
Abstract
Acute lymphoblastic leukaemia (ALL) is the most common childhood malignancy. Caring for children with ALL is an uncommon experience for parents without medical training. They urgently need professional assistance when their children are recovering at home. This paper documents the process of developing an Android application (app) “Care Assistant” for family caregivers of children with ALL. Key informant interviews and focus group studies were used before programming the app. The key informants and focus group members included: caregivers of children with ALL, cancer care physicians and nurses, and software engineers. We found several major challenges faced by caregivers: limited access to evidence-based clinic information, lack of financial and social assistance, deficient communications with doctors or nurses, lack of disease-related knowledge, and inconvenience of tracking treatments and testing results. This feedback was used to develop “Care Assistant”. This app has eight modules: personal information, treatment tracking, family care, financial and social assistance, knowledge centre, self-assessment questionnaires, interactive platform, and reminders. We have also developed a web-based administration portal to manage the app. The usability and effectiveness of “Care Assistant” will be evaluated in future studies.
Introduction
Paediatric cancer ranks second in leading causes of death in children in developed countries. 1 Acute lymphoblastic leukaemia (ALL) accounts for 26.8% of all paediatric cancers and remains a leading cause of cancer death in children. 2 It is the most common childhood malignancy among children less than 15 years old. 2 In developed countries, annually about 38 out of 1,000,000 children are diagnosed with ALL. 2 The peak incidence of childhood ALL occurs among children from 2–4 years old. 3 Due to improved diagnosis and treatments, the cure rate for childhood ALL have increased considerably from 10% to nearly 85% in recent decades. 3
Receiving a diagnosis of cancer is a significant stressor to both the patient and their family. Unlike healthcare providers, most family caregivers normally perceive providing care to cancer patients as a chronic stressor. 4 Caregivers often experience physical stress, negative emotion, economic burden, and undesirable behavioural and physiological impacts.4–8 The enormous burden reduces the caregivers’ quality of life, which may reduce their ability to take care of the cancer patients. 9,10 Due to the limited cognitive ability of the children with ALL, family caregivers, particularly the parents, play an important role in delivering complex health care services in and out of the hospital. Caring for children with ALL can be a very challenging experience for the parents who lack clinical knowledge. Thus, caregivers of paediatric cancer patients are in desperate need of knowledge and support from healthcare professionals.
Many researchers have noticed the lack of support for the parents of ALL patients once their children were discharged from hospital and recovering at home. 11 However, existing interventions are mostly focused on adult cancer patients’ caregivers and are aimed at decreasing their care burden and psychological distress and increasing quality of life. Researchers have used educational programmes, 12 brief behavioural sleep interventions, 13 and physical exercises 14 for caregivers of adult cancer survivors. Recently, m-health has been used in supporting the caregivers of adult cancer patients. Comprehensive Health Enhancement Support System (CHESS) is a web-based lung cancer information, communication, and coaching system for caregivers. 15 A randomized controlled trial of 285 caregivers showed that CHESS improved caregivers' coping skills and moods and relieved their burden. 15 Our project is to develop a smartphone application (app) to support the family caregivers of ALL children in China. The purpose of this paper is to document the process of developing the smartphone app and share the qualitative study results with the research community.
Methods
A multidisciplinary research team including cancer care physicians, nurses, and software engineers worked collaboratively to design and conduct the research. A systematic literature review was first conducted to review all smartphone interventions for long-term health management of chronic diseases. 16 A qualitative approach was then used to collect data to conceptualize the structure and content of the app. We sent invitation letters and made follow-up calls to family caregivers, cancer care doctors and nurses, and software engineers in order to recruit participants for the interviews and focus group discussions.
We first conducted semi-structured interviews with individual caregivers to conceptualize the features of the app. Followed by three rounds of focus group discussions (one focus group per round) with caregivers, physicians, nurses, and software engineers. The interviews and focus group discussions were recorded and continued until the same stories, themes, and issues were emerging from the interviewees. Data collection spanned from October 2012 to July 2013. Interviews and discussions were transcribed verbatim within two days of the interview or group discussion. This research received ethical review approval from the Second Military Medical University and Shanghai Children’s Medical Centre. Figure 1 shows the workflow of the qualitative research and app development.
Workflow of developing “Care Assistant.”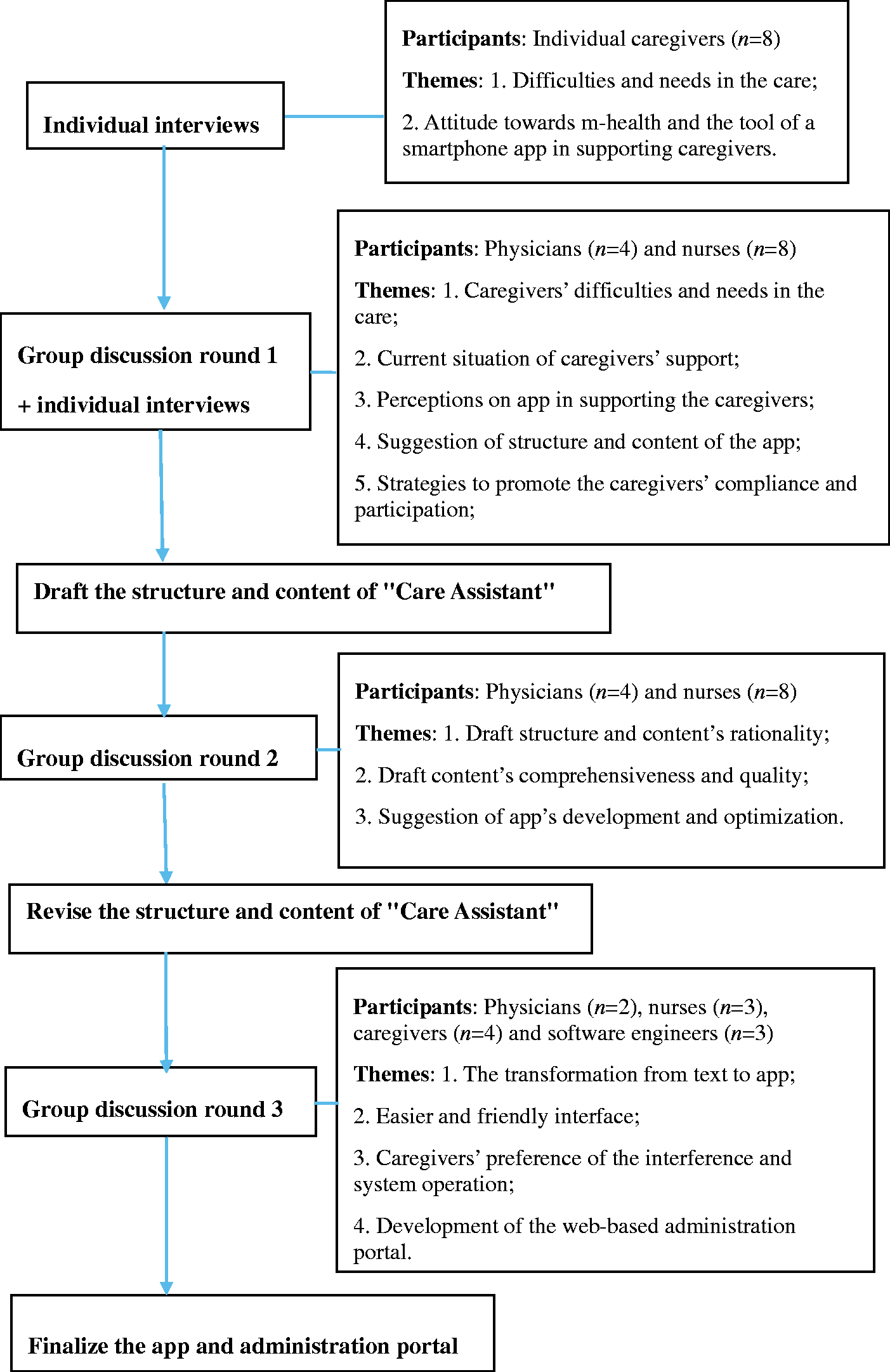
Interviews with individual caregivers
The interviews were conducted in a conference room at a metropolitan academic medical centre in China and lasted between 30–45 min. The eligibility criteria for participating in this research as a caregiver included: (a) the caregiver’s child was diagnosed with ALL and receiving treatments, and the child was less than 15 years old; (b) the caregiver had a high school diploma or higher and was able to communicate fluently in Mandarin Chinese; (c) the average monthly family income was 2000 Chinese Yuan (CNY) or over; (d) the caregiver was willing to use smartphone apps to manage his/her child’s disease. Informed consent was acquired from those caregivers who wished to participate. The participants were asked to describe their difficulties and needs in taking care of the ALL children, and their attitude towards m-health and smartphone apps that could assist them in caregiving. Follow-up questions were then posed in order to gain a deeper understanding of their challenges and demands.
Group discussion round one: physicians and nurses
Based on the literature review and the information from the individual caregiver interviews, we conducted the first round focus group discussions with cancer care physicians and nurses. The discussions were conducted in a conference room at a metropolitan academic medical centre in China and lasted between 120–150 min. These physicians have treated patients of ALL before and have more than five years of working experience in haematology/oncology with an education level of masters degree or above. The nurses had more than three years of working experience with ALL patients. These physicians and nurses were supportive of developing a smartphone app to assist caregivers of ALL children and gave informed consent to participate in the study.
The discussion was focused on: (a) caregivers’ major challenges and needs in taking care of the ALL children from the physicians and nurses’ perspective; (b) current interventions or support for caregivers; (c) perceptions of the smartphone app in supporting the caregivers of children with ALL; (d) structure and content of the smartphone app; (e) strategies to promote the caregivers’ compliance and participation; and (f) the app’s administration portal. After the first round of group discussion, one-on-one interviews ranging from 20-45 min were conducted in a private space with those participants who were relatively active in the group discussion to provide more information and suggestions.
Draft the structure and content of the smartphone app
Data collected from the key informant interviews and the first round of focus group discussion were analysed by two researchers independently. A qualitative content analysis aimed at finding manifest and latent meanings of data was applied to analyse the information manually. 17 A stepwise approach was adopted for the content analysis. Firstly, the transcribed data were read several times by the researcher in order to find the sense of the whole. Secondly, the segmentation of information was done to organize the segments and sub-segments of information. Thirdly, the significant information related to research questions was extracted. Finally, data were coded and grouped into categories and abstracted into subthemes and a main theme. We used these findings to draft the protocol of the app.
Group discussion round two: physicians and nurses
We held the second round group discussions with the same participants of the first round of group discussion and presented them the draft structure and content of the app. The discussions were conducted in the same conference room as the first round group discussion and lasted between 120–150 min. The discussions were focused on: (a) the rationality of the structure and content of the app; (b) features that need to be added or deleted; and (c) suggestions that may benefit the development and optimization of the app. We then revised the structure and content of the app based on collected information and suggestions. Similar qualitative analysis as the last round was performed to provide information for the next round of discussion.
Group discussion round three: caregivers, physicians and nurses, software engineers
The third round group discussion included caregivers, physicians, nurses, and software engineers. The caregivers, physicians and nurses were chosen according to their performance in previous interviews. We chose the active ones to join the third round of group discussion. The participants were given the revised structure and content of the app and were asked to come up with an acceptable way of transforming the text into app functions. The discussions lasted between 120–150 min. The discussions were focused on: (a) how to achieve the transformation from text to smartphone app; (b) designing a user interface; (c) defining the interaction; and (d) the administration portal. The smartphone app and the web-based administration portal were then finalized after the last group discussion.
Results
A total of eight caregivers, 12 cancer care providers, and three software engineers participated in the study. These caregivers were aged from 26–40 years. Five of them had a college degree, and four of them were fathers of sick children. Their family income ranged from 2000–10,000 CNY a month. Their children were aged between one and 11 years. There were three physicians and eight nurses in the study. They were aged 25–45 years with a college degree or above. The direct quotes from participants which supported the results are available in Appendix 1.
The need of a smartphone app to support caregivers of children with ALL
The interviews and discussions with caregivers, physicians and nurses revealed caregivers’ need for an interactive tool to help them in taking care of their ALL children. Most of the caregivers have smartphones and Internet access. All of caregivers in the interviews highly appreciated the idea of using a smartphone app to acquire more knowledge and receive more support.
Structure and key functions of the smartphone app
Most Chinese smartphone users have Android phones, so we developed the app on the Android system. The app has eight major modules: Personal Information, Treatment Tracking, Family Care, Financial and Social Assistance, Knowledge Centre, Self-assessment Questionnaires, Interactive Platform, and Reminders. There is also a web-based administration portal to help manage the app.
The Personal Information module helps both the caregivers and researchers. Several features of this app are dependent on the personal information of caregivers and their children. We also use this module to collect their demographic data for future research. Collecting data with an app is highly efficient and convenient. The data collected by the app could be more complete than other traditional methods since caregivers are required to input their basic information before using other features of this app.
Caregivers and cancer care physicians and nurses all emphasized the importance of treatment tracking (Appendix 1). Caregivers expressed their urgent need for information and knowledge to take care of their children at home. They felt helpless when their children were discharged from hospital and recovering at home (Appendix 1). We found that caregivers need information about financial and social assistance for which they are eligible. A discussion platform that offers them the opportunity to share information about financial and social assistance is needed (Appendix 1). It is necessary to provide caregivers with evidence-based scientific knowledge of ALL. The interviews and focus group studies revealed that caregivers need knowledge of all aspects related to ALL (Appendix 1). Not surprisingly, caregivers also want to know their own physical and psychological state. We think that providing them with scientific self-assessment tools and results will benefit them (Appendix 1). Stakeholders have expressed common interests in building an interaction platform. Caregivers and medical staff want easier interactions between each other (Appendix 1). Though caregivers rarely forget their children’s appointments, a reminder function is recommended to make caregivers feel relaxed, so as to reduce their care burden (Appendix 1). Finally, we feel we need to develop a web-based administration portal (Appendix 1).
More details about the function of these eight modules and the administration portal are as follows:
Personal Information stores the primary caregiver and ALL child’s demographic data, including caregiver’s age, educational level, occupation, residence, child’s diagnosis, treatment, and other clinic information. The Treatment Tracking module has a detailed record of time of diagnosis, treatment hospital, treatment phase, each treatment phase’s beginning and ending time, therapy modality, medication’s name and dosage, complications’ name, time of occurrence and following treatments, and time and results of examination. All the information can be recorded and revised in this module by the caregivers. The Family Care module provides knowledge and solutions of common problems and symptoms that may occur in the family care during the intermittent of treatment. The Financial and Social Assistance module forms an online portal of existing information about leukaemia-associated financial assistance organizations and also suggestions such as how to help the child transit back to normal life. The Knowledge Centre module provides caregivers with credible and systematic knowledge related to leukaemia, such as diagnostic tests, treatments, nutrition, and prescriptions. The Self-assessment Questionnaires help caregiver’s to evaluate their own psychological well-being such as anxiety,
18
depression,
18
social support,
19
care burden,
20
and quality of life.
21
These questionnaires are widely used and we have received permissions from their copyright owners. The results can be uploaded to the central server. Then caregivers will receive the self-assessment results, and researchers can obtain the data through the administration portal as well. In the Interactive Platform, caregivers can ask questions, and discuss anything with healthcare providers related to the disease and its care via Wechat. Due to our limited resources, we are not able to provide real-time communication with caregivers. Reminders: Using the smartphone's alarm clock function, caregivers can the set time of reminders and choose the reason of reminders such as medications, follow-up visits, etc.
A web-based administration portal is designed to host caregivers and ALL children’s demographics, diagnosis, treatment, and self-assessment data uploaded by the users. The administrator will be able to download data for research and revise the health education information. The system also records the exact time and the length of time every user stays on each page of Family Care, Financial and Social Assistance, Knowledge Centre modules. This may indicate their information needs and interests. This information is quite valuable for medical staff so they can provide targeted information and support to the caregivers.In line with stakeholders’ suggestions, the smartphone app was made user friendly to both caregivers and children. The interface is colourful with bigger icons and the background is of bright colour. Some screen shots are given as examples to visualize the smartphone app in Appendix 2.
Discussion
Family caregivers have enormous burdens are in desperate need of professional and real-time support. Inspired by the idea of m-health, a smartphone app to support caregivers was developed based on findings from qualitative studies with caregivers, professional medical staffs and software engineers. A web-based administration portal was also developed to manage the app.
The protocol of the smartphone app was developed based on data collected from key informant interviews and three rounds of focus group discussions. Group discussion is an efficient way to collect participants’ suggestions and also stimulate new ideas in the brainstorming session. Additionally, a multidisciplinary panel of participants promotes communication across disciplines and increases their understanding of each other’s role in cancer care.
A couple of limitations should be noted for this study. Firstly, the participants were recruited from a single academic institution, and the sample size was relatively small. Therefore the findings may not be generalizable to caregivers from other regions of the country or other cultures. Secondly, “Care Assistant” is an app that only operates on the Android system. Computer and iOS based applications can be developed if we receive additional funding.
Future research is needed to examine whether “Care Assistant” meets expectations and whether transmitting health information is safe over the Internet. Our next step is to test the usability of this app. We will revise it according to users’ experience and the data collected. The aim is to make “Care Assistant” user-friendly and suitable to be promoted to a larger group of ALL caregivers. Then a randomized intervention study will be done to evaluate whether it meets the goal of supporting the caregivers. So far, incorporating smartphone app interventions into healthcare practice is just at the exploratory stage in China and other developed countries. A few studies focusing on this research field have developed apps to manage chronic diseases, such as diabetes, mental health problems, overweight, cancer, and chronic obstructive pulmonary disease. 16 Additionally, health-related smartphone apps could serve as the therapist’s extended arm into the daily life of the patients, and may improve patients’ or caregivers’ confidence in self-management or caregiving. 16 It is really challenging to introduce a new technology and develop a new tool in health care. However, it is also promising and meaningful to give caregivers of children with ALL real-time and effective support.
Footnotes
Acknowledgements
Changrong Yuan is the principal investigator of this research project who was responsible for the entire study design. Jingting Wang, Yuanyuan Wang, Fen Zhou, Yanyan Liu, Zhaohui Geng conducted the study, and Jingting Wang drafted the manuscript. Nengliang Yao performed critical revisions of the manuscript.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: The Science and Technology Commission of Shanghai Municipality, China (project no. 12410707900) and Oncology Nursing Society (ONS) Foundation.