
Abstract
Background
Telehealth neuropsychological services can increase the availability of specialised care for individuals in rural areas where barriers to these services are faced. As this practice becomes more commonplace, the reliability and validity of neuropsychological assessment administered by telehealth continues to be established. The Montreal Cognitive Assessment, a screener for general neurocognitive dysfunction, may be particularly useful since this measure can be given by telehealth with minimal adaptation.
Methods
Veterans from a rural area of the country who were referred to an outpatient neuropsychology clinic were administered the Montreal Cognitive Assessment either in-person or by telehealth by a clinician. A second clinician observed the administration in-person or by telehealth and independently scored the each participant’s performance. The inter-rater reliabilities across conditions were compared to assess for differences between in-person and telehealth consultations.
Results
The inter-rater reliability of the Montreal Cognitive Assessment across the three conditions of interest was acceptably high and values ranged from r = 0.88 to r = 0.98. Reliability correlations were compared and no significant differences among the conditions were observed (p’s > 0.10). Beyond reliability, univariate comparison of the absolute mean differences of clinician scores showed no significant differences among the actual raw scores of the three conditions tested, indicating good accuracy (p = 0.56).
Conclusions
The inter-rater reliabilities of Montreal Cognitive Assessment scores across conditions were all acceptably high, and administration of the Montreal Cognitive Assessment using telehealth technology did not significantly alter the total scores. Overall, the lack of significant differences suggests that administering the Montreal Cognitive Assessment by telehealth is reliable, accurate and well received by participants.
Keywords
Introduction
Elderly individuals living in rural areas face additional barriers to accessing essential medical care and social services, and this has become an increasing priority nationally.1,2 The elderly population in the USA (individuals over the age of 65 years) is not uniformly distributed, with older adults being most concentrated in rural areas, 3 and the age distribution of a location tends to become older as rurality increases. 4 A large portion of individuals living in rural areas are faced with a range of disabilities that are particularly prevalent in, and specific to, geriatric populations. Even normative physical changes associated with aging, such as impaired hearing, loss of vision, decreased mobility and other self-care issues, can increase the difficulty of attaining appropriate physical and mental health care in a rural setting.
Minimising and eliminating obstacles obstructing access to care is particularly important for individuals in rural areas with possible neurodegenerative disorders who are part of the ever increasing geriatric population. Driving restrictions, reliance on family and friends for assistance, restricted income, unfamiliarity with newer healthcare models, physical weakness and other medical diagnoses all increase the difficulty of obtaining needed care. These difficulties are even more pronounced when trying to access specialised services such as neuropsychological testing services which tend to be located in larger populous centres. Less than 25% of patients with dementia or probable dementia are diagnosed by their primary care physicians, 5 so improving access to specialised services may lead to earlier identification of dementia and improved clinical outcomes.
Access to quality care and specialised services is a particularly relevant issue for veterans. 6 Twenty-four percent of living veterans are in rural areas, and 36% of the veterans living in rural areas utilise the Veterans Affairs (VA) healthcare system. Veterans living in rural areas are at a higher risk for facing additional barriers to accessing adequate health care since they are also more likely to have long-standing service connected disabilities. 7 To help facilitate and address the specific needs of underserved veterans living in rural areas, the Office of Rural Health was established in 2007 to support a wide range of projects such as telemedicine, rural facilities and expansion of services into rural areas. The improvement of neuropsychological assessments administered by telehealth is critical since there is a large increase in neuropsychology requests now that Vietnam War veterans are experiencing dementing disorders along with the substantial increase in blast-related head injuries in younger veterans as a result of the Operation Enduring Freedom, Operation Iraqi Freedom, and Operation New Dawn conflicts.
The feasibility, acceptance and use of telehealth services continues to develop across a wide range of healthcare disciplines and specific disorders such as Parkinson’s disease.8–10 The expansion of telehealth has not been limited to one aspect of care but includes all stages of care including interview, examination, intervention and rehabilitation. These efforts also span across multiple fields such as telepsychiatry, teleneurology and telemental health. Cullum et al. 8 noted that many of these services rely inherently on verbal and visual communication and are particularly well suited for telehealth applications. Many forms of psychotherapy, diagnostic interviewing and case management appear to be appropriate for use over video teleconferencing equipment.11–13 The specific use of video teleconferencing to complete remote neuropsychological assessment is becoming increasingly feasible with growing acceptance among providers and patients.6,11,14,15 Patient acceptance and satisfaction of teleneuropsychology services are often as high as 98% with a large majority of participants reporting having no preference between in-person versus video assessment modalities. 16
Establishing reliability and validity is a critical component for the appropriate use of teleneuropsychology as an empirically supported practice. Studies assessing the reliability and validity of neurocognitive screening measures have had positive results.8,17–19 A systematic meta-analysis of remote neuropsychological testing looked at 12 studies that used common tests and concluded that videoconference administration did not clearly lead to inferior performance compared to on-site administration. 20 The only test where there was a consistent difference between remote and on-site observed scores was for the Boston Naming Test, and even this effect was small (one-tenth of a standard deviation (SD)). This systematic review highlights the relative lack of investigations into the use of video conferencing for neuropsychological assessment and provides a clear rational for the need of additional studies.
Neurocognitive screeners have received the most attention due to their brevity and significant impact on clinical decision making. The Mini-Mental State Exam (MMSE) has the most support with the first comparisons of face-to-face versus telehealth administration dating back to the late 1990s.21,22 Evidence suggesting that the administration of MMSE using telehealth is reliable and valid across a diverse set of populations and settings continues to grow.8,18,23 The reported intraclass correlations between face-to-face and telehealth administration have exceeded 0.85 across multiple studies in addition to high intra-rater agreement.8,24 One of the well-documented weaknesses of the MMSE is it’s poor sensitivity for mild cognitive impairment.24–27 To overcome this weakness in the MMSE several other neuropsychological measures have been evaluated for suitability for telehealth administration.8,28
The Montreal Cognitive Assessment (MoCA) 29 is a widely used neurocognitive screener that has a higher sensitivity to mild cognitive impairment compared to the MMSE. It assesses several cognitive domains including Visuospatial/Executive, Naming, Immediate and Delayed Memory, Attention, Language, Abstraction, and Orientation. Despite the popularity of this neuropsychological screener in person, very few investigations have looked the reliability and validity characteristics when administered by telehealth. Wong et al. 30 used a modified MoCA profile that excluded all of the visual components so that it could be administered remotely by phone to patients post ischaemic stroke/transient ischaemic attack. Participants were given the full MoCA in person as part of an annual assessment and then given the abbreviated telephone-based MoCA four weeks later. Face-to-face and telephone scores were highly correlated (r = 0.87), and total scores were on average only 1.8 points higher on the abbreviated protocol compared to the full version administered in person. Lindauer et al. 31 is the only known study that specifically gave the MoCA, along with other neurocognitive tests, via video telehealth. A test-retest design was used where participants were administered the MoCA at two time-points with a two-week interval in between in-person and telehealth administrations. Consistent with many telehealth studies, they made minimal modifications to accommodate the telehealth administration such as enlarged stimuli. Like the MMSE, the MoCA had very strong intraclass correlation coefficient (ICC) of 0.93 suggesting good reliability.
The limitation of the test-retest methodology is that it introduces practice effects and time influences into the method which can potentially influence overall results. This study used multiple raters simultaneously so that the participant would only be administered the MoCA at one time. The results of this study can be used in further demonstrating the reliability and accuracy of the MoCA. Further demonstrating the appropriateness of telehealth administration of the MoCA by telehealth will give mental health professionals additional options when choosing the best measure to give when completing telehealth assessments. Overall, this study represents another important step forward to support the practice of neuropsychological evaluation using telehealth technology.
Method
Participants
Seventeen participants (age, mean (SD) = 62.8 (14.50) years, 15 male/2 female) who were referred to an outpatient neuropsychology clinic for wide range of cognitive concerns were recruited for this project. All but one participant identified themselves as Caucasian. The mean length of education was 13.7 (1.8) years ranging from 11–18 years.
Procedure
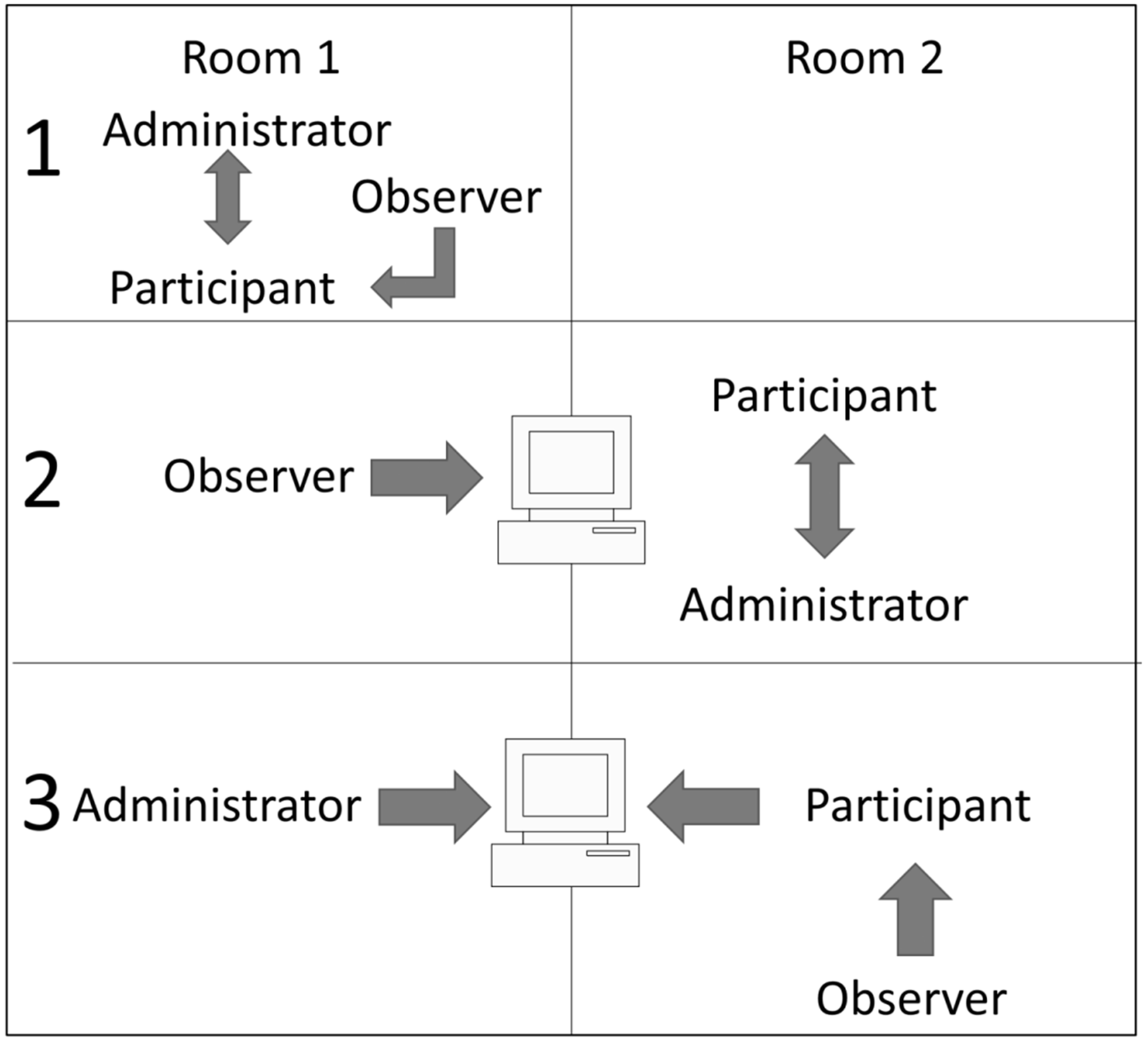
Patients were approached after completing their scheduled appointment in a general neuropsychology clinic and asked if they were interested in participating in this study. Individuals who expressed interest were informed that the clinic was validating a new way to administer a neurocognitive screener to improve access to neuropsychological assessment in rural areas and that they would be asked to complete a short cognitive screener either in person or using telehealth. Participants had the opportunity to take a short break while materials were prepared to help minimise fatigue. Individuals who agreed to participate completed the informed consent process approved by the institutional review board (IRB) and were randomly assigned to one of three conditions (see Figure 1) and then administered the geriatric version of the MoCA with enlarged visual stimuli.
Condition 1: this condition represented the control group where the participant was administered the MoCA face-to-face by a clinician physically present in the room. A second rater, also physically present in the room, observed the administration and scored the participants’ performances independently. Condition 2: the participant was administered the MoCA face-to-face by a physically present clinician; however, this time the second rater scored the participants’ responses independently from a different room using a video-based telehealth system. Condition 3: the roles of the clinicians from Condition 2 were reversed so that the clinician physically present in the room assumed the role of the independent rater, and the clinician in the remote location was administering the MoCA. Thus, in Condition 3, the participant was administered the MoCA by telehealth while the second rater in the room independently scored the administration. The rater physically in the room with the participant helped facilitate the administration by placing the MoCA stimuli in front of the participant and then holding the participants written responses up to the camera. They were not allowed to converse or engage with the participant in any other way. All instructions and participant questions were conducted using the telehealth system. Raters were not allowed to discuss the participant responses or collaborate in any other way.
Description of the three assigned conditions.
Videoconferencing equipment and setup
For this current project, the 384 kbit/s Internet connection available for use at our facility was used to connect two endpoints of two non-adjacent rooms within the facility. When the MoCA was administered by telehealth, the administrator sat at their work station 20 in away from a computer monitor mounted Cisco TelePresence Precision HD USB Web camera utilising Cisco Jabber Video for Telepresence Software. Participants in the non-adjacent room were seated approximately 72 in in front of a 32 in LCD television monitor equipped with a Cisco Telepresence System SX20 Quick Set with Precision HD 1080p that ran proprietary VA software.
Analysis
All analyses were completed using IBM SPSS Statistics version 21.0. The mean difference between the overall MoCA score across the three conditions was computed and the absolute agreement was calculated using ICCs.
Results
Participant characteristics.
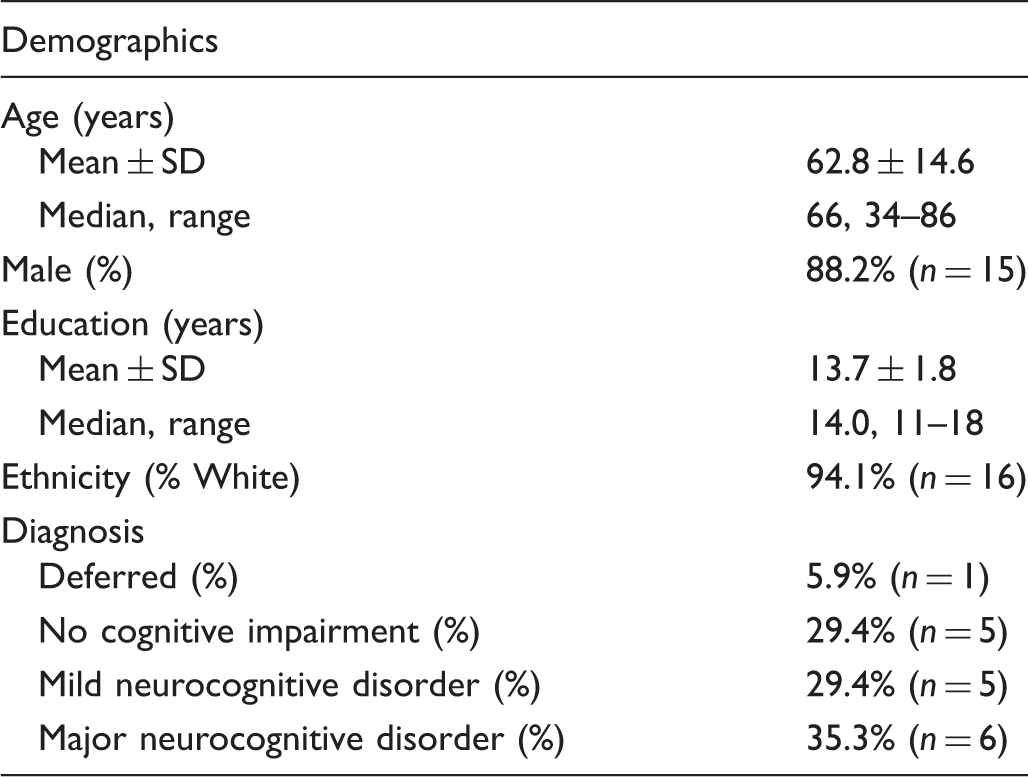
SD: standard deviation.
Mean (SD) Montreal Cognitive Assessment (MoCA) score agreement by condition.

ICC: intraclass correlation coefficient.
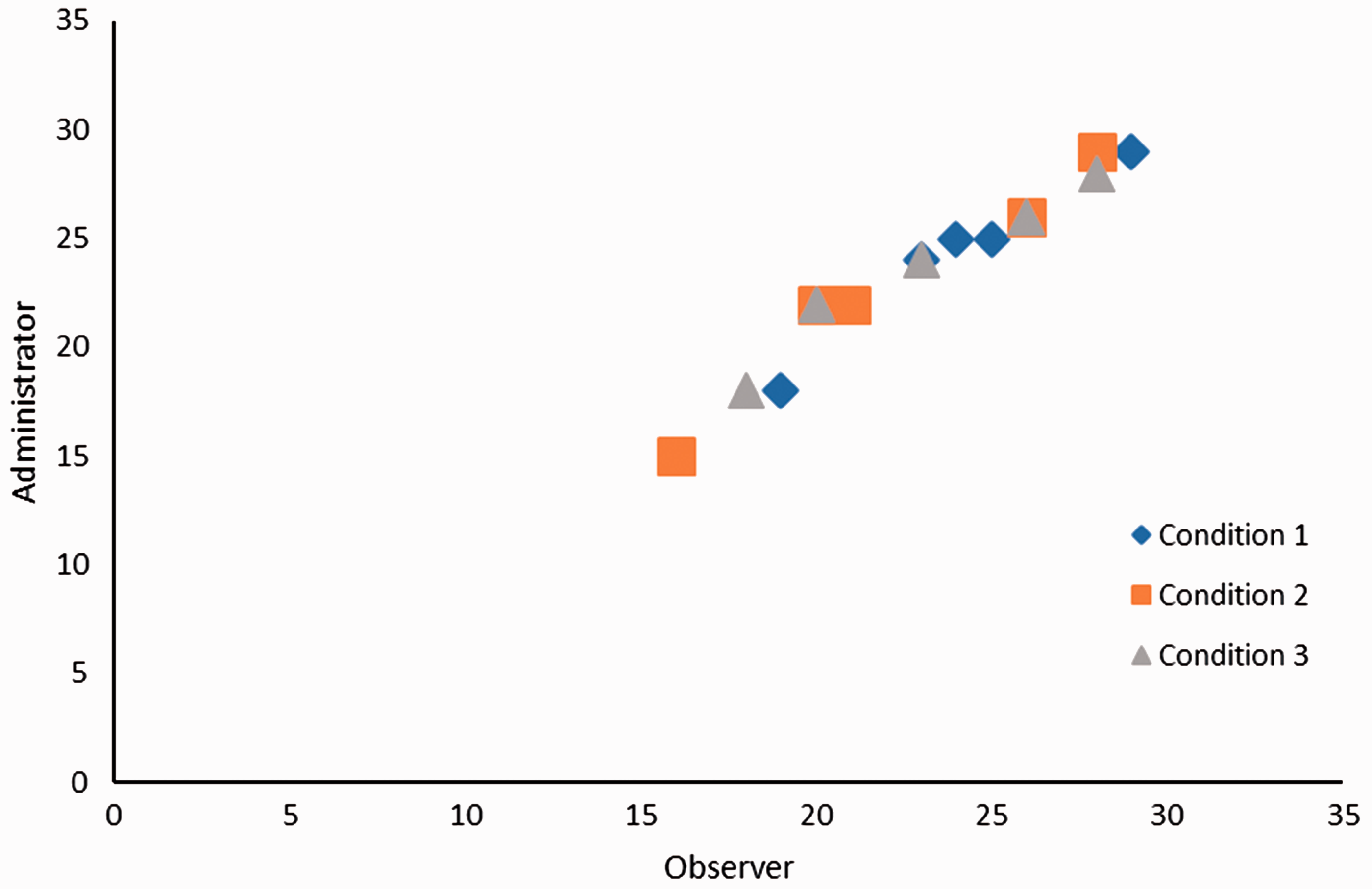
Scatterplot of MoCA scores separated by condition.
Montreal Cognitive Assessment (MoCA) score agreement by diagnosis.

ICC: intraclass correlation coefficient.
As expected the mean MoCA scored decreased as the severity of neurocognitive diagnosis increased. The highest agreement was observed within individuals not diagnosed with cognitive impairment (r = 0.99), and individuals in the mild cognitive impairment range had the lowest inter-rater agreement (r = 0.93). However, there was no meaningful decline in agreement based on severity of the diagnosis and the ICCs remained very high across all groups.
Discussion
With 24% of all veterans (5.3 m) living in rural areas, it is essential for specialty medical services within the VA to continue developing and improving ways to best serve these individuals. The number of individuals living with neurocognitive disorders is expected to rise to unprecedented levels in the next decade. Telehealth applications for neuropsychology services within the VA network are already numerous with the potential to significantly improve access, cost of care, efficiency and diagnostic accuracy far into the future. Establishing which tests are reliable and valid to give over telehealth and establishing what conditions should be met to engage in the practice of teleneuropsychology is an important step in this process. Ongoing research on telehealth-based neuropsychological assessment helps ensure patient and provider safety alike.
The results of this study are consistent with the original hypothesis that administering a cognitive screening tool, the MoCA, using videoconferencing equipment, would not have a significant negative impact on the reliability or validity of the test. When two raters independently scored the performance of participants, there was very high agreement across all conditions. No meaningful decrease in the absolute agreement between raters was observed when the test was either observed remotely or administered by telehealth. No decease in the overall performance of the participants was seen when the MoCA was administered by telehealth which supports not only the reliability but also the validity of giving this neurocognitive screener by telehealth. These findings are consistent with the ever growing body of evidence showing high agreement between tests given face-to-face and remotely.8,32 The agreement is marginally higher in the current study, but it is suspected that this reflects the minimal amount of facilitation that the raters in the room provided to each participant. Even this slight provision of assistance could minimise measurement error by helping the participants feel more comfortable, stay oriented to the task and ensure that written responses were clearly seen over the videoconference system. This study adds to the growing body of research suggesting that tele-neuropsychological assessment is an appropriate way to increase the availability of neuropsychological assessment services to individuals who are unable to otherwise access this type of specialised service.
This study indicates that teleneuropsychological assessment for individuals diagnosed with either major or mild neurocognitive impairments is feasible, which is consistent with the use of telemedicine in other clinical populations.9,10 These participants were able to successfully complete the testing by telehealth and their scores appeared as reliable and accurate as when the test was given in-person. This may have significant impact going forward since individuals experiencing cognitive decline are those most likely to face the largest barriers to accessing speciality care services. While not formally measured, participants with major neurocognitive impairments reported that they felt comfortable interacting with an evaluator by telehealth and felt that the actual setup and execution of the testing was fluid and not aversive. This is important and beneficial, considering the role of remote testing as part of more encompassing treatment protocols for individuals experiencing cognitive decline. It is becoming increasingly clear that the use of the MoCA, or other brief cognitive screeners, can be incorporated into the larger effort to provide both initial evaluation and sustained clinical intervention for patients using video telehealth. 33 Several participants from rural areas commented on their desire to utilise telehealth services through their local community based outpatient clinics in the near future.
For this study, the alternate rater in Condition 3 was allowed to help manipulate the test stimuli to orient the participant to an area of the sheet and to help the administrator get a clear view of the participants written responses. This approach has been utilised to differing degrees in other studies that have included telehealth clinical technicians.12,29 This may have helped improve agreement. This approach was chosen at the onset of the study since the VA often has telehealth technicians present with patients to help administer these types of procedures, overcome technical difficulties, and to improve the overall experience of the patient. In many ways, having the observer present and slightly active during the procedure is a more accurate representation of how this procedure could be used within the VA healthcare system and helps determine the positive effects of having a second professional present with the patient when remote testing is being completed.
Limitations to this study include the small sample size and cross-sectional design. Despite the small sample size and cross-sectional design, the conclusions are unlikely to significantly change even if more participants were added to the study. The highly select sample characteristics of the participants for this study inherently decreases the external validity of the findings. Additional large studies that address the influence of education, more severe cognitive impairments and older age would be particularly useful in the future.
Conclusions
The intraclass coefficients and inter-rater reliabilities of the neuropsychological screener scores across all conditions were all acceptably high, and administration of the MoCA using telehealth technology did not significantly alter the total scores. The reliability of the MoCA when administered and scored using videoconferencing equipment did not decrease in the subset of participants with the highest level of cognitive difficulties. Overall, the lack of significant differences suggests that administering the MoCA neuropsychological by telehealth is reliable, accurate and well received by participants. Additional research to further assess the performance of this measure over telehealth in different populations will continue to be useful.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: N DeYoung was the Neuropsychology Fellow at the Salem Veteran Affairs Medical Center at the time of the study. BV Shenal is the director of the Center for Neurocognitive Services at the Salem Veteran Affairs Medical Center.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.