
Abstract
Introduction
We evaluated two modes of delivery of an inflammatory arthritis education program (“Prescription for Education” (RxEd)) in improving arthritis self-efficacy and other secondary outcomes.
Methods
We used a non-randomized, pre-post design to compare videoconferencing (R, remote using telemedicine) versus local (I, in-person) delivery of the program. Data were collected at baseline (T1), immediately following RxEd (T2), and at six months (T3). Self-report questionnaires served as the data collection tool. Measures included demographics, disorder-related, Arthritis Self-Efficacy Scale (SE), previous knowledge (Arthritis Community Research and Evaluation Unit (ACREU) rheumatoid arthritis knowledge questionnaire), coping efficacy, Illness Intrusiveness, and Effective Consumer Scale. Analysis included: baseline comparisons and longitudinal trends (R vs I groups); direct between-group comparisons; and Generalized Estimating Equations (GEE) analysis.
Results
A total of 123 persons attended the program (I: n = 36; R: n = 87) and 111 completed the baseline questionnaire (T1), with follow-up completed by 95% (n = 117) at T2 and 62% (n = 76) at T3. No significant baseline differences were found across patient characteristics and outcome measures. Both groups (R and I) showed immediate effect (improved arthritis SE, mean change (95% confidence interval (CI)): R 1.07 (0.67, 1.48); I 1.48 (0.74, 2.23)) after the program that diminished over six months (mean change (95% CI): R 0.45 (−0.1, 0.1); I 0.73 (−0.25, 1.7)). For each of the secondary outcomes, both groups showed similar trends for improvement (mean change scores (95% CI)) over time. GEE analysis did not show any meaningful differences between groups (R vs I) over time.
Discussion
Improvements in arthritis self-efficacy and secondary outcomes displayed similar trends for I and R participant groups.
Introduction
Inflammatory arthritis and patient education
Inflammatory arthritis is a chronic disease characterized by joint pain and stiffness that can lead to joint destruction. Rheumatoid arthritis, the most common of the inflammatory arthritis conditions, currently affects more than 272,000 Canadians, which represents 0.9% of the adult population. 1 In the next 30 years, this number will increase to 1.3%.
Patient education is an important component of arthritis care and complements medical treatment by helping people learn to effectively self-manage their disease.
Development and evaluation of the “Prescription for Education” program
The Prescription for Education (RxEd) program is a one-day interactive self-management educational program aimed at helping people with inflammatory arthritis manage their condition more effectively. RxEd was designed using a problem-based approach that encourages patients to take responsibility for the management of their disease. 2 A patient-based needs assessment and patient feedback guided the program development. An interprofessional arthritis care team, a person with arthritis, and clinical researchers were involved in creating the program content and delivering and adapting the program to patient needs. 2
The format of the program includes presentations followed by question and answers, panel discussions, small group learning, and case studies. It incorporates fundamental principles of patient education and adult learning best practices, as well as the integration of self-management strategies. The program is facilitated by an interprofessional team, including Advanced Clinician Practitioner in Arthritis Care (ACPAC) program-trained extended-role practitioners from St. Michael’s Hospital in Toronto, Ontario, Canada.
The RxEd program has demonstrated effectiveness in a wait-listed controlled study that showed improvement in arthritis self-efficacy and other health-related outcomes in people with inflammatory arthritis. 2 A number of other studies with a concurrent comparison group have also shown short and long-term (>1 year) positive effects for outcomes such as arthritis self-efficacy (short,3–9 long-term8–10), coping (short,8,11,12 long-term8,13,14), and arthritis knowledge (short,4,9,15–18 long-term9,17,19). Further, observational studies have shown that effective self-management of arthritis through education can reduce pain, decrease physician visits, and improve knowledge and behaviours related to arthritis.20,21
While the RxEd program has benefited patients who live in the greater Toronto area, the burden of travel excludes patients living in rural and northern Ontario communities where there is the highest prevalence of arthritic disease. 22 Arthritis care providers working in these communities recognized that their patients were at a distinct disadvantage with limited access to interprofessional patient education programs. In collaboration with their clinical colleagues in Toronto, they developed a plan to extend the RxEd program to their communities using telemedicine (i.e. videoconferencing) as a “distance learning” modality.
Telemedicine application in patient education
Telemedicine has been shown to improve access to healthcare services, particularly in sparsely populated areas.23,24 In doing so, it can improve the efficiency, quality, and timeliness of healthcare service provision. 23 Several studies have evaluated the use of telemedicine for medical consultation for musculoskeletal conditions including rheumatology25–28 and orthopaedics. 29 Most reported positive outcomes such as improved feedback to referring physicians and patients, effective case-based learning and transfer of knowledge, improved accessibility, and cost/time effectiveness. In recent years, there has been considerable growth in the use of telemedicine, particularly in the area of chronic disease management. 30 Several studies have utilized telemedicine for patient education and self-management programs in chronic disease.31–34 However, we have not identified any studies that specifically evaluated the use of telemedicine for the delivery of arthritis patient education.
This project included two objectives. Initially, we set out to evaluate the feasibility of using videoconferencing (telemedicine) to deliver the RxEd program. In another publication, we have reported process outcomes (i.e. recruitment rates, educator/facilitator reflective logs, and debriefing meetings), conducted qualitative interviews with participants to explore perceptions and expectations of the program, and collected feedback on the quality of the videoconferencing methods used to deliver the RxEd program. 35
The purpose of this paper is to report findings from our second objective, which was to compare two modes of delivery of the RxEd program, telemedicine versus direct face-to-face (in-person), in terms of improving arthritis self-efficacy and other secondary outcomes (arthritis knowledge, coping efficacy, illness intrusiveness, and effective consumer).
Methods
Study design
The impact of the RxEd program across two different modes of delivery was evaluated using a non-randomized, pre-post design (“Remote” (R) sites versus “In-person” (I) site). Participants completed self-report questionnaires at baseline (T1), immediately after the RxEd session (T2), and at six-month follow-up (T3) (refer to Figure 1).
Study design and participation.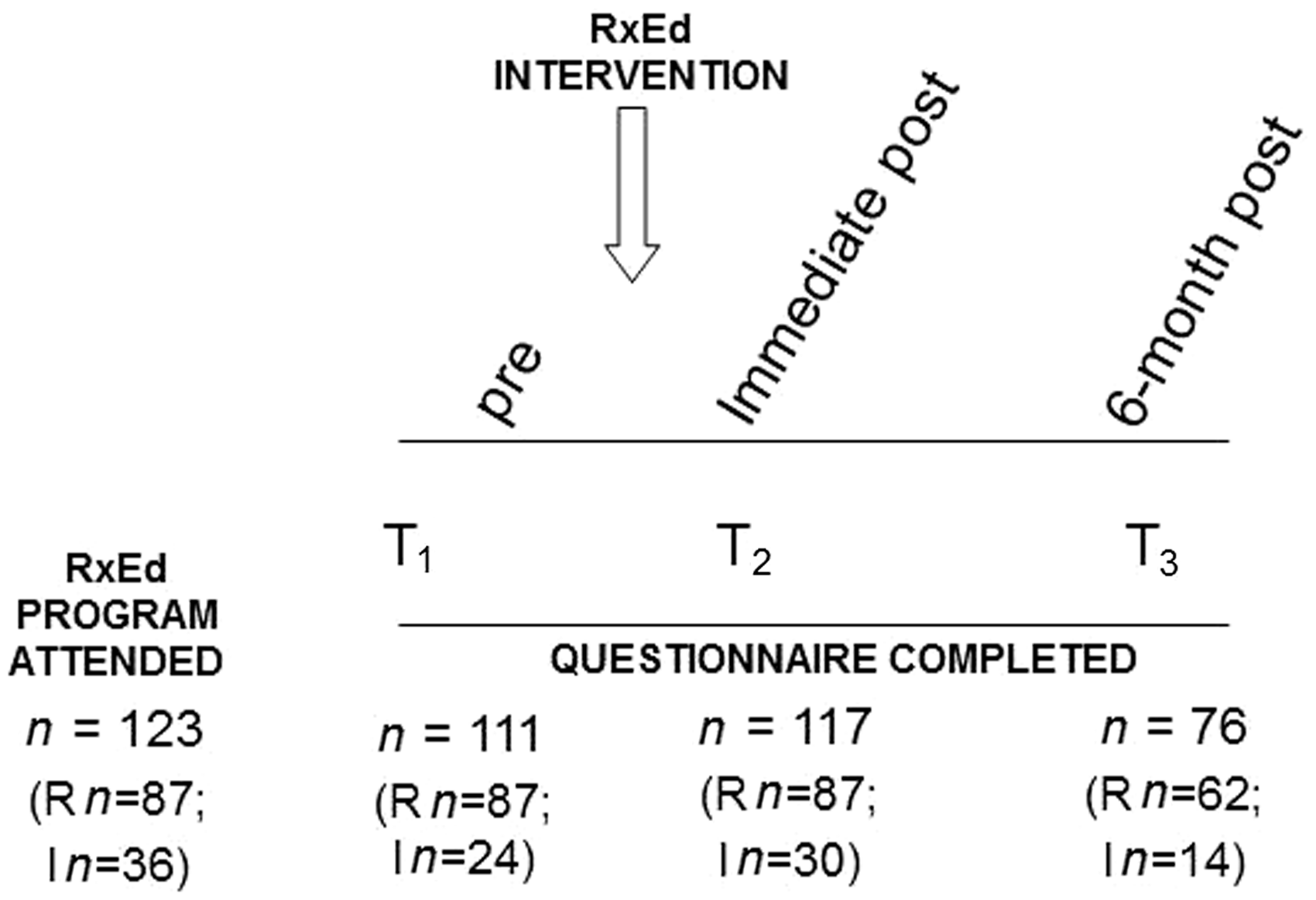
Participant selection
Patients were recruited from arthritis care clinics at an urban teaching hospital (I site), as well as through six ACPAC extended-role practitioners working across six rural and remote Ontario communities (R sites). Patients were eligible if they were 18 years of age or older, and had been diagnosed with one or more of the following inflammatory arthritic disorders: rheumatoid arthritis, psoriatic arthritis, lupus erythematosus, inflammatory bowel disease-related arthritis, gout, or ankylosing spondylitis. Excluded from the study were those who were unable to complete the questionnaires in English.
Intervention
The RxEd Telemedicine Program was delivered using multi-point videoconferencing over a secure virtual provider network supported by the Ontario Telemedicine Network.36 St. Michael’s Hospital served as the host site for each session. Presentations were communicated to participating locations using a Cisco TelePresence Quick Set C20 system. The dual-display functionality enabled simultaneous sharing of the presenting educator along with associated visual presentations. The remote participants linked to the conferences using H-323 compatible telepresence systems.
Educators and in-person study participants were based in a conference room at St. Michael’s Hospital. All sessions were moderated by an ACPAC therapist situated at the host site. At the same time, remote participants and local ACPAC therapists from six remote telemedicine locations in rural and northern Ontario joined the sessions.
The one-day RxEd program was adapted for telemedicine delivery through two workshops. First, the local RxEd educators received public speaking training and feedback on their presentations through consultation with an expert. Secondly, the Telemedicine Program, in collaboration with the Patient and Family Education Centre at St. Michael’s, developed a Videoconferencing Workshop that incorporated fundamental principles of patient education and adult learning, and telemedicine best practices. This interactive session was delivered using videoconferencing and provided to the educators and facilitators of the RxEd program to help them facilitate an effective educational program through telemedicine.
This study received Research Ethics Board approval at St. Michael’s Hospital (REB# 12-244).
Primary outcome
Self-efficacy is the degree of confidence one has in the ability to effectively manage some part of their health. 37 The literature on coping styles proposes that the sense that one has the ability to do something to control symptoms has been associated with improved adherence to health behaviours and adjustment to chronic disorders.38–41 Lorig et al. have developed a measure of self-efficacy with a focus on the management of pain, function, and other symptoms (20-items).39,42 A shortened 8-item scale has been tested on people with arthritis and demonstrated good internal consistency (alpha = 0.94). 43
Secondary outcomes
Knowledge about arthritis was assessed using the 31-item Arthritis Community Research and Evaluation Unit (ACREU) Rheumatoid Arthritis Knowledge Questionnaire. 44 Coping efficacy was assessed using a 4-item scale measuring respondents’ confidence in their current ability to manage or cope with different aspects of their condition.45,46 Studies have found that people’s assessment of their efficacy for coping is related to their coping efforts and well-being47,48 and their ability to adapt to musculoskeletal disorders. 45 Intrusiveness of illness on life was assessed using the 13-item Illness Intrusiveness scale to measure the degree to which an individual’s illness and/or its treatment interferes with life domains central to quality of life.49–53 The Effective Musculoskeletal Consumer Scale was used to measure an effective consumer who manages and participates in their care.54,55 A 17-item scale has been validated in various self-management interventions. 56
Patient demographics, disease activity (Rapid Assessment of Disease Activity Index), 57 and disability (8-item Health Assessment Questionnaire) were also assessed.43,58
Statistical methods
Baseline characteristics of participants by group. Data are reported as frequency (%) for categorical data and mean (SD) for continuous data.
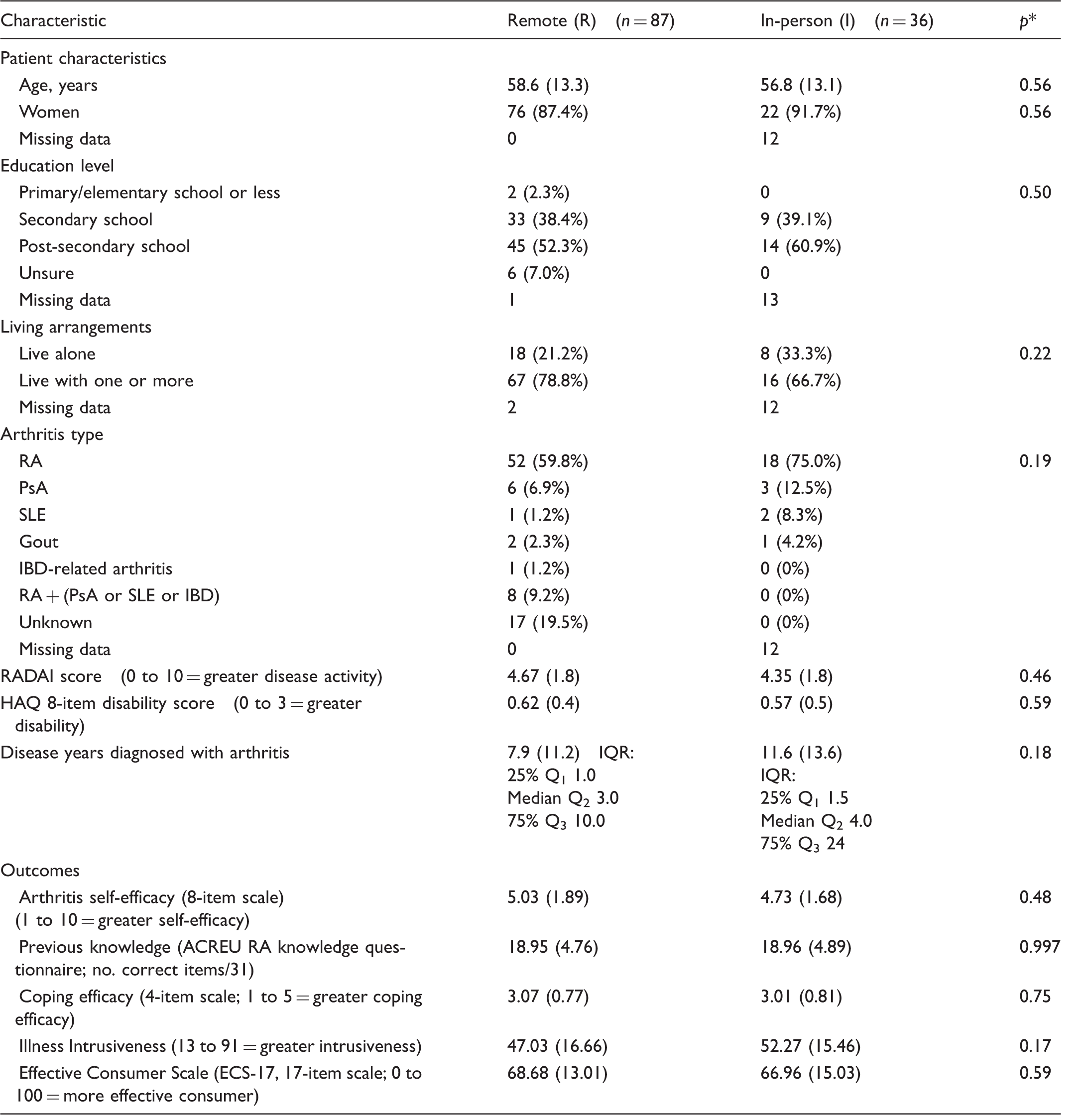
p: differences across groups (Chi-square tests for categorical variables and ANOVA for continuous variables).
RA: rheumatoid arthritis; PsA: psoriatic arthritis; SLE: systemic lupus erythematosus; IBD: inflammatory bowel disease; IQR: interquartile range; RADAI: Rapid Assessment of Disease Activity Index; HAQ: Health Assessment Questionnaire; ACREU: The Arthritis Community Research and Evaluation Unit; RxEd: Prescription for Education program.
A direct between-group comparison of the change in self-efficacy at immediate post-program and at six months was used to estimate the effect size. The standardized effect size between the two groups (R vs I) was calculated as the ratio of the treatment effect [ΔR–ΔI] to the pooled standard deviation (PSD) of these differences (i.e. (standardized effect size [T3–T1] = [mean ΔR–mean ΔI]/PSD)). 59 Dividing the estimated treatment effect by the variability (or uncertainty) of that estimate results in a standardized effect size, which enables a direct comparison between competing measures. Similar analyses were repeated for the secondary outcomes as exploratory and hypothesis-generating. Interpretation of the effects sizes was based on Cohen,60,61 where an effect size of 0.2 indicates a small effect, 0.5 a medium effect, and 0.8 a large effect.
We hypothesized that, at immediate post-program and at six months post-program, participants in both groups (R vs I) would demonstrate similar improvements (standardized effect size <0.2) in arthritis self-efficacy (primary outcome). We anticipated a similar trajectory for the other secondary outcomes. The expected results were based on our previous data from a pilot study of the RxEd program that demonstrated a positive impact on patient outcomes. 2
A pooled analysis, including all subjects and marking data as to whether the observations were made before or after the intervention, was used to estimate differences between pre and post intervention and to check whether similar for both groups (R vs I) for the primary and secondary outcomes. Generalized Estimating Equations (GEE) methods (identity link, normal errors, autoregressive(1)) were used to create a statistical model for the repeated measures (T1 to T3), using SAS PROC GENMOD. The model was set up for a pre-post design, estimating differences before and after intervention (see Figure 2). Group membership was also recorded as I and R. The main effect of the intervention (RxEd) over time was measured through the variable “time”. The interaction between the variables “group” and “time” was used to assess for differences in outcome between groups.
GEE: Generalized Estimating Equations model for repeated measures.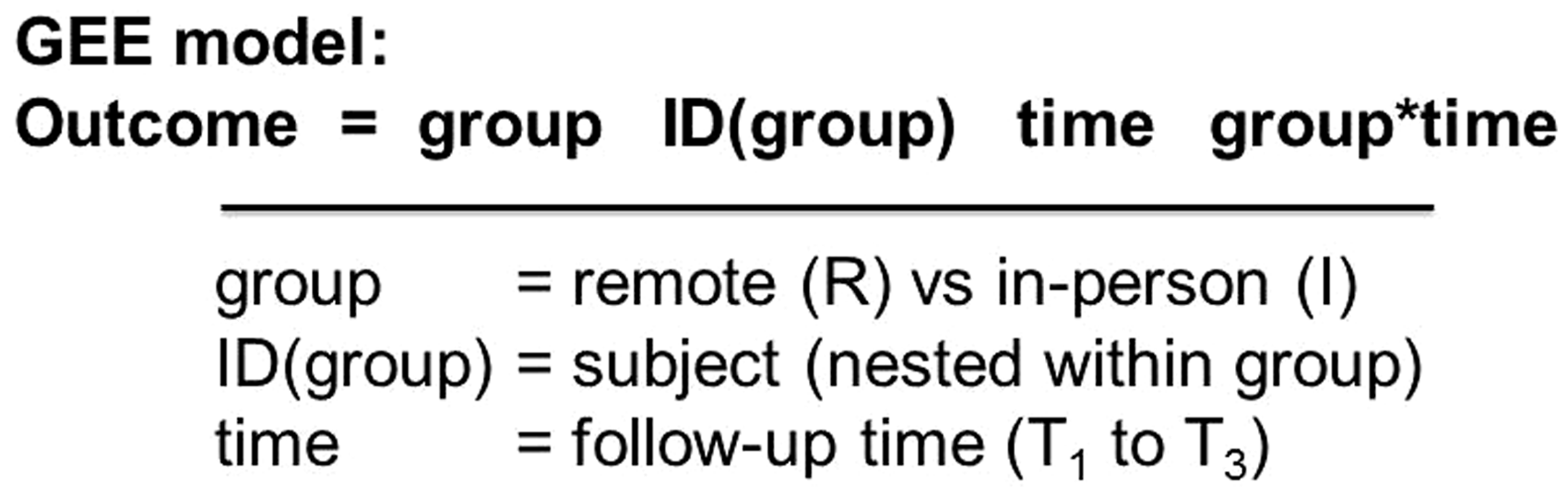
Results
A total of 123 persons attended the RxEd program − 36 were I participants and 87 were R participants. One hundred and eleven completed the baseline questionnaire (T1). Immediately after the RxEd session (T2) questionnaires were completed by 117 participants (95%), and six-month follow-up (T3) by 76 participants (62%) (Figure 1).
No significant baseline differences were identified between the R and I groups for any of the demographics, disease activity, or disability measures (Table 1). Similarly, no significant baseline differences were found for the primary and secondary outcomes (Table 1). Because 38% did not return the six-month follow-up survey, we looked for any differences between responders and non-responders. These groups were very similar across the patient characteristics and outcome measures assessed at baseline (p > 0.05). Responders reported higher education levels (63% having completed post-secondary school versus only 35% in non-responder group, p = 0.03).
Mean scores plotted over time revealed consistency in results across outcomes. For the primary outcome, both groups (I and R) showed immediate effect (improved arthritis self-efficacy) after the intervention that diminished over six months. Both groups showed similar trends for improvement for each of the secondary outcomes over time (Figure 3).
Longitudinal plots of mean scores over time.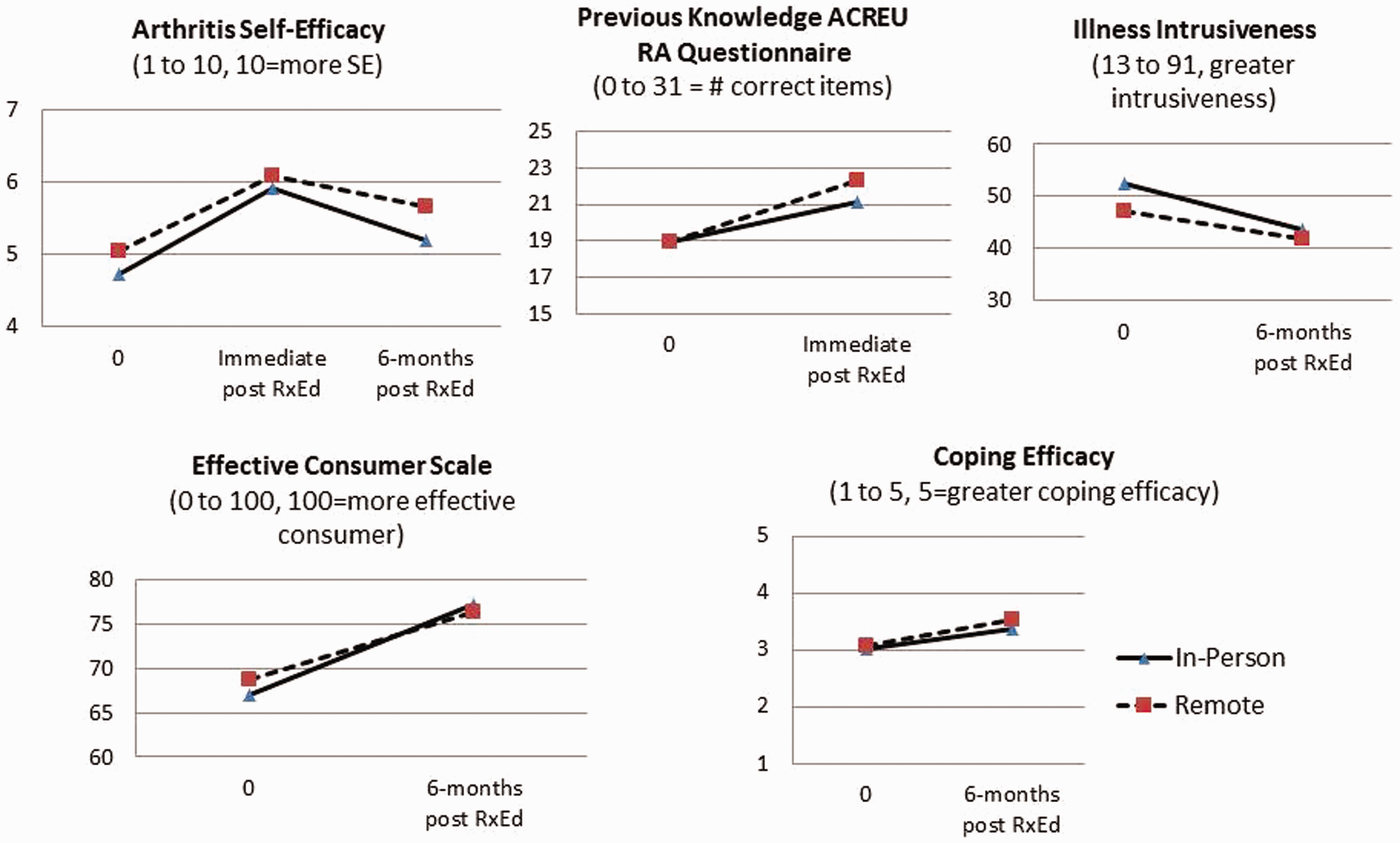
Analysis of direct between-group comparison (R vs I) of mean change at immediate post RxEd (T2) and standardized effect size.
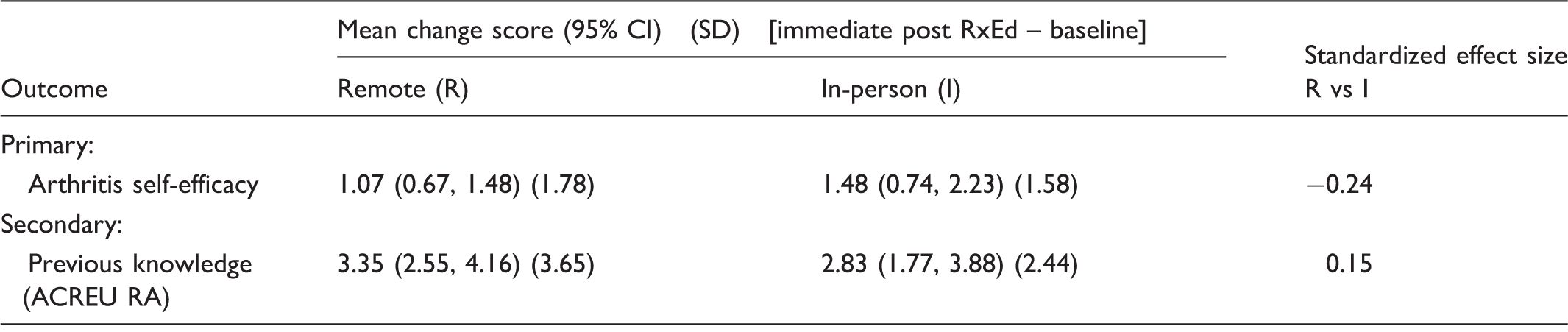
Positive change score = better; negative change score = worse; 95% CI = 95% confidence interval for mean change score (lower limit, upper limit); Standardized effect size = ratio of change between groups (mean change in R group – mean change I group) to PSD (pooled standard deviation) of these differences (Buchbinder et al., 1995). 59
Analysis of direct between-group comparison (R vs I) of mean change at six months (T3) and standardized effect size.
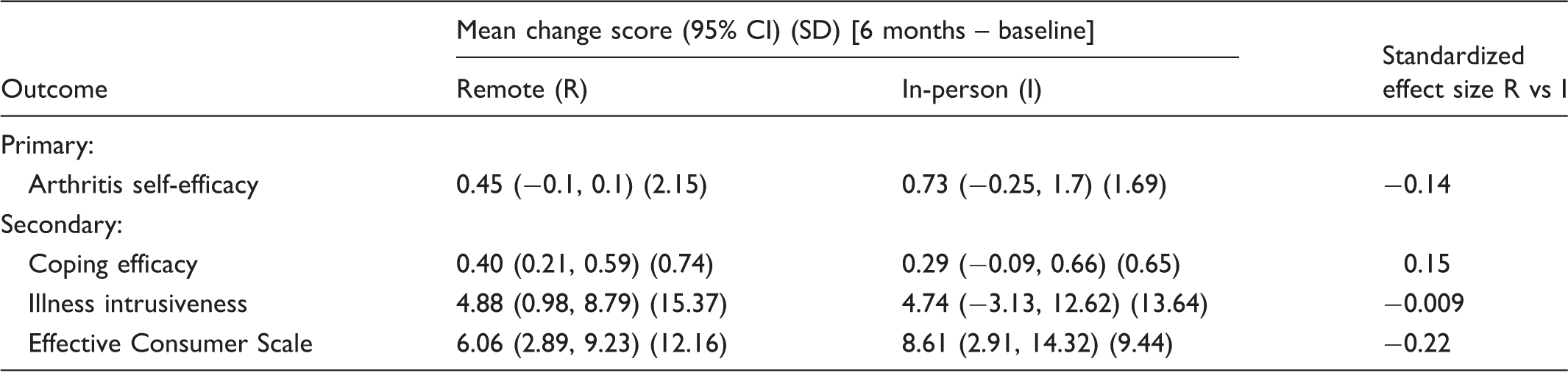
Positive change score = better; negative change score = worse; 95% CI = 95% confidence interval for mean (lower limit, upper limit); Standardized effect size = ratio of change between groups (mean change in R group – mean change I group) to PSD (pooled standard deviation) of these differences (Buchbinder et al., 1995). 59
For each of the secondary outcomes, the mean change and standard deviation of the mean change were very similar across groups (R vs I). This is further evident by the smaller standardized effect sizes (ranging from 0.009 to 0.22) when comparing R and I groups (see Tables 2 and 3). However, there are some differences in the 95% CI widths, largely due to the differences in the sample size of the groups, with the larger sample size (n = 87) of the R group having smaller 95% CIs and the majority (5 of 6 assessed) not including zero (or no change). Conversely, the smaller sample size (n = 36) of the in-person group had wider 95% CIs and more (3 of 6 assessed) including zero (or no change).
GEE interaction between “group” and “time” for primary and secondary outcomes.
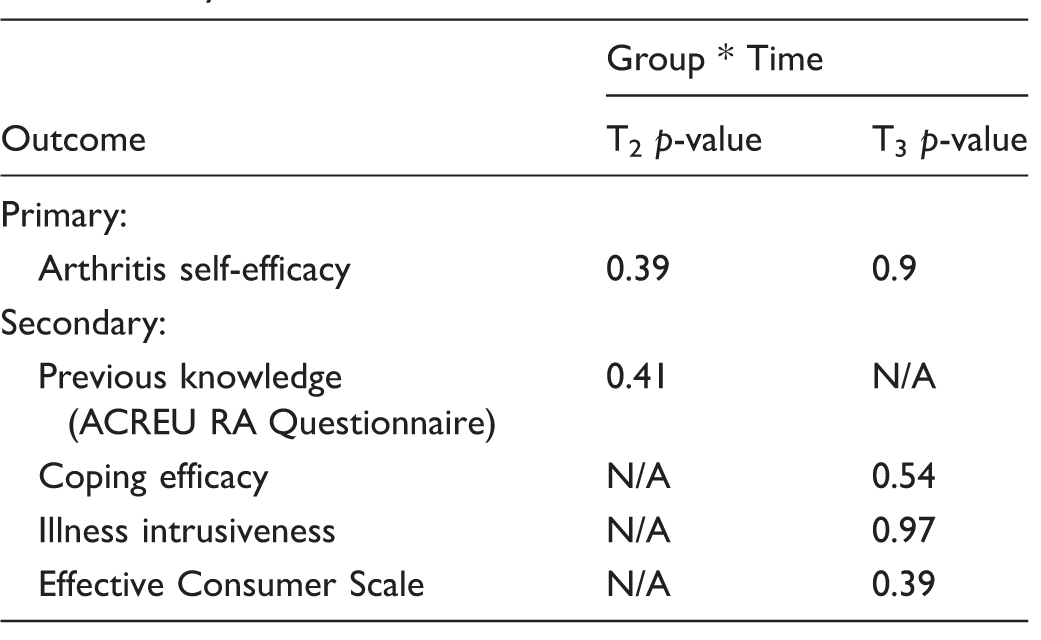
GEE: Generalized Estimating Equations; ACREU RA: The Arthritis Community Research and Evaluation Unit Rheumatoid Arthritis; N/A = outcome not assessed at this time point.
Main effect of RxEd intervention on primary and secondary outcomes.
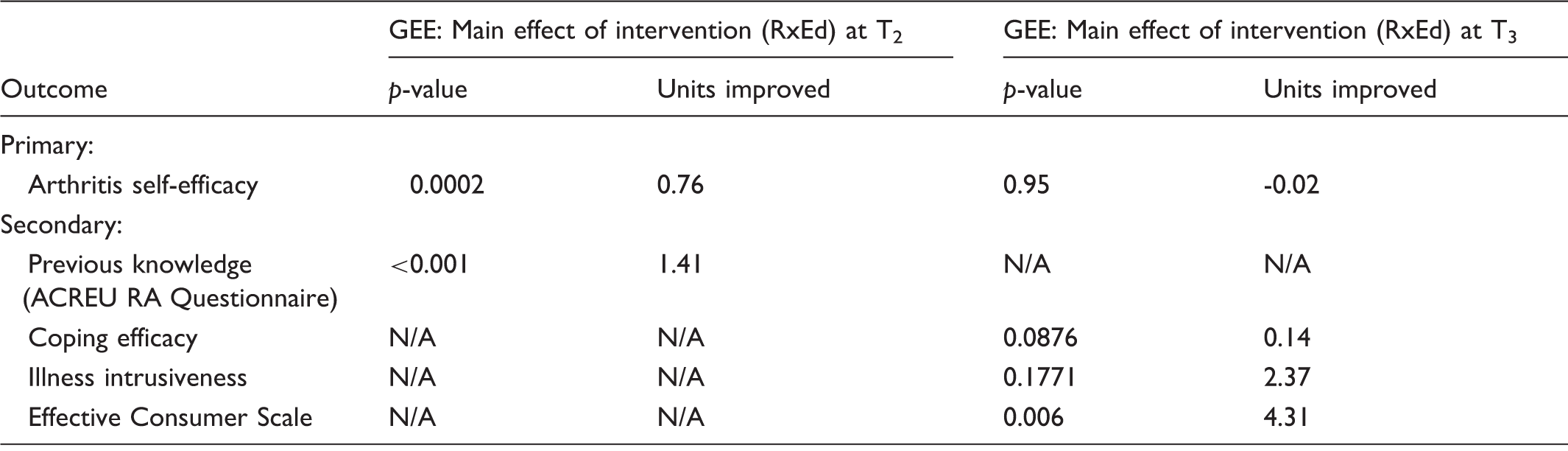
RxEd: Prescription for Education program; GEE: Generalized Estimating Equations; ACREU RA: The Arthritis Community Research and Evaluation Unit Rheumatoid Arthritis; N/A = outcome not assessed at this time point.
Discussion
The findings of this study support the extension of the RxEd program through telemedicine delivery to rural and remote communities in the province of Ontario. The results of this study confirm similar improvements are experienced (immediate and six months post-program) in arthritis self-efficacy and other secondary outcomes (arthritis knowledge and effective consumer) in participants attending the RxEd program remotely (by telemedicine delivery) compared to those attending in-person.
An earlier evaluation of the RxEd program (in-person) has demonstrated effectiveness in a wait-listed controlled study that showed improvement in arthritis self-efficacy and other health-related outcomes (arthritis knowledge, coping efficacy, and illness intrusiveness) in people with inflammatory arthritis. 2 The current study has replicated the pilot study results through similar trends of improvement (i.e. plots over time, mean change scores), and GEE main effect of the RxEd program in both I and R groups combined. Further, effect sizes (mean change/standard deviation of change) in the R participant group were mostly in the medium to large range (0.6–0.9) across the primary and secondary outcomes, and similar to those found in the intervention group of our pilot study.
Telemedicine has been used for patient education and self-management programs in a range of chronic diseases. Jaglal et al. (2013) 33 evaluated the delivery of a six-week chronic disease self-management program, comparing two telemedicine formats, point-to-point videoconferencing, and multi-point conference design. This study concluded that the self-management program could be successfully delivered using telemedicine and showed that outcomes were similar across the two groups (improved self-efficacy, positive health behaviours, and health status). 33 Another group explored the feasibility and efficacy of a telehealth stroke self-management program for rural participants and found this program to be well-received by all participants and was associated with improvement in patient outcomes, compared to a wait-listed control group.62,63 In addition, several studies have explored the feasibility and effectiveness of using a variety of telemedicine technologies for diabetes education.32,34,64,65 These studies have reported improvements in clinical outcomes and in assisting patients in the management of their disease. However, only a few have directly compared telemedicine to in-person delivery. As with our study, both found similar trends in outcomes over time in comparing different modes of delivery.32,34
There are some limitations to the study. First, we did not randomly allocate participants to R and I groups. This was deliberate since it was not possible to ask R participants to travel to an urban centre to receive arthritis education. However, we used a prospective design and rigorous statistical methods (GEE analysis) to evaluate the repeated measures data in a pooled analysis that compared the two groups. Our sample sizes were uneven (I group (n = 36) vs R group (n = 87)) due to the multiple sites participating remotely and the space limitations at the I site. The limitation of the sample size overall, and particularly the smaller of the two groups, comes into play primarily in the testing of the interaction (GEE analysis (Table 4)). Our sample size is sufficient to show changes in scores over time. However, the conclusion that there is no treatment by time interaction is impacted because we may have insufficient power to detect important differences in the treatment effect. For this reason, we have placed more emphasis on the similarities in the outcome trends through the analysis of between-group comparison (R vs I) of mean change scores and 95% CIs (Tables 2 and 3), as well as using longitudinal plots of mean scores over time (Figure 3). Finally, there was reasonable loss to follow-up at six months (62% responding). However, we looked for differences between responders and non-responders at T3 and found these groups were very similar across patient characteristics and outcome measures assessed at baseline.
The strengths of this program include the preparation of identical educational material given to participants, and the simultaneous delivery of the one-day program to the I and R sites. Secondly, the facilitator at each of the R sites was led by highly experienced, program-trained ACPACs, with the same training as those facilitators at the I site. Further, prior to conducting the study, efforts were made to provide additional training for the educators and facilitators of the program. The local RxEd educators received one session aimed at improving their public speaking and presentations skills. Secondly, an interactive videoconferencing workshop was conducted for both local educators and remote facilitators to provide telemedicine best practices training.
In conclusion, this study has shown that the RxEd program can be effectively delivered through telemedicine with a facilitator at R sites. Improvements in arthritis self-efficacy and other secondary outcomes were similar in R and I participant groups. The use of telemedicine technology to deliver an inflammatory arthritis education program to rural and remote communities provides an opportunity for people living in these underserviced areas to have access to interprofessional, educational programs. Future evaluation is needed to explore ways to maintain improvements in health outcomes through enhancements to the RxEd program. For example, offering small group education with health professionals as additional resources to manage their health condition. Further, combining the one-day program with a chronic disease self-management program (i.e. linked to local programs, or internet-based) could potentially lead to changes in behaviour and self-management activities.
Footnotes
Acknowledgements
In kind (time, program delivery, intellectual contribution): St. Michael’s Hospital RxEd team: Dr Louise Perlin, Angelo Papachristos, Rosaleen Crooks, Caroline Jones, Maureen Riley, Melissa Heidebrecht, Sasha Miles, Donna Scaffidi, Josie Rockman, Catherine Walther, and Kevin Curley; rural/remote Ontario sites: Jocelyne Murdoch, Mary Ellen Marcon, Tiffany Larsen, Anne MacLeod, and Lisa Denning; and St. Michael’s Telemedicine team: Mark Kinach and Rashmi Bhide.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by CIORA (Canadian Initiative for Outcomes in Rheumatology Care), 2012–2013 funding cycle.