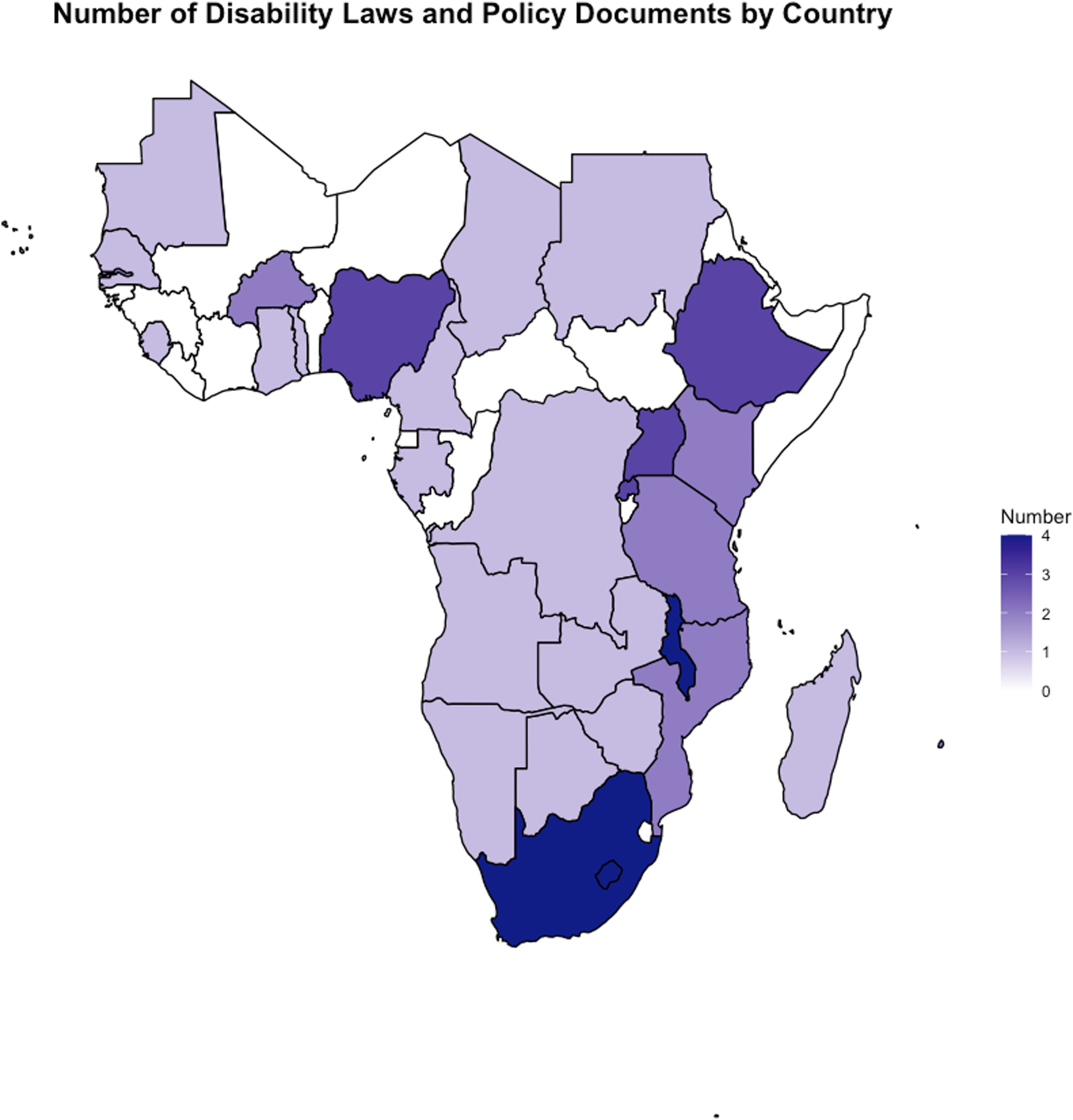
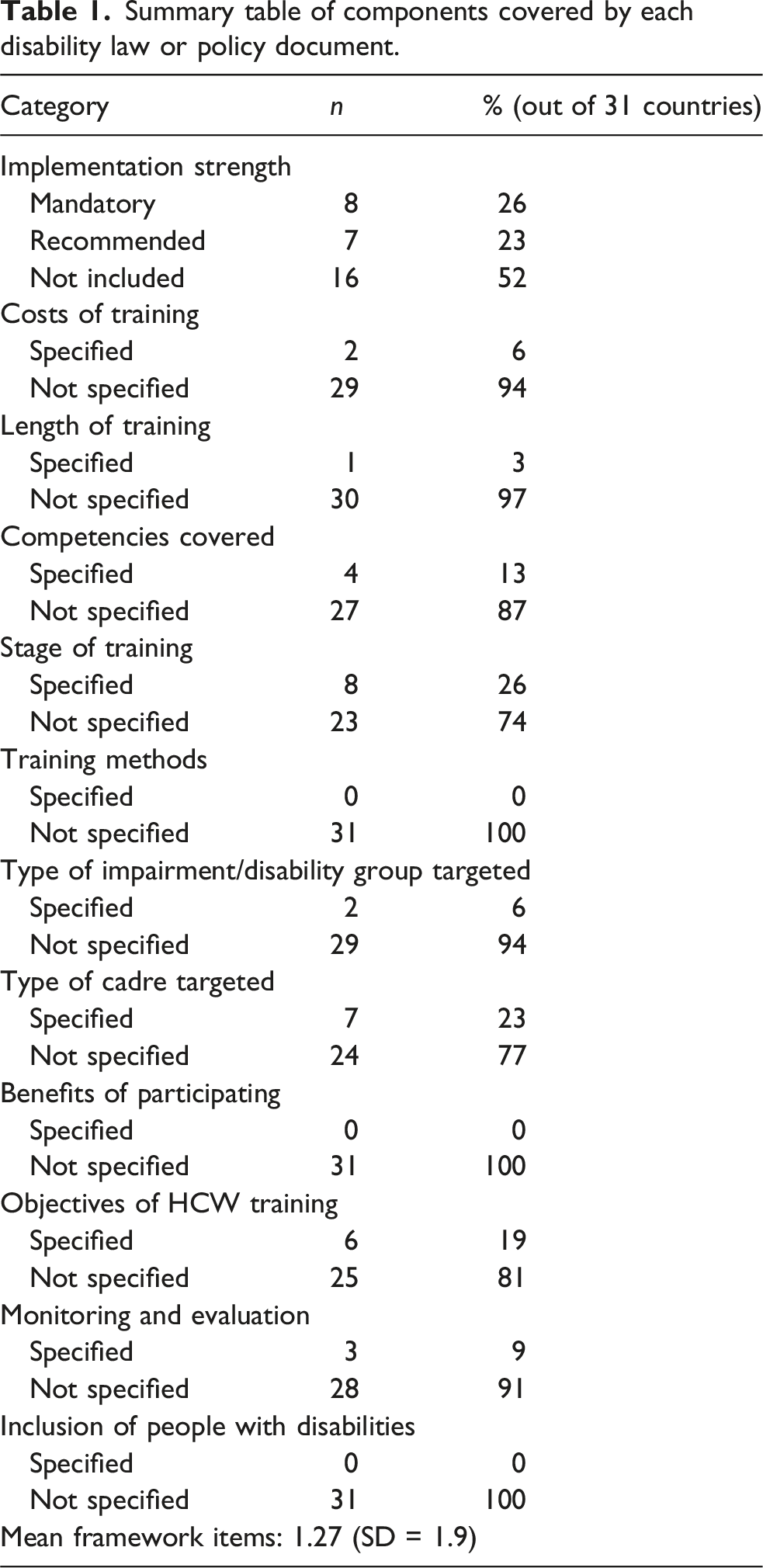
In terms of content, over half of countries with documents (n = 16; 52%) had no mention of disability training for health workers within their national disability laws or policies. Over a third of countries with documents recommended or mandated disability training for health workers (n = 15; 49%), with seven recommending (23%) and eight mandating (26%). 63% of the eight documents that mandated disability were laws, while language around recommendations were mostly in other documents (71%). Countries included a mean of 1.7 items from the framework (SD = 1.9), with most signalling the cadres that should be trained and the educational staging for training. Almost all countries mentioned the need to train health workers in the curriculum or through continuing professional development (CPD) for those already qualified. For example, in The Gambia, the law specifically mentioned integrating disability training into health programmes’ curricula and CPD for all current health and rehabilitation staff. 24 Ghana’s laws highlighted the importance of including training on general health and rehabilitative care for disabled people within training for health professionals and health care programs. 25 Sign language was highlighted as a competency that should be included in training in Lesotho, Malawi, and Uganda, but only Lesotho specifically included that health service providers such as nurses, doctors, and HIV testing and counselling (HTC) counsellors should be trained in sign language. 26 While most countries included broad cadres, such as “all health workers”, others adopted a narrower scope, limiting eligibility to specific groups such as rehabilitation staff or allied health professionals, as demonstrated by Ethiopia. 27 Policy and law details are outlined in Supplemental Table 1.
Nearly a fifth of countries’ laws and policies listed knowledge and skills acquisition as a primary objective of the training (19%), but Lesotho and Uganda also included sign language skills as the goal of training. Only two countries’ policies (6%) included a budget or cost of training; Malawi has one policy (National Disability Mainstreaming Strategy and Implementation Plan 2018-2023) which provided a specified budget (50 million MK; nearly £50,000 in 2018) and Sierra Leone’s Persons with Disabilities Act, 2011 stated the government would contribute to the budgets of institutions’ that trained health workers on disability. Kenya was the only country to have a report that mentions the length of training for rehabilitation staff (CRPD report - 3 years), while one of South Africa’s national policy’s (The National Development Plan 2030 Persons with Disabilities as Equal Citizens) makes it the only country to state methods and highlight the need for training to be led by people with disabilities themselves. Furthermore, few countries (6%) mentioned specific impairment types, except for Malawi (albinism) 28 and Lesotho (people with intellectual disabilities and d/Deaf and hard of hearing individuals). 26
Summary table of components covered by each disability law or policy document.
Malawi had substantial details about the specifics of training. For example, Malawi’s National Disability Mainstreaming Strategy and Implementation Plan 2018-2023 had the highest score of all documents analysed, with specific details in 73% of categories included in the framework (n = 8). This document emphasized disability training for health workers since access to health services was selected as one of the priority areas for the government. Accordingly, the policy specifies the budget and specific competencies (sign language, causes of disability, early intervention, assessment, and referral services), disabilities (albinism), health cadres (physiotherapists, orthopaedics, Dermatologists and ophthalmologists, HTC service providers), and objectives of the training (highlighted above).
Discussion
Our findings highlight the diversity of disability laws and policies in sub-Saharan Africa with respect to including clauses about training health workers on disability. Of the 49 countries, 18 countries lacked any disability legislation, and most adopted disability policies post-UN CRPD (2006). Over half of the countries did not address disability training for health workers in their laws or policies. Language around mandatory requirements were more common in legal documents, whereas recommendation was more common in other policy documents. While many countries recommended or required such training, the scope varied, with some focusing on broad cadres while others specified certain groups. Less than 10% of countries with laws had clauses that allocated budgets for training or mentioned evaluation plans for their laws. Malawi stood out for its comprehensive approach, including detailed training objectives, budget allocation, and plans for evaluation across its laws and policies. This comprehensiveness makes it a model within SSA, but further research is needed to understand the actual implementation and impact to ensure this is the correct approach to disability-inclusion within health worker training.
It is important to note that disability laws and policies may not be fully reflective of the full remit of activities related to disability training for health workers. There is a critical distinction between laws and policies and actual implementation; however, laws and policies are nonetheless important indications of how countries conceptualise and actualise their commitments to the health-related clauses of UN CRPD. Given that some of these laws and policies were enacted several years ago, it is possible that there are new governments in place, potentially with different priorities that may not include disability-inclusion and disability training for health workers, though many countries in sub-Saharan Africa have had the same political party or president in power for over a decade. 31 While these documents provided some evidence that there has been some attention to training to improve health equity for disabled people, the majority of these inclusions were minimally modified articles of UN CRPD (i.e., they copied the language of the UN CRPD verbatim or near-verbatim) and highlight this challenge in translating policy into practice. For example, in Ghana, the language of their Disability Act is similar to UN CRPD, yet there have been various successful individual disability trainings and interventions.32–34 While this shows how some institutions and individuals within countries have adopted the laws and policies into practice, it suggests that there remain gaps in universal adoption of the UN CRPD clauses.
Furthermore, most of the countries only listed information about the requirements for training, rather than in-depth content. The absence of disability action plans or policies adjacent to the laws may suggest that the laws themselves may not further these objectives. Whilst laws stated that disability training was required, this mandate does not necessarily translate to high-quality disability training. Countries with more detailed training descriptions within their laws may not necessarily produce better trained health workers. For example, Lesotho’s focus on sign language competency can be exceptionally beneficial for d/Deaf and hard of hearing patients, but this requires that health education systems have the capacity to teach all these individuals sign language. Therefore, having further documents that delineate plans, budget, and evaluation (i.e., Malawi’s mainstreaming strategy) can support disability training integration into the health worker education system. While this level of detail is important, it is also important to consider the opportunity cost to investing in training for only one impairment type, since this focus would not translate into effective service coverage for other impairment types (i.e., supporting blind and visually impaired people). That is not to say sign language and improving health worker communication with d/Deaf individuals is not important, but rather further studies should seek to understand what might be most effective and cost-efficient in delivering more disability-inclusive care to the broadest population of disabled people. For example, it may be more appropriate and cost-effective to have sign language interpreters available or have a few staff fluent in sign language and the rest trained on disability-inclusion, rather than expecting sign language fluency from all health workers. Adopting a competency approach—which was not done in most laws—may be a more optimal route for systematically training health workers, as it considers these challenges and offers a standardised, principled approach to training. For example, in India, the National Medical Commission of India has included a set of 8 disability competencies in their new curriculum to ensure all doctors are reached with the same skills to serve patients with disabilities. 35 Efforts to create global competencies for health workers are underway by WHO and will provide an important opportunity to harmonise and implement competency-based disability training around the world.
While laws and policies are essential tools for guiding actions and allocating resources, they are most effective when developed in collaboration with affected communities and relevant stakeholders. In many cases, the voices and experiences of disabled people, healthcare professionals, advocacy groups, and other stakeholders are not adequately incorporated into the policymaking process. 36 This limited engagement can result in policies that do not fully address the needs and priorities of those directly impacted by disability issues, leading to gaps in implementation and effectiveness. For example, whilst Malawi has made strides in development of policies aimed at addressing the healthcare needs of people with disabilities, challenges such as limited accessibility to healthcare facilities, a high unmet need for assistive technology and insufficient trained personnel remain.37–39 Therefore, future policy development efforts should prioritise inclusive and participatory approaches that ensure the meaningful involvement of all stakeholders throughout the policymaking cycle, from initial design to implementation and evaluation. By fostering greater collaboration and partnership between policymakers, people with disabilities, healthcare providers, and disability advocates, it is possible to develop more comprehensive and responsive policies that better address the complex challenges faced by people with disabilities in accessing healthcare services and achieving health equity.
There is a broader question of whether laws and policies are the appropriate place for such detailed inclusions. Laws and policies can be essential to trigger implementation and funding, or may be aspirational, without sufficient actions, meaning that their utility is undermined. For example, Malawi’s documents outlined a clear picture of the training topics, budget, and ministerial responsibilities for accountability. Since this level of commitment and planning was rare in the other reviewed documents, integration of disability competencies into health worker certification may be the more appropriate mechanism for improving health worker competency in these countries. Intervention at this level could enable certified health workers to be trained, examined, and refreshed on their competency in treating disabled patients. Therefore, further research should examine whether these competency, licensing, and Ministry of Health budget documents have greater potential for inclusion of disability than laws. This is particularly important since experimenting with this approach to licensing may trigger more stringent implementation of disability training for health workers. There is a pressing need for further research that delves into the specific provisions and implementations of disability laws and policies related to health worker training globally. Such investigations could offer valuable insights for policymakers, healthcare practitioners, and advocates striving to enhance the inclusivity and effectiveness of healthcare systems across the world.
Limitations of this study
One of the limitations of this study was the lack of comprehensive database from which to search for disability laws and policies and our lack of ability to cross-refence these with local policymakers. Funding for these databases to ensure they are up-to-date can help others learn from best practices in disability policy and legislation. Another limitation was the potential discord between the laws and policies and implementation on the ground. Further surveys and research may help illustrate what is happening in-practice regarding disability training for health workers to strengthen the evidence-based in this field. By design, we only examined laws and policies, but an analysis of medical, nursing, or other health worker curricula could elucidate more information about actual practices, since these activities could be happening regardless of whether they are legally mandated. However, since there is no comprehensive database of curricula, this was not possible to analyse for this study.
Conclusion
Laws, policies, and action plans often signal a country’s intent to change, provide background on specific interventions, or demonstrate values. While mandating, or even including disability training for health workers in laws, policies, and strategies may not necessarily translate into better health outcomes for disabled people, it can be an important step for further action. The policies of many countries in the sub-sample of sub-Saharan African countries have included clauses on disability training, but these lightly recommended actions with limited follow-up plans, strategies, or public funding mean that further work in this area is needed. Policies with specific implementation and monitoring plans need to be developed to financially support and expand health worker training on disability. Examining whether there are licensing requirements related to some form of disability-training would be helpful to understand how countries are implementing these laws.
Supplemental material
Supplemental material - Have we forgotten our obligation to train health workers on disability? A policy analysis in sub-Saharan Africa
Supplemental material for Have we forgotten our obligation to train health workers on disability? A policy analysis in sub-Saharan Africa by Sara Rotenberg, Veronika Reichenberger, Tracey Smythe in Journal of Health Services Research & Policy
Footnotes
Acknowledgements
The authors wish to thank Professor Sue Ziebland, Professor Sara Ryan, and Dr Emily McFadden for their feedback on the original draft.
Ethical considerations
Ethical approval for this type of study is not required by our institutions.
Author contributions
SR conceived the study, led extraction, and wrote the first draft of the manuscript. TS and VR acted as second reviewers. All authors contributed to and reviewed the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SR received funding from the Rhodes Trust for this work and receives salary support from the FCDO-funded Program for Evidence to Inform Action on Disability (PENDA) project. SR, TS, and VR are funded by an NIHR Global Research Professorship awarded to Professor Hannah Kuper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All documents are publicly available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.