
Abstract
Background
Missed clinic appointments cause delays in treatment of other patients, under utilization of clinical manpower or facilities and impact upon hospital finances.
Aims
The primary aim of this study is to evaluate whether a text messaging reminder service reduces the Did Not Attend rate. The secondary aim is to evaluate the cost-effectiveness of a mobile text message reminder service.
Methods
The study focused on the outpatient department of a district general hospital. In January 2011 a patient text messaging reminder service was implemented across the outpatient departments in the trust. Data were collected prospectively 24 months prior and 24 months following the implementation of this service. A reminder was sent to patients one week prior to the scheduled appointment as a text message. All patients attending the orthopaedic department were included in the study. Patients who had an appointment and cancelled/rescheduled it prior to their original consultation date were excluded. Children were also excluded from the study.
Results
The overall Did Not Attend rate was reduced by 12% following the intervention (p < 0.0001). The new appointment follow-up rate was reduced by 2% (p = 0.74) and the follow-up rate decreased by 13.7% (p < 0.0001). The economic analysis revealed a saving of £19,853 over a two-year period following the intervention.
Conclusion
Thus mobile technology is a feasible tool in improving attendance rates at outpatient clinics and is economically viable.
Introduction
Missed clinic appointments lead to inefficiencies within hospital departments. Consequences include delays in treatment of other patients, under utilization of clinical manpower, whilst simultaneously impacting on departmental revenue as well as the overall hospital finances.
In 2011–2012 the National Health Service (NHS) conducted approximately 53 million outpatient appointments. Despite various efforts, there were still around 5.5 million missed clinic slots, 1 meaning that approximately one in 10 patients did not attend the hospital for their booked consultation. Costs of outpatient appointments can vary significantly but on average an appointment costs £100 to organize. The above figures translate to a £500m per year financial inefficiency. 1
Patients often have genuine reasons for not being able to attend their scheduled visit. However, research has shown that frequently it is caused by a patient's forgetfulness or miscommunication. 2 In order to address these issues several different modalities have been employed including appointment card reminders, telephone calls, email alerts and text messages.
A recent systematic review demonstrates a significant benefit of sending reminders prior to appointments to reduce the Did Not Attend (DNA) rate. It also interestingly found that manual phone calls were more effective than automated messages and there was no difference in DNA rate whether the reminder was sent a day or a week before the appointment. 3 This study also courageously states that ‘although formal evidence of cost-effectiveness is lacking, the implication of the review is that all hospitals should consider using automated reminders to reduce non-attendance at appointments’. However, a recent Cochrane Systematic Review research reported that text messaging reminder is superior to no reminder and shows similar effectiveness to telephone reminders in reducing DNA rates. 4 The authors of this study clearly label these findings as ‘moderate quality evidence’. Thus, more research in this area is needed for large quality systematic reviews and meta-analysis to be useful.
In summary, there is sufficient evidence in the current literature that using messaging services to reduce DNA numbers is effective, but economic analysis is still weak and often lacking.
The primary aim of this study is to evaluate whether a text messaging reminder service reduces the DNA rate. The secondary aim is to evaluate the cost-effectiveness of a mobile text message reminder service at reducing patient DNA rates within the Trauma & Orthopaedic Department in a district general hospital.
Thus, the null hypothesis in our study is that the DNA rate after the introduction of the text messaging service would be no different from the DNA rates prior to the intervention.
Method
The study focused on the outpatient department of a district general hospital, which serves a population of approximately 200,000 people.
In January 2011, a patient text messaging reminder service was implemented across the outpatient departments in the hospital. The system was the iRemind system (X-ON, Suffolk, UK). All patients provided a mobile number at the time of receiving their appointment, and a text message reminder is sent to the patient one week prior to the scheduled appointment.
Data was collected prospectively 24 months prior (2009–2010) and 24 months following the implementation of this service (2011–2012). All financial data including set-up costs and annual maintenance costs were acquired from the hospital's financial department.
Inclusion and exclusion criteria
All patients attending the orthopaedic outpatient department were included in the study. Only patients capable of receiving a text message on an appropriate mobile phone were included in this study. Patients who had an appointment and cancelled or rescheduled it prior to their original consultation date were excluded from the study. Appointments for children were excluded from the data as messages would be sent to parent/guardian and possible DNA may act as a confounding factor.
Data collection
Data was obtained from the hospital records, which were created automatically to monitor patient attendance at the clinic. No identifiable patient data was used as the hospital number for each patient was sufficient to check that a message had been sent and whether they attended or not. Statistical analysis was conducted to establish the significance of the observed effect. The two groups to be compared were the pre and post intervention. The results were analysed using the Chi-squared test because unpaired categorical data would be obtained as patients would be recorded as either DNA or attended. The significance level was set at p< 0.05.
Advice from the local ethics committee was sought and it was deemed that such a study would not need formal ethics approval as it is a type of service review, evaluating a new technology in clinical practice with no direct patient involvement.
Results
The pre-intervention period had a total of 61,244 appointments, while the intervention period had 65,567 appointments, an increase of 7.1%. All patients during the intervention period were sent a text message reminder. The overall DNA in the pre-intervention period was 3774 (6.2% of total number of appointments), and the total number of patients that DNA in the intervention period was 3555 (5.4% of the total number of appointments). The actual change in the rate of DNA over the whole of the two periods is a 12% decrease in the overall rate of DNA, which was statistically significant (p < 0.0001).
For the new appointments, the numbers were 17,233 total number of new appointments prior to the intervention, and 19,366 in the intervention period. Therefore appointments increased by 12.4%, with a DNA rate of 4.7% and 4.6%, respectively. This is a decrease of 2% in the rate of DNA, which did not reach a statistically significant level (p value = 0.74).
Overall Did Not Attend (DNA) rate analysis pre intervention and post intervention, with subset analysis of new and follow-up appointment clinics.
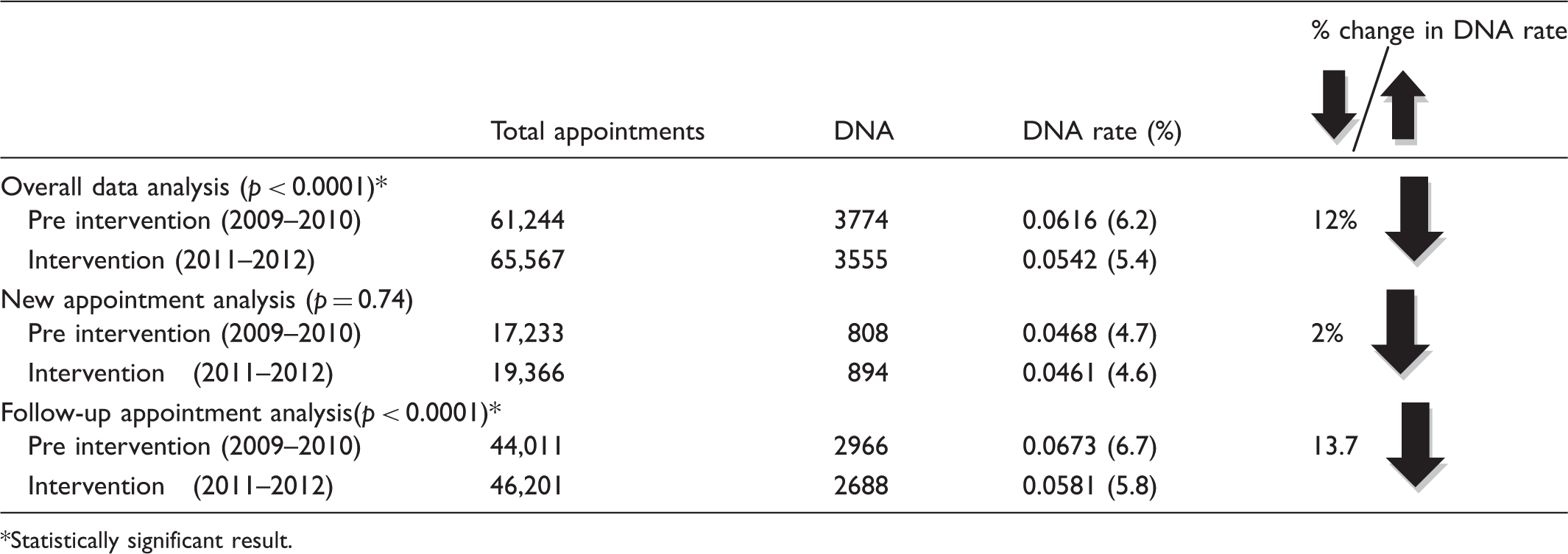
Statistically significant result.
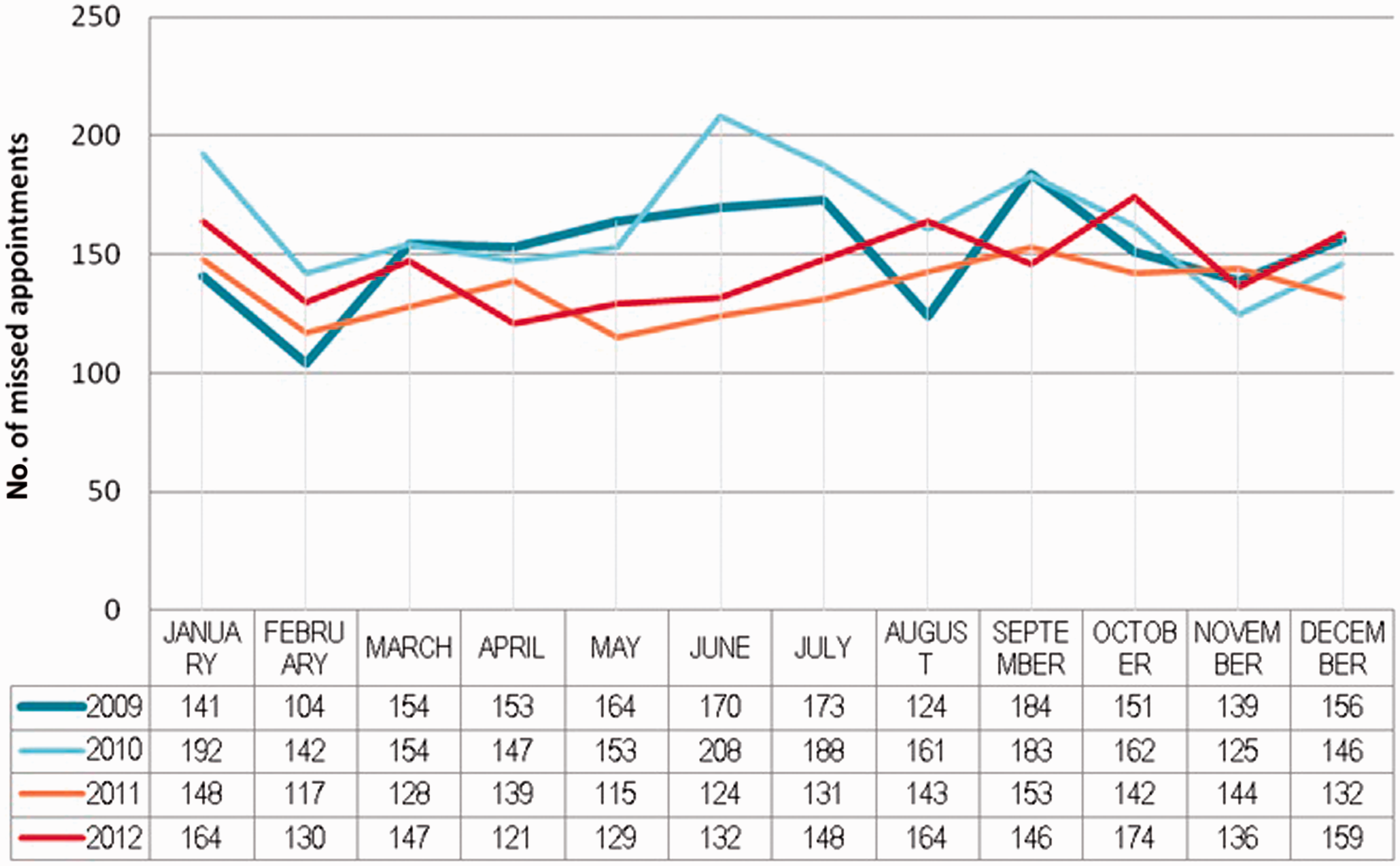
The overall DNA rates decreased following the implementation of the reminder service. The trends are illustrated in Figure 1. Furthermore, the number of missed appointments (DNAs) in each month of the entire study period is presented in Figure 2.
Trends in the Did Not Attend (DNA) rates observed before (2009 and 2010) and after (2011 and 2012) introduction of the text messaging service expressed as ratios of all missed appointments. Monthly breakdown of missed appointments (both new-patient and follow-ups) throughout the study period.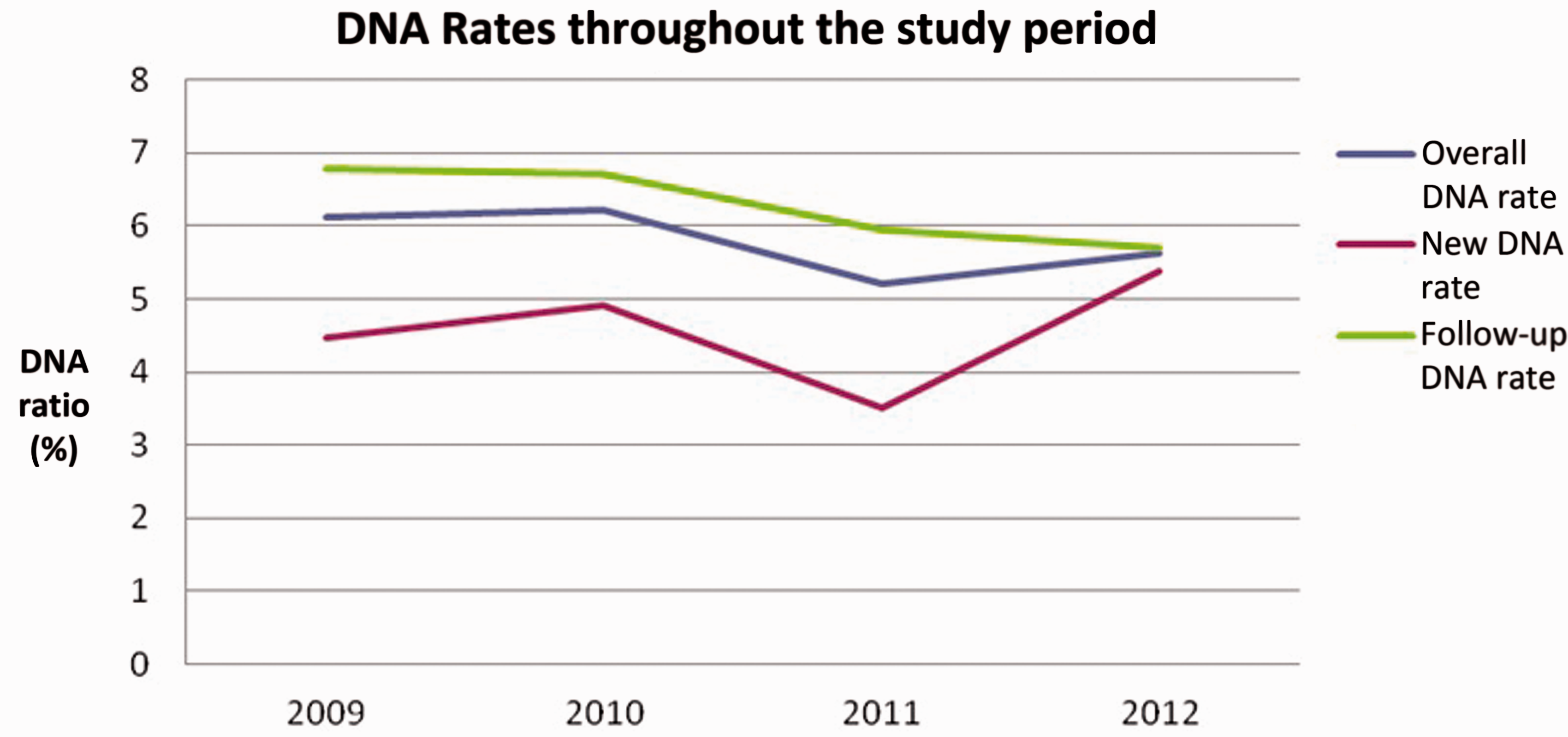
Cost analysis
The secondary objective of our study was to establish the cost-effectiveness of the proposed new system. The revenue for a new-patient appointment is £175.00 and £75.00 for a follow-up visit. The set-up cost for the messaging service was £56,000 (for the entire hospital). The annual maintenance cost of the system is £6000 (for the entire hospital). The set-up cost was amortized over a 10-year period, giving a proportional set-up cost over the 24-month operational period of £11,200 for the entire hospital. Therefore taking into account that on average Orthopaedics made up 11% of all appointments the proportional attributable set-up costs for Orthopaedics over the 24-month operational period is £1232.
The actual savings are calculated based on the baseline defined by the pre-intervention period. Because the cost of new appointments and follow-up appointments are different, and the increase in volume of appointments is different, both groups are examined separately.
If we assume that the DNA rate would have remained the same in the intervention period if we had not conducted the intervention (the null-hypothesis), the number of DNA patients in the new patient group is expected to have been 4.7% of the total number of new patients in the second period. The null-hypothesis would have given 910 patients that DNA, while the intervention actually resulted in 894 patients that DNA. Thus the savings are calculated based on 16 patients in the new appointments group, which equates to £2800.
The predicted number of patients that DNA for the follow-up group, according to the null-hypothesis, should have resulted in 2915 (6.7%) patients that DNA, while the actual DNA number for the follow-up group in the intervention period was 2688; that is, the intervention meant that 227 potential patients that DNA actually turned up for their appointment in the follow-up group. This equates to a saving of £17,053.
Therefore the total savings in the intervention group over a two-year period is £18,621 (£19,853 – set-up costs over 24 months).
Discussion
During each year of the study period an average of 11.40% of all outpatient appointments were for Trauma & Orthopaedics out of 92 departments that offer outpatient appointments at the hospital.
In our study, we looked at how text messages can be used to send out reminders for patients attending an outpatient orthopaedic department of a district general hospital.
Throughout the study period, there was an increase in the total number of appointments offered to patients each year. Despite that, following the introduction of the system there was an overall reduction of DNA rate by 12%. This indicates that we have not reached the target originally set in the business case. However, this still is a statistically significant reduction in overall DNA rate. Furthermore, the time periods audited pre and post intervention are statistically very small and a larger effect maybe seen with longer-term analysis. The reduction in DNA rate amongst new appointment patients was 2% and despite this not being statistically significant the authors anticipated such a result in this sub-group, as they have found anecdotally that patients with new appointments are probably more likely to turn up for their appointment. Thus, the DNA rate was anticipated to be similar pre and post intervention.
The DNA rate amongst the follow-up group reached statistical significance with the introduction of the text messaging service and there was a 13.7% reduction in DNA rate.
Within this sub-group, the authors anticipated that the total DNA numbers would be higher, as patients may forget the times and dates of repeat appointments and indeed many also choose not to attend follow-ups without cancelling when they subjectively feel their injury/ailment is better. Nevertheless, the intervention appears to have significantly reduced the DNA rate.
Our results are in keeping with current literature, which demonstrates digital reminder messaging as an effective tool to reducing DNA rates.5–7
Based on simple calculations and tests the cost analysis of the system is encouraging. The proposed system does appear to be financially sustainable at this stage given that we have only examined the department of orthopaedics. Therefore, the conclusion is based on the current trend and may not be definitive. The fact that there was a reduction in the DNA number despite the increase in the demand shows that the system has potential to improve clinic attendance and help achieve financial savings.
Limitations in this study include not knowing what percentage of patients actually ‘received’ text messages, as the IT department was able to confirm that all patients were ‘sent’ messages. However, when patients were given an appointment a mobile phone number was requested each time so that the patient may receive a text reminder. Though this may be seen as a major limitation of this study, given the large number of patients assessed it was not feasible to ascertain from each patient whether they received the message or not. However, patients that did not have a mobile phone were excluded from the study. As no other variables changed between the two study periods it is unlikely that there would be any other confounding factors, thus attributing any change in DNA rate to the intervention of a text message reminder. Furthermore, more detail on costs such as ICT equipment depreciation and replacement would enhance the cost analysis. In addition, such studies would be greatly enhanced by carrying out a formal health economic analysis, thus considering not only the cost of health service but also the health outcomes of the patient.
Since the text messaging service has been introduced at the hospital, examining the Trauma & Orthopaedic outpatient service only gives a snapshot of the effectiveness of such a service and all other areas using the service need to be evaluated for a complete assessment of clinical and cost effectiveness.
In addition, any study evaluating new technology would always be enhanced by questioning the patients directly as to the effectiveness of such a service, as they are the end user of such technology. This study lacks a detailed analysis of the patients that DNA in terms of their age, gender, number of previous appointments etc., as such, factors have been demonstrated to increase the likelihood of the patient's not attending. 8 Such information may help the system better target ‘high risk’ groups of patients that are statistically more likely to not attend.
Our analysis revealed patterns of seasonal variations that are potential areas for improvement and therefore if addressed could increase the cost-effectiveness of the system. For example, it is notable that there are certain months throughout the four years studied that have lower DNA rates (e.g. February and November). Conversely, December and January have increased numbers of DNA. This suggests that there are additional factors that need to be considered when booking appointments or sending reminders. Thus sending extra reminders during holidays may be a prudent step as DNA rates always increase during these periods. Furthermore repeating reminders less than a week in advance could improve the DNA rate.
Factors associated with missed appointments have been the subject of previous research. Most studies on the topic identified patient forgetfulness to attend or cancel the appointment as the main reason for not attending. Some of the other reasons include lack of transportation, scheduling problems and oversleeping. Timing of the reminder may also play a role, although a recent review of 29 studies showed that there is a small relationship between the effect and the time at which reminders are sent. Furthermore, the actual form of the reminders needs to be considered – there is some evidence that human generated telephone reminders are more effective than generic text messages. 3
Numerous ways to tackle the problem have been proposed over the years with variable effect. One example by airline companies is to over book for anticipated non attendance. This particular intervention can be effective at improving provider productivity, however, it also can result in an increase in patient wait times or provider overtime. Another example is introduction of a refundable booking fee. At the time of booking of an appointment patients would be required to pay a certain amount of money, which would later be refunded when they attended the clinic. This intervention can undoubtedly motivate patients to stick to their scheduled visit, however, it also involves numerous potential obstacles. Patients may simply not agree to pay a booking fee for an appointment, or they might simply not be able to afford it.
More innovative methods to reduce DNA rates taking advantage of modern technology have also been proposed over the years. Perhaps the most common example is the use of mobile phone messages to send out reminders about clinic appointments as well as various other purposes related to improving healthcare.3,4 Some hospitals offer virtual appointments to their patients via Skype. Newham University Hospital ran a pilot where some diabetic patients, who did not need physical examination, were consulted virtually. As a result, the number of missed appointments was reduced by 11%. At the same time feedback from patients showed that the quality of those appointments equalled that of the normal ‘face-to-face’ consultations. 9
Conclusion
Our analysis showed that in a district general setting mobile technology is a feasible tool in improving attendance rates at outpatient clinics. There was a statistically significant reduction in the overall number of missed appointments after the introduction of the text messaging service. The system appears to be cost effective and we would encourage other institutions to look at such mobile technology to increase clinical effectiveness.
Thus the null-hypothesis is rejected.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.