
Abstract
Introduction
Innovative eHealth solutions that improve access to child weight management interventions are crucial to address the rising prevalence of childhood obesity globally. The study aimed to evaluate the feasibility and preliminary efficacy of a 12-week online telehealth nutrition intervention to improve child weight and dietary outcomes, and the impact of additional text messages (SMS) targeted to mothers and fathers.
Methods
Families with children aged 4 to 11 were randomised across three groups: Telehealth, Telehealth+SMS, or Waitlist control. Telehealth and Telehealth+SMS groups received two telehealth consultations delivered by a dietitian, 12 weeks access to a nutrition website and a private Facebook group. The Telehealth+SMS group received additional SMS. Feasibility was assessed through recruitment, retention, and intervention utilisation. Efficacy was assessed through changes in measured child body mass index (BMI), waist circumference and diet.
Results
Forty-four (96%) and 36 (78%) families attended initial and second telehealth consultations, respectively. Thirty-six families (78%) completed week 12 assessments. Child BMI and waist circumference changes from baseline to week 12 were not statistically different within or between groups. Children in Telehealth+SMS had significantly reduced percentage energy from energy-dense nutrient-poor food (95% CI −21.99 to −0.03%E; p = .038) and increased percentage energy from healthy core food (95% CI −0.21 to 21.89%E; p = .045) compared to Waitlist control.
Discussion
A family-focused online telehealth nutrition intervention is feasible. While the modest sample size reduced power to detect between-group changes in weight status, some improvements in child dietary intakes were identified in those receiving telehealth and SMS.
Introduction
Childhood obesity has been recognised as a global health problem. The World Health Organization Commission on Ending Childhood Obesity 2016 report highlighted that progress in combating childhood obesity has been slow and inconsistent worldwide. 1 The report indicated that more effort is required to address childhood obesity and contained six recommended strategies including the ‘provision of family-based, multicomponent, lifestyle weight management services for children and young people’ with obesity. 1 Existing reviews also suggested that family-focused behavioural lifestyle interventions with direct parental involvement lead to improved indicators of child weight status (e.g. body mass index (BMI), percentage overweight).2–5 A review of systematic reviews recommend that family-focused intervention strategies should include both parents (i.e. mothers and fathers) as the agents of change, foster positive parenting skills, and provide parental resources to encourage lifestyle changes within the home. 6 Despite the development of evidence-based strategies for family-focused childhood obesity treatment, personalised child weight management services for families of children with overweight or obesity remain scarce within Australian public health services.7–9 The current lack of public health services for managing childhood obesity in relation to the scale of the issue means that capacity to address the extent of childhood obesity across the geographically diverse Australian population is inadequate. 8
A worldwide increase in access to the Internet and smart devices has facilitated research into the use of web-based electronic health (eHealth) interventions that include family-focused healthy lifestyle programmes.10,11 In the US and UK, approximately 90% of adults use the Internet and 91% of millennials own a smartphone. 12 In Australia, more than 97% of households with children under the age of 15 have access to the Internet via computer, smartphone or tablet. 13 Australian data shows that technology use is increasing and is not limited by socioeconomic status (SES) or geographic location. 13 This is important for intervention development in families of low SES where children are more likely to be affected by overweight or obesity. 14 The use of an eHealth intervention has the potential to overcome traditional barriers to participation offers flexibility for busy families to engage in treatment, improves access, extends the reach of nutrition services to rural regions and reduces costs, travel time and leaves of absence from work/school that are often associated with attendance at face-to-face clinical appointments. 15
The application of eHealth in childhood obesity interventions is an emerging area of practice. 10 A review of eHealth interventions for childhood obesity identified only five studies that involved children aged 5 to 10 years and the remaining 13 studies involved adolescents aged 12 to 18 years, with intervention strategies including text messages (SMS), websites and smartphone apps. 16 Telehealth intervention (defined by the International Organisation for Standardisation as the ‘use of telecommunication techniques for the purpose of providing telemedicine, medical education, and health education over a distance’) 17 for childhood obesity is scarce. 18 A review of telehealth use in childhood obesity treatment found only four studies (one pilot trial, three observational studies), all published since 2008. 18 The pilot trial comprised a group-based telehealth intervention delivered by a psychologist to parents in a school setting, while the children participated in an activity-based group intervention. 19 There remains a knowledge gap, in terms of feasibility, concerning an online childhood obesity intervention with a family-based telehealth connection using household electronic devices. Therefore, the current study aimed to investigate the feasibility and preliminary efficacy of a novel 12-week family-focused online telehealth nutrition intervention in improving child weight status and dietary intake. The secondary aim was to investigate whether additional evidence-based SMS messages targeted to mothers and fathers enhanced the intervention.
Methods
Study design
The study was a pilot randomised controlled trial (RCT) with participants randomised to three study arms: i) Telehealth, ii) Telehealth+SMS, iii) Waitlist control. Both intervention groups (Telehealth, Telehealth+SMS) received intervention access immediately following randomisation after completing baseline assessments. Telehealth+SMS received additional SMS plus all intervention components of the Telehealth group. The Control group received no intervention for 3 months and was given access to all intervention components (the same as Telehealth+SMS) after the week-12 assessments. The study adhered to the checklist adapted from the Consolidated Standard of Reporting Trials (CONSORT) guidelines for pilot and/or feasibility studies. 20 The overall study design is illustrated in a CONSORT Diagram (Figure 1).
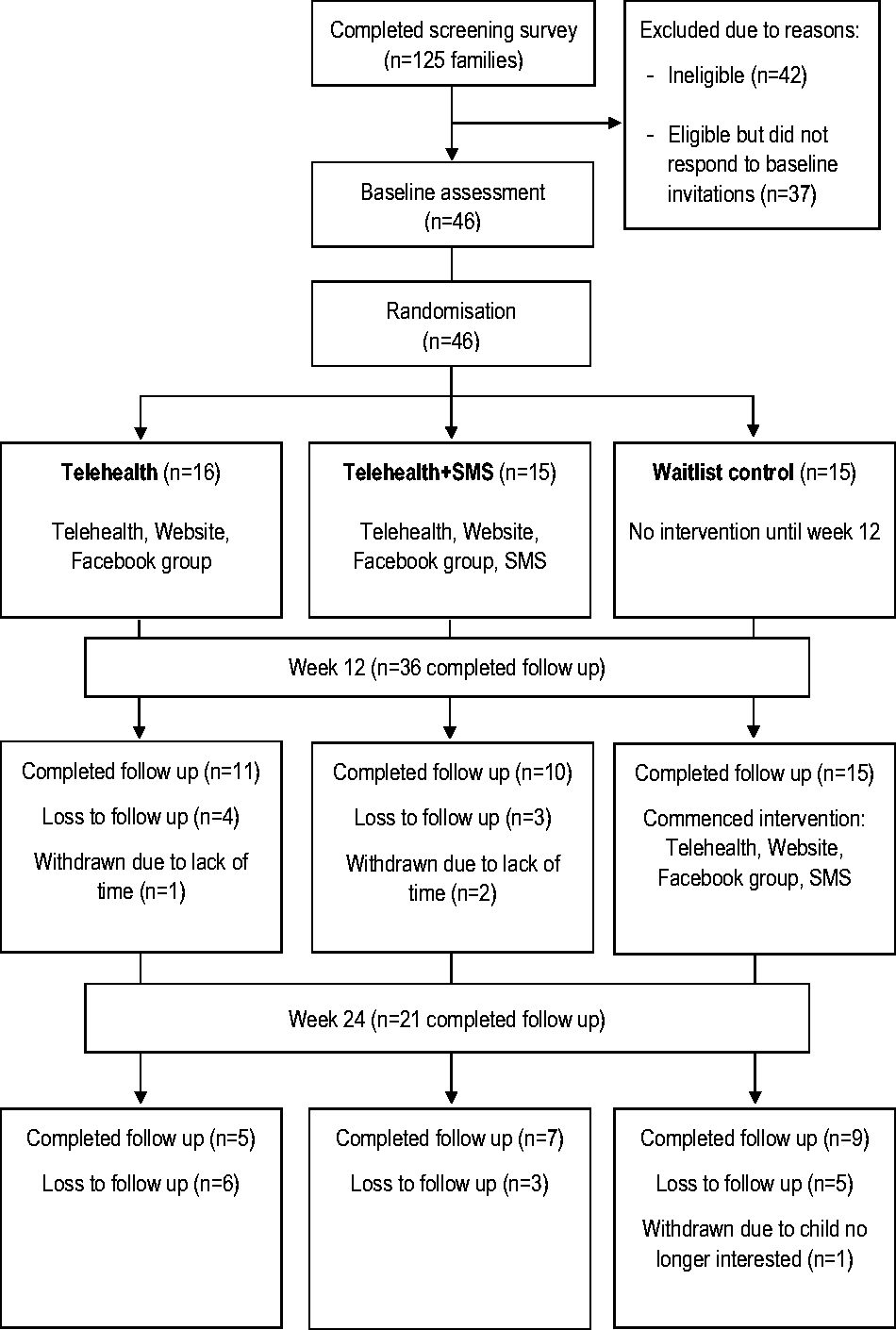
CONSORT 2010 flow diagram.
The study was approved by the Hunter New England Local Health Districts Human Research Ethics Committee (16/07/20/4.04) and University of Newcastle Human Research Ethics Committee (H-2016-0329).
Recruitment and participants
Participants were children aged 4 to 11 years with BMI ≥21.5 kg/m2 (International Obesity Task Force children cut-offs) 21 and their parent/s who consented to attend assessments at one of the three study sites in New South Wales, Australia, and to access the online intervention using their own electronic devices. The eligible child BMI was kept broad for recruitment, as previous studies showed that parents of children with overweight or obesity often fail to recognise their child’s weight status as being overweight 22 and tend to under-report their child’s weight, especially in the case of children with overweight or obesity.23,24 Therefore, the eligible child BMI was set to be above the mid-point of the healthy weight category (≥21.5 kg/m2) in order to be inclusive in recruiting children with overweight or obesity.
Families were recruited to one metropolitan (i.e. Newcastle) and two rural sites (i.e. Tamworth, Armidale) between July 2017 and May 2018. Extensive recruitment strategies were used to distribute study information (including a direct link to the online screening survey) through networks surrounding the Hunter New England region: John Hunter Children’s Hospital dietetics clinic (a regional tertiary weight management service; only one of three centres in New South Wales offering such service), health professional networks (including flyers mailed out to 136 general practitioners), 92 primary schools, family-friendly community venues (e.g. libraries, gyms, cafes), contemporary media (television news, newspaper and radio), and social media networks targeted to the Newcastle, Tamworth and Armidale regions.
Families were excluded if the index child was participating in another weight management intervention during the study period; had a secondary cause for obesity or significant learning difficulties; required medication (except insulin) that influences growth, weight or appetite; or required a therapeutic (i.e. texture modified) diet. Parental written consent and child assent were obtained prior to baseline data collection. To reduce the waiting time for families who enrolled early, families commenced the programme in six different cohorts at various time frames ranging from July 2017 to April 2018 and attended their respective data collection sessions for each time point. Families received AU$10 gift vouchers at each data collection session (total $30 for three sessions) to subsidise travel costs.
Sample size and randomisation
Existing research recommends a sample size of at least 12 per group for pilot studies when there is no prior information on which to base samples on. 25 A researcher not involved in data collection and analysis generated computer-based block randomisation sequences and prepared concealed envelopes, which were revealed following baseline assessments by a researcher not involved in data collection. Researchers performing lab measurements were blinded to the participant’s group. Dietitians delivering interventions were blinded to the intervention groups (i.e. Telehealth or Telehealth+SMS) but not to the Control group.
Back2Basics Family intervention
Telehealth dietitian consultation
Semi-structured telehealth consultations (approximately 20 min each) were delivered in weeks 1 and 4 by an accredited practising dietitian (APD) using Hunter New England Local Health District’s clinical telehealth online videoconferencing software (Scopia) 26 during scheduled clinic appointments. Families received instructions to download and install Scopia through a website link. 26 Families initiated telehealth connections from their device during the consultation where at least one parent and the index child were present, while other family members were also welcome to participate. Telehealth consultations were guided by the CALO-RE taxonomy of behaviour-change techniques related to healthy eating (Table 1). 27 Discussion topics included Australian Dietary Guideline (ADG) recommendations for children, 28 the Australia Eating Survey (AES) dietary report (for further details see ‘Outcome measures’), family goal settings (e.g. first goal focused on increasing servings of nutrient-rich core food; second goal focused on reducing energy-dense, nutrient-poor (EDNP) food or excessive EDNP portion sizes) aligned with the ADG28 and previous effective interventions,29,30 and rewards. The AES dietary report and behavioural goals discussed were emailed to parents following the initial consultation. The second consultation, in week 4, addressed progress towards goals and to problem-solving in relation to barriers to change.
Back2Basics Family telehealth consultations guided by CALO-RE taxonomy of behaviour change techniques.
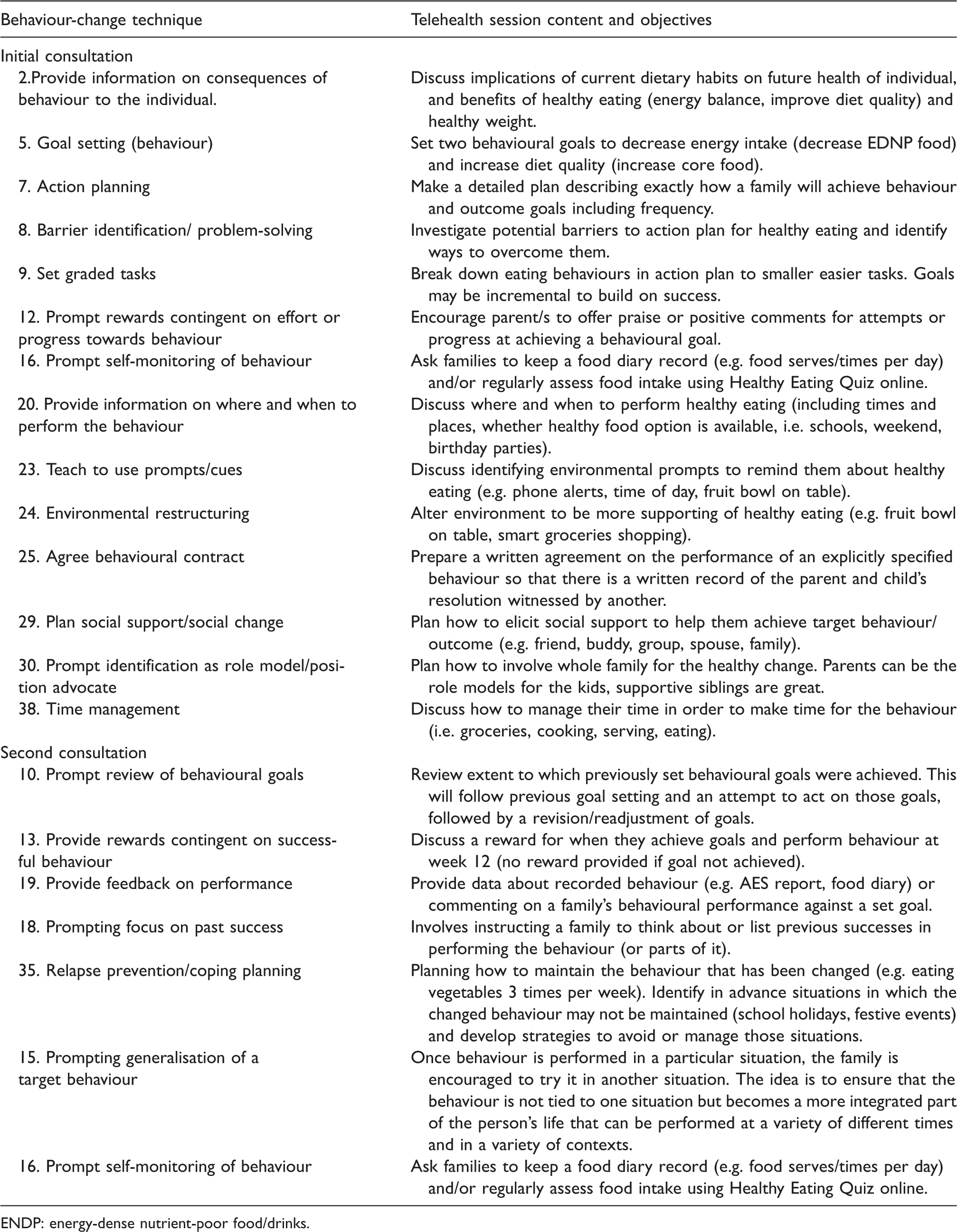
ENDP: energy-dense nutrient-poor food/drinks.
Website
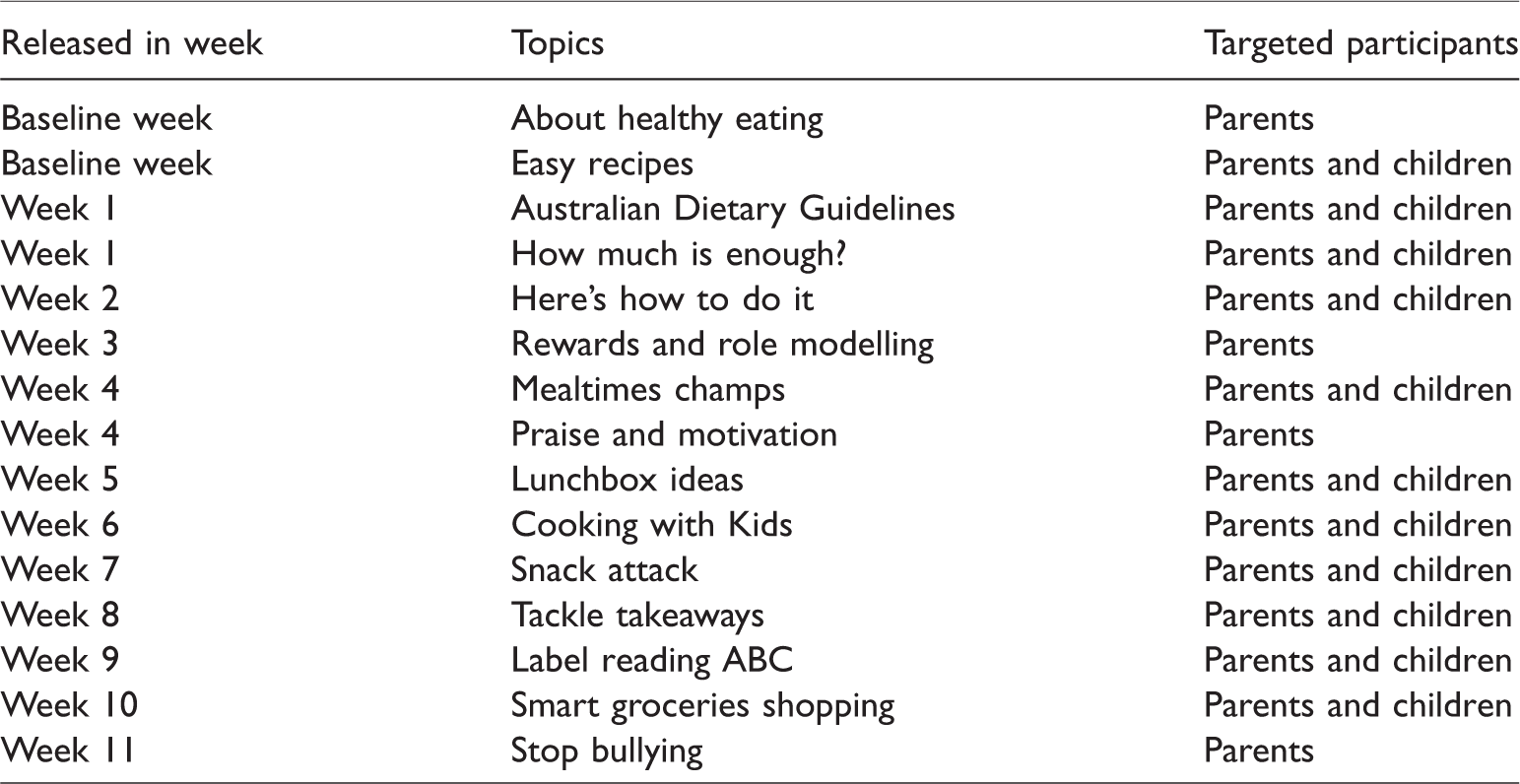
The Back2Basics Family (B2BF) website contained information on various nutrition topics (Table 2) adapted from the efficacious HIKCUPS child obesity treatment programme,30,31 purpose-built healthy cooking videos 32 previously designed for families with low-level literacy and on a low budget, and additional topics based on a previous survey with 75 parents. 15 Families were free to access the website at their preferred time and frequency. New topics were introduced each week throughout the programme to maintain participants’ engagement, which has been shown to be effective in previous research. 33
Examples of Back2Basics Family website content and schedule.
Facebook group
The B2BF Facebook group was a closed online medium (membership upon invitation only) for parents to exchange ideas and information related to the B2BF website. The Facebook group included weekly announcements posted by the researchers when new topics were released on the B2BF website (Table 2). The Facebook groups for the three study arms were kept separate to reduce cross-group contamination.
Text messages
A series of SMS targeting healthy eating for children was delivered to both parents (e.g. mother and father) of the child in 4-weekly rotations of decreasing frequency 34 (i.e. 5, 4, 3, then 2 messages per week). For sole-parent families, SMS were delivered to the sole parent only, except where another co-parent (e.g. grandparent) regularly shared childcare. In total, 42 SMS were delivered over the 12-week intervention to each consenting parent. The SMS were grounded in behaviour-change theory and informed by evidence-based child weight management strategies. 35 Details of the SMS development and content validation process has been published elsewhere. 35
Outcome measures
Feasibility
Feasibility was measured through recruitment, retention, and intervention utilisation using process measures documented by researchers, telehealth attendance recorded by dietitians, and demographic and process evaluation surveys completed by parents. Demographic data were collected via baseline surveys and included parents’ and child’s age, sex and BMI; parents’ education level; postcode; and family context (i.e. single or both biological/step-parents living with the child). Postcodes were matched to the Modified Monash (MM) Model, which categorises metropolitan, regional, rural and remote areas into seven MM categories for geographic classification36,37; and to the Socio-Economic Indexes for Areas: Index of Relative Socio-Economic Advantage and Disadvantage for Postal Areas ranking, which determines SES (i.e. low, middle and high). 38 Additional data on intervention fidelity and acceptability (participants’ satisfaction) were also collected and have been reported elsewhere. 39
Efficacy
The preliminary efficacy of the interventions was indicated by differences between group changes in measured child BMI, zBMI (BMI z-scores), waist circumference, and dietary intake from baseline to week 12. Child height, weight, and waist circumference were measured by trained research assistants using standard protocols. Height was measured to the nearest 0.1 cm using a Biospace BSM370 Automatic Stadiometer with children barefoot and their head positioned in the Frankfort horizontal plane. 40 Weight was measured to the nearest 0.1 kg without shoes and in light clothing using an InBody 720™ body composition analyser (Newcastle and Tamworth sites) or a SECA 803 electronic weighing scale (Armidale site). Waist circumference was measured around the umbilicus to the nearest 0.1 cm using a KDS Steel Measurement Tape, on bare skin, the children standing with legs shoulder-width apart and arms at resting position. All measures were conducted twice, and a third measure was obtained if the first and second measures were not within 0.3 cm for height, 0.4 kg for weight, or 0.5 cm for waist circumference. Child BMI was calculated and zBMI were computed using Cole’s LMS statistical method. 21
The child version of the online AES semi-quantitative food frequency questionnaire (FFQ) was used to evaluate child dietary intake, with a personalised dietary report generated and used as the basis of the telehealth consultations. The child version of the AES is a 120-item semi-quantitative FFQ that captures parent-reported child dietary intake, 41 and has previously been validated for fruit, 42 vegetables, 42 dietary fats 43 and energy intake 44 in Australian children using plasma carotenoid concentrations or red blood cell membrane fatty acids as biomarkers. An individual response is required for each food item in the AES, with options ranging from ‘never’ to ‘four or more times per day’; and for some beverages up to ‘seven or more glasses per day’. Parents were asked to report the child dietary intake over the past 3 to 6 months as this reporting period is designed to capture usual eating habits. At follow-up visits, parents reported child dietary intake for the previous 3 months. The AES uses child-specific serving sizes and the following nutrient databases: Australian AusNut 1999 database (All Foods) Revision 14, and AusFoods (Brands) Revision 5 (Xyris Software (Australia) Pty Ltd, 2004: Brisbane Australia). 45 A personalised dietary report was generated and sent to the dietitian once a parent completed the online AES. The report includes evaluation of total energy intake (kJ) and the percentage energy (%E) derived from nutrient-rich food groups (core food) compared to EDNP food, and overall diet quality assessed by the Australian Recommended Food Score (ARFS), which has a maximum score of 73, with subgroup scores of 21 for vegetables, 12 for fruits, 13 for meat and alternatives (i.e. legumes, nuts), 13 for grains, 11 for dairy products, 2 for condiments, and 1 for water.46,47
Child physical activity level (PAL) was assessed as a confounding factor, due to its effects on weight changes, using the Physical Activity Questionnaire for Children. 48 The questionnaire is a nine-item, 7-day recall instrument that has been validated, demonstrating high accuracy in estimate energy expenditure with moderate reliability.49,50
Statistical analysis
All data manipulation and statistical analyses were undertaken using STATA, version 12 (Stata Corp LP, College Station, TX, USA) by a researcher not involved in data collection. Results were considered statistically significant where p < .05. Descriptive analysis was used to assess feasibility outcomes: recruitment, retention, and intervention utilisation collected from intervention families at week 12 and control families at week 24 (i.e. at the conclusion of the intervention). Differences between groups at baseline were assessed using analysis of variance. The primary analyses for intervention outcomes were intention-to-treat, defined as using available data from all randomised participants and multiple imputation by chained equations for missing data, and were performed using linear mixed models to examine changes of child anthropometry and dietary intake, expressed as differences in the means and 95% confidence intervals between baseline and week 12. The p-value associated with the interaction effect between group and time was used to determine the statistical significance of any difference between groups over time.
Results
Feasibility
Recruitment
Of the 125 families who completed the screening survey, 83 eligible families were invited to participate in the study, and 46 families (n = 28 Newcastle, n = 18 Tamworth/Armidale) completed baseline assessments and were randomised to one of three study arms: Telehealth group (n = 16), Telehealth+SMS group (n = 15), and Control group (n = 15). The most successful recruitment avenue was through Facebook posts (35%; n = 16), followed by emails to corporate mailing lists (33%; n = 15), school newsletter (15%, n = 7), word of mouth from family or friends (9%; n = 4), general practitioners (4%, n = 2), magazine (2%, n = 1) and flyer from a local café (2%, n = 1). Baseline characteristics between groups were not significantly different (p > .05). Children (mean age 9 ± 2.3 years) were predominantly male (59%), living with both biological parents (65%), and had overweight/obesity (70%). Baseline percentage energy intakes from core food and EDNP food were 62%E and 39%E, respectively. Parents (mean age 41 ± 7.2 years) were predominantly female (96%), of middle SES (65%), living in major cities (61%), and had overweight/obesity (79%), a certificate/diploma (30%) followed by postgraduate degree (26%). Detailed baseline characteristics of children and their parents are presented in Table 3.
Baseline characteristics of children and their parents.
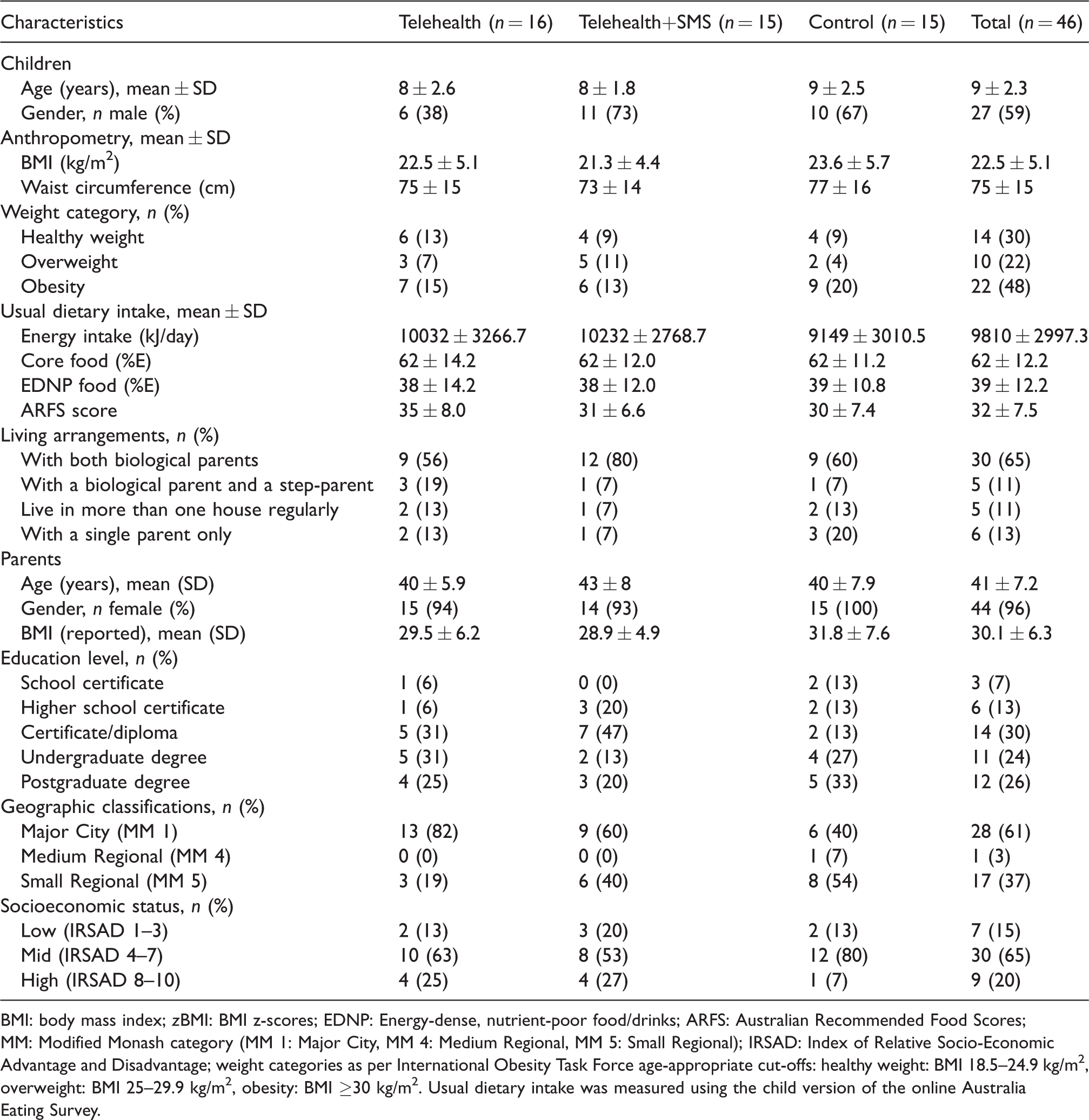
BMI: body mass index; zBMI: BMI z-scores; EDNP: Energy-dense, nutrient-poor food/drinks; ARFS: Australian Recommended Food Scores; MM: Modified Monash category (MM 1: Major City, MM 4: Medium Regional, MM 5: Small Regional); IRSAD: Index of Relative Socio-Economic Advantage and Disadvantage; weight categories as per International Obesity Task Force age-appropriate cut-offs: healthy weight: BMI 18.5–24.9 kg/m2, overweight: BMI 25–29.9 kg/m2, obesity: BMI ≥30 kg/m2. Usual dietary intake was measured using the child version of the online Australia Eating Survey.
Retention
The overall retention rate at week 12 was 78% (n = 36 families). Three intervention families, reported as having a lack of time, withdrew within the first month of participation, and seven intervention families were lost to follow-up (defined as not responding after three reminders about assessments) at week 12. All control families (n = 15) completed week 12 assessments, however, one family withdrew as the child was no longer interested, and nine (60%) completed process evaluation survey at week 24. The baseline characteristics of children (e.g. age, sex, BMI, energy intake, proportion of healthy food groups compared to less healthy foods) and parents (e.g. age, sex, BMI) who were and were not followed up at week 12 and week 24 were not significantly different.
Intervention utilisation
Telehealth consultation attendance showed that 96% (n = 44 of 46 families: Telehealth n = 16, Telehealth+SMS n = 14, Control n = 14) attended the initial consultation and 78% (n = 36 of 46 families: Telehealth n = 12, Telehealth+SMS n = 12, Control n = 12) attended the second consultation. Additional SMS were delivered to 29 families (sole parent n = 4, co-parents n = 25) who received the SMS intervention component (Telehealth+SMS n = 15, Control n = 14). The SMS intervention engaged 14 out of 25 fathers (56%) who were co-parents. Further intervention utilisation data were reported by 30 parents (n = 21 intervention families at week 12 and n = 9 control families at week 24) who completed the process evaluation survey. Utilisation of other web-based intervention components were reported by the majority of families and included logging into the B2BF website at least once (77%; n = 23), visiting the B2BF Facebook group at least once (80%; n = 24), and 100% received the SMS (
Efficacy
Child outcomes at week 12 are summarised in Table 4. Overall, child BMI, zBMI, waist circumference and PAL changes were not significantly different within groups or between groups. Interaction effects between group and time demonstrated that the total daily energy intake was significantly reduced in the Telehealth compared to Control group (−2835 kJ; p = .026), but not statistically significantly different to the Telehealth+SMS (−2291kJ; p = .078). Child dietary intake improved in both intervention groups, with changes statistically significant for the Telehealth+SMS, in terms of reduced percentage energy from EDNP food (−11%E; p = .038) and increased percentage energy from nutrient-rich core food (+11%E; p = .045) compared to the controls, who demonstrated the reverse trend (i.e. increased total energy intake, increased percentage energy from EDNP food and decreased percentage energy from core food).
Intention-to-treat analysis of changes in child outcomes at week 12 (n = 46).
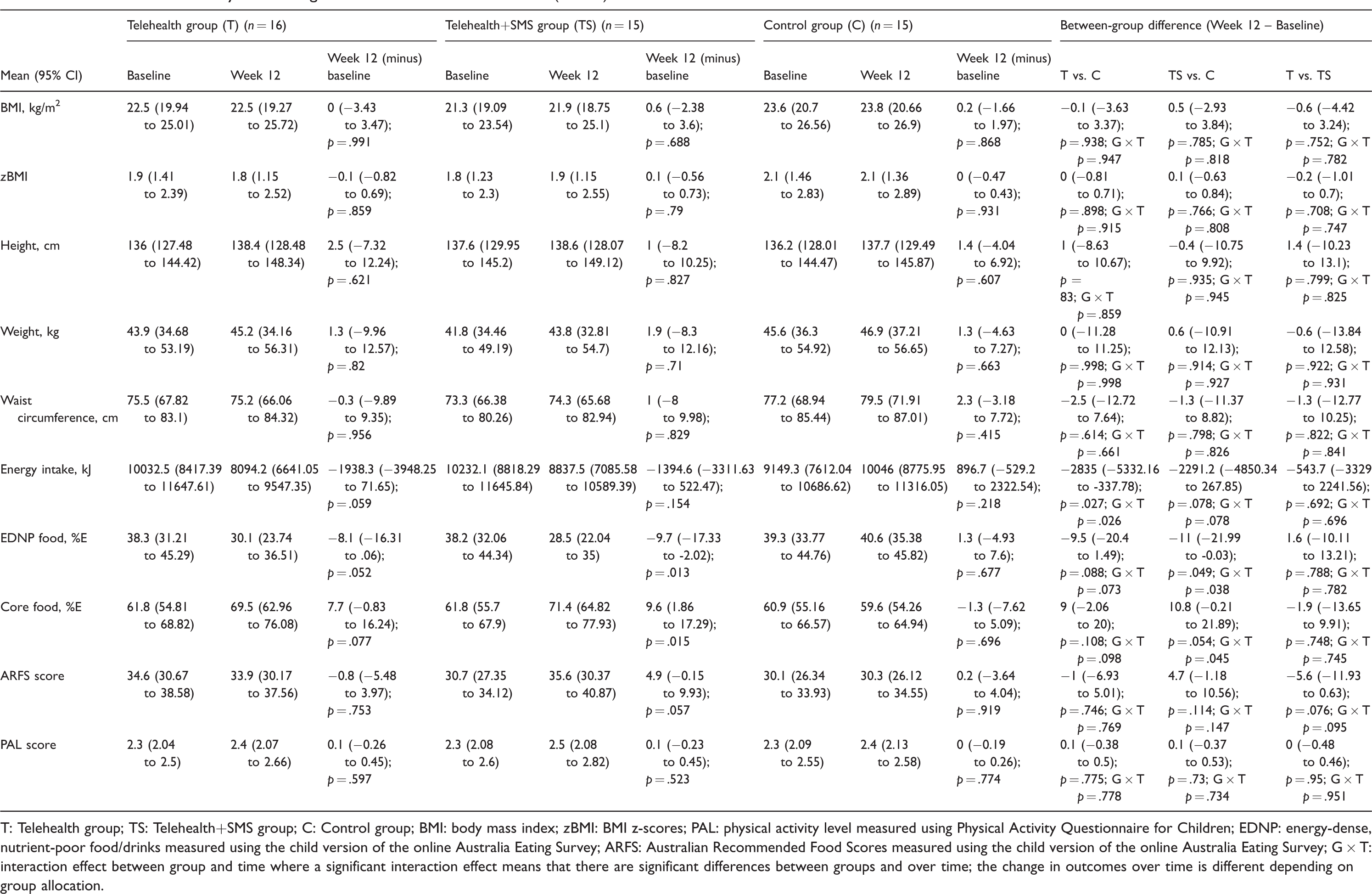
T: Telehealth group; TS: Telehealth+SMS group; C: Control group; BMI: body mass index; zBMI: BMI z-scores; PAL: physical activity level measured using Physical Activity Questionnaire for Children; EDNP: energy-dense, nutrient-poor food/drinks measured using the child version of the online Australia Eating Survey; ARFS: Australian Recommended Food Scores measured using the child version of the online Australia Eating Survey; G × T: interaction effect between group and time where a significant interaction effect means that there are significant differences between groups and over time; the change in outcomes over time is different depending on group allocation.
Discussion
The current study evaluated the feasibility and preliminary efficacy of a novel 12-week family-focused online telehealth nutrition intervention to support families of children aged 4 to 11 years who were, or were at risk of overweight and obesity in improving child weight status and dietary intake. Findings demonstrate that a tailored family-focused online nutrition intervention delivered by APDs using telehealth consultations is feasible, with no major technological problems encountered and very few participants requiring additional support to download and install the telehealth platform (Scopia). Consistent with existing research, there were no significant technological problems noted in using telehealth.19,51,52 It is encouraging that parents were able to set up and initiate the telehealth connection independently based on written instructions provided on the website, indicating that telehealth can be offered as an alternative modality for family-based childhood obesity nutrition intervention. A previous systematic review reported that telehealth showed promise for addressing childhood obesity and could be a reasonable approach for reaching a wider population, especially geographically isolated families. 18 The current study was able to provide telehealth intervention to families living in medium to small regional areas (40% of participants were from MM 4 and 5) and has demonstrated that dietitian-led individualised telehealth consultations with a family-initiated telehealth connection using household electronic devices are feasible.
Preliminary results highlight that children in the intervention groups had maintained their BMI, waist circumference, and showed improved dietary intake at week 12. This supports findings reported in previous group-based telehealth childhood obesity interventions where children decreased energy intakes,51,52 increased fruit and vegetable servings, 51 and decreased their consumption of sugar-sweetened beverages 51 and EDNP food.51,52 The lack of statistically significant changes in child weight status have also been consistently reported in these studies.51,52 It is likely that the current study being a feasibility and pilot trial, which was not sufficiently powered to evaluate efficacy for primary outcomes, had insufficient sensitivity to detect statistically significant between-group differences in child weight status. Consequently, we conducted a post hoc sample size calculation using the standard deviation of child BMI (i.e. 5.1) and would recommend a sample size of at least 104 per group to be able to detect two units of difference in BMI at 80% power.
Evidence has shown the use of SMS in combination with additional behavioural interventions is effective in supporting parents to improve child weight-related behaviour.53,54 This represents a potential strategy to engage more than one parent in interventions by giving information that is complementary to telehealth consultation to both parents, thereby including parents who are not able to attend consultations. The current study also aimed to investigate whether additional SMS targeted to parents, when delivered as part of an online telehealth nutrition intervention would enhance intervention efficacy in improving child outcomes. The lack of a statistically significant difference between the Telehealth and Telehealth+SMS groups led to the hypothesis that both intervention groups may be just as effective. However, these results need to be interpreted with caution given the relatively small sample size overall, and the smaller group of mother–father dyads (n = 14 pairs) who received SMS. This small sample size had limited statistical power to detect significant differences in child outcomes both within and between groups. Thus, potential benefits of additional SMS should be explored in a future larger trial.
The overall retention rate for the current study was 78% at week 12, which is slightly higher than existing childhood obesity intervention studies, which reported retention rates ranging from 27% to 73%. 55 Research has reported that programme enrolment is enhanced by a parent’s awareness of and desire to improve their child’s overweight status, 56 while programme attendance is improved by child involvement in attendance decisions. 57 The current study targeted both parents and children through telehealth and the web-based intervention components and hence was more inclusive in engaging the entire family in the intervention. This may be a potential reason for the comparatively higher retention rate in the current study. Interestingly, all drop-outs at week 12 in the current study were from the intervention groups, with 100% week-12 retention in the Control group. This suggests that families remained motivated to improve child weight status and dietary intake once they had signed up for the programme, even though 3 months had elapsed since enrolment.
A previous survey (n = 75 parents) indicated that parents would be interested in participating in an online family lifestyle programme, with a preference for an online programme that was easy to use, practical, engaging, endorsed by qualified health professionals, and that had the facility to involve their children while providing individual tailored feedback for the children. 15 However, it remains uncertain whether the in-person data collection appointments of the current study were a barrier to families’ participation, as transportation and scheduling conflicts have been some of the identified barriers to programme engagement in childhood obesity interventions. 58 Future studies should explore whether a solely online programme could attract a greater number of families to enrol in the programme, thereby increasing participation rates. A solely online programme offers the potential to combine telehealth and use of the personalised nutrition and dietary intake report generated from the validated parent-reported child AES, which can be completed online at home. 45 Existing validation studies identified that parents are relatively accurate reporters of their child’s height and weight.23,59 Hence, by using web-based approaches, clinicians can collect child anthropometrics and dietary intake data remotely without families having to travel and schedule for in-person appointments at clinics.
The preliminary efficacy results warrant caution in their interpretation and generalisability given the study limitations. The AES has been associated with an over-reporting bias, consistent with previous studies reporting validation results for FFQs relative to other reference methods. 60 While the AES may not be suitable for estimating absolute dietary intake for children, it has been demonstrated to provide a relative validation of parent-reported child fruit and vegetable intake using plasma carotenoid concentrations: beta-carotene (r = 0.56, p < .05), alpha-carotene (r = 0.51, p < .001) and cryptoxanthin (r = 0.32, p < .001). 42 The short time frame and small sample size of the current study are likely to have contributed to the insufficient power to detect a statistical significance in child anthropometry outcomes. However, the purpose of feasibility studies is to determine whether the intervention warrants further testing and to identify areas for refinement. The current study showed that a personalised family-focused online telehealth nutrition intervention is feasible for families facing the issue of childhood obesity, and likely to improve child weight-related and dietary outcomes. Using technology-based dietary assessment, this intervention offers families easy access to personalised, credible and timely dietetics consultations using telehealth in the comfort of their own home. The intervention modalities are highly scalable, and the novel approach may increase access for a large number of families to health services without the inconveniences of transportation, travel time or cost, an important clinical implication.
In conclusion, a 12-week family-focused online nutrition intervention delivered using telehealth technology to support parents in improving child weight status and dietary intake is feasible. The feasibility of the intervention and modest improvements in child outcomes warrant further investigation in a fully powered RCT assessing intervention efficacy and whether a solely online programme will increase participation, retention and reach.
Footnotes
Acknowledgements
We would like to acknowledge the support of Professor Jennifer May and staff members at the University of Newcastle Department of Rural Health in Tamworth, staff members of the University of New England at the Tablelands Clinical School in Armidale, and Ms Reena Bilen from Newy with Kids (formerly The Mummy Project). We are grateful for the use of their facilities, equipment, social media and support. We would like to thank Head Dietitian Ms Denise Wong See, of John Hunter Children’s Hospital, for her support in reviewing the Back2Basics Family website; Mr Ashley Young for providing technical support related to Hunter New England Clinical Telehealth; Accredited Practising Dietitian Ms Erin Clarke, for delivering the telehealth consultations; research assistants Dr Lee Ashton, Ms Katherine Brain, Ms Madison Beringer and Ms Ellen Payne for their assistance in lab assessments and data collection. We also thank the parents and children involved in the Back2Basics Family programme for their time and participation. This study forms part of the PhD thesis of LKC at the University of Newcastle.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received funding from nib foundation through the Hunter Medical Research Institute. The funding body was not involved in the research design, implementation, data collection, analysis and interpretation, or writing of the manuscript. LKC is supported by the University of Newcastle International Postgraduate Research Scholarships, Barker PhD Award Top-up Scholarship, and Emlyn and Jennie Thomas Postgraduate Medical Research Scholarship through the Hunter Medical Research Institute. CEC is supported by an NHMRC Senior Research Fellowship and a Faculty of Health and Medicine, Gladys M Brawn Senior Research Fellowship, the University of Newcastle. TLB is supported by a Faculty of Health and Medicine, Early Career Brawn Fellowship, the University of Newcastle.