
Abstract
Introduction
Patients with multiple sclerosis (pwMS) face barriers accessing specialty care for evaluation and treatment. Telemedicine, the practice of clinical care at a distance with the aid of technology, may be a potential bridge to close the access gap for pwMS separated by distance or disability. The objective of this review was to investigate the types of telemedicine being utilized and overall outcomes for pwMS and their providers.
Methods
A Boolean search of the medical literature was conducted between January 2000 and January 31, 2018. PubMed, EMBASE, PsycINFO and the Cochrane databases, were used to identify all relevant citations. Two reviewers independently appraised the articles for meeting study criteria and for study quality using the CASP system. Financial costs of the telemedicine applications were assessed.
Results
A total of 28 studies involving 3252 participants met criteria for inclusion. Telemedicine interventions were classified, and outcomes were assessed systematically by the following categories: general MS care; rehabilitation and exercise; and neuropsychology/mental health. Studies showed a range of outcomes with variable quality. Overall, remote clinical examinations, long-term telemedicine management interventions and telerehabilitation were shown to be beneficial, cost-effective and satisfactory for patients and providers.
Discussion
Telemedicine is a viable platform for delivering specialty MS care. Remote neurological assessments and several forms of therapy have been shown to be technically feasible. Optimal implementation and barriers to the use of telemedicine in the current healthcare system should be explored.
Introduction
Multiple sclerosis (MS) is the most common progressive neurologic disease of young adults affecting over two million persons worldwide. 1 MS can produce a variety of neurological deficits, making it difficult for patients to access specialty care. 2 The management of MS has become more complex as more disease-modifying treatments and specialty care interventions have become available, requiring the need for neurology, medical specialists (e.g. rehabilitation, mental health) and primary care providers to coordinate care. 3 Despite improvements in therapy, at least 31% of patients with MS (pwMS) do not have access to specialty care. 2 With the advent of the high-speed internet, inexpensive cameras and monitoring software, telemedicine has shown promise in bridging the gap between providers and their patients who have limited access to MS specialty care.4–6
Telemedicine is defined as the use of technology to provide access to clinical care when distance separates patients and providers.5,6 There are several types of telemedicine relevant for MS care. First, clinical video telemedicine (CVT) uses internet-based videoconferencing allowing providers and patients to communicate in real-time. CVT technology can be used for patient consultations requiring an examination at a remote medical facility or the home. Store-and-forward telemedicine (SFT) is the use of technologies to asynchronously acquire and store information, typically by a trained technologist, to be forwarded for later evaluation by a specialist. Home telemedicine (HT) utilizes mobile monitoring, messaging and video technologies to coordinate neurological care, synchronously or asynchronously in the home environment. 6
Telemedicine within neurology (teleneurology) is growing as an approach for evaluating patients with stroke, Parkinson’s disease, MS and epilepsy.4–6 Telemedicine has been used as a platform for rehabilitation, 7 neurological examinations, 8 neuropsychology 9 and other specialty services. 10
But telemedicine services also present with their own unique hurdles. First, reimbursement policies for telemedicine are variable in the USA, with many states not covering services. In other cases, such as with Medicare and Medicaid, reimbursement is allowed for a selected group of telemedicine assessments. 11 Second, the cost of equipment and the limited geographic reach of high-speed internet is an obstacle to accessing telemedicine for patients in several regions of the USA. 12 Finally, if a provider is not licensed in the state where the patient is living, many states restrict telemedicine service delivery. 13
Though there have been some general assessments14,15 and targeted reviews of telemedicine applications7,16,17 in MS care, there has not been a comprehensive review of the telemedicine literature related to MS. Our aim was to perform a literature review on the use of telemedicine for MS specialty care. We examined the broad use of telemedicine in the peer reviewed literature, its effectiveness, general cost for implementation and the quality of evidence.
Methods
A comprehensive literature review was conducted using several online databases including: PubMed, PubMed Central, PsycINFO, EMBASE and the Cochrane Library from 1 January 2000 to 31 January 2018. When searching the databases, a Boolean search was conducted using the same principles and terms between searches. All searches contained a variant of the following search terms: ‘Multiple Sclerosis AND (Telemedicine OR Telehealth OR Telerehabilitation OR Teleneurology).’ When available, ‘Multiple Sclerosis’ was set as to be required in the title when searched. The use of more specific search terms for telehealth (such as ‘video’, ‘store-forward’, ‘home-based’, ‘synchronous’) alone or with the search terms noted above did not increase the number of relevant articles returned.
A manual search of bibliographies of relevant studies and literature reviews was also conducted. All citations for this review were required to be indexed in the peer-reviewed literature. This project was approved by the Washington, DC VA Medical Center Institutional Review Board.
Study selection and data extraction
From the web-based search, we identified and triaged manuscripts based on the following criteria. Inclusion criteria: peer-reviewed, full-text and English language manuscript. Exclusion criteria: single case studies, paediatric studies, poster and symposium abstracts and non-peer reviewed publications. Publications were examined by both SY and MW for their title and abstract to ensure they met criteria for inclusion. Articles meeting criteria were retrieved, summarized and coded in an online database. We used the Critical Appraisal Skills Program (CASP) system, to independently assess study validity, methodological quality, presentation of results, bias and external validity. 18 The CASP system allowed us to produce a numerical value and a total sum for the appraisal of each study. Each article was evaluated independently by SY and MW using the CASP system. Discrepant scores between the two reviewers was resolved by discussion until a consensus was reached. Screening queries were resolved by consensus.
We also provided an assessment of the annual general cost for a pwMS to implement the telemedicine system based on the following: low cost (< US$ 900/year (approximately the average yearly internet cost or cost for cellular phone service), moderate cost (US$ 900–US$ 2500 for annual cost or one-time purchase), and high cost (>US$ 2500 for annual cost or one-time purchase). These estimates were used to put added equipment costs in perspective as many telemedicine interventions were simply internet-based. We used recent average USA costs of equipment and services to estimate costs for the telemedicine (see Supplemental material).
Results
We identified 1116 peer-reviewed articles in our combined search of databases, which was narrowed to 601 unique articles once duplicates were removed from the different search engines (Figure 1). A total of 97 articles met the criteria for the study. Of these, 73 articles were excluded as they did not meet study selection criteria. Three additional studies were included from cross referencing other sources. After triage was complete, 28 studies involving 3252 participants remained (Figure 1). These final articles were divided based on telemedicine topic: general clinical MS care; rehabilitation and exercise; and neuropsychology and mental health (Table 1). Key findings are displayed in Table 2. Study quality as measured by the CASP system was variable (Table 2). Major statistical outcomes and conclusions of the telemedicine studies are reviewed in Table 3. Because of heterogeneity of the study methodology, a meta-analysis was unable to be performed. Of the 28 articles reviewed, 22 involved the use of a HT platform, five utilized CVT only, and one utilized both CVT and SFT. The HT studies were assessed to be of low (n = 14) or medium (n = 8) cost with an average CASP score of 6.3/11. Of the six studies that utilized CVT, implementation was found to be either low (n = 4) or medium (n = 2) cost with an average CASP score of 9.4/11. The one study which highlighting SFT (in addition to CVT) was identified as being low cost with a CASP score of 9/10.
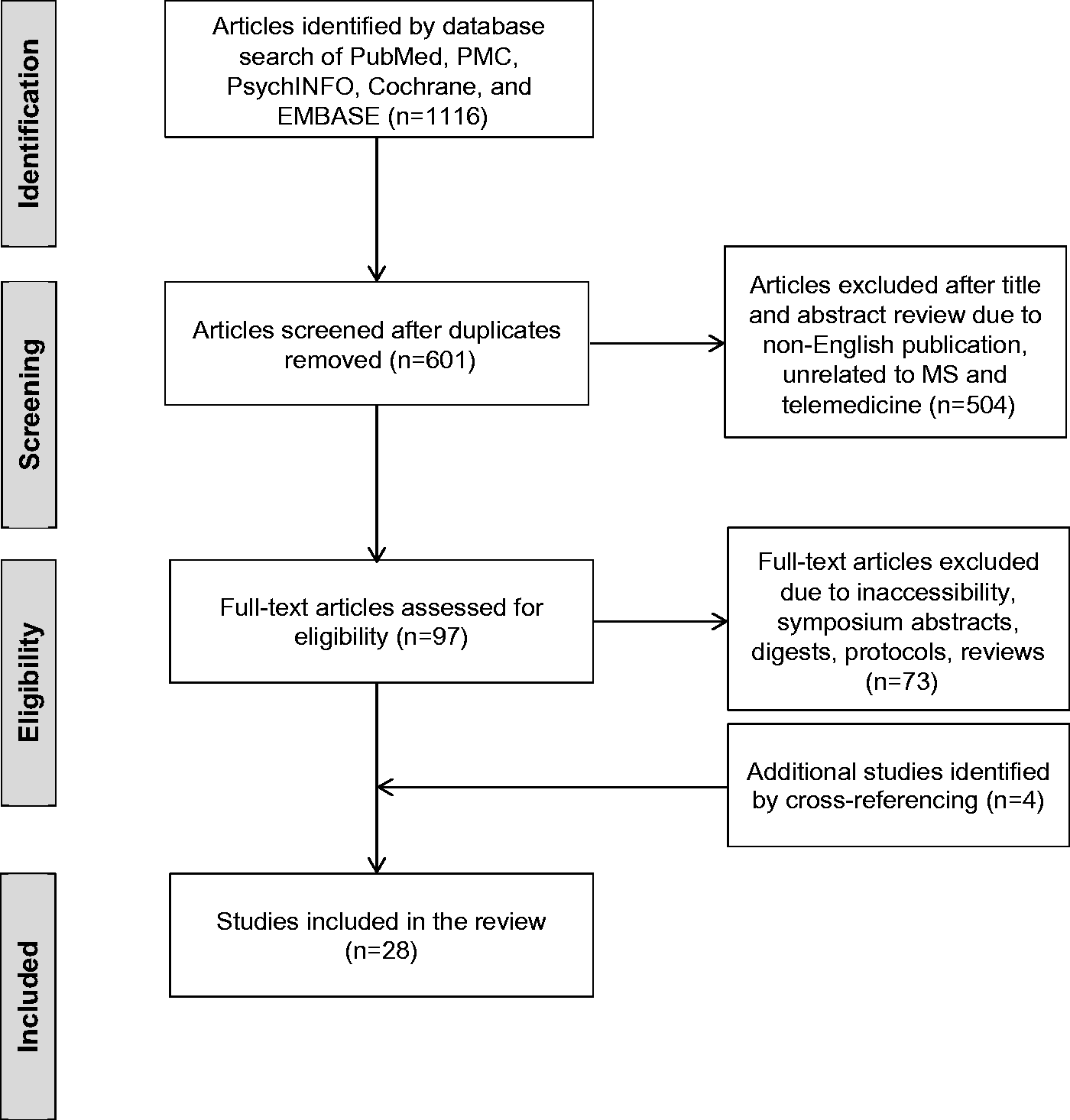
PRISMA flow diagram showing selection of article review.
Summary table of peer-reviewed articles on MS telemedicine.
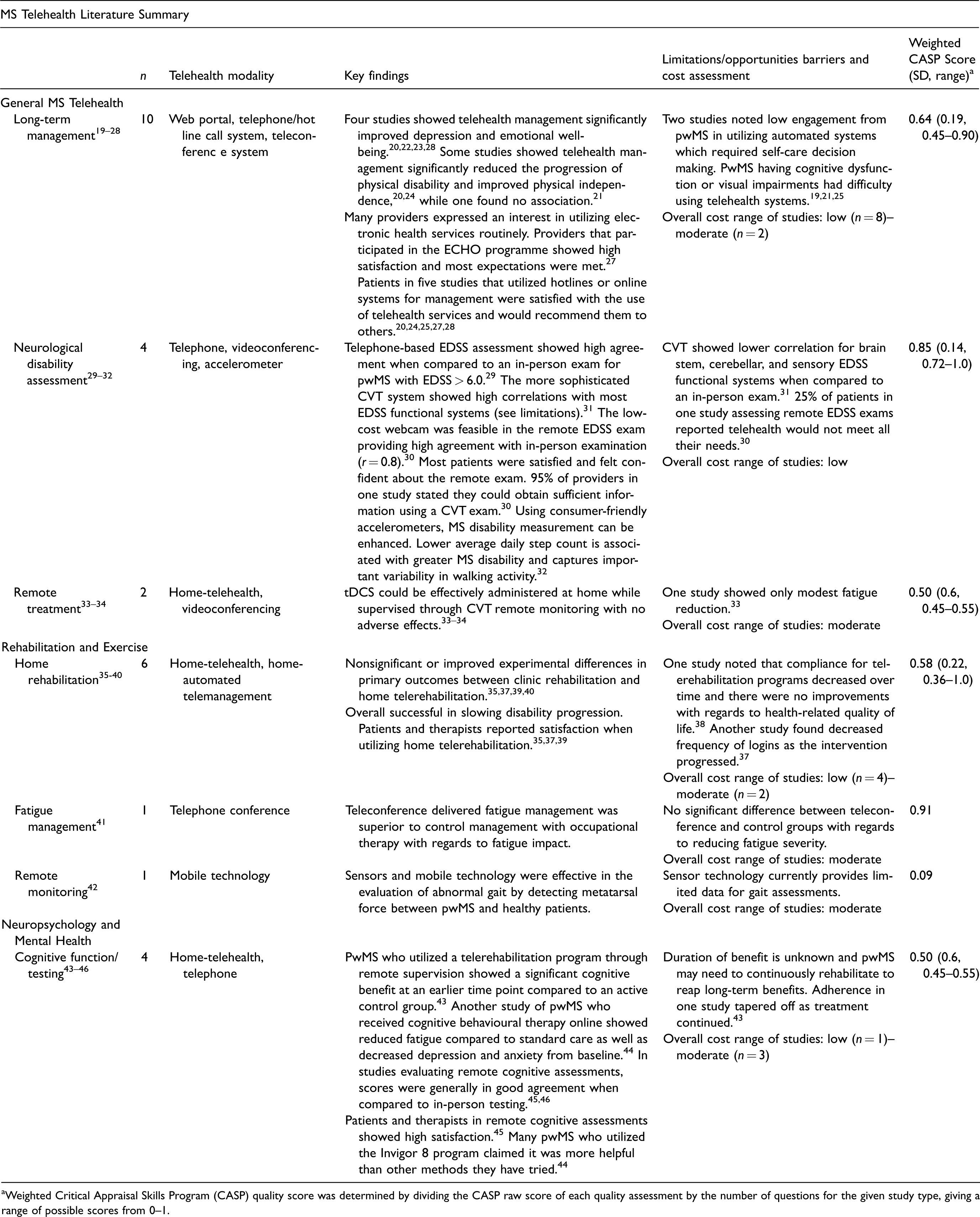
aWeighted Critical Appraisal Skills Program (CASP) quality score was determined by dividing the CASP raw score of each quality assessment by the number of questions for the given study type, giving a range of possible scores from 0–1.
Key findings in MS telemedicine studies. (a) Home telemedicine; (b) clinical video telemedicine. Costs were estimated by using the average monthly values for internet and phone when they were utilized. The costs of other hardware, such as a webcam or gaming system, were estimated by comparing the prices via an online search. Some studies also explicitly stated costs, in which case this value was used for our cost assessment.
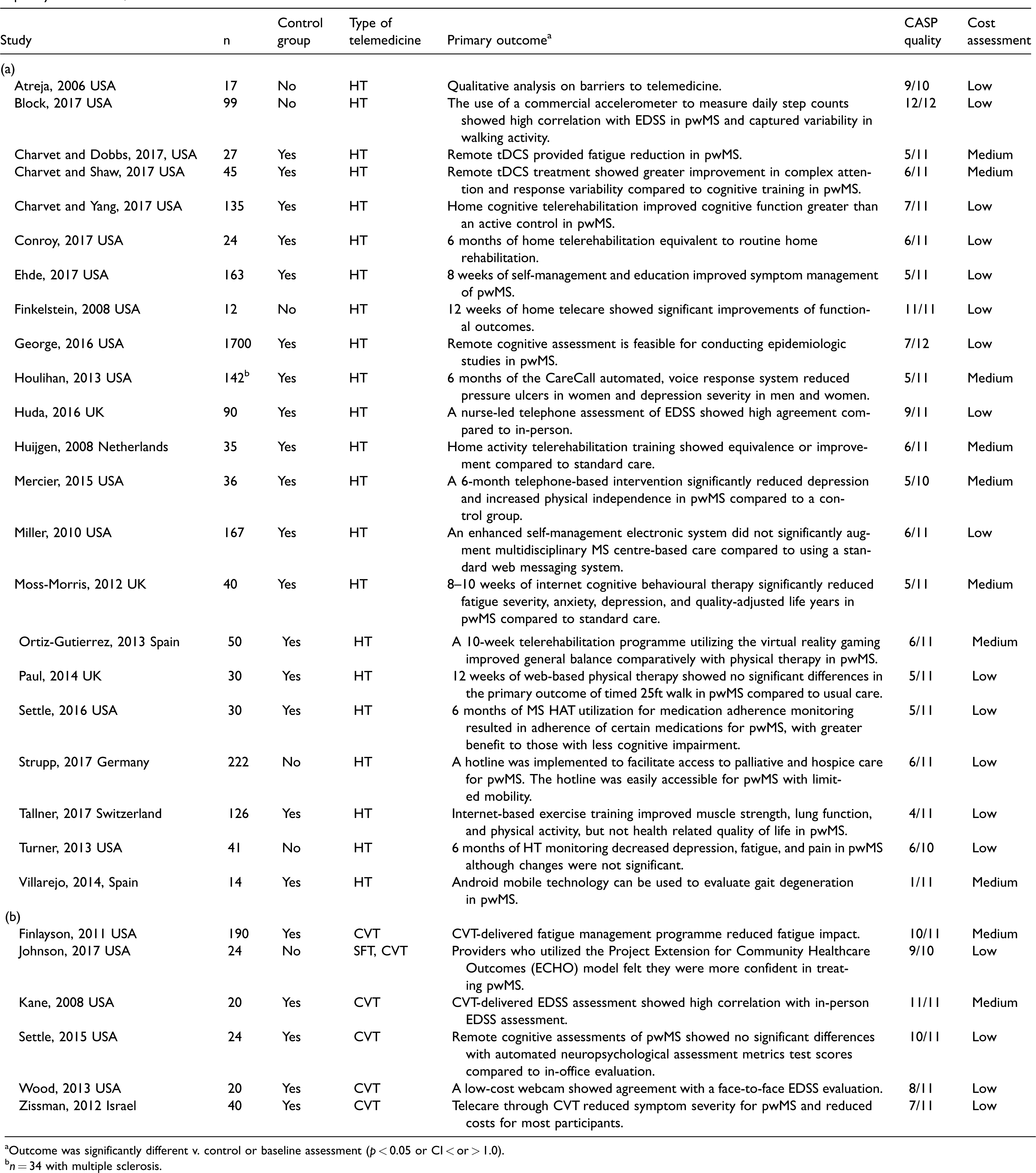
aOutcome was significantly different v. control or baseline assessment (p < 0.05 or CI < or > 1.0).
bn = 34 with multiple sclerosis.
Quantitative and qualitative MS telemedicine studies, statistical outcomes and conclusions of the telemedicine studies.
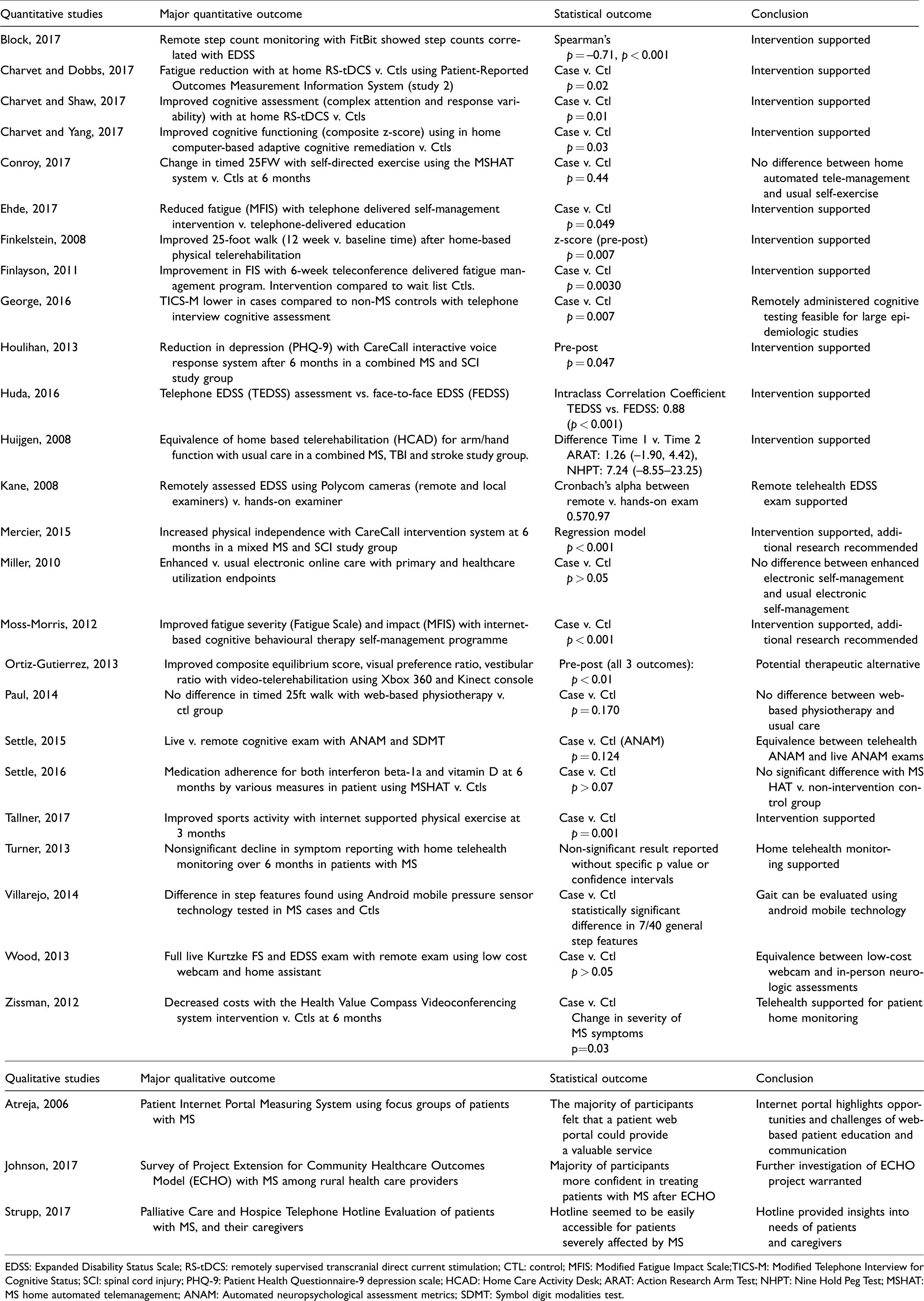
EDSS: Expanded Disability Status Scale; RS-tDCS: remotely supervised transcranial direct current stimulation; CTL: control; MFIS: Modified Fatigue Impact Scale;TICS-M: Modified Telephone Interview for Cognitive Status; SCI: spinal cord injury; PHQ-9: Patient Health Questionnaire-9 depression scale; HCAD: Home Care Activity Desk; ARAT: Action Research Arm Test; NHPT: Nine Hold Peg Test; MSHAT: MS home automated telemanagement; ANAM: Automated neuropsychological assessment metrics; SDMT: Symbol digit modalities test.
General multiple sclerosis telemedicine
One of the most common applications assessed was the use of telemedicine in the longitudinal management of pwMS.19–28 Web-based systems and telephone hotlines were shown to provide patient access to their providers during non-clinic hours from the convenience of their home.19–25 Patients could utilize these systems to review results, order prescriptions and learn new concepts about MS. Studies which compared the telemedicine management of pwMS with traditional in-person management were mixed. Some telemedicine studies showed a significant reduction in pressure ulcers 23 and depression.20,23 Telerehabilitation significantly improved physical independence in two studies20,24 while showed no significant differences in another study. 21 Patients with cognitive 25 and visual 19 impairments had challenges using telemedicine systems. Through telemedicine self-management and education platforms, pwMS were able to reduce the impact of MS symptoms.26,27 Finally, healthcare provider education and case consultation was useful in extending MS care into rural regions of the Pacific Northwest. 28
Four studies found telemedicine utilization to be effective for remote neurological disability assessments of pwMS.29–32 Telephone- (Interclass correlation = 0.8829) Clinic CVT- (α = 0.97–0.9630) and Home CVT-based (p > 0.05)31 Expanded Disability Status Scale (EDSS) assessments showed high correlation and no significant differences compared to in-person examinations, particularly those with higher disability (EDSS > 6.0). Certain aspects of the remote examination, however, showed lower correlations with the live assessment including the brain stem (α = 0.79–72), 30 cerebellar (α = 0.57–0.56)30 and sensory (α = 0.74–0.72)30,31 functional systems (FS). A study by Block et al. found that step counts measured by a Fitbit™ accelerometer correlated with greater disability on the EDSS (p < 0.001) and showed important variability in walking activity within individual EDSS categories. 32
With regards to therapy delivered by telemedicine, two studies from the same group evaluated remote transcranial direct current stimulation (tDCS) for the treatment of fatigue and cognitive dysfunction.33,34 Using the Patient-Reported Outcomes Measurement Information System-Fatigue Short Form, the study team showed a statistically significant, but modest reduction of fatigue with tDCS treatment compared to sham sessions (p = 0.02). 33 Remote tDCS combined with cognitive training produced greater improvements in complex attention (p = 0.01) and response variability (p = 0.01) when compared to cognitive training alone. 34 The authors noted remote tDCS provided a low-cost alternative to patients when compared to other stimulation methods.
Rehabilitation and exercise telemedicine
Home-based telerehabilitation for pwMS was evaluated in six studies.35–40 The Multiple Sclerosis Home Automated Telemanagement system (MS HAT) was the platform used in two telerehabilitation studies in pwMS.35,36 MS HAT is an internet-based patient and provider module designed for the self-management of pwMS. 35 In a pre-post design pilot study using this platform, there was significant improvement in the timed 25-foot walk (p = 0.007) and the 6 minute walk (p = 0.02). 36 However, a larger randomized trial conducted by Conroy et al. showed no significant difference in the timed 25-foot-walk (primary outcome) compared to a control group at six months. Participant engagement over the course of this larger study was reported to be challenging. 35
Another randomized, controlled study conducted by Paul et al. examined the effectiveness of 12 weeks of web-based physical therapy compared to usual care in pwMS. 37 There was no significant difference in the primary outcome, the timed 25-foot walk (p = 0.170), between the intervention and control group. Participants in the intervention who had less experience using the internet needed support using the web-based therapy, and login rates decreased throughout the programme.
A randomized, controlled telerehabilitation study conducted by Tallner et al. noted significant improvements in muscle strength (p = 0.003–0.015) and sports activity (0.001). 38 Compliance for home-telerehabilitation, however, decreased over time in the intervention and control groups and no improvements were appreciated in health-related quality of life after six months.
Home-based telerehabilitation interventions were shown to be similar or more beneficial than usual rehabilitation care in pwMS.39,40 Finlayson et al. examined fatigue management using a telephone conference intervention with a two-group time series design and wait list controls.41 This tele-occupational therapy programme was more effective than the control group for reducing fatigue impact but not fatigue severity. Changes in fatigue were maintained for six months with moderate effect sizes. 41
A gait evaluation study used smartphone sensors placed inside the shoe to record gait abnormalities in pwMS and controls. 42 This technology was sufficient to effectively evaluate gait degeneration by monitoring step features such as metatarsal force between pwMS and healthy participants. The results indicated significant differences in gait in 7 of 40 general step features for pwMS. This preliminary data provided evidence that simple remote monitoring could be used to evaluate gait degeneration, but more work is required in larger samples.
Neuropsychology and mental health telemedicine
Four studies investigated the use of telemedicine in evaluating cognitive function for pwMS.43–46 In a randomized, double blind, controlled trial of a home-based CVT telerehabilitation in pwMS, there was a significantly greater improvement in the primary outcome of cognitive functioning in the telemedicine group compared to the routine care control group (mean change in composite z-scores: 0.25 v. 0.09, p = 0.03). 43 Another study found that internet-based cognitive therapy was associated with improvements in fatigue severity and impact (p < 0.001), anxiety (p < 0.001) depression (p < 0.001) and quality adjusted life when compared to only receiving standard care. 44 The authors noted that adherence to the remote therapy decreased over the 10 weeks of the study.
Finally, two studies assessed the feasibility of remote cognitive evaluations in pwMS.45,46 Settle et al. showed statistical equivalence between pwMS who completed a remote CVT or in-office cognitive assessment using the automated neuropsychological assessment metrics test (p = 0.124). However, there was some variability in the scores for the home-based CVT symbol digit modalities tests (p = 0.018). 45 George et al. found that the Modified Telephone Interview for Cognitive Status, a validated phone assessment for cognitive function in the elderly, distinguished a significant cognitive impairment between pwMS and a control group (mean difference = –0.60, p = 0 .001). It also highlighted that the participation rate for pwMS was high but lower than the control participation (86 v. 93%). 46
Cost
Of the 28 studies meeting our criteria for the study, 18 were found to be low-cost interventions and 10 were considered medium cost for pwMS using our metric (see Table 2 and Supplemental data). Low-cost modalities typically required internet/phone access and hardware such as a webcam for CVT. Telephone hotlines and web-portal systems proved to be cost effective methods of long-term management and remote assessments (disability, cognitive, etc.). Telerehabilitation studies which relied on in-home exercises and did not utilize extra hardware or equipment were low cost as well.35–37
Patient and provider satisfaction
Both patients and providers appeared to be satisfied with the telemedicine for general MS care services.20,24,25,28,30 However, one study noted that there was low engagement from pwMS when utilizing automated systems that required more decision making. 21 Regarding satisfaction with telerehabilitation platforms, participants and therapists felt positively about using telemedicine, particularly regarding convenience of telerehabilitation in the home setting.35,37,39 Many pwMS who utilized the MS Invigor8 programme stated it was more helpful than other methods they have used. 44 Therapists, providers and pwMS who participated in remote cognitive assessment studies also reported high satisfaction. 45
Discussion
Our review provides support for the benefits of telemedicine as a method of MS care delivery. We highlight the success of many studies as well as the limitations and often preliminary nature of telemedicine interventions to date. We found that studies showed a range of quality based on the CASP system. Interventions were largely low cost for patients with a handful of studies in the medium cost range. Overall, long-term telemedicine management interventions, telerehabilitation, and remote clinical examinations were shown to be beneficial, cost-effective and satisfactory for patients and providers.
The potential impact of telemedicine on access to mental health and neuropsychology services should be highlighted. The general improvement of emotional well-being and decreased severity of depression was shown in several studies.20,22,23,28 Remote-cognitive behavioural therapy was particularly helpful in allowing access to a specialized therapy to pwMS while reducing the time needed to participate in face-to-face traditional cognitive behavioural therapy.43,44 These studies illustrate that telemedicine can be a useful means to access mental health and neuropsychological care.
Most randomized controlled studies examined either showed no significant difference between a telemedicine intervention versus non-telemedicine,21,25,31,35,39,45 or telemedicine interventions to be beneficial with regards to outcomes for pwMS.20,24,33,34,40,41,43,44 This, along with the findings that patients and providers seemed to be satisfied with the level of care delivered through telemedicine indicates the large potential for widespread implementation of telemedicine services. This conclusion correlates with the findings of a provider survey conducted by Kern et al. showing that electronic health services were highly appreciated by neurologists when managing pwMS. 47
We found that there are, however, still hurdles that come about with telemedicine. One of the most consistent drawbacks noted was a lack of compliance and low engagement from pwMS when utilizing telemedicine for extended periods of time. Certain aspects of the software and hardware may also pose challenges for these patients with neurological deficits. Moreover, there may be limits to what can be accomplished in a home setting as shown by Atreja et al., Mercier et al. and Settle et al.19,20,25
Previous reviews covering telemedicine in pwMS have focused on telerehabilitation. A 2015 review conducted by Amatya et al. concluded that there was low-level evidence for the effectiveness of telerehabilitation in improving functionality, short term symptoms and long-term symptoms in pwMS but insufficient evidence as to what types of telemedicine are effective. 7 The authors also claimed that the evaluated studies score were assessed to be of low methodological quality. Tallner et al. also evaluated telerehabilitation use in pwMS, specifically web-based interventions, and found high patient acceptance and satisfaction with the programmes, although decreasing compliance was a major issue. 48 A more recent review by Block et al. also concluded that internet-based interventions were beneficial in promoting objectively reported physical activity along with attenuating disability in pwMS. 17
Approximately two thirds of the studies investigated were considered to be low cost. These typically involved studies which exclusively utilized a web or telephone system, without the need for sophisticated equipment. Having access to these low-cost treatment options could be especially beneficial for pwMS who are home-bound due to disability or are separated geographically from MS specialty clinics.
The implementation of telemedicine is also restricted by limited or no insurance reimbursement. Many states do not cover telemedicine services while others have mandated parity pay laws which reimburse a telemedicine visit similarly to an in-person one. 49 State licensing also introduces roadblocks for healthcare providers as they must also be licensed in the state where telemedicine services are delivered to patients, impacting patients in geographic regions where multiple states overlap (e.g. New England). 13
Strengths and limitations
Strengths of this review include the systematic process for searching the literature combined with independent review from two authors to minimize bias and ensure only relevant articles were included. The evidence quality and cost assessments were also assessed independently to reduce potential bias.
Limitations include our exclusion criteria for studies. We did not review case reports, meeting abstracts and Non-English studies which limited the number of articles reviewed. Our review likely had a reference bias as we only focused on peer-reviewed studies and may have overlooked negative or non-significant reports. Other telemedicine modalities presented in isolated reports or negative studies were missed.
Conclusion
This review provides evidence that supports telemedicine as a platform for affordable access to clinical care for pwMS. This is especially true for remote clinical examinations, longitudinal management and telerehabilitation. The telemedicine studies reviewed were relatively small and further research is needed with larger sample sizes and more methodological consistency across studies. There is also limited data on the rate and pattern of utilization of telemedicine by pwMS.
Optimizing telemedicine services will require more discussion with, patients, providers, insurance companies and policy makers. Further investigation into these issues can aid in the implementation of effective telemedicine strategies that will benefit pwMS, their families and providers.
Supplemental Material
Supplemental material for Telemedicine and Multiple Sclerosis: A Comprehensive Literature Review
Supplemental Material for Telemedicine and Multiple Sclerosis: A Comprehensive Literature Review by Samuel Yeroushalmi, Heidi Maloni, Kathleen Costello and Mitchell T. Wallin in Journal of Telemedicine and Telecare
Footnotes
Authors' note
Samuel Yeroushalmi is also affiliated with George Washington University School of Medicine, Washington, DC, USA.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The content is solely the responsibility of the authors and does not necessarily represent the official views of the Department of Veterans Affairs or the US government, or any of the institutions with which the authors are affiliated
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preparation of this manuscript was supported by the National Multiple Sclerosis Society (HC-1610-25978) and the US Department of Veterans Affairs Multiple Sclerosis Center of Excellence.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.