
Abstract
Introduction
One-third of the Australian population lives outside major cities and this group has worse health outcomes. Telehealth is becoming an accepted way to improve patient access to specialist healthcare. Over 200,000 Australian’s have hepatitis C virus (HCV) and new treatments are very effective and well tolerated. We aim to demonstrate that HCV treatment utilising telehealth support for care delivery has cure rates similar to onsite care in clinical trials. We also report length of consultation and calculate reductions in travel and carbon output.
Methods
Patient demographic, clinical, and treatment outcome data were collected prospectively from hospital software and analysed retrospectively. This was an audit of all patients treated for HCV in one year from a single tertiary hospital that included telehealth in their care delivery.
Results
Sustained virological response was achieved in 51/52 (98%) patients with completed treatment courses, and 51/58 (88%) of those who had a planned telehealth consultation as part of their management. A median of 634 km of patient travel was saved per telehealth consultation.
Discussion
We found that a telehealth-supported outreach programme for patients in regional Australia with HCV produced similar outcomes to clinical trials. There was a considerable saving in time and cost for the patients and significant environmental benefit through the reduction in carbon footprint associated with travel to distant specialist health services. We conclude that telehealth facilitated outreach is a feasible and effective way to access HCV treatment and cure in regional Australia.
Introduction
Hepatitis C virus infection (HCV) is a significant health problem in Australia affecting over 200,000 people, or 1% of the population. 1 Many infected individuals do not live in major cities, 2 and so access to care is more limited and health outcomes are worse.2,3,4 Most HCV is acquired through injecting-drug use.4,5 In Australia, over 28% of the population were born in other countries, 6 including many immigrants originating from countries with reported high rates of HCV.6,7 The regional population also has higher rates of obesity and alcohol consumption, which are associated with poor liver health. 8
Prior to 2016, only approximately 20,000 individuals had received HCV treatment.4,5 This was mainly because the available treatment options, interferon and ribavirin, had suboptimal cure rates and high levels of toxicity. However, direct-acting antiviral therapy (DAA) has revolutionised HCV treatment demonstrating high efficacy and low toxicity. Since March 2016, this has been subsidised by the Australian Government for the treatment of all adults with HCV.4,5 By the end of June 2017 over 43,000 people had commenced with DAA treatment. 9 Without treatment, a significant number of people living with HCV are expected to develop major morbidity including cirrhosis and hepatocellular carcinoma. 10
Tertiary hospital specialist centres have been at the forefront of treatment delivery to this cohort, but the wide geographic distribution of Australia’s population has meant that patients often have to travel considerable distances, and as a result many have not yet accessed care.
The increasing availability of internet-based videoconferencing platforms has provided unprecedented capacity to manage patients remotely. A computer with a webcam and speaker, and a reasonable speed internet connection is all that is necessary to conduct a consultation. 11 Telehealth is well-accepted by patients and can improve healthcare efficiency. 12 The Victorian Infectious Diseases Service (VIDS) currently provides medical consultations via telehealth for rural and regional patients. This clinic was initially established for refugees and immigrants who, on arrival in Australia, settled in regional areas. 11 It has now expanded to include patients with HCV who can be seen in conjunction with local general practitioners (GPs).
Previously described successful hepatitis C management via telehealth has involved specialists providing advice to treating clinicians at remote sites, rather than direct clinical consultations with patients 13 or intensive review. 14 More recently, a large increase in the use of telehealth for HCV care has been described 15 and an international database analysis has shown good clinical outcomes using telehealth. 16 Our study outlines the outcomes of HCV treatment supplemented with the use of telehealth to both increase access to care and reduce patient travel.
The purpose of this study was to determine the virological outcomes of telehealth-supported HCV management and to compare these with results achieved in clinical trials.
The primary outcome was the rate of sustained virological response (SVR) achieved 12 weeks after completion of therapy (SVR12) amongst patients treated for HCV who had telehealth included as part of their management.
Secondary outcomes were the patient travel distance saved through the use of telehealth consultations and the reduction in carbon output that this was expected to have.
Materials and methods
The study was part of a quality audit of the hepatitis outreach service. Data were collected prospectively and analysed retrospectively. Ethics approval was received from the Royal Melbourne Hospital (RMH) Human Research and Ethics Committee.
This study was conducted in conjunction with the VIDS integrated hepatitis C service (IHCS) at the RMH. The IHCS provides outreach services to smaller regional cities through both regular visits by infectious disease specialists providing onsite clinics, and a nurse who works in an outreach capacity and provides support for HCV patients, including facilitating telehealth consultations. The nurse ensures appropriate patient workup occurs before the specialist appointment. All regional HCV patients seen via the IHCS are considered for telehealth management. Any patients referred to the service with decompensated cirrhosis were redirected for specialist onsite gastroenterology management.
All patients who had a telehealth appointment from the RMH for the management of HCV in the 12 months from 1 March 2016 and who were on treatment were included. This study included patients with multiple genotypes and also some patients with compensated cirrhosis. Patients either commenced treatment at outreach clinics and then had ongoing follow-up via telehealth or had treatment commenced during a telehealth consultation with ongoing follow-up through either telehealth or through outreach clinics. Patients were not required to have any onsite visits. Patients were commenced on treatment at the first specialist visit based on patient preparedness and the availability of sufficient clinical information. Patients then had a first follow-up appointment 4–6 weeks after commencement of treatment. Treatment selection was based on Australian Clinical Practice Guidelines.4,5 The patient treatment outcome was determined by a blood test for the presence of HCV performed at least 12 weeks after completion of therapy (SVR12).
During telehealth consultations, patients attended their local GP’s clinic while the specialist was located at the RMH. Although the patient attended the GP’s clinic, a health practitioner was not always present with them during every consultation. The IHCS nurse was available for telephone advice and support in addition to the specialist consultations.
Clinical data were collected from the clinical software (CAReHR®) used within the clinic for patient management.
Also measured was patient travel kilometres saved through not attending the clinic in person and the reduced carbon production due to reduced travel (assuming the Australian average for passenger cars of 258 g of carbon produced per kilometre). 17 Travel data were based on the patient’s home address postcode and the address where the telehealth consultation took place. Duration of the consultation and any technical difficulties were recorded by the tertiary hospital specialist.
Results
In the 12 months from March 1, 2016, 58 patients were treated for hepatitis C via telehealth. The mean age was 51 years and 76% of patients were male. The most common genotype was genotype 1 (36 patients) and then genotype 3 (20 patients). The majority (34) had their treatment commenced at an onsite visit and 24 had treatment commenced during a telehealth consultation. One patient of Afghan descent required the use of a telephone interpreter during the telehealth consultation.
Thirteen patients had previously failed treatment with pegylated interferon and ribavirin and one patient who was lost to follow-up also had previous DAA treatment (boceprevir). No patients were hepatitis B surface antigen positive.
Eleven patients had cirrhosis based on a Fibroscan® score above 12.5 kPa but none had decompensated cirrhosis. Patients with cirrhosis had liver ultrasound performed for hepatocellular carcinoma (HCC) screening, and gastroscopy referral where indicated. After completion of treatment when ongoing HCC screening was required, this was organised through the local GP with the support of the IHCS. Gastroscopy was performed by gastroenterologists, where available locally, or alternatively through referral to a tertiary hospital.
Treatment included sofosbuvir/ledipasvir for 34 patients and 24 patients had sofosbuvir and daclatasvir. Twenty patients had genotype 3 diseases, and all received a combination of sofosbuvir and daclatasvir. Genotype 3 patients were treated for 12 weeks, or for 24 weeks if patients had cirrhosis or had previously failed treatment. Thirty-six patients had genotype 1 disease, 33 of whom received sofosbuvir/ledipasvir and three received sofosbuvir and daclatasvir (due to drug interactions). Six patients with genotype 1 HCV, viral loads of less than 6 million IU, and no cirrhosis had short course 8-week treatment. The other 30 genotype 1 patients had 12 weeks of treatment. The single patient with genotype 2 HCV received 12 weeks of sofosbuvir and daclatasvir, and the single genotype 6 patient received 12 weeks of sofosbuvir/ledipasvir. Two patients had co-infection with HIV, both of whom achieved an SVR.
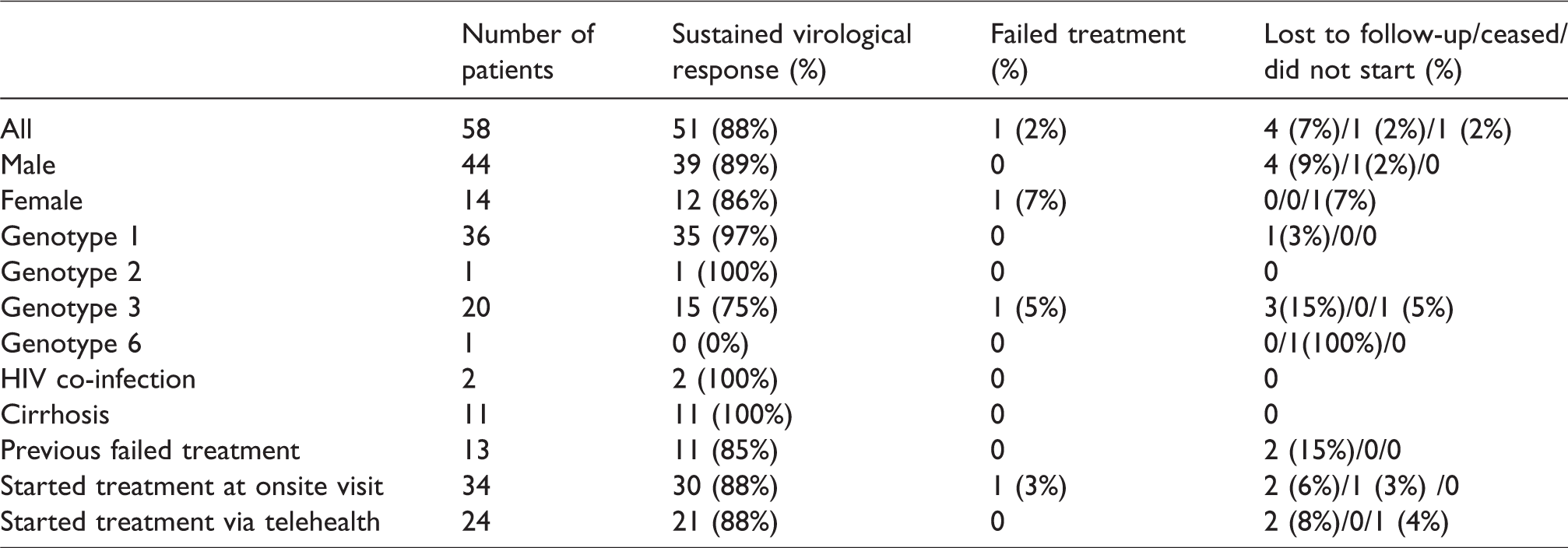
Based on clinical trials using intention to treat analysis, the expected SVR rates for hepatitis C genotype 1 treated with 8–12 weeks of sofosbuvir and ledipasvir is 95–99%18,19 in previously untreated patients, and 94% in previously treated patients.20,21 For genotype 3, SVR rates of 86–97% 22 are reported after treatment with sofosbuvir and daclatasvir. In our cohort, SVR was achieved in 51 patients. One patient had a relapse and one patient withdrew from treatment for personal reasons. One patient did not start the prescribed treatment and four were lost to follow-up.
The SVR rate amongst this cohort for those who had blood tested for HCV at least 12 weeks after completion of treatment was 51/52 (98%; comparable to a per protocol analysis). Amongst all those who had a planned telehealth consultation as part of their management 51/58 (88%) achieved an SVR (Table 1). Of those patients who commenced treatment 51/57 (89%) achieved an SVR (comparable to a modified intention to treat analysis in a randomised trial). All 11 cirrhotic patients achieved an SVR (eight with genotype 1 and three with genotype 3). Only one patient (genotype 3, not cirrhotic, no previous treatment, treatment commenced onsite) has had a known relapse after completing a full treatment course (12 weeks of sofosbuvir and daclatasvir). The relapse was with genotype 3 virus. The patient had ongoing risk factors for reinfection but unfortunately a stored sample was not available for comparison viral sequencing. Patients who were lost to follow-up had received multiple attempts at contact by both the local site staff and the IHCS, using phone and written communication.
Patient outcomes.
The median travel avoided for each telehealth consultation was 634 km (mean 626 km) and each patient had a median of three (mean 3.06) visits during their treatment course, of which a median of two (mean 2.4) were telehealth consultations. For one year, an estimated 86,720 km were saved through seeing patients via telehealth. This will have reduced the carbon output by a total of 22.37 tonnes, assuming that the trips avoided would otherwise have been completed by car.17,23,24
Technical difficulties occurred in less than 10% of consultations and the mean telehealth consultation duration was 15 min or less (83% of visits were for treatment continuation and 17% for treatment initiation).
Discussion
Health outcomes for those living in regional Australia are worse than for those living in major cities. 3 This is also the case in regional areas of other developed countries. 25 The availability of specialists in regional areas is lower than in capital cities 8 and it has been demonstrated that fibrosis scores are higher in regional HCV patients, suggesting later access to care. 26 Telehealth is one way of reducing barriers to care and ensuring that a person’s place of residence does not negatively impact on their health outcomes. The use of telehealth is expanding rapidly both in the number of users and in the range of areas of healthcare in which it is used. 27 With the introduction of novel modes of healthcare delivery, it is important to demonstrate similar health outcomes to the current method of care.
The availability of DAAs has revolutionised HCV care and made cure a reality for many patients. 28 Studies of real-world treatment outcomes for HCV patients using DAAs managed with onsite care have shown similar outcomes to clinical trials.28,29 Our successfully treated real-world patient cohort has demonstrated comparable virological outcomes (SVR) for telehealth-managed HCV patients using DAAs compared with onsite management in clinical trials. It is notable that the cure rate was the same for patients who had treatment commenced at an onsite visit and those who had treatment commenced via telehealth. The comparison with clinical trials offers a reference point to results that can be achieved under ideal conditions. The comparison with clinical trials has also been used in other HCV studies of real-world care29–31 although direct statistical comparison may not be considered appropriate and has not been performed in this study. 32
This telehealth cohort included those with cirrhosis, those with previous treatment failure, and a small number with HIV co-infection. Patients were treated as per Australian guidelines.4,5 The results presented suggest that efforts to improve access to DAA therapy using telehealth can be achieved without compromising quality patient outcomes.
Telehealth also had significant logistical and financial benefits for patients by reducing their travel burden. Telehealth has additional benefits for clinicians in either reducing the amount of travel that is necessary or increasing the number of patients who can be managed at onsite visits if they are partially managed using telehealth (as was the case in this study). In this study, patient travel savings were calculated using the home address postcode and the location of the tertiary hospital. It is appreciated that the patients may have incurred a small travel cost in going to their local doctor for the telehealth appointment, although most commonly patients lived in the same postcode as their GP. Many professional medical groups now support the use of telehealth for clinical care delivery.33,34
An additional potential advantage of telehealth is direct involvement of local staff at the time of specialist consultation. This offers the opportunity to directly communicate treatment plans but also to implement locally directed management of comorbidities such as alcohol use and obesity that are problematic for liver health. Although local medical staff were not present during all telehealth appointments they were readily contactable when required.
The low rate of technical complications reflects that this is an established telehealth programme. Earlier studies had demonstrated a higher rate of technical complications in the initial phase of this telehealth programme. 11 This suggests that after an initial period of programme development, a telehealth programme using internet-based videoconferencing platforms can operate reliably with few technical complications.
This study had limited participant numbers and was based at one health service, therefore results may not be generalisable to other centres. The use of telehealth is dependent on patients having access to the internet, either at home or at their local health service. All patients who utilised telehealth through our health service were included in the study and all patients from regional areas were offered telehealth consultation, although it is possible that the referring clinicians chose only a subset of their HCV population for referral to a programme that included telehealth.
The World Health Organization (WHO) has identified the health impacts of climate and environmental change as one of the leading priorities for global action. 35 The use of telehealth has the potential to significantly reduce the carbon footprint associated with the provision of healthcare. 36 It has been estimated that the carbon footprint associated with a telehealth consultation is between 40–70 times less than that of an onsite consultation with greater benefit for longer distances. 36 This reduction in carbon footprint has a potential societal benefit that extends beyond the individual patient.
The use of telehealth to improve access to specialist care offers one way of improving outcomes for regional patients with HCV. This is already occurring in other parts of Australia. 15 This complements other recent changes to HCV care including improved support for GP prescribing and the development of nurse-led models of care.4,5
Conclusion
Providing HCV management via telehealth to patients in regional areas is feasible and effective and should be considered for broader use in other regional areas as one way to improve access to HCV treatment and cure.
Footnotes
Acknowledgements
Victorian Government, Department of Health, Refugee Health Programme and Christalla Hajisava for her editorial support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.