
Abstract
In 2009, we established a mobile ear-screening service for children in a remote community approximately 350 km north-west of Brisbane. We compared pre-implementation health service utilisation data (2006-2008) with data for the following three years. The study included only children in schools that had participated in screening since the start of the screening programme and for which data for the 6-year study period were available. In the baseline period there were 329 ear, nose and throat (ENT) outpatient appointments at the Royal Children's Hospital (RCH) in Brisbane for children from the selected catchment area. Of these, 166 (51%) were failure-to-attends (FTAs). In the following three years, there were 105 appointments, of which 40 (38%) were FTAs. In the baseline period, 100 children received surgical procedures at the RCH; in the following three years there were 43. In the three years following implementation, 136 children were booked to receive surgical procedures locally at the Cherbourg hospital, and 117 (86%) were completed. Since no other major health service changes occurred in the region during the study period, we conclude that the telemedicine-enabled screening service improved access to specialist care in the community and resulted in fewer outpatient and surgical appointments at the tertiary centre in Brisbane.
Introduction
In Queensland, ear health screening and intervention services for indigenous children are provided by the Deadly Ears Aboriginal and Torres Strait Islander Ear Health Service. 1 The services are provided primarily at the Royal Children’s Hospital (RCH) in Brisbane and occasionally during outreach visits. In certain cases, surgical procedures such as the insertion of grommets may be conducted during outreach visits, thus avoiding the need for travel to the RCH.
In 2009, we established a mobile telemedicine-enabled ear-screening service in the South Burnett region, a rural area about 350 km north-west of Brisbane with a population of approximately 1500 indigenous children. 2 The service was led by a trained indigenous health worker (IHW) who routinely travelled to and assessed children at 21 schools in the area. After each day of screening, the IHW uploaded clinical records to a secure database. Once a month, the ear, nose and throat (ENT) team at the RCH reviewed the screening results and devised treatment plans remotely. Outreach visits were carried out twice a year.
We have previously reported on screening activity and outcomes. 3 The aim of the present study was to examine whether the introduction of the telemedicine service led to changes in referral trends at the RCH and in the remote community.
Methods
Health service data for the three year period prior to the implementation of the mobile ear-screening service (2006-2008) were compared with data for the following three year period (2009-2011). Although the screening service commenced at the beginning of the 2009 school year, schools in the region were progressively included in the screening service over time. To ensure a valid comparison, the study included only children in the catchment area of schools that had been involved in the screening service since the start of screening and for whom data for all six years were available. These children were identified by having a residential address with the 4605 postcode (Cherbourg/Murgon).
Children from the catchment area who attended or failed-to-attend outpatient clinic appointments or had surgical ENT procedures at the RCH during the study period were identified from health service records. Similarly, children who had received a surgical procedure during an outreach visit to the region were identified. Data on failure to attend (FTA) for surgical procedures were unavailable. The study was approved by the appropriate ethics committees.
Results
The activity data pre and post implementation of the ear-screening service (see Figure 1) showed reductions in the number of patients travelling to Brisbane for an outpatient appointment (Table 1), and an increase in the number of specialist surgical services being provided in the remote community (Table 2).
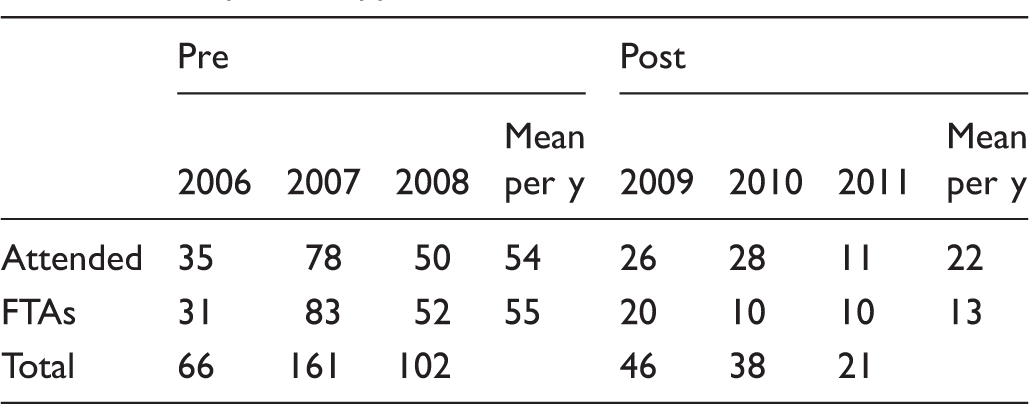
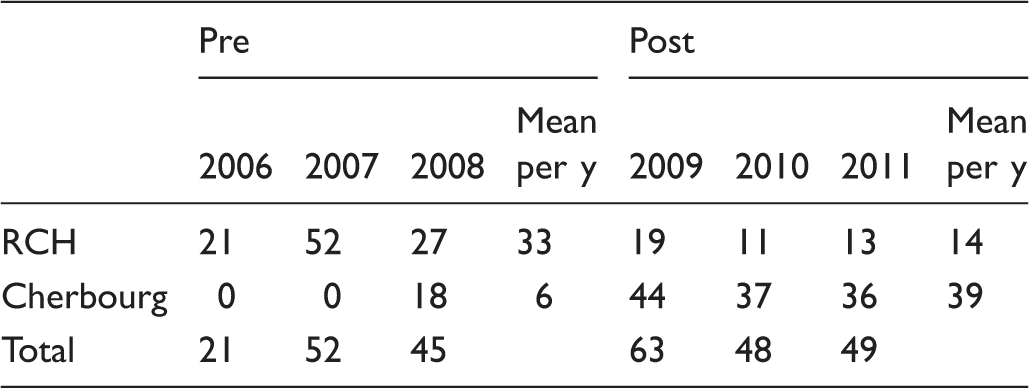
Number of ENT surgical procedures performed on children from the Cherbourg region, either locally or in Brisbane. Outpatient appointments at the RCH. Surgical procedures completed.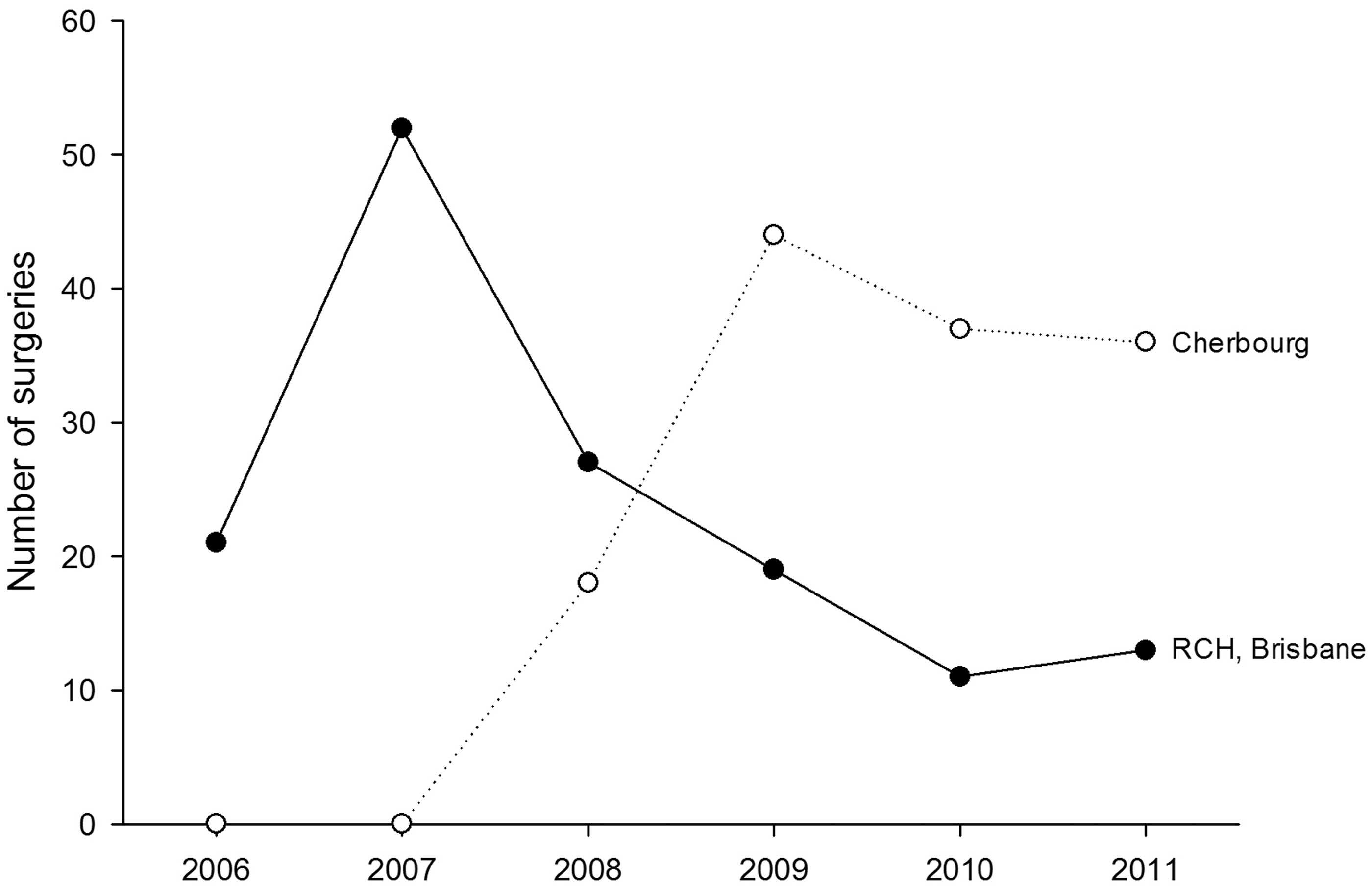
Outpatient appointments
From 2006 to 2008, 329 ENT outpatient appointments were arranged at the RCH for children from the selected catchment area. 163 children attended their appointment and 166 (51%) were FTAs. Post-implementation, the number of appointments arranged at the RCH reduced to 105, of which 65 children attended and 40 (38%) were FTAs.
Surgical procedures
The overall number of ENT surgical procedures conducted for children from the catchment area increased in the post-implementation period. There was also an increase in the number of surgical procedures being completed in the community and a reduction in the number of children attending an ENT surgical procedure in Brisbane.
The average number of ENT surgical procedures performed on Cherbourg/Murgon patients at the RCH from 2006-2008 was 33 per annum. During 2008-2011, an average of 14 surgical procedures were carried out per annum at the RCH, see Table 1. There was a 58% reduction in the number of children undergoing procedures in Brisbane, and a 550% increase in the number of procedures conducted by the ENT surgical team during outreach visits to the region.
In the three years following implementation, 136 children were booked to receive surgical procedures at the Cherbourg hospital by the outreach team. Of these procedures, 117 (86%) were completed, 11 procedures were no longer required, one was declined by the patient, three children left the area and two were rebooked for surgery at the RCH.
Discussion
After the mobile ear-screening service was established in 2009, there were marked increases in the number of children being routinely screened by indigenous health workers and assessed by an ENT specialist at a distance. More than 80% of children in the region are now assessed at least once per year for conditions which may affect hearing; and cases are reviewed by an ENT specialist within one month from time of referral.2,3
The present study examined the utilisation of ENT services for patients in the Cherbourg/Murgon community. The overall number of ENT surgical procedures for children living in the selected catchment area increased gradually during the six year period, and there were changes in the methods used to deliver these services. The introduction of the community-based mobile ear-screening service combined with a surgical outreach team visiting twice per year led to improved screening and reduced the need for families to travel to Brisbane for treatment.
Travelling long distances for a specialist appointment in Brisbane is difficult for people living in remote communities. It is also expensive, both for the families and for the health department in Queensland which subsidises a proportion of the travel costs.4,5 In addition to the potential cost reduction, the observed decrease in FTA rates is a positive outcome in terms of efficiency and utilisation of specialist resources. Other than the implementation of the mobile ear-screening service, we are not aware of any other health service related changes that occurred during the six year period that could account for the changes that we have observed. In particular, the population in the selected catchment area remained relatively stable (Figure 2).
Population in the selected catchment area (data from the Australian Bureau of Statistics).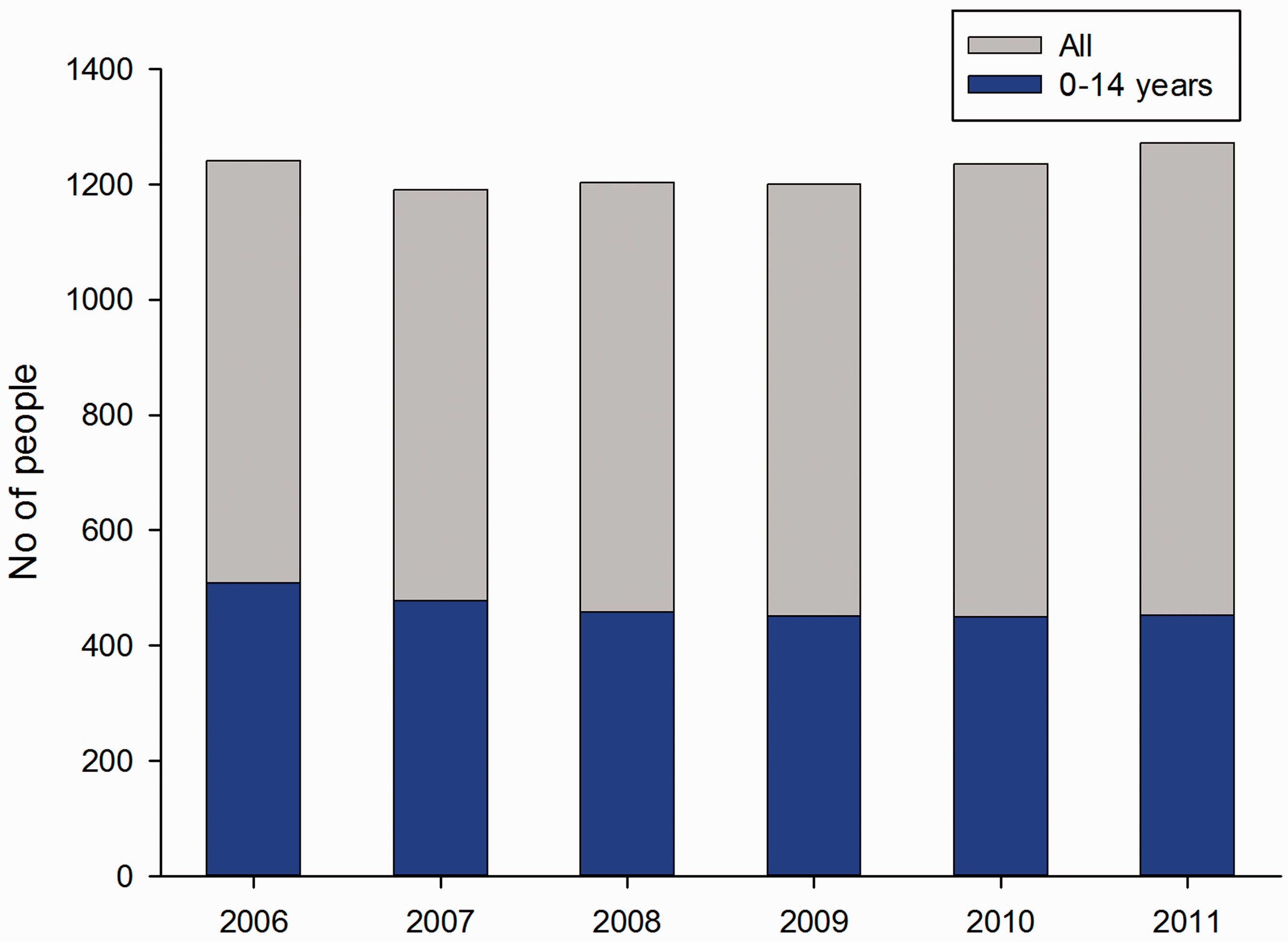
The factors which we believe have contributed to the success of the screening programme include ongoing community consultation and participation; strong indigenous leadership; close alignment with primary care services in the community; executive management and academic support; and accessibility. This is similar to other successful services which have been established for indigenous people.6,7
Conclusion
The results suggest that the mobile ear-screening service allowed the local assessment of children to be managed effectively within the community and helped to reduce the need for families to travel to the tertiary centre. Since no other major health service changes occurred in the region during this period, we conclude that the use of telemedicine improved access to specialist care in the community and resulted in a reduction in outpatient and surgical appointments at the RCH.
Footnotes
Acknowledgements
We are grateful for the support of the Cherbourg Aboriginal Community. We thank the following collaborators: Queensland Department of Health, the Cherbourg Community Health Service and the Deadly Ears Aboriginal and Torres Strait Islander Ear Health Service. We also thank Galen Elliot, Matthew Brown, Chrissie Stewart, Elizabeth Jacobs and Markeeta Ahsam. Start-up funding was provided through the Queensland Children’s Health Foundation by corporate and community sponsors. The service is funded by the Darling Downs Hospital and Health Service.