
Abstract
Introduction
There remain a number of UK military veterans who are not able to access psychological therapies for post-traumatic stress disorder (PTSD). Some of these barriers are practical, including the need to balance work and other life commitments with attendance at residential or outpatient appointments. There is a need to investigate more accessible and flexible methods of delivering psychological therapies to veterans. One such alternative is to use remote-access video technology, often referred to as tele-therapy. The aims of the present study were to explore the feasibility of using tele-therapy in this population, whilst also reporting mental health outcomes for those who accessed the intervention.
Methods
Participants were recruited from a UK veterans mental health charity. The intervention consisted of 12 sessions of cognitive processing therapy delivered via Skype. Participants completed various measures of mental health, including PTSD at three time points: pre-treatment, post-treatment and at three months follow-up. A measure of therapeutic alliance was also completed by participants and the clinician.
Results
A total of 27 participants engaged in tele-therapy, with a treatment completion rate of 79% and a ‘did not attend’ rate of 12%, which compared well against similar outpatient services. All mental health outcomes showed maintained improvement at three months follow-up, with the highest effect size recorded for PTSD. Therapeutic alliance was also rated highly by both participants and the clinician.
Discussion
The findings suggest that tele-therapy could provide a viable alternative format for delivering trauma-focused psychological therapies to veterans. Limitations and recommendations for future research are also presented.
Introduction
In the past 20 years, the number of UK veterans seeking help for post-traumatic stress disorder (PTSD) has significantly increased.1 The impact of this is notable, as veterans with PTSD are at increased risk of unemployment and social exclusion2–5 and it has been found that PTSD creates higher costs to society than any other mental health issue in veterans.6 In the UK, there has been an increasing focus on military mental health in recent years, reflecting an increased awareness in the mental health needs of veterans.7
Research of UK veterans suggests that only 30–50% of those who experience mental health problems go on to access services for support,8 although more recent evidence suggests this might be improving.9 Reasons for low help-seeking include issues related to stigma about experiencing mental health problems (e.g. being seen as weak) and practical issues around not being able to access services due to time constraints, commitments such as work and childcare, or not knowing where to access support.10
Given the potential barriers to accessing support, there is a need to investigate more accessible, flexible and cost-effective methods of delivering psychological therapies to veterans. One such alternative is to use remote-access technology (e.g. videoconferencing over the Internet) to deliver psychological talking therapies, often referred to as tele-therapy.
In the UK, mental healthcare provision is provided by statutory, government-funded services via the National Health Service (NHS) and third-sector, charity organisations that specialise in military mental health. Standards of clinical excellence are used to determine appropriate, evidence-based interventions for mental health disorders. Currently, cognitive-behavioural therapies (CBTs) and eye movement desensitisation and reprocessing therapy (EMDR) are recommended as first-line treatments for PTSD in adults.
There is evidence to suggest tele-therapy can be effective in treating military veterans with PTSD,11 and in many cases it is just as effective as face-to-face interventions.12 Tele-therapy has been trialled in US and Canadian veterans using a variety of treatment methods, such as prolonged exposure,13–17 CBT18–21 and cognitive processing therapy (CPT).22–27
Despite this evidence, remote-access interventions are not routinely offered to veterans with PTSD in the UK. The current study is part of a wider project investigating the acceptability and feasibility of tele-therapy with UK veterans, with recently published findings suggesting that it is acceptable to those accessing the treatment.28 The aims of the present study were to explore the feasibility of using tele-therapy in this population, whilst also reporting mental health outcomes for those accessing the intervention. Given the evidence for tele-therapy reported in other countries, and the fact that an evidence-based intervention was selected for the purposes of the study (see intervention and materials), it was expected that reported PTSD symptoms would reduce following the intervention. However, given the lack of evidence in the UK for tele-therapy, the study was designed primarily as a pilot to assess the feasibility of the intervention, whilst also reporting on mental health outcomes.
Methods
Setting
The study was conducted at Combat Stress (CS), a national charity and provider of veteran mental healthcare in the UK. The research team responsible for the study are embedded within the CS treatment centre from where clinical services operate. Veterans can be referred to CS via their local general practitioner (GP) or by self-referral. CS offers residential, inpatient treatment programmes using evidence-based interventions such as CBT.29 At first contact, veterans undergo an initial community assessment and, where indicated, a psychiatric assessment. Following this process, veterans are offered treatment in accordance with their needs.
Participants
Members of the CS clinical team referred participants to the research team if they were considered to be eligible for the study. The research clinician then contacted participants to complete a screening interview. CS have clinical teams based throughout the UK and, as such, the study was open to participants from anywhere in the country.
Inclusion criteria were veteran status (defined as having served a minimum of one day in the UK Armed Forces); and having difficulties with PTSD. Some participants were referred via psychiatrists at CS and had an existing PTSD diagnosis. Others were referred to the study prior to a psychiatric assessment and did not have a formal diagnosis. For the purposes of the study, PTSD symptoms were measured by a self-report questionnaire which was used to determine PTSD severity. Participants were not excluded if they had co-morbid mental health difficulties, and measures of depression and anxiety were included in the battery of outcome measures, so that co-morbidities could also be assessed. Those deemed to be high-risk in terms of suicidality were not eligible due to concerns about remote risk management. This was assessed during the initial telephone screening. Access to the Internet was essential as all appointments were conducted online, as well as access to a private space from which participants could complete therapy sessions.
The aim was to offer tele-therapy to a minimum of 24 participants in total. This sample size was based on a power calculation of the number of participants required to detect a meaningful reduction of scores on the PTSD Checklist for DSM-5 (PCL-5) measure (see outcome measures) between the start and end of therapy, at 90% power and 5% significance level with a standard deviation of 15. These figures are based upon previous research within this population.29
Outcome measures
Health outcomes
PCL-5: the PCL-530 is a 20-item self-report questionnaire which measures symptoms of PTSD. Items are rated on a five-point Likert scale, with participants indicating the level to which they have been affected by given problems. Example items include ‘Avoiding memories, thoughts or feelings related to the stressful experience’ and ‘Feeling jumpy or easily startled’.
Patient Health Questionnaire (PHQ-9): the PHQ-931 is a nine-item self-report questionnaire which measures symptoms of depression. Items are rated on a four-point Likert scale, with participants rating the extent to which they have been affected in the past two weeks. Example items include ‘Having little interest or pleasure in doing things’ and ‘Feeling tired or having little energy’.
Generalised Anxiety Disorder (GAD-7): the GAD-732 is a seven-item self-report questionnaire which measures symptoms of generalised anxiety. Items are rated on a four-point Likert scale, with participants rating the extent to which they have been affected in the past two weeks. Items include ‘Feeling nervous, anxious or on edge’ and ‘Worrying too much about different things’.
Dimensions of Anger Reactions (DAR-5): the DAR-533 is a five-item self-report questionnaire used as a measure of anger in relation to trauma. Items are rated on a five-point Likert scale. Items include statements such as ‘I often find myself getting angry at people or situations’ and ‘When I get angry, I stay angry’.
Alcohol Use Disorders Identification Test (AUDIT): the AUDIT34 is a 10-item self-report measure used as a screening tool for harmful alcohol consumption. Items are rated on a five-point Likert scale, with participants reporting on their alcohol use over the past six weeks. Items include ‘How often do you have six or more drinks on one occasion?’ and ‘How often in the last year have you had a feeling of guilt or remorse after drinking?’.
Acceptability
Scale to Assess Therapeutic Relationships in Community Mental Health Care (STAR): the STAR35 is a 12-item self-report measure of therapeutic relationships. The measure has two versions, one completed by the participant (STAR-P) and the other by the clinician (STAR-C). Items are rated on a five-point Likert scale, with a maximum score of 48. Items include statements such as ‘My clinician and I shared an honest relationship’ and ‘We agreed what was important for me to work on’. Both versions of the STAR give an overall rating of the therapeutic relationship, as well as each having subscales of Positive Collaboration (both STAR-P and STAR-C), Positive Clinician Input (both STAR-P and STAR-C), Non-Supportive Clinician Input (STAR-P only) and Emotional Difficulties (STAR-C only). Total and subscale mean scores are provided in a validation sample.35
Feasibility
Feasibility was assessed by measuring attendance and dropout rates; the number of ‘did not attend’ appointments (DNAs); the amount of time spent per client by the clinician; and the average number of weeks it took for participants to complete the 12-session course of therapy.
Demographic information
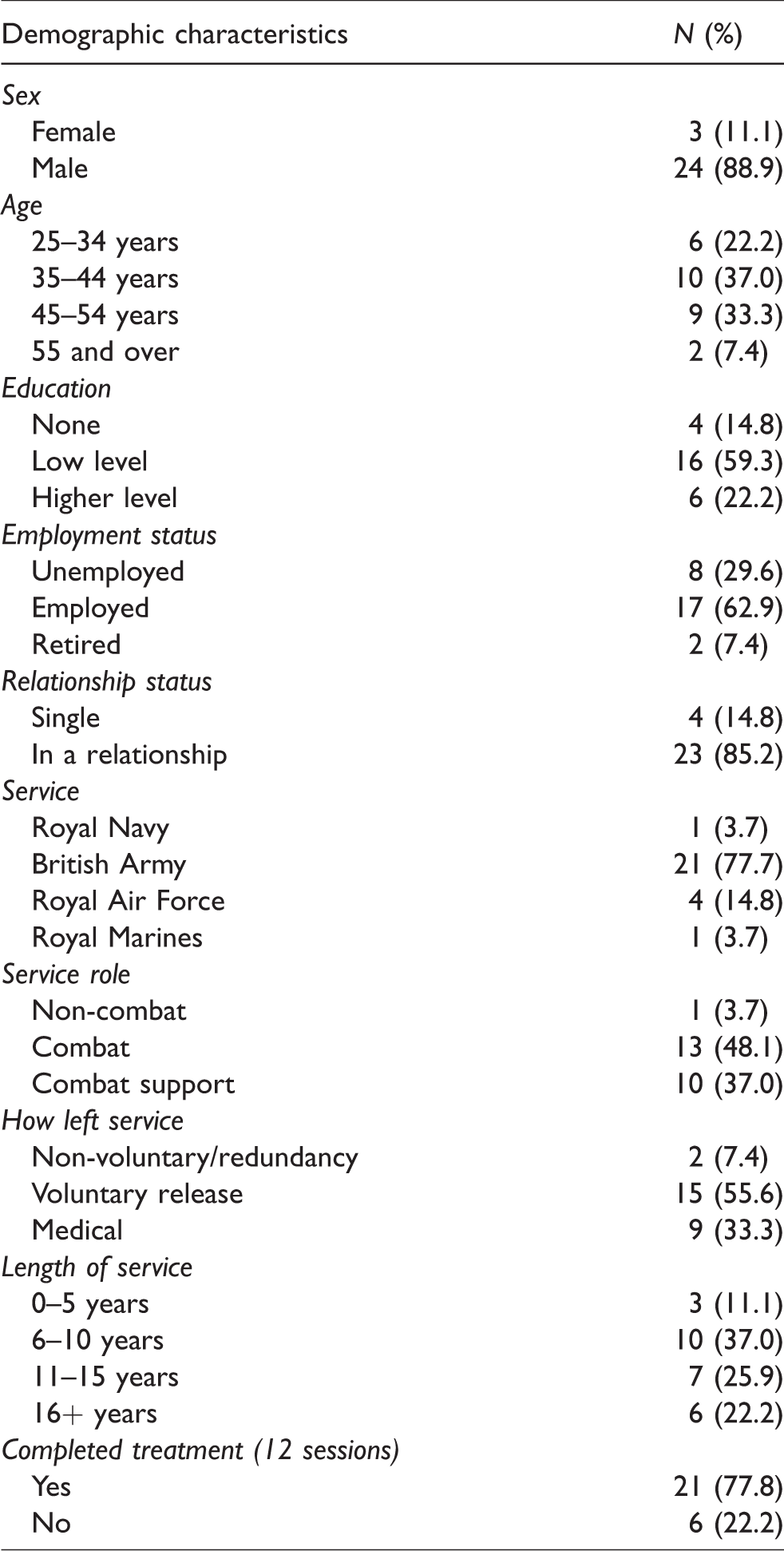
In addition, several demographic characteristics were recorded at baseline (Table 1). These included, sex, age, education, employment status, relationship status, the Armed Forces service in which they served, service role, circumstances in which they left the service and the length of service.
Demographic data.
Intervention and materials
CPT was chosen as it has an established evidence base and because it has been adapted for use with veterans and standardised into a 12-session programme,36 ensuring the participants in the current study received a consistent treatment. The CPT manual also includes information and worksheets corresponding to each treatment session. A single research clinician (second author) was used to deliver the CPT intervention to each participant. The clinician was a qualified Clinical Psychologist (DClinPsy) and had undergone further training in CPT for the purposes of the study.
Procedure
Once referred to the study, participants were contacted by the research clinician by telephone to gauge their interest in taking part and to complete a screening assessment, which included suitability for psychological therapy; hopes and goals for treatment; screening for current risk and suicidality; assessing readiness to engage in therapy; and exploring any potential barriers to engagement such as having time available for appointments and access to appropriate technology. All CPT sessions were conducted via Skype, an encrypted, free to use and readily available software application for videoconferencing. Sessions were conducted from clinic rooms at CS treatment centres to ensure confidentiality. The clinician used Skype for Business to conduct appointments, with a webcam attachment.
Participants were also asked about their confidence and previous experience in using Skype and were advised about how to use it if they had not done so before. Tablets were available to send to participants who did not have access to a device with which to use Skype. Tablets were programmed by the CS IT department, which included setting appropriate security settings and pre-loading Skype. An instruction sheet about how to use Skype was sent to participants where required. Participants were asked to complete the outcome measures at three time points: before therapy, immediately after therapy and at a three-month follow-up point. Measures were either sent in the post or via email depending on each participant’s preference. Post-treatment measures also included a measure of therapeutic alliance, which was completed by the participant and clinician. Following completion of CPT, participants completed a clinical review with the research clinician a month later to assess their current mental health. At this stage they were either discharged from CS or referred for further treatment if required.
Ethical approval was granted by the CS research ethics committee. Formal consent was taken from each participant during the telephone screening, as described previously.
Data analysis
Responses from mental health outcome measures were entered and analysed using SPSS. Firstly, descriptive statistics were used to explore the sample in terms of demographics. Following this, regression models were fitted to explore differences in primary and secondary mental health outcomes at pre-therapy, post-therapy and at follow-up, with effect sizes then calculated.
Results
Participants and recruitment
In total, 54 referrals were made to the tele-therapy service between January and August 2017. Attempts were made to contact all participants who were referred, although it was not possible to establish contact with four of these. Fifty veterans completed an initial telephone assessment, with 11 opting out at this stage. Reasons for opting out included having a lack of social support and, therefore, concerns about managing strong emotions evoked in therapy, preferring face-to-face therapy and not being able to commit to therapy at the time. A further 12 veterans who had initially expressed an interest then subsequently opted out before starting therapy. Overall, of the 54 referrals made, 27 started tele-therapy.
Most of the participants were male and between the ages of 35 and 54. There was a range of education levels in the sample, but most had lower levels of education, such as GCSE (General Certificate of Secondary Education) or equivalent. The majority of participants were in work (n = 17). Of those who were not in work, in most cases this was due to health reasons. Most participants were in a relationship.
Participants predominantly presented with combat-related traumas. A small number of participants had an index trauma relating to combat support, such as being involved in medical emergencies. Most participants reported more than one trauma, but in keeping with the CPT protocol, attention was focused on the index trauma, as defined by the participant.
Chi-square analyses were conducted to assess whether certain demographic variables made participants more or less likely to complete treatment. Results showed that none of age (X2 (4, N = 27) = 2.41, p > .05), education (X2 (4, N = 26) = 2.93, p > .05), employment (X2 (4, N = 27) = 3.31, p > .05) or relationship status (X2 (4, N = 27) = 5.91, p > .05) were related to treatment completion.
The vast majority of participants completed sessions in a private room at home, although some scheduled appointments during work – for example, in their lunch break. Three participants required evening appointments, which was accommodated. The clinician completed sessions in a clinical room at CS. Because of the importance of having an appropriate environment for sessions was discussed with participants beforehand, there were no occasions where appointments had to be rescheduled due to a participant not being in a suitable location.
Feasibility outcomes
Of the 27 participants who started therapy, six terminated the therapy before completing all 12 sessions. Two participants were sent tablets to use for therapy sessions as they did not have suitable equipment at home. In total, 255 tele-therapy sessions were completed, with a DNA rate of 12%. On average, it took 14 weeks for a participant to complete 12 sessions of therapy (the range for time to complete therapy being from 6 to 24 weeks). The CPT manual advises that, where possible, clinicians should aim to hold two sessions per week with a client, meaning therapy can be completed in six weeks, but findings here suggest that this was not possible in most cases.
Mental health outcomes
Of the 21 participants who completed the therapy, 20 completed post-therapy outcomes measures, and 18 completed measures at three-months’ follow-up. There were no significant differences in PTSD scores between those who did and did not complete post-therapy and follow-up measures.
Table 2 shows mental health outcome scores pre-therapy, post-therapy and at three months’ follow-up. The data suggest that there is overall improvement in mental health scores following tele-therapy, an effect which is maintained at three months. The effect size for PTSD score reduction between pre-therapy and three-month follow-up was large.
Comparison of mental health outcomes before and after tele-therapy.
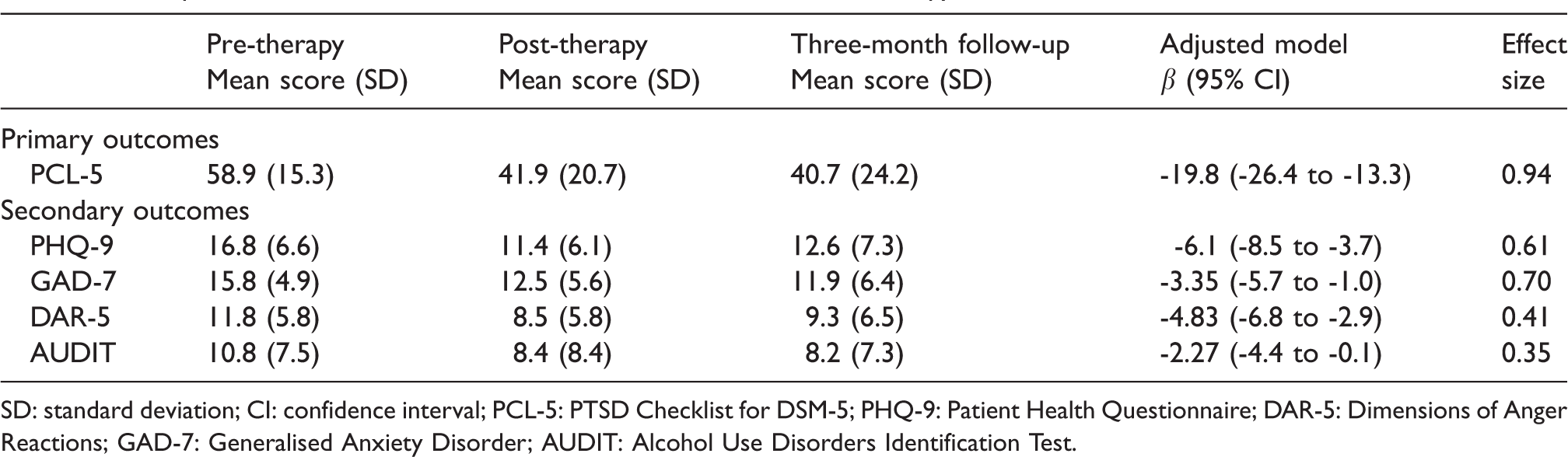
SD: standard deviation; CI: confidence interval; PCL-5: PTSD Checklist for DSM-5; PHQ-9: Patient Health Questionnaire; DAR-5: Dimensions of Anger Reactions; GAD-7: Generalised Anxiety Disorder; AUDIT: Alcohol Use Disorders Identification Test.
Out of a total score of 48, the mean score on the participant version of the STAR measure of therapeutic alliance was 44.8 (n = 19 participants). For the clinician’s version, the mean score was 45.9 (n = 21 participants).
Discussion
The aims of this study were to investigate the feasibility of offering trauma-focused psychological therapy to UK veterans with PTSD. The main findings were that tele-therapy appeared to be a feasible alternative in terms of participant engagement. Using a structured 12-session programme of CPT, 27 veterans started the therapy with 21 completing it in total. Six participants (22%) dropped out of treatment and, overall, there was a 12% DNA rate. The results also showed that PTSD and other mental health outcomes had significantly reduced at three-month follow-up, albeit from a sample of limited size.
The DNA rate of 12% compared favourably with previous research, which has shown that an outpatient mental health service for UK veterans reported a DNA rate of around 19%.37 The same study reported a dropout rate of just over 21%. In the current study, six participants dropped out of tele-therapy, at a rate of 22%. This suggests that the use of tele-therapy did not negatively impact on rates of engagement.
This paper reports on findings from a wider study looking at the feasibility and acceptability of using tele-therapy with a sample of UK veterans with PTSD. The approach has been found to be acceptable to veterans,28 and the current findings support existing literature reporting the effectiveness of using CPT via tele-therapy in improving PTSD.24,27
In terms of therapeutic alliance, there are few studies from which a direct comparison can be made of overall STAR scores. However, one study found mean participant-rated scores of 37.2 in a mental health crisis service, and 28.3 in an acute mental health ward,38 which would suggest that the tele-therapy format allowed for good levels of therapeutic alliance. In this study, participants commented on the flexibility that tele-therapy afforded them in terms of where and when they accessed appointments. In some cases, participants were able to engage in therapy where it had not previously been possible because of work, family commitments or the inability to travel to outpatient appointments.
Strengths and limitations
The modest sample size within this study makes it hard to draw confident conclusions about its effectiveness in terms of treatment efficacy. Going forward, if tele-therapy were to be used more widely, outcomes and feedback should continue to be collected so that stronger conclusions can be drawn about its effectiveness.
The study benefited from the fact that the sample used was representative of the wider veteran population who are accessing support from CS. Other than active suicidality, there were no further restrictions on eligibility criteria, meaning that the findings were based on a sample of veterans that were a fair reflection of the population typically seen at CS. The use of Skype as the means of delivering the tele-therapy increased the accessibility of the treatment as this service is freely available.
CPT seemed an appropriate choice of intervention because it has an emerging evidence base in veteran mental health (albeit not in the UK). CPT is also time-limited, which was useful given the relatively short period of time (12 months) in which this pilot study was undertaken. Using this manualised approach should also have improved treatment fidelity, although this was not formally assessed. It also meant that participants received an intervention that was standardised as much as possible. However, some participants may have benefited from a more flexible, person-centred and formulation-based approach. In terms of the sample, this was self-selecting, so those participants who opted to take part may have been more pre-disposed to engage in tele-therapy.
Another limitation regards the fact that only self-report outcome measures were used to ascertain mental health symptoms. The study would have benefited from more robust diagnostic measures, such as clinical interviews, in order to have more confidence in the presence of and reduction in mental health symptoms prior to and following the intervention. Whilst this was a pilot study, clearly a more experimental approach would have been preferable, such as the use of a comparison group. The study would also have benefited from a comparison with a group who completed CPT in person. This intervention is not routinely offered at CS, but any future research could utilise this approach.
Recommendations for future research
This paper refers to a pilot tele-therapy service, which was set up to meet the needs of a sub-group of UK veterans who required more flexible provision of services, due to reasons such as work and childcare commitments and travel difficulties. Tele-therapy offers one alternative therapy format to improve the accessibility of treatments. There is a clear need to for larger-scale, controlled studies to verify the effectiveness outcomes from this study. Furthermore, alternative treatments should be investigated to discover which treatment models are best suited to the tele-therapy format. Further research is needed to investigate factors related to treatment adherence and mental health outcomes to explore whether there are types of cases where tele-therapy is most effective.
Conclusion
The findings from this study suggested tele-therapy for UK veterans with PTSD are a feasible alternative to face-to-face interventions. Significant improvements were seen in mental health outcomes following the intervention, although the relatively small sample size prevents any firm conclusions about the effectiveness of tele-therapy in this study. Larger-scale and controlled studies are needed to add further evidence regarding their effectiveness.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Forces in Mind Trust (grant number FiMT15/1204CSTele).