
Abstract
We assessed the accuracy and reliability of teledermatoscopy with images taken by a general practitioner (GP) compared to face-to-face dermatological examination. GPs selected patients for teledermatoscopy and took both macro and dermatoscopic photographs. Patients were then referred to the local dermatologist for face-to-face examination. Accuracy and inter-observer reliability were calculated for the diagnosis and management plan. Image quality was rated by two observers on a three-point scale. A total of 108 teledermatoscopy consultations sent by 13 GPs were assessed by four dermatologists. Agreement was 0.61 (kappa) on diagnostic group and 0.23 on management plan. The inter-observer reliability was 0.65 on diagnostic group and 0.36 on management plan. The image quality was reported as bad in 36% of cases, reasonable in 28% and good in 36%. Agreement for cases with good quality images was 0.66 on diagnostic group and 0.42 on management plan. Teledermatoscopy in general practice had overall a lower accuracy and reliability than face-to-face consultation. In cases where a good quality image was reported, the accuracy increased, which emphasises that teledermatoscopy is highly dependent on a good quality images.
Introduction
The prevalence of melanoma continues to increase in Europe and The Netherlands.1–3 Since the therapeutic options for metastatic melanoma are poor, methods for early diagnosis, which will have a positive effect on the prognosis, are needed. Dermatoscopy is a technique often used by dermatologists, and increasingly in primary care, for early diagnosis of melanoma and other types of clinically suspicious skin lesions.4,5
Dermatoscopy is a non-invasive examination method. A dermatoscope is a lens with 10x magnification combined with either immersion fluid or light-emitting diode (LED) lighting with polarizing filters for glare reduction of the corneal layer of the skin allowing a clear examination of the entire epidermis and the superficial papillary dermis. The use of dermatoscopy by trained dermatoscopists increases diagnostic accuracy for pigmented skin lesions, especially for melanoma.6,7 Several review articles have shown teledermatology as diagnostically accurate and reliable for non-pigmented skin conditions.8–10 A recent study showed that teledermatology provided by general practitioners (GPs) contributes to more efficient and cheaper healthcare. 11
Diagnostic accuracy of dermoscopy and teledermatoscopy.
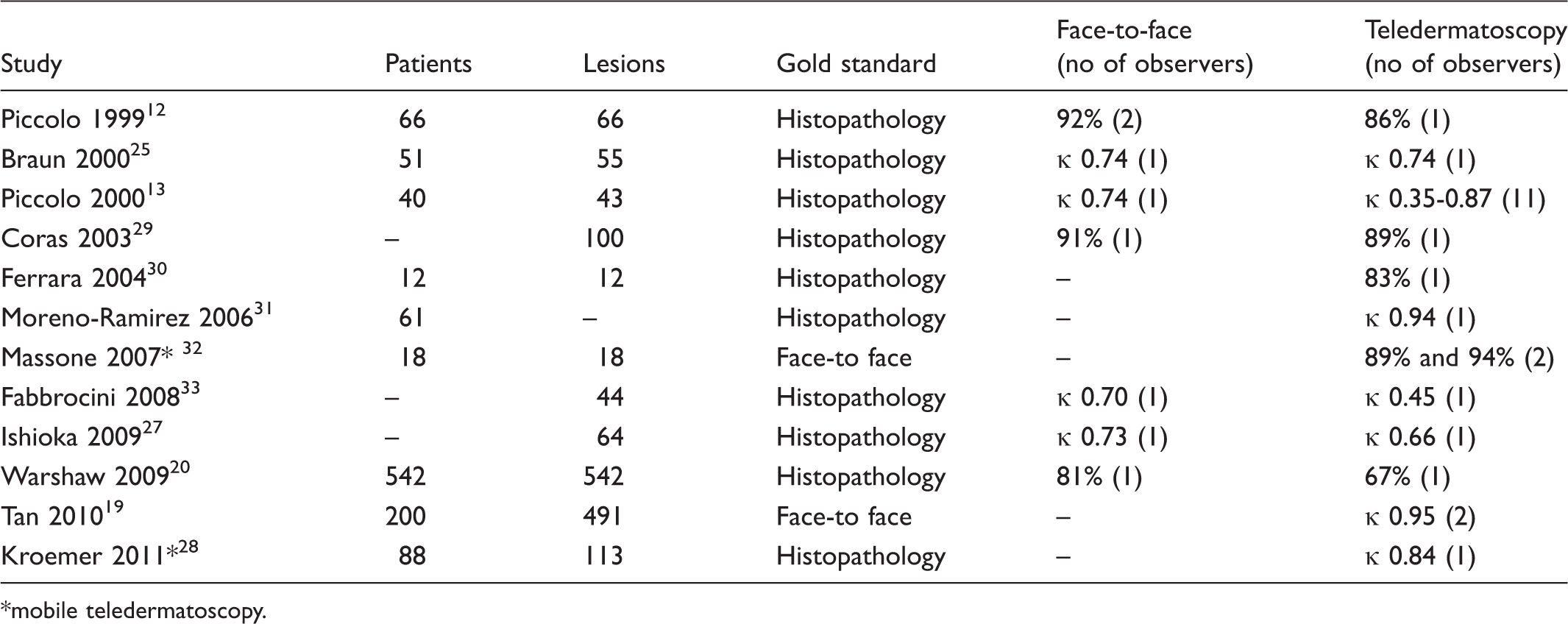
mobile teledermatoscopy.
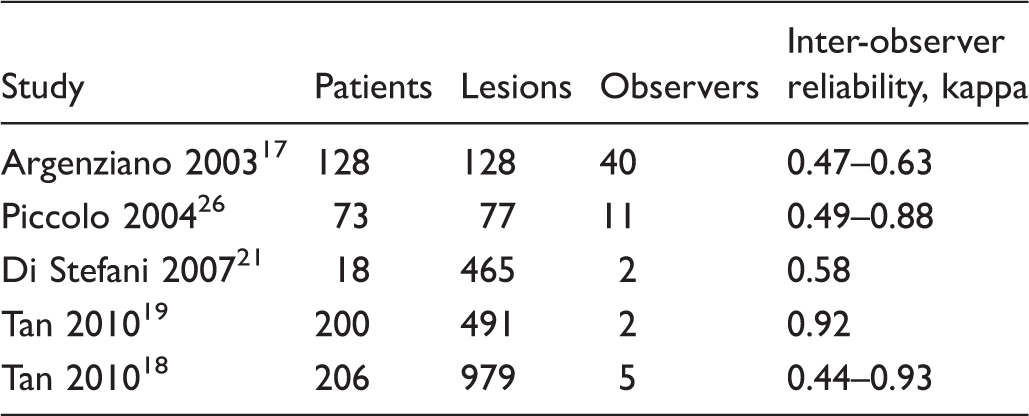
Diagnostic inter-observer reliability of teledermatoscopy.
Teledermatoscopy enables a diagnostic tool for clinically suspicious skin lesions to be used in the general practitioner’s practice. A recent study by Lim et al. reported on the first reimbursed teledermatoscopy triage service for skin lesions. 14 Instead of a live visit, patients could be referred to a commercially run virtual lesion clinic. The results showed that 88% of referrals to the dermatologist could be prevented and that access to a screening clinic was two-thirds faster for the teledermatoscopy patient group.
However, most studies on accuracy and reliability have taken place in a laboratory setting with a clinical photographer or a highly skilled dermoscopist with experience in taking dermatoscopic images. The aim of the present study was to assess the accuracy and reliability of teledermatoscopy with images taken by GPs applied during regular practice.
Methods
A digital camera (Cybershot DSC-W560, Sony, Japan) was used for all macro images of the lesions (camera setting: no flash, auto-focus, resolution 2048x1536 pixels, JPEG compression). The dermatoscope (3Gen DermLite Pro II HR, 3Gen, USA) was used with an adapter for the digital camera. A store-and-forward teledermatology consultation system (KSYOS TeleMedical Centre, The Netherlands) was used for the teleconsultations. 11 This system is integrated with all GP information systems in the Netherlands.
All participating GPs received a training course lasting one hour in using the teledermatology system and the camera and how to apply the dermatoscope in order to obtain a high quality image. During each teleconsultation the following information was recorded: patient identification information, medication, patient history (patient and family history of skin cancer), location of the lesion, recent changes in the lesion, sun exposure in hours during the last 3 months, estimated number of moles and skin type (Fitzpatrick scale), images and the questions posted to the dermatologist. Patient history and questions were free text. It was recommended that four images of the lesion (1 overview, 1 macro, 2 dermatoscopic) were included.
A teledermotoscopy consultation.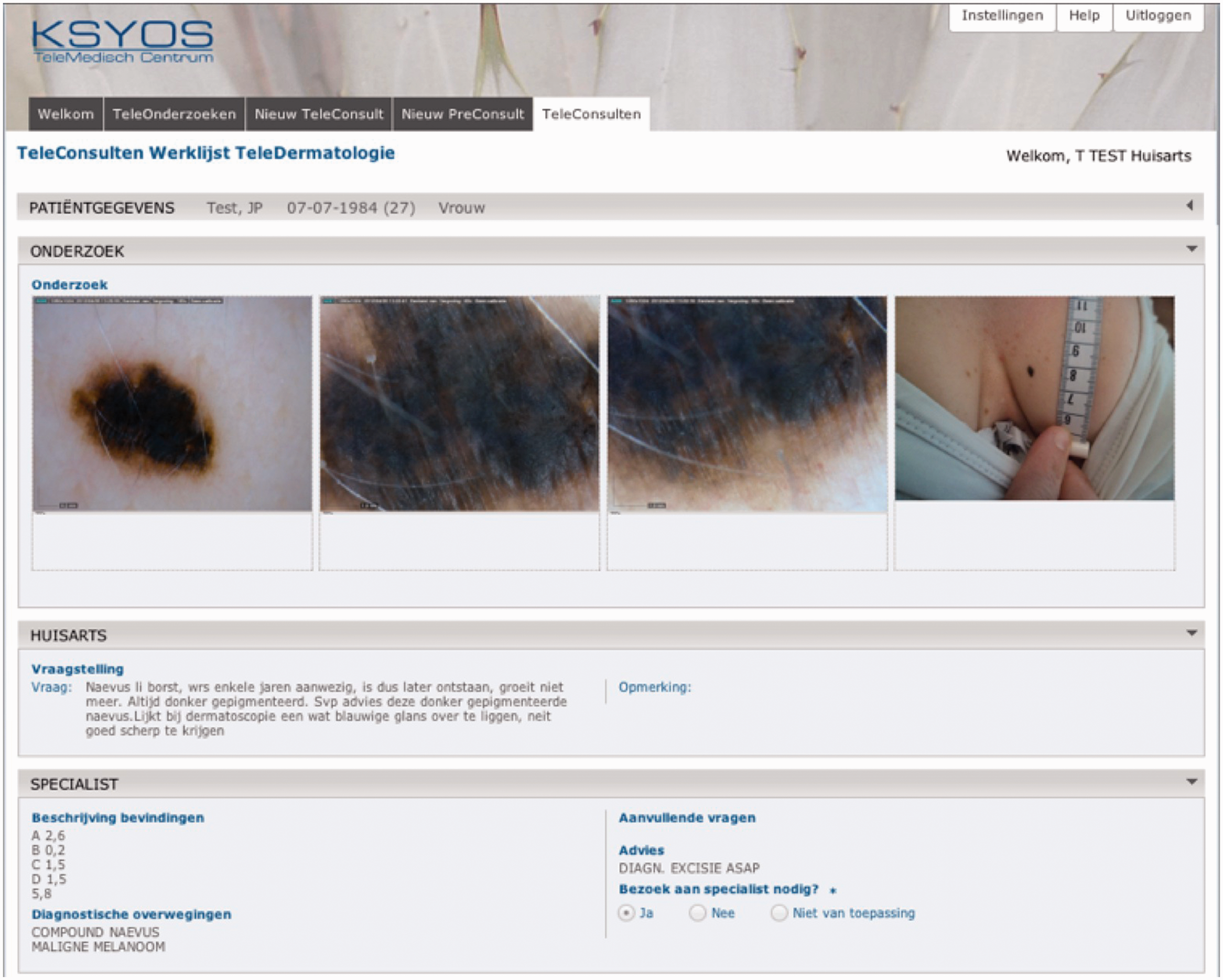
The dermatologists were required to answer a teledermatoscopy consultation within 2 working days. All patients who had a teledermatoscopy consultation were also referred to the local dermatologist (who was not necessarily the teledermatologist) for face-to-face examination. A histopathological examination was not mandatory, but depended on the decision of the treating dermatologist during the face-to-face consultation. As this decision was a standard care process independent of teledermatoscopy and extra costs for the patient were associated with histopathology, it could not be made mandatory. For those patients who did receive histopathological examination the final diagnosis was collected. The time between the teledermatoscopy consultation and face-to-face consultation was not more than 2 weeks.
Ethics permission for the study was not required. All patients were seen face-to-face by a dermatologist for the delivery of usual care.
Inclusion criteria
All dermatologists who participated in the study had a minimum of 5 years experience of dermatoscopy and 3 years experience of teledermatology. All GPs who participated had a minimum of three years experience using teledermatology, but no experience with dermatoscopy prior to the study. The participating GPs selected all consecutive patients who presented with a (pigmented) skin lesion and who were, in their opinion, suitable for a teledermatoscopy consultation. Urgent cases were excluded. Patients gave informed consent for the teledermatology consultation and its use for research purposes.
Statistics
Both accuracy and reliability were calculated using Cohen’s kappa statistic. 15 The kappa values were interpreted as: 0-0.20 as slight agreement, 0.21-0.40 as fair, 0.41-0.60 as moderate, 0.61-0.80 as substantial, 0.81-1.0 as almost perfect agreement. 16 Power analyses for an intraclass kappa test used the following values: 0.05 significance level, 2-sided test, 0.70 proportion successes, alternative agreement 0.80, null hypothesis agreement 0.40, power at 80% resulted in a sample size of 107 cases.
Accuracy
All teledermatoscopy consultations were assessed by four independent dermatologists, one of whom reported on the initial teleconsultation and three at a later time. Each provided a diagnosis blinded to the diagnosis of the other dermatologists and the three latter dermatologists also provided a management plan. The management plan consisted of four options: no treatment, excision, cryotherapy or topical medication. All diagnoses (face-to-face, histopathology and teledermatology) were assigned to an aggregated diagnosis group, see Table 3 (see XXXX, online archive) based on consensus decision. Diagnostic accuracy was calculated based on the outcome of the diagnosis group for all four teledermatoscopy assessments compared to the face-to-face assessment. Where histology was available it was compared with the four teledermatoscopy assessments and the diagnostic accuracy of the face-to-face assessment. Management accuracy was calculated between the teledermatoscopy assessments provided by the latter three dermatologists and the face-to-face assessment.
Inter-observer reliability
Inter-observer reliability (agreement between observers) was calculated between 4 dermatologists on the outcome of diagnosis group and between 3 dermatologists on management plan.
Image quality
The two most experienced dermatologists (>20 years of practice) of the four who assessed the teleconsultations independently rated the quality of the images provided in each teledermatoscopy consultation on a 3-point scale (bad, reasonable, good). If ratings differed for a case, the lowest quality rating was used.
Results
Between February 2010 and May 2011 a total of 108 teledermatoscopy consultations were performed by 13 GPs and reported by four dermatologists. The teleconsultations concerned 105 patients (3 patients had two lesions) with a median age of 47 years (range 6–84) and consisted of 55% females (n = 59). The number of excluded patients due to urgency is not known. Four images were supplied in 83 teledermatoscopy consultations, three, two and one image(s) in 17, 7 and 1 teledermatoscopy consultation, respectively.
Of the 108 lesions diagnosed through teleconsultation, 76 were seen face-to-face (70%). Table 3 shows the number of cases per face-to-face diagnosis. The face-to-face diagnosis was not available for the other 32 lesions for various reasons: the patient did not go to the dermatologist (n = 25), patient moved away (n = 6), GP did the excision (n = 1). A histopathological diagnosis was made for 36 lesions (33%), of which 35 also had a known face-to-face diagnosis.
Accuracy
The agreement between teledermatoscopy diagnosis and histopathology diagnosis was κ = 0.41-0.63. The agreement between the teledermatoscopy diagnosis and the face-to-face diagnosis was κ = 0.55-0.73. The agreement between face-to-face diagnosis and histopathology diagnosis was κ = 0.90. The agreement between teledermatoscopy management plan and face-to-face management was κ = 0.19-0.29. Histopathology diagnosed 7 cases as skin cancer (2 melanoma, 5 non-melanoma skin cancers); concordance of management plan for these 7 patients was 100%. All kappa values are shown in Table 4 (see XXXX, online archive).
Inter-observer reliability
Agreement for the 4 observers on the diagnostic group was κ = 0.56-0.78. Agreement for 3 observers on the management plan was κ = 0.31-0.38. The kappa values are shown in Table 4.
Image quality
The image quality was reported as bad in 36% of cases, reasonable in 28% and good in 36%. Accuracy for the teleconsultations with a good image quality rating between teledermatoscopy diagnosis and histopathology diagnosis was κ = 0.53-1.0. Agreement between the teledermatoscopy diagnosis and the face-to-face diagnosis was κ = 0.53-0.77. Agreement between face-to-face diagnosis and histopathology diagnosis was 1.00. Agreement between the teledermatoscopy management plan and the face-to-face management plan was κ = 0.34-0.47, see Table 4.
Reliability for teleconsultations with rated good image quality on the diagnostic group was κ = 0.48-0.79 and on the management plan κ = 0.33-0.57, see Table 4. Kappa scores for bad and reasonable image quality are also shown in Table 4.
Discussion
The aim of the study was to assess whether teledermatoscopy is equally accurate and reliable as face-to-face consultation when images are taken by a GP during everyday practice. The results showed a moderate diagnostic accuracy, a moderate diagnostic reliability, fair management accuracy and management reliability. However diagnostic and especially management accuracy was higher in cases with good quality photographs.
The diagnostic accuracy was lower than studies in which dermatologists or highly trained nurses provided the dermatoscopic images (Table 1). Management plan accuracy in other studies was higher than in the present study. A limitation on the accuracy estimation was the incomplete face-to-face diagnoses due to patients not visiting the dermatologist after the physical referral. For 70% (n = 76) of the cases a face-to-face diagnosis was available, and histopathology diagnosis was available in 33% (n = 36). There is a risk of bias (type 1 error), as the most probable reason that patients did not attend for face-to-face assessment was because their complaints had ceased or because they were adequately reassured (the telemedicine diagnosis for the 32 cases with no face-to-face assessment were melanocytic naevus (n = 19), seborrhoeic keratosis (n = 11), 1 lentigo and 1 mongolian spot). Face-to-face assessment of these more simple cases might have improved the overall accuracy. Few other studies that have been based on more than 100 cases can be compared with our results, as the images in those studies were all gathered in either a laboratory setting (by the researchers) or by a dermatoscopic nurse.17–20 Although no definitive conclusions on the outcome of accuracy could be made, our findings suggest that obtaining high accuracy from dermatoscopy applied in general practice is more difficult than in other settings.
The diagnostic reliability was similar to the upper end of reported reliability outcomes in teledermatoscopy studies (Table 2). Management plan reliability has been reported in one other study as moderate (κ 0.58) 21 and is thus better than in our own study. However, results on reliability (and maybe even accuracy when compared to face-to-face) may not entirely be ascribed to teledermatoscopy, as face-to-face diagnosis and management of skin lesions can differ among dermatologists as a result of different definitions of terms, lack of consensus guidelines, diagnostic drift and different perspectives on treatment. In contrast with teledermatology and teledermatoscopy, the literature on clinical inter-rater reliability in dermatology is scarce. The results on the reliability of clinical examination are similar to our own.22–24
Seven cases in the present study were high-risk patients (diagnosed with skin cancer). In these cases diagnostic and management accuracy was 100%. Other studies also show accurate diagnosis and management of high risk patients,12,13,21,25,26 but there are also examples of false negatives.20,27
Image quality was rated as good in only about one-third of the cases. This shows clearly that taking a good quality dermatoscopic image was difficult for the GPs participating in the study. Several reasons were reported:
Lack of time. GP practices were generally busy and overloaded, thus taking the time to take proper dermatoscopic images could have been difficult Lack of skills. GPs received training in the use of the equipment, but since suitable patients for inclusion did not present themselves every day, skills were lost over time Equipment problems. GPs reported failing/empty batteries in the camera and the dermatoscope, probably because of long intervals between uses. In addition, difficulties with attaching and detaching the adapter and focussing the camera with the adapter attached were reported.
Our study did not make a distinction between the image quality of macro clinical images and dermatoscopic images. In future research this distinction should be made as the clinical image can provide at least equivalent information for the diagnosis.
28
In cases where a good quality image was reported, the accuracy increased. This is similar to other studies (Table 1). This emphasises that teledermatoscopy is highly dependent on a good quality images.
Conclusions
The present study is one of the first to report on both diagnostic accuracy and reliability of teledermatoscopy applied in an everyday general practice setting. When teledermatoscopy is used in general practice under the conditions described in this study, it has mediocre image quality leading to an overall lower accuracy and reliability compared to face-to-face examination. However, high accuracy and reliability can be achieved under the right circumstances. Staff must be properly trained in acquiring high quality dermatoscopic images.