
Abstract
Introduction
An increasing number of patients with diabetes mellitus has created a need for innovative delivery of specialized care not only by diabetes specialists but also by primary care providers (PCPs) as well. A potential avenue to address this need is training of PCPs by specialists via telehealth. The Veteran Affairs (VA) Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) program includes education and case-based learning for PCPs by a multidisciplinary specialty team utilizing videoconferencing technology.
Methods
Two PCPs completed a year of SCAN-ECHO diabetes training. These two PCPs set up “diabetes mini-clinics” to treat difficult-to-control high-risk patients with diabetes mellitus from their own panel and from their colleagues in the same community-based outpatient clinic (CBOC). We utilized a retrospective program evaluation by t-test using pre/post glycated hemoglobin (HbA1c) lab values after being seen by the two PCPs.
Results
A total of 39 patients, all with HbA1c > 9.0%, were seen in the two PCP mini-clinics over 15 months. The mean HbA1c improved from 10.2 ± 1.4% to 8.4 ± 1.8% (p < 0.001) over the average follow-up period of five months. This was not explained by system-wide changes or improvements.
Discussion
Care of veteran patients with poorly controlled diabetes by PCPs who participated in SCAN-ECHO program leads to improvement in glycemic control. This model of health care delivery can be effective in remote or rural areas with limited availability of specialists.
Introduction
Diabetes is a serious chronic medical disease managed thorough lifestyle interventions and pharmacological treatment. According to the Center for Disease Control, 26% of US residents aged 65 years and older had diabetes in 2010. 1 This number is only expected to grow in coming decades. 2 A continued increase in the population of individuals diagnosed with diabetes and pre-diabetes has created a need for efficient, competent delivery of specialized medical care not only by diabetes specialists but also by primary care providers (PCPs) as well.
Involving PCPs in expert or advanced care of chronic illnesses such as diabetes mellitus would be one way to provide efficient care to such a large population, especially in remote or rural areas. Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) is the Veterans Health Administration (VHA) version of virtual specialty support and training of primary care providers to treat patients with complex chronic illnesses, modeled on the project ECHO work done at the University of New Mexico in Albuquerque, USA. 3 Within the VHA there are five major sites for delivery of SCAN-ECHO diabetes training, Cleveland being one such site since the inception of the program in 2011. Our diabetes SCAN-ECHO program offers 24 sessions per year, each session consisting of 20 min didactic instruction on the clinical management of diabetes mellitus presented by the expert diabetes team from the main hospital, followed by two to three case studies presented by PCPs with discussion modulated by the expert team. The expert team provides the management recommendations at the end of the each case discussion. The sessions are held twice a month. The Cleveland team is comprised of an endocrinologist, a health psychologist, a nurse practitioner who is a certified diabetes educator (CDE) and a registered dietitian who is also a CDE. Team members take turns in presenting the pertinent diabetes-related topics (such as diagnosis of diabetes and prediabetes; is it type 1 or type 2 diabetes?; types of insulin and different regimen; non-insulin medications for diabetes; motivational interviewing; adherence; nutrition: common misconceptions; nutrition: when not to use calories chart). Previous studies related to use of the ECHO model in the care of diabetes mellitus have shown efficacy in improving providers’ diabetes knowledge and confidence level in caring for diabetic patients. 4 No study details outcomes related to glycemic control of the patients with diabetes in such a program. This evaluation aims to determine the efficacy of the Cleveland Veteran Affairs (VA)’s SCAN-ECHO program for diabetes mellitus by examining change in glycemic control in patients treated by participating PCPs.
Methods
Two of the PCPs, who completed one year of participation in the SCAN-ECHO diabetes training, initiated a quality improvement pilot project of diabetes “SCAN mini-clinics” at two remote rural outpatient sites within the Cleveland VA hospital network. Each primary care provider at the two diabetes mini-clinics was scheduled to see patients with diabetes mellitus in a half-day clinic for one to two times a month depending on the clinic size. This included patients from the practices of all the PCPs at that primary care center, including patients from their own clinic. The patients with poorest control of diabetes were offered these appointments. The majority of referred patients included those with glycated hemoglobin (HbA1c) > 9.0% identified by screening the diabetes registry maintained at Cleveland VA. Some overtreated patients with low HbA1c were also referred for safety reasons to help eliminate hypoglycemia. The PCPs who see patients at these clinics continue to attend the SCAN-ECHO sessions for diabetes and have a choice to present their cases in that session.
After discussion with the local Institutional Review Board (IRB) administrator, this quality improvement project was deemed exempt from the IRB approval process (with written documentation) as there was no systematic intervention and gathering of individual private data. The Standards for Quality Improvement Reporting Excellence (SQUIRE) guidelines 5 indicate that quality improvement work describes the specific aim (changes/improvements in care processes and patient outcomes) of the proposed intervention, specifies who (champions, supporters) and what (events, observations) triggered the decision to make changes, and why now (timing). 5 Quality improvement is described by SQUIRE as improvement efforts focused primarily on making care better at local sites, rather than on generating new, generalizable scientific knowledge. This was evaluation of a program which effected a change in delivery of health care at a local level.
We conducted a retrospective chart review of all patients seen in the SCAN-ECHO trained PCP diabetes mini-clinics starting 19 December 2012–28 March 2014. Of all the patients seen in the mini-clinics, only those patients who had HbA1c estimated before the first mini-clinic visit and any time after the last mini-clinic visit were included in this analysis (as some are still being followed-up). Two patients on insulin who were seen for a presenting problem of hypoglycemia were excluded from the data set although, appropriately, their HbA1c did come up. To see if change in HbA1c was a health-system wide improvement or unique to these SCAN-ECHO diabetes mini-clinics, we examined the trends in change in percentage of the patients with diabetes and HbA1c > 9.0% seen during one month at the beginning and during one month at the end of the same time frame as the SCAN-ECHO diabetes mini-clinics. Comparisons were made between the primary care centers where these two clinics were located to two other primary care clinics in the rural area which are about the same distance from the referral tertiary center. The comparison clinics were of approximately the same size, and the diabetes patients were given usual care by their primary care providers over the same time period. Results for the comparison clinics were given as percentages of all the veterans with diabetes seen in that month who had HbA1c > 9%.
Results are expressed as mean ± standard deviation (SD). Student’s t-test was used for statistical comparison.
Results
The total number of patients seen in the SCAN-ECHO diabetes mini-clinic at the two centers was 39. The average age of the patients seen in the SCAN-ECHO diabetes mini-clinics was 67.3 ± 7.3 years with a range of 53–91 years. The mean baseline HbA1c of the diabetes mini-clinic group was 10.2 ± 1.4%, indicating a patient population with poor glycemic control. The average body mass index was 34.8 ± 7.2 kg/m2 with a range from 24.4–52.7 kg/m2, indicating an obese population. A majority of the patients were seen for one to three clinic visits (mean = 2.4 visits).
This reflects data only from the patients seen by the two providers who participated in the diabetes Specialty Care Access Network-Extension for Community Healthcare Outcomes (SCAN-ECHO) training sessions. HbA1c: glycated hemoglobin.
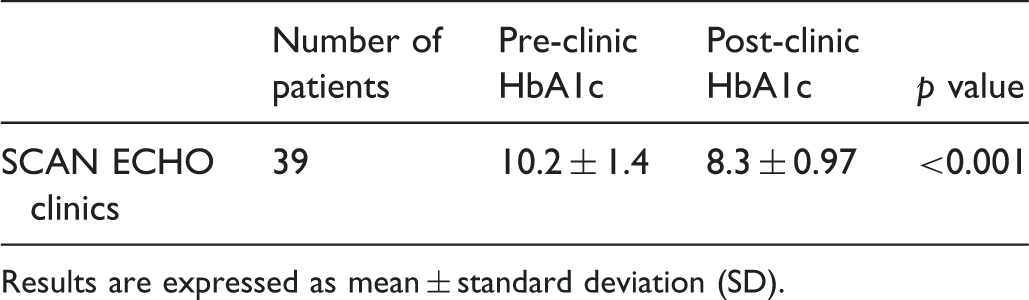
Results are expressed as mean ± standard deviation (SD).
Percentage of veterans with diabetes mellitus who had glycated hemoglobin (HbA1c > 9%) seen in different clinics over one month at the beginning and the end of the period of evaluation of diabetes mini-clinics.
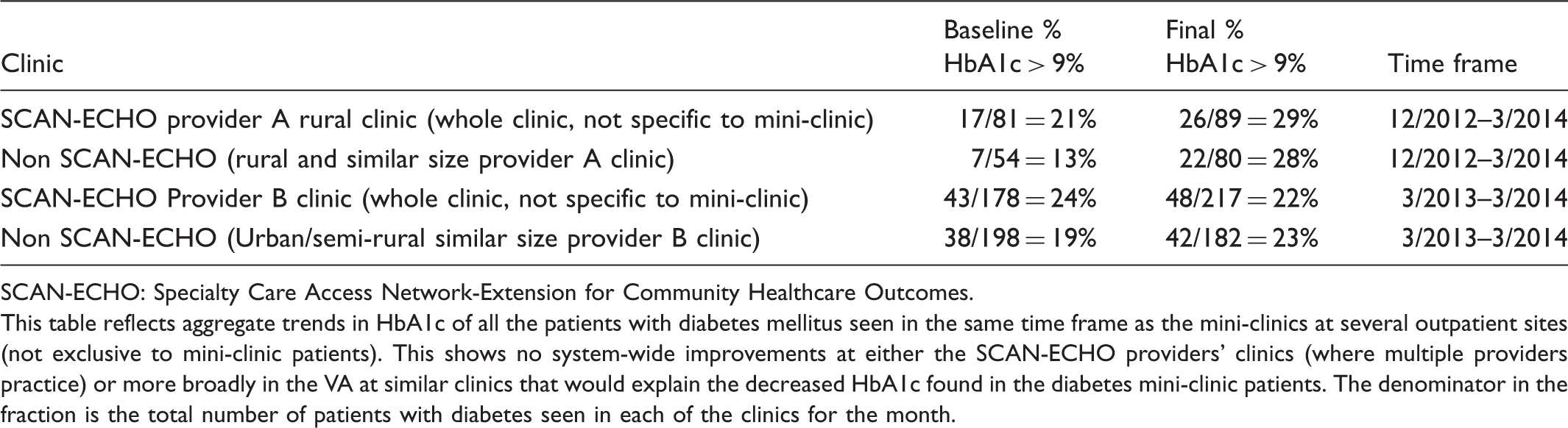
SCAN-ECHO: Specialty Care Access Network-Extension for Community Healthcare Outcomes.
This table reflects aggregate trends in HbA1c of all the patients with diabetes mellitus seen in the same time frame as the mini-clinics at several outpatient sites (not exclusive to mini-clinic patients). This shows no system-wide improvements at either the SCAN-ECHO providers’ clinics (where multiple providers practice) or more broadly in the VA at similar clinics that would explain the decreased HbA1c found in the diabetes mini-clinic patients. The denominator in the fraction is the total number of patients with diabetes seen in each of the clinics for the month.
Discussion
The efficacy of the ECHO program in management of chronic disease such as hepatitis C was demonstrated at University of New Mexico in Albuquerque, USA. 7 The ECHO model has subsequently been applied to the management of other diseases including diabetes mellitus. This model was used as a template for the SCAN-ECHO program in the Veteran Health System. It uses videoconferencing technology to foster collaboration between a diabetes specialist team and off-site rural PCPs. Each SCAN-ECHO session includes a didactic presentation along with peer-to-peer case presentations where patients are discussed and recommendations are made by the remote multidisciplinary specialty team. This leads to health care delivery with specialist team consultation for the management of diabetes in underserved areas. Goals for the VA SCAN-ECHO sessions include training expert PCPs and their team members as “specialist extenders” of diabetes specialty care at remote sites so that veterans would not need to travel long distances or deal with wait times in specialty clinics at the tertiary center. At the same time, it is expected that the case-based learning in this group environment will translate to better care for other diabetes patients managed by these PCPs in their primary care clinics in non-SCAN-ECHO settings.
However, data is limited on the studies demonstrating improvement in diabetes care using this model of care. Colleran et al. 8 recently demonstrated improvement in diabetes knowledge, attitudes and confidence in a small review of New Mexico community health workers (n = 23). The health workers participated in a three-day training session plus six months of weekly ECHO conferences. Results from standardized tests (Modified Diabetes Knowledge Test (mDKT), Diabetes Confidence Survey for Community Health Paraprofessionals (DCS-1) and the Diabetes Attitude Survey (DAS)) were used for pre/post evaluation. Results demonstrated significant improvements in diabetes knowledge, diabetes attitudes, and confidence in both clinical and nonclinical skills. Although the results are taken from a small sample, they indicate the viability of training community health workers with this form of remote virtual format.
Similarly, the US Air Force also surveyed providers after participation in an adopted ECHO diabetes model of training. 4 Fifty primary care providers (12 were either advanced practice nurses or physicians assistants) answered pre- and post-session knowledge and confidence levels along with intention to change their practice. The study indicated an increase in perceived diabetes knowledge and increased level of personal confidence for treating complex diabetes patients, although the response rate was low at 27.9%.
In our program evaluation we have demonstrated that the care provided by PCPs who participated in the SCAN-ECHO program leads to significant improvement in HbA1c for veterans with diabetes and poor glycemic control. The improvement in HbA1c demonstrated in the patients seen in the SCAN-ECHO diabetes mini-clinic is clinically quite significant and has occurred without these patients seeing a specialist. Since, overall, there was no change in prevalence of patients with poor diabetes glycemic control in the usual care comparison clinics, the improvement in glycemic control does not appear to be the result of some system wide improvement in glycemic control of patients with diabetes from other interventions.
Limitations of this program evaluation include that this was a retrospective analysis of the patients who agreed to be seen in the SCAN-ECHO diabetes mini-clinics. Since it is not a randomized study it does not remove the confounders which can affect the results. There would have been some patients with poor glycemic control who would have been offered appointments but refused to be seen in the clinic. It is possible that those patients who were motivated to make a change agreed to be seen in these clinics. Moreover, data used for comparison between the different clinics utilized aggregate clinic data. The lack of individualized patient data in the analysis limits the analysis of variance for the results and thus potential confounding variables could bias the outcome.
Our analysis demonstrates that using the SCAN-ECHO model, PCPs can deliver effective care for high-risk diabetes patients in improving glycemic control. This model can be used to provide care to diabetes patients in remote and distant sites. Future research may use the findings of this quality improvement project from SCAN-ECHO diabetes mini-clinics to proceed with a randomized-controlled study of usual care versus mini-clinics run by PCPs for high-risk diabetes patients.
Footnotes
Acknowledgements
The authors would like to acknowledge those who have helped develop and support the SCAN-ECHO project at the Cleveland VA Medical Center, including Ali Mchaourab, Stacey Hirth, Scott Ober, and C Boyd. They wish to acknowledge the work of Thomas Tambouratzis and Helen Rizi, the primary care providers of SCAN diabetes clinics. In addition, they would like to acknowledge the assistance of Kevin Young with some of the statistical analyses. The content of this manuscript presents the findings and conclusions of the authors and does not necessarily represent the VA.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AS is co-investigator on a grant to the Louis Stokes Cleveland VA institution from Novo Nordisk for multicentric clinical trials. Other authors have no conflict of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the SCAN-ECHO project was received from the Department of Veterans Affairs, Office of Specialty Care Transformation.