
Abstract
Introduction
Telehealth has been widely promoted as a technology to make healthcare more effective and affordable. However, current telehealth systems suffer from vendor lock-in and high cost, and are designed for managing chronic diseases rather than preventing them.
Methods
We address shortcomings of existing consumer-level health informatics applications in supporting senior health consumers, and provide designers of such systems with a design framework. We assess the feasibility of patient-centred health management systems (HMSs) that are designed based on the proposed framework. In contrast to traditional telehealth, HMSs are patient centred and aim at enabling health consumers to take control of their own health by providing functionality for health self-management. Quantitative and qualitative methods were adopted in evaluating a prototype HMS.
Results
Senior healthcare consumers viewed our HMS prototype positively, and experienced a positive change in their attitude towards their health. We identified requirements and challenges for HMSs. In particular, participants indicated that social networking features must have a clear purpose beyond simple broadcasting of emotions and opinions.
Discussion
Our study indicates that seniors are able and motivated to leverage a web-based patient-centred HMS, provided that there are suitable health support applications tailored to their needs. This could be achieved by making it attractive for third party application developers to contribute HMS content.
Keywords
Introduction
The healthcare systems in many developed countries are struggling with an increasing number of seniors, more chronic diseases affecting them, a shortage of healthcare professionals and healthcare spending rising faster than the GDP.1,2 There are three main emerging issues concerning public health: providing access to affordable healthcare, solving chronic health problems and preventing diseases. 3 One promising approach to achieve these goals is to empower healthcare consumers to better manage and monitor their health. Telehealth systems can enable users to track their health status and to actively participate in treatment regimens and preventive strategies. However, telehealth systems are mostly confined to health monitoring in a home environment. Adoption and use is further constrained by the high initial costs, the lack of extensibility, and a system design which is centred around the clinical users.
In order to reduce overall healthcare spending, healthcare systems for consumers need to be widely available and affordable. Web-based solutions are promising interventions that could facilitate desired lifestyle changes and are capable of reaching a wider section of the senior population (65+) at a low cost. 4 Seniors are often said to experience anxiety and usability issues when dealing with technology, but the trend is changing and more than half of US seniors are online today. 5 Searching for health-related information is the third most popular online activity, after email and online search in general. 6
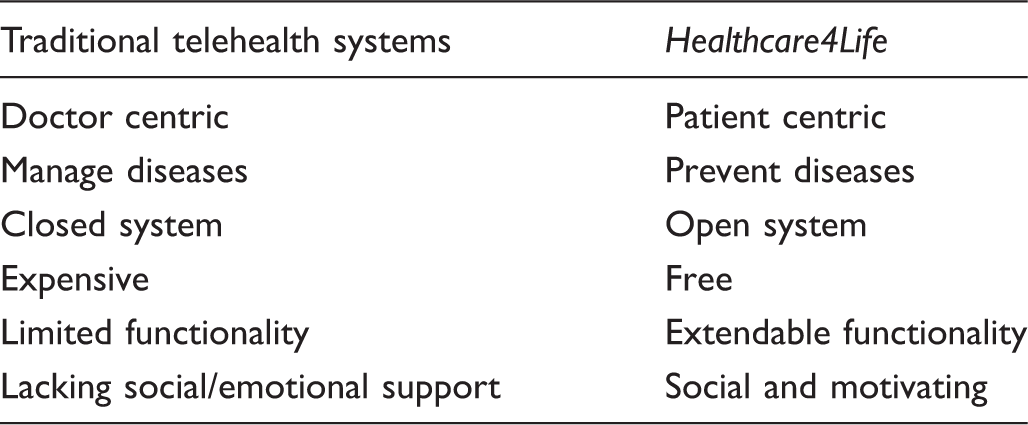
There is a need for systems that support health consumers in managing their own health, in contrast to monitoring and treating diseases as telehealth systems do. In the following, we will refer to such systems as health management systems (HMSs). The main idea of a HMS is that it is patient centred rather than clinician centred. A HMS aims at lowering the barrier for health consumers to take control of their own health, by providing functionality for health self-management. This does not exclude telehealth functionality, but sets a focus different from traditional telehealth systems.
In this paper we propose a design framework for a HMS targeting seniors, which is web-based, patient centric, affordable and extendable by third parties. We use the framework to design a system, and then assess the system's feasibility. We explain in detail the design of a prototype, Healthcare4life, based on this framework. Healthcare4life is envisioned as a general healthcare system containing a wide variety of health support applications. The idea is to empower patients to take control of or manage their own health independently, unlike most doctor-centric management systems for health that are solely designed for clinicians to provide effective care. Healthcare4life serves as a prototype of novel patient-centred computer-based health interventions, especially HMSs that are seen as transformational tools for the delivery of health services from a distance. We try answering the research question ‘how best to design a patient-centric HMS that is widely available, affordable, extendable by third parties, and is well accepted by seniors?’
Design
Healthcare4Life was designed bottom up through the eyes of senior healthcare consumers with the aim of enabling them to be more proactive in managing their own care. We have employed a patient-centred approach (suggested by Arsand and Demiris 7 ) in developing Healthcare4Life by working closely with seniors from the outset. In this section, we describe the proposed framework design and general design principles of Healthcare4Life. The framework provides a complete view of the suggested solution to overcome shortcomings of present consumer-level health informatics applications. We also present the design of a prototype that was developed to assess the overall concept, content and its feasibility with seniors.
Framework design
The framework combines the power of social media with telehealth systems to enable patients to take charge of their own health. Its goal is to aid the development of HMSs that are ubiquitous, extendable by third parties, contain social aspects, encourage cognitive engagement and put the user in control.
8
The overall structure of the proposed framework is illustrated in Figure 1, consisting of various components with the overall vision to empower healthcare consumers to take better care of their health. The framework has an open Facebook-like architecture enabling third-party developers to contribute new content and functionalities. Examples are applications for monitoring, health information, mental fitness and education. Physical fitness and rehabilitation can be achieved by adding applications using consumer sensing devices.
9
Accessibility is further improved by making the system web-based, so that it can be assessed on a PC, tablet and mobile phone. In order to assess the quality of content we propose a ranking system displaying user satisfaction and levels of use of each service, as common in modern software repositories. The ranking system should contain separate scores from patients and registered clinical/academic users.
Conceptual framework for healthcare management system.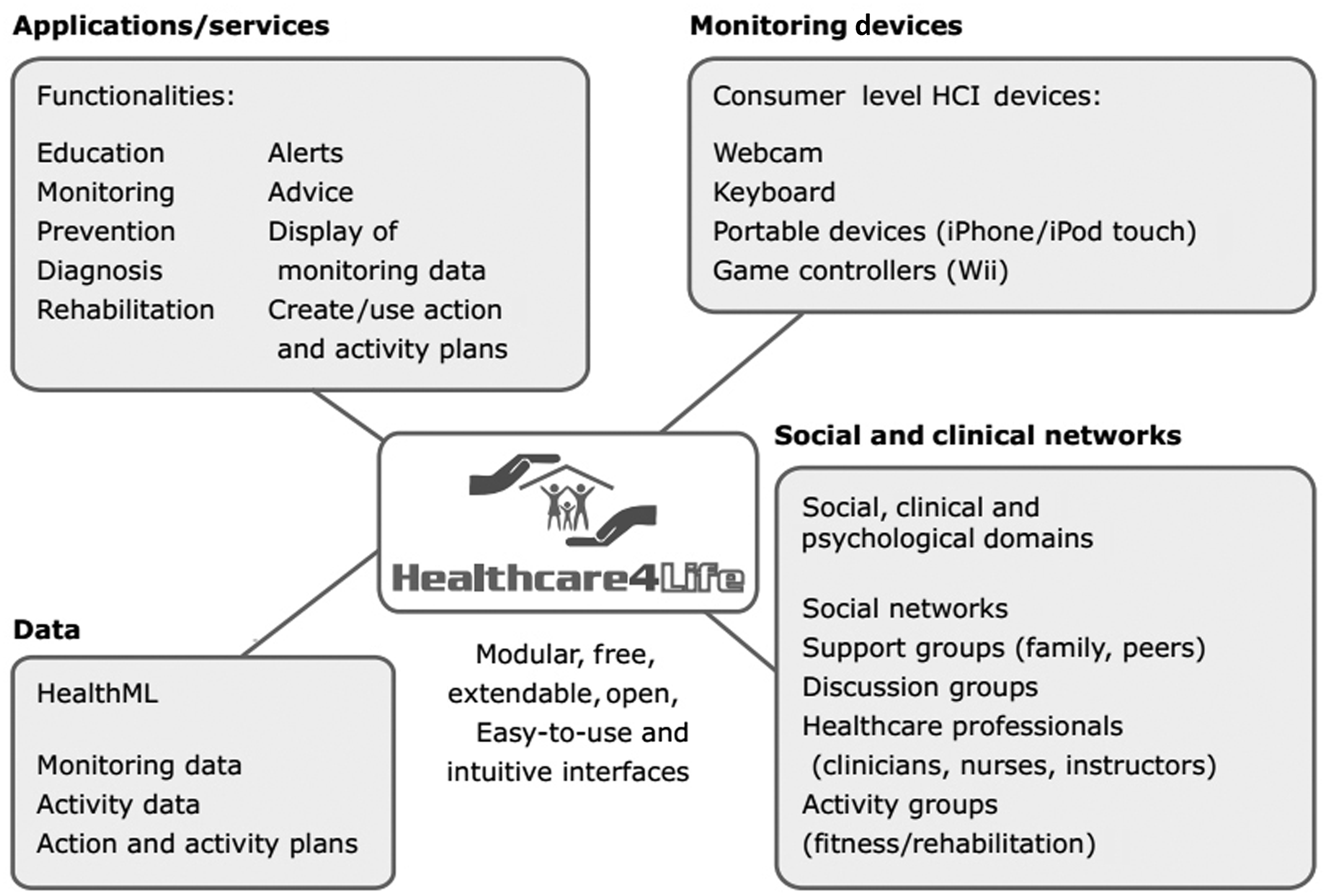
In order to share data among multiple applications, unifying data elements must be introduced that relate different types of data. This can be achieved by using a triplestore database: data consist of subject–predicate–object triples, where the predicate represents the unifying element. For example, different exercise games might use the same predicate for a ‘perceived-level-of exertion’ 10 scale. The unified data can then be used by monitoring applications to enable users to design activity plans and track progress.
While commercial telehealth systems put an emphasis on clinical networks, we utilise social networks to help users get in touch with their family, make new friends and discuss medical complaints with peers and support groups. The aim is to improve emotional health, which is essential for the overall well-being. Social networks can also help with motivating the patient, for example, by achieving family support, and competing/exercising together via a video link or in a virtual environment.
Key design principles
The understanding we gained from analysing the advantages and shortcomings of consumer-level health informatics applications
8
and requirements elicited from potential users
11
resulted in the following requirements or key design principles that were addressed in Healthcare4Life
Open and extensible: A HMS should offer a wide variety of health-related applications that are tailored towards the needs and preferences of patients. Otherwise, the content can become repetitive and uninteresting to users and result only in short-term lifestyle changes. The system should be ‘open’, so that third-party developers can contribute content via a plug-in mechanism (to eliminate vendor lock-in). Ubiquitous and affordable: A HMS should be accessible online for free via a common Web browser, ideally such that it can be viewed on PCs, tablets and smartphones. Social and emotional support: A HMS should create a caring community, enabling users to provide and obtain social support to and from other users. Social features should be incorporated to reduce loneliness, for example, enable users to become friends of other patients, to perform activities together and motivate each other. Feedback and motivation: A HMS should provide users with feedback on their health progress and motivate them to become more proactive, for example, make positive lifestyle changes. Visual feedback via easy-to-understand graphs and charts is particularly important to users with limited health literacy. Privacy control: User privacy must be maintained and users must be able to fully control their health data, for example, sensitive health data such as diagnosis, symptoms and treatments must not be visible to others without the explicit permission of a user. Personalised user interface: Users should be able to customise the HMS and select applications tailored towards their needs, for example, to easily add health applications to and remove them from their profile. Sufficient information about available applications should be provided to enable users to select desired functionalities. Linear structure and clear instructions: A HMS should follow a linear structure wherever possible in order to avoid confusion and frustration, for example, the system should allow users to complete a health related task such as tracking their weight using a linear sequence of simple steps.
Key differences between traditional telehealth systems and Healthcare4Life.
Prototype design
Based on the framework in Figure 1, we designed a prototype in order to demonstrate the utility of the key design principles and provide evaluation results with the help of user studies. The prototype can be divided into two parts: Healthcare4Life (the system itself) and Healthcare4Life applications (health applications developed and integrated with the system).
The Healthcare4Life system
Patients are provided with the following functionalities (see top of Figure 2): Activities to motivate friends with positive comments and to share their status; Health Apps to access applications added by developers; Profile to create a basic online health profile to get located by other users; Mail to send mails to users listed as ‘friends’; Friends to access the profile pages of ‘friends’, find and add new friends, and invite others to join Healthcare4Life; and Settings to make changes to general system settings such as privacy settings.
Main menu depicting key functionalities (top) and social networking functionalities (bottom) of Healthcare4Life.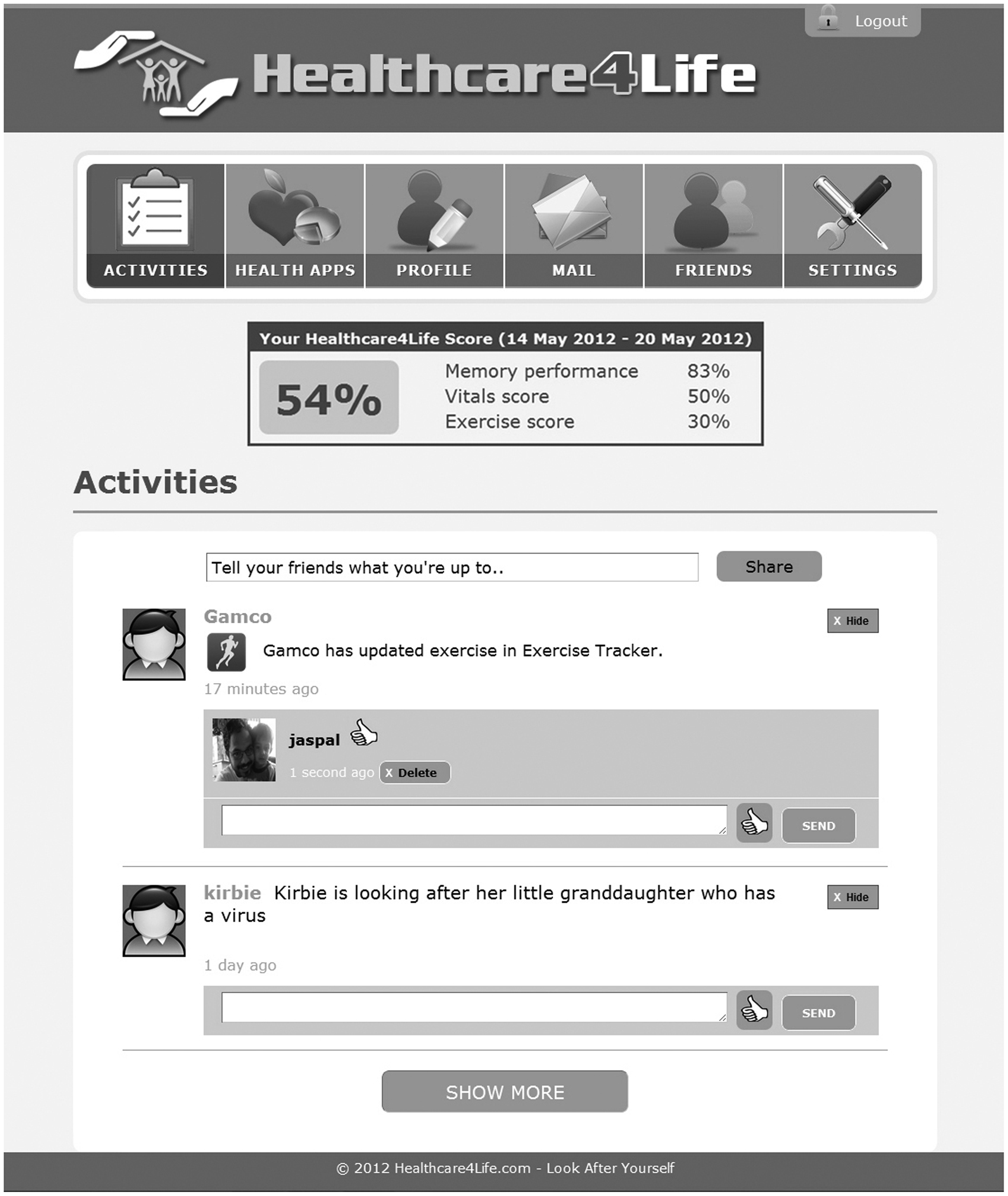
Similar to emerging commercial tools,12,13 the system provides immediate summative feedback about the user's health in the form of a Healthcare4Life score (Figure 2). The score combines the current health status and exercise and memory performance: vital signs measures with scales from the literature,14–16 scores from exercise games and other applications measuring physical activity, 9 and a memory game score. There are many commercial applications17,18 that could also be considered in the future. To be cautious with regard to interpretation of the scores, during enrolment, patients are made aware that the scores are just an indication of health based on an average user and patients should always check with their doctor how these scores can be used/interpreted in individual cases.
In terms of the social networking functionalities, users can create social support groups using a Facebook-like interface. Other members can be searched for, for example, by name, hobbies and general health conditions. The actual, specific health conditions of other users are not displayed and users are encouraged not to use their real name for privacy protection. Users can send ‘friend requests’ and accept or decline other users’ requests. The system allows users to share information about their activities (i.e. generated by the health applications they use), and view and comment on the activities of their friends.
Healthcare4Life applications
In order to test the plug-in functionality of Healthcare4Life, several health-related applications were developed and integrated. To be successful Healthcare4Life requires a large number of health applications catering for different needs of users. The user can select applications from the application directory. The following is an overview of the applications that were implemented for the prototype.
The Weight Tracker application allows users to input their current weight at arbitrary points of time. A weight graph is generated enabling users to see their weight trend and their progress in achieving a target weight, which should be set together with a health professional. In the Matching Pairs game players find pairs of matching cards. The game can be played remotely by two users located at different locations, who can play either collaboratively or competitively. The Exercise Tracker is used to monitor the duration of physical activity and to educate users about the amount of calories they need to burn to look after their health. Exercise goals can be set and users are advised to discuss them with their health professional. The application suggests an amount of exercise based on the user's weight, corresponding to low/moderate intensity exercises in STRRIDE studies. 19 Similarly, the Vital Tracker allows users to input vital signs measurements, for example, blood pressure, using a tabular interface, and displays them as a graph over user-defined time periods. The prototype also included an existing third-party application called Calorie Calculator from LabPixies.com, which helps users to determine their daily calorie consumption.
Evaluation
Methodology
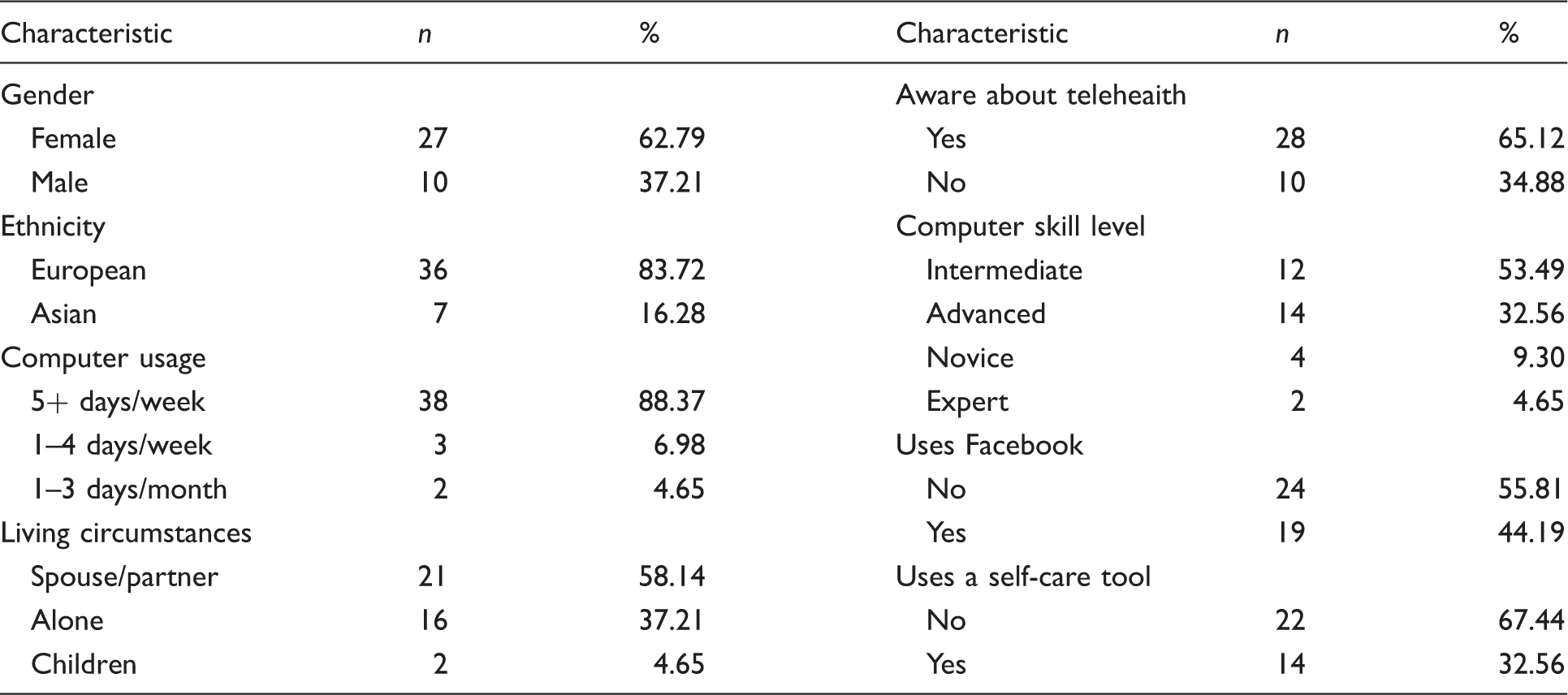
Demographic characteristics of the evaluation study participants.
Participants were invited to use Healthcare4Life (made accessible via the Web) at their own pace over a six week period. Activities in the system were logged and participants were asked to complete questionnaires at the start of the study (initial questionnaire), at the end of the third week (interim questionnaire) and at the end of the sixth week (final questionnaire). The questionnaires consisted of established scales, that is, the Multidimensional Health Locus of Control (MHLC), 20 the Intrinsic Motivation Inventory (IMI) 21 and the System Usability Scale (SUS). 22 The readily available shortened version of MHLC and IMI were administered as these scales retained adequate internal consistencies and test–retest reliabilities.23,24 Each scale was employed for a specific purpose, that is, MHLC to investigate whether Healthcare4Life can positively affect the users' attitude towards managing their health, IMI to evaluate users' subjective experience (levels of intrinsic motivation) in their interaction with Healthcare4Life, and SUS to assess the overall usability of the system. At the end of the study, a short interview was conducted with four selected participants to gain further insights into their experience with and perceptions of Healthcare4Life. Further details of the evaluation study can be found in Dhillon et al. 25
The MHLC consisted of nine statements with six response choices, ranging from strongly disagree (1) to strongly agree (6). Change scores for each MHLC subscale were calculated by subtracting baseline scores from follow-up scores. Paired Wilcoxon signed rank tests were used to compare the two MHLC mean scores (i.e. initial and interim questionnaire) of the subscales based on the a-priori hypothesis that participants would feel more in control when using Healthcare4Life (i.e. more, Internal; less, Powerful Others and Chance). Statistical significance was set to p < 0.05.
Results
Figure 3 depicts the use of the various functionalities of Healthcare4Life over the trial period. Overall, 1638 activities were performed by the participants.
Participants' activities in Healthcare4Life.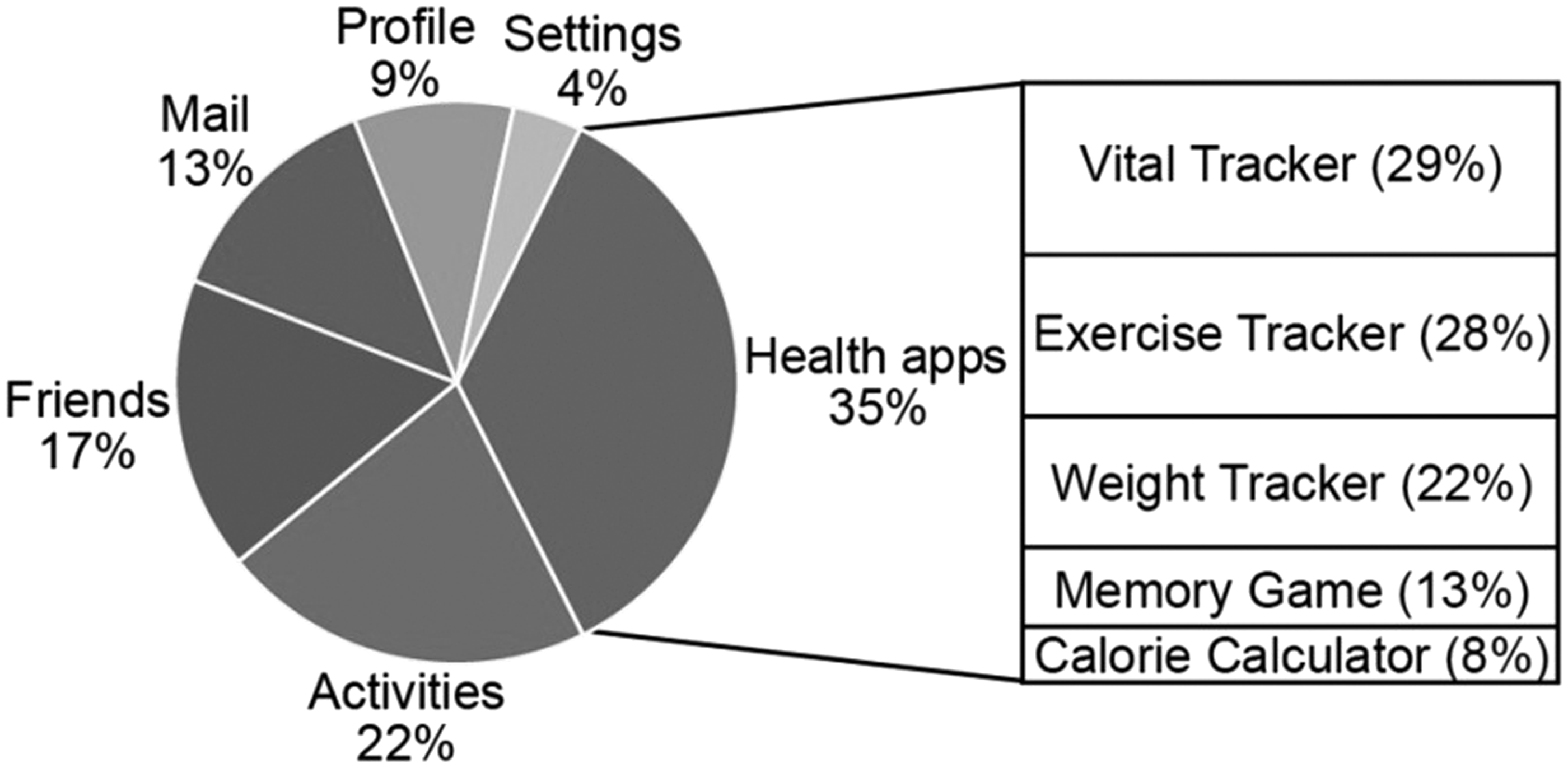
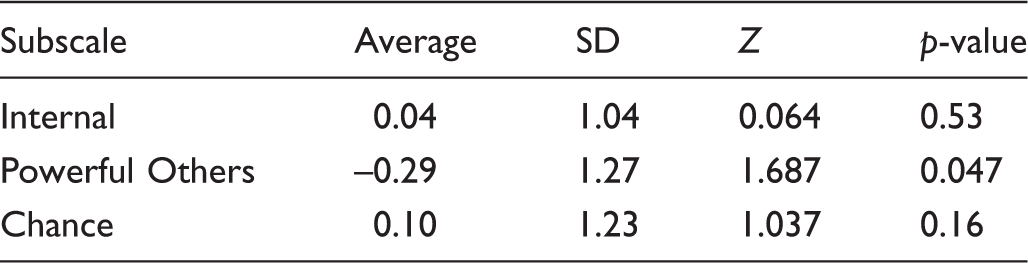
Change in user responses to the Multidimensional Health Locus of Control subscales within the three week period between user surveys (n = 23).
Change in user responses to the ‘Powerful Others’ subscale before and after using Healthcare4Life.
Results of the Intrinsic Motivation Inventory on a scale from 1 (strongly disagree) to 7 (strongly agree), with mean ± standard deviation and midpoint comparison test results for each subscale.

Most common positive and negative comments about Healthcare4Life.
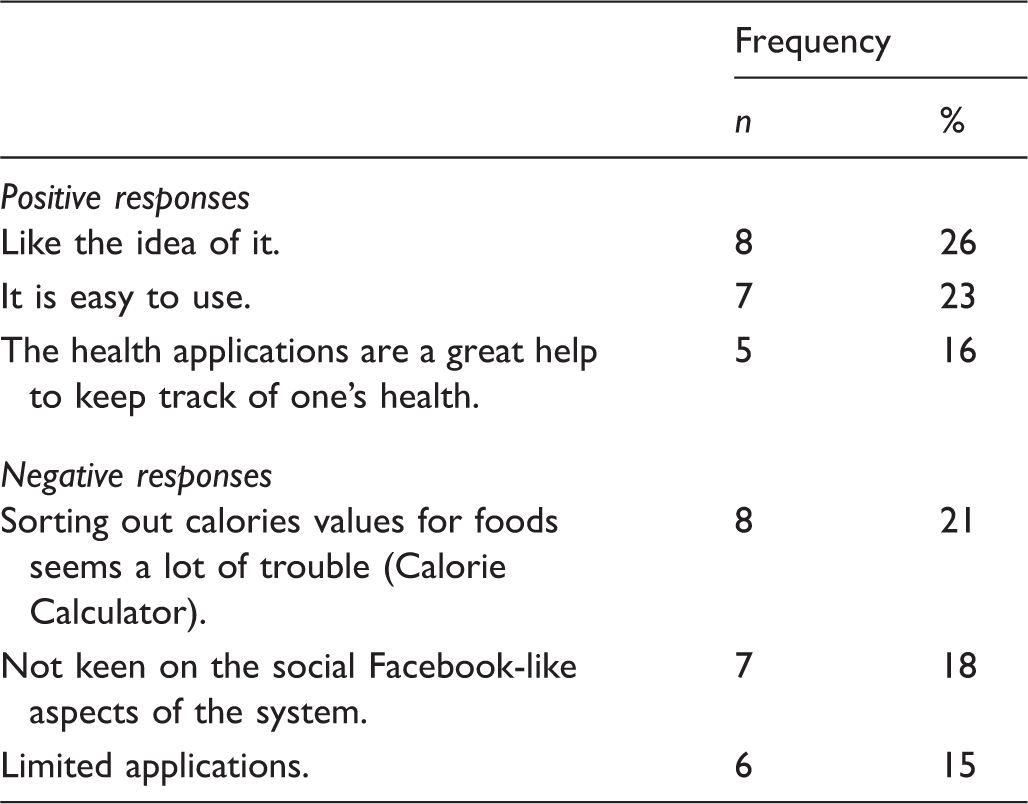
In order to evaluate usability issues and the usefulness of different functionalities we used a survey with responses rated on a six-point Likert scale. Participants stated that Healthcare4Life encourages them to be better aware of their health (80% agreement), that the charts/graphs help to better understand health progress (80% agreement) and that the health applications reduce the need to use different websites for managing health (72% agreement). Sixty-five per cent of participants agreed that Healthcare4Life has the potential to positively impact their life, and 56% found that it simplifies cumbersome health monitoring tasks.
However, only 33% of users agreed that the social features motivated them to use the system, and only 31% agreed that the involvement of ‘friends’ helped them to better manage their health. Four participants of the study expressed disappointment that their friend requests were not responded to. Most of the participants were not comfortable to accept strangers as ‘friends’ in the system. A typical comment was: ‘I would not share my medical details with someone I don't know’. One participant elaborated on this: ‘I find the use of the word “friends” for people I don't know and will never meet very inappropriate and off-putting. Also it's really important to learn more about the people in your circle so that you care enough about them and their goals to be able to offer support.’
Discussion
The results show that health applications were mostly used by the participants, which points to the importance of having an open plug-in architecture that facilitates the creation of new content. The social networking features, that is, the Facebook-like comment page (‘Activities’) and ‘Friends’ were the second most commonly used features, which indicates that users are interested in sharing experiences and making social connections. The Calorie Calculator was least used by the participants because of its comparably complex user interface, the time required to input data, and because many food items were not relevant to a New Zealand context, according to user feedback. This observation emphasises the need for customising applications according to the user's location, culture and language.
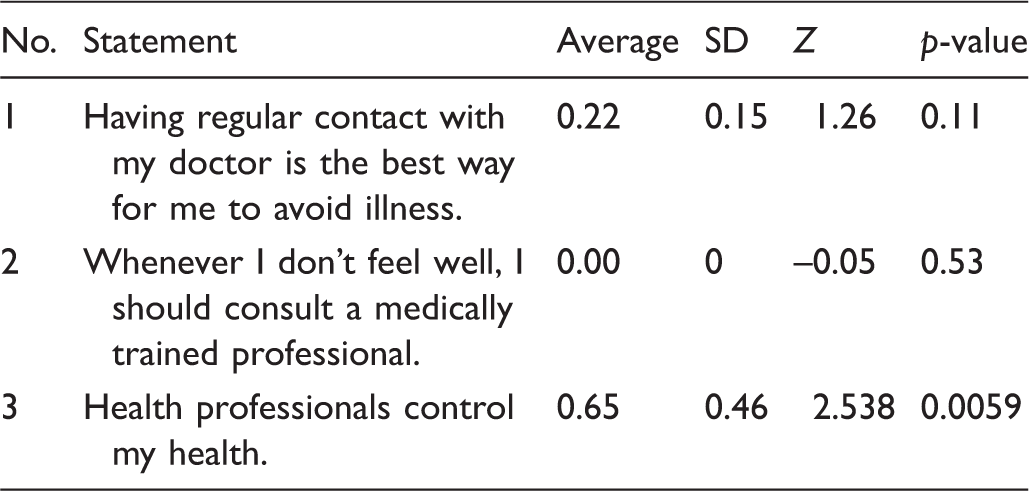
The results of the MHLC scale, especially in the ‘Powerful Others’ subscale, were encouraging. Statement 2 (refer Table 4) indicates that users rely on healthcare professionals for diagnosis and treatment and Healthcare4Life does not make a difference. However, overall the ‘Powerful Others’ scores and in particular participants’ disagreement with Statement 3 (Table 4) have decreased significantly (Z = 1.687, p = 0.047 and Z=2.538, p = 0.0059), which indicates that users have obtained a better understanding of their health and how their own decisions affect it. This suggests that the use of Healthcare4Life has the potential to positively change the attitude of users that their health is not controlled by health professionals, that is, potentially encouraging users in taking control of their own health.
The results of the intrinsic motivation scale presented at Table 5 imply that the participants were fairly interested in the system, were adequately competent, made a reasonable effort in using the system, and felt that the system has some value or utility for them. The ‘Pressure/Tension’ subscale obtained a low score, indicating that the participants did not experience stress while using the system. Seniors within the age range 60 to 69 considered themselves more competent and found the system more valuable than older seniors. Participants rated the usability of the system positively. The adjective rating of the resulting mean SUS score for 68.33 is ‘OK’, which indicates it is an acceptable system. 26 The results indicate that social networking functionalities are desired by seniors, but not in the form we might know from Facebook and similar sites. Hence, it is necessary to revise the social component in a way which fosters the building of personal relationships (possibly using a video conferencing facility) and which overcomes concerns about privacy issues.
Conclusions and future work
We proposed a novel framework for patient centric HMSs and designed a prototype called Healthcare4Life targeted at seniors, which was well accepted by healthcare consumers. Crucial for the success of such an application is a sufficiently large user community and developer support. This means in particular that a HMS needs to take the needs of content contributors into account, that is, it should be attractive to researchers and developers.
Our research confirmed that healthcare consumers with similar health conditions have widely varying needs in terms of form and level of desired support. Not meeting these needs limits acceptance and usage of the software. Some applications, such as weight trackers, exercise trackers and memory games, are useful to the majority of users. However, patient-specific needs, in particular those related to health conditions, must also be taken into account. Eventually, the number of applications in a system might become difficult to manage and new tools for this need to be developed. One possibility is to create default settings for specific health conditions. For example, a user with diabetes would by default use a medication reminder and applications for tracking diet, exercises and vital signs.
The users' attitude towards social networking functionalities was mixed. On the one hand, users confirmed that social isolation is an important issue, and many users expressed the desire to make new friends online. On the other hand, many users felt uncomfortable to become friends with somebody not personally known and there were privacy concerns. It has become clear that Facebook-style social media functionalities cannot be directly transferred to healthcare applications. Researching this issue is a major direction of future work. One possibility is to allow users to get to know each other better, for example, by video chat, in order to build trust. Another direction is to allow users to assume a new identity without any links to their real identity, similar to the model used in SecondLife.com and other virtual worlds.
An important result of our research is that HMSs such as Healthcare4Life have the potential to change the attitude of seniors towards their own health positively, that is, empower patients and reduce doctor reliance. To explore this further, more health psychology research needs to be incorporated, for example, by using visual information to promote behavioural change.27,28 Longer term studies with larger patient populations and more content are necessary to confirm and quantify the long-term health effects of Healthcare4Life.
Limitations
The Healthcare4Life vision covers a large scope and therefore only essential features of the framework were implemented and tested. Only a few health applications were developed and most of the applications created concentrate on health monitoring. Although the system was intended for two groups of users, that is, healthcare consumers and application developers, our focus was on healthcare consumers, especially seniors, in ensuring that the overall concept was feasible and accepted by them.
Most participants of the evaluation study had experience with computers and results for users unfamiliar with computers may differ. The relatively small size of the sample did not allow us to determine whether the system is more useful for some subgroups than others (e.g. particular health issues, psychological or emotional conditions). We also did not provide the necessary equipment, such as blood pressure measuring devices and glucometers, to enable the participants to track their vital signs data. Furthermore, we administered the MHLC scale at different stages of the study to compare changes in their measures, but there was no control group for comparison.
Footnotes
Acknowledgements
We would like to thank the participants of the user study for their kind support, patience and valuable feedback. We acknowledge Wellington ICT, SeniorNet Eden-Roskill and SeniorNet HBC for advertising the study and for allowing us to use their premises to conduct the introductory sessions. We also thank Nilufar Baghaei for her inputs in conducting the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.