
Abstract
Introduction
Primary care provider (PCP) competency in dermatology is inadequate despite the high volume of patients with skin conditions. Better education and access to dermatology expertise is vital to improve patient care. We present a comprehensive case-based evaluation of Dermatology Extension for Community Healthcare Outcomes
Methods
This is a retrospective cross-sectional study evaluating the use and impact of Dermatology ECHO over a 2-year period. Outcomes assessed include patient demographics, PCPs’ diagnostic accuracy, and expert treatment impact. Results were analysed using summary statistics and Pearson’s chi-square test to describe the adult and paediatric populations.
Results
One hundred and sixty-seven adult cases and 56 paediatric cases were presented in 2016–2017. Among the 223 cases, 137 adult and 44 paediatric cases were complete and eligible for analysis. The mean lesion duration was 3.3 years in adults and 2.9 years in children prior to presentation. Upon case presentation, almost half (43.8%) of the adult cases were incorrectly diagnosed by their PCP with 18.8% receiving a partially correct diagnosis. PCPs had greater diagnostic accuracy in children (45% correct diagnosis, 27.5% partially correct, 27.5% incorrect). Expert treatment recommendations benefited 83.6% of adult cases and 72.5% of paediatric cases.
Discussion
This study highlights the need for better dermatology access and teaching opportunities among PCPs in Missouri. Dermatology ECHO provides a platform for didactic learning and case presentations to improve dermatology competency among PCPs.
Keywords
Introduction
Dermatology, including the recognition and treatment of common skin conditions, is a vital component of the primary healthcare experience. Skin conditions account for the primary complaint in 5% of all patient primary care visits and up to 30% of paediatric primary visits in the outpatient setting,1–5 and over one-third of patients at primary care visits have at least one dermatologic condition. 6 Additionally, skin cancer is the most common malignancy in the United States with an estimated incidence of 5.4 million cases of nonmelanoma skin cancer in 2012. 7 Despite the frequency of dermatologic complaints during primary care visits, residents and practicing physicians typically lack formal training in dermatology. 8 Many medical schools do not offer dermatology electives and less than 40% of primary care residents feel adequately prepared to diagnose and treat common skin conditions. 9 Multiple studies have also shown a knowledge gap in this subject among primary care providers (PCPs).6,10,11 As the dermatology physician shortage continues to result in long patient wait times and difficult regional access,12–14 more patients will inevitably rely on local PCPs for diagnosis and treatment of their various skin conditions.
Extension for Community Healthcare Outcomes (ECHO) is an innovative approach to increase competency of specific areas of specialty care among PCPs. First developed in New Mexico to increase competency in the treatment of hepatitis C, 15 this teaching modality has now expanded across several areas including chronic pain management, endocrinology, community healthcare workers, and autism with positive results on PCPs’ self-efficacy and knowledge.16–19 The ECHO model uses videoconferencing technology to link specialists to PCPs at regular intervals. During these conferences, specialists provide teaching via didactic presentations and expert recommendations on de-identified case presentations from participants.
The University of Missouri-Columbia (MU) Show-Me ECHO Project is the first to adapt this technology to the field of dermatology. Herein, we present a comprehensive programme evaluation and quality improvement project in Dermatology ECHO, which determined the diagnostic and treatment accuracy of dermatological conditions by PCPs over a 2-year period.
Methods
MU Institutional Review Board reviewed and discussed our project and determined it did not qualify as a human subject research project since all data were de-identified prior to data collection. Our project was designed as a retrospective, cross-sectional pilot study analysing ECHO dermatology case presentations over the 2016–2017 period. Analysed datasets included archived recorded video Dermatology ECHO sessions, submitted case presentation forms from participating PCPs, and case recommendation forms from the team of dermatologists. Dermatology ECHO conferences occurred in 1-h sessions once a week. Board-certified dermatologists, including a general dermatologist, paediatric dermatologist, and dermatopathologist, led these weekly session in which a 15-min didactic presentation on different dermatology topics was presented, followed by real-life case presentations from attending PCPs: family practitioners, internists, physician assistants and nurse practitioners. Free continuing medical education credits were given as an incentive to participate. Due to limitations of state funding, only Missouri providers were invited to attend.
PCPs were encouraged to present complex de-identified cases from their patient population for expert evaluation, which included evaluation of probable diagnoses and treatment recommendations. Cases were considered complex by the PCP, which translated into patients with unique symptoms, an inconclusive diagnosis, multiple comorbidities, socioeconomic barriers in accessing medical care, etc. Cases were presented to the entire cohort of dermatologists and participants, with the expert dermatologists evaluating cases verbally to enable group learning.
Data on case characteristics, PCP diagnostic accuracy and treatment impact were collected. Case characteristics included age, gender, race/ethnicity, lesion duration and reason for presentation to their PCP. PCP diagnostic accuracy (three categories: incorrect, partially correct, correct) was assessed by comparing the PCP differential diagnosis at the time of case presentation to the expert differential diagnosis. A ‘partially correct diagnosis’ was assigned when the PCP listed the correct diagnosis among his/her provided differential diagnosis. Meanwhile, an ‘incorrect diagnosis’ was assigned when the PCP differential diagnosis did not contain the correct diagnosis, while a ‘correct diagnosis’ was assigned when the PCP listed a single correct diagnosis. Treatment impact was determined by assessing changes to the existing PCP treatment plan after expert recommendations were given (four categories: changed treatment plan, provided treatment plan, added to existing treatment plan, no change). The category ‘changed treatment plan’ was considered to have the highest impact factor, as this indicates the original treatment plan was incorrect and could have led to patient harm or extra cost to the healthcare system. ‘Provided treatment plan’ indicates the PCP did not have an original treatment plan in place, which was then provided by the experts, and ‘added to existing treatment plan’ denoted when experts expanded on the original treatment plan given by the PCP.
Only cases with enough information to be categorised as described above were included and analysed. Participants submitting cases were provided access to standardised case-forms to facilitate consistent data collection. PCP accuracy and treatment impact were assessed on new case presentations only, as follow-up cases that had already been presented at an earlier ECHO conference were excluded. These results were compared in the adult and paediatric populations. Results were analysed using summary statistics. Pearson’s chi- square test was performed to evaluate significant differences in diagnostic accuracy and treatment recommendation when comparing paediatric and adult cases, with α = 0.05 for both tests. Chi-square tests of independence and Fisher’s exact test (for cell counts of less than five) were performed to examine the relation between the accuracy and the treatment categories for each group.
All data analyses were performed using SPSS version 25 (SPSS Inc., Chicago, IL, USA) and SAS version 9.3 (Cary, NC).
Results
From January 2016 to December 2017, 74 ECHO conferences occurred with a total of 18.5 h of dedicated didactic time presented over this 2-year period. The remaining time was devoted to case discussion. Sixty providers attended these sessions with 12 providers presenting cases eligible for analysis. The remaining 48 providers enrolled as ‘observers’, in which they did not present cases for discussion and telementoring but gained new knowledge from case discussions and observing didactic presentations.
A total of 223 cases, 167 adult and 56 paediatric, were presented at Dermatology ECHO sessions. Each case was discussed for an average of 14.9 min. Of the 223 cases, 81% had complete data eligible for analysis (137 adult and 44 paediatric cases). Among these 181 cases, 93% were new cases (128 adult and 40 paediatric) (Table 1). The majority of cases were presented for diagnosis verification (80% adult and 65.9% paediatric cases) with paediatric cases having a higher emphasis on seeking treatment recommendations (25%). The mean lesion duration prior to presentation was similar in the adult and paediatric populations (3.3 years in adults and 2.9 years in children) (Table 1).
Case demographics.
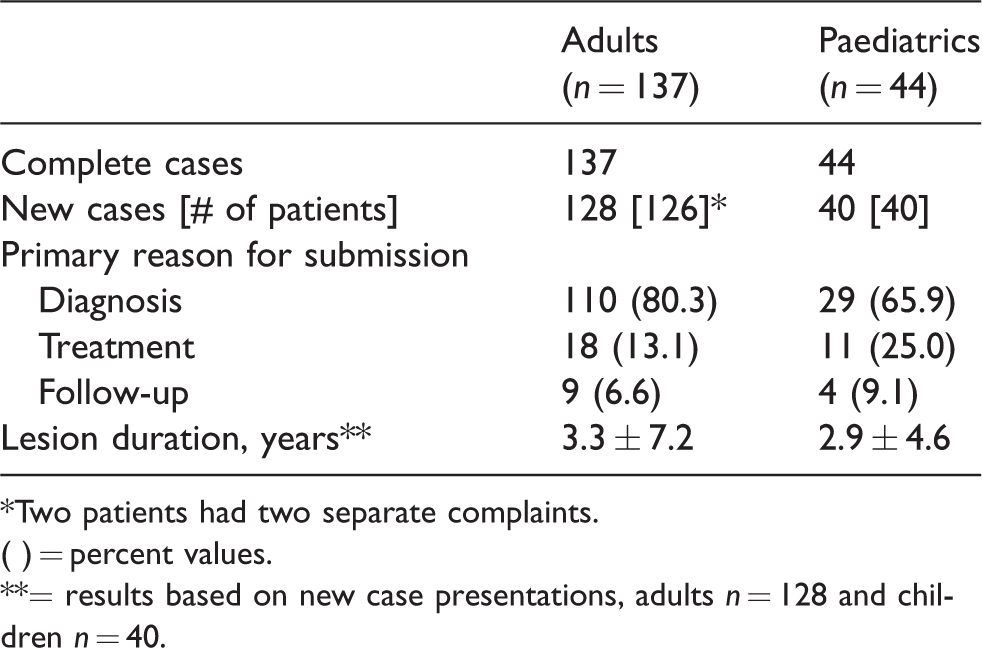
*Two patients had two separate complaints.
( ) = percent values.
**= results based on new case presentations, adults n = 128 and children n = 40.
Patient demographics are available in Table 2. Among the 168 eligible cases, about a third of the adult patients and half of the paediatric patients were male. The mean ages were 50.5 years and 8.5 years in adults and children respectively. Race and ethnicity demographics are reflective of the Missouri population.
Patient demographics.
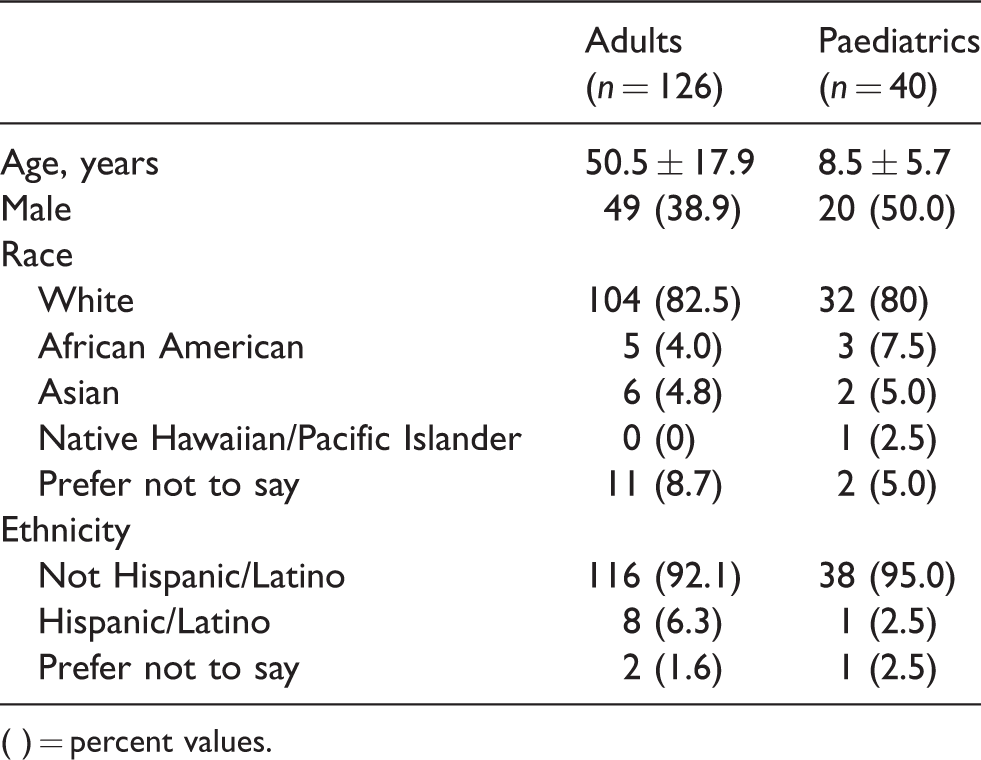
( ) = percent values.
There was no statistical significance when comparing diagnostic accuracy in the paediatric and adult cases, χ2(2, N = 168) = 3.574, p = 0.167. Nor was there statistical significance when comparing treatment impact in the paediatric and adult cases, χ2(3, N = 168) = 3.107, p = 0.375.
However, overall diagnostic accuracy was poor with 43.8% (n = 56) of adults and 27.5% (n = 11) of children being incorrectly diagnosed (Table 3). Of the 66 correctly diagnosed cases, 85.4% (n= 41) of adult cases and 77.8% (n = 14) of paediatric cases benefited from expert treatment intervention (Table 4). Overall, only 16.4% (n = 21) of adult cases and 27.5% (n = 11) of paediatric cases did not require any changes to the treatment plan from experts (Table 4). Thus, a significant proportion of cases benefited not only from expert diagnosis, but from the expert-provided treatment recommendations as well. Interestingly, PCPs were less likely to need treatment intervention in the paediatric population even though there were a higher percentage of cases submitted specifically for the purpose of treatment intervention mentoring in this population.
PCP accuracy of initial diagnosis.
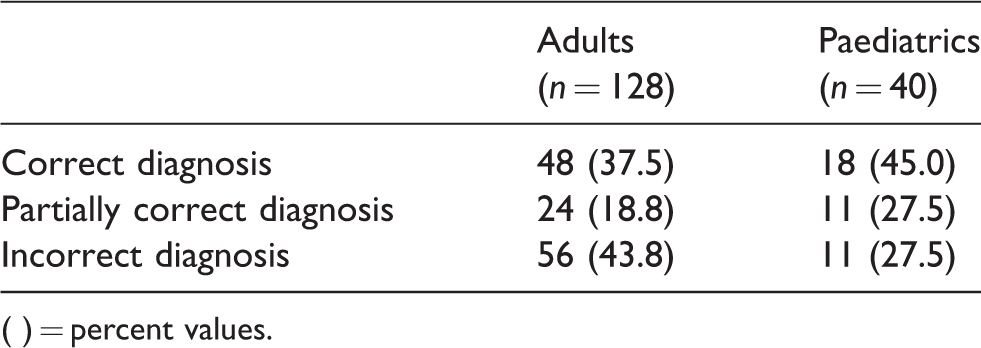
( ) = percent values.
Treatment impact of cases.
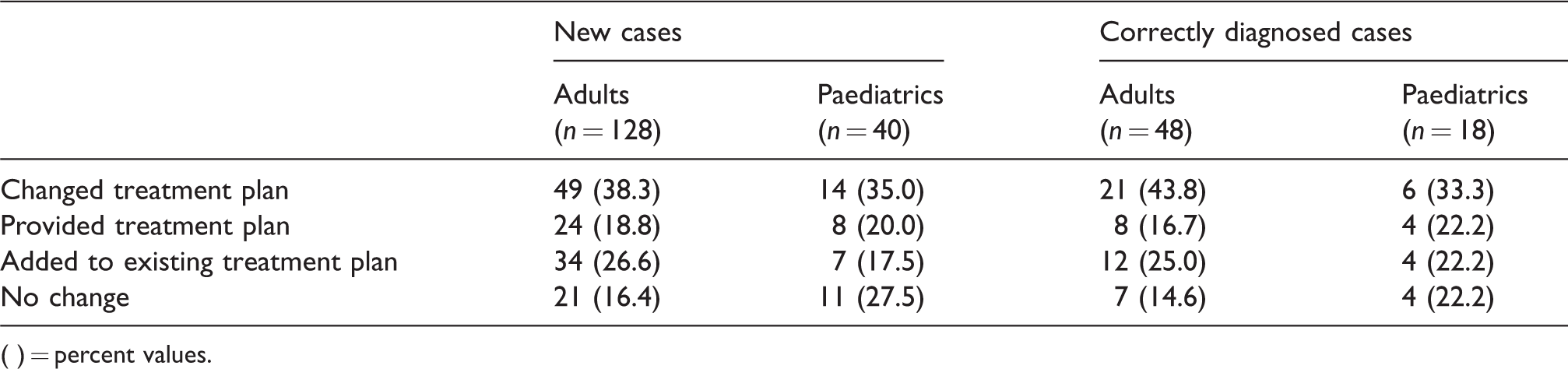
( ) = percent values.
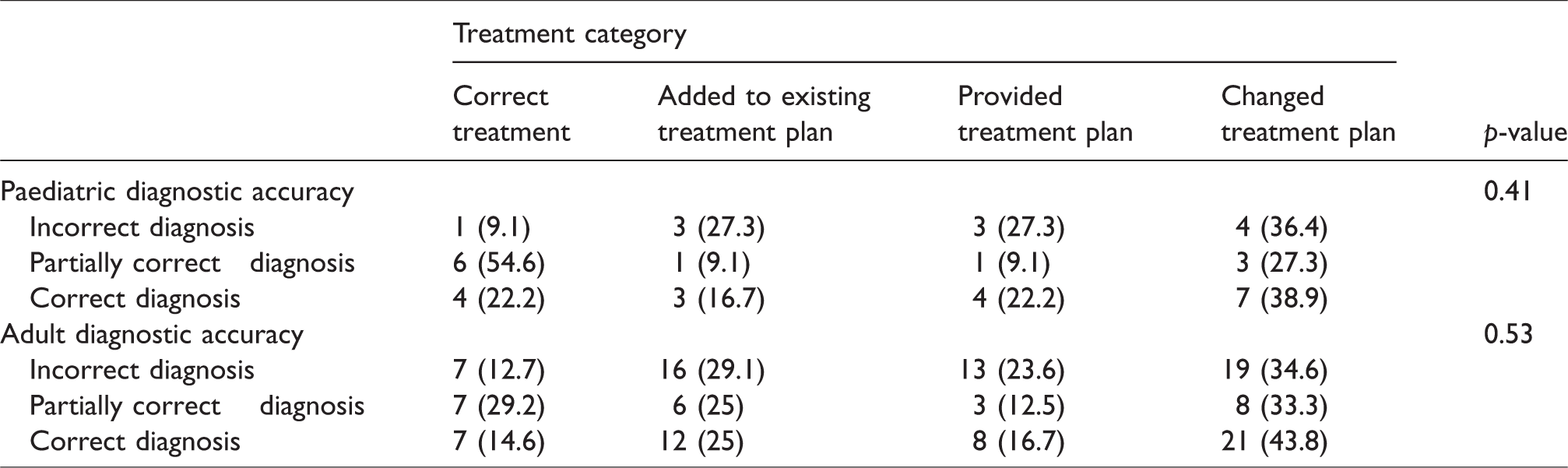
There was no evidence of diagnostic and treatment independency in paediatric or adult patient groups (Table 5).
Accuracy of diagnosis by PCP according to recommended treatment by ECHO hub dermatologist for paediatric and adult patients.
Discussion
PCPs and their patients benefited greatly from the implementation of these Dermatology ECHO conferences, as only a small portion of providers had a singular correct diagnosis and no SUBSEQUENT changes REQUIRED to their treatment plan. Our results also showed that the accuracy of the diagnosis was not related to initial treatment provided by the participating PCPs for either the paediatric or adult patients. This project highlights the need for better education and access to dermatology expertise for PCPs in the state of Missouri. Since almost 44% of all medical office visits are scheduled with PCPs, 20 these providers will inevitably continue to encounter both common and complex skin conditions.
Discordance between diagnoses provided by PCPs and dermatologists has been demonstrated before: a 2001 study by Lowell et al. demonstrated agreement between PCPs and dermatologists in only 57% of cases, 6 while Federman et al. found the diagnostic accuracy of nondermatology physicians to be 52%. 21 This is similar to our adult data where 56.3% of cases had a correct or partially correct diagnosis. There have been many educational interventions implemented to improve skin cancer detection and treatment among PCPs, which have been successful.22–24 However, this evaluation demonstrates that PCPs’ educational needs extend beyond this singular topic. Furthermore, these interventions were brief, one-time educational opportunities, as opposed to the longitudinal learning provided in the Dermatology Show-Me ECHO project.
Dermatology ECHO’s education-centred approach addresses real-time cases and uses them as a teaching modality with structured didactic sessions to improve dermatology competency among PCPs. It breaks from the traditional referral model in which PCPs outsource complex or unfamiliar cases. This traditional model does not allow for learning and commits the patient to long-term specialty care, which is often regionally inconvenient and expensive. Less than 10% of dermatologists practice in rural areas and 88% of rural counties in America have zero dermatologists.25,26 This lack of access also extends to low socioeconomic and minority areas. 25 Dermatology ECHO goes beyond the standard telemedicine approach currently being used to improve patient access to specialty care. By using real-time provider-supplied cases as teaching opportunities, Dermatology ECHO addresses knowledge deficiencies and enables PCPs to better treat skin conditions in their own communities.
The implementation of Dermatology ECHO in Missouri not only improved patient access to specialty care, it also allowed PCPs to obtain the correct diagnosis and optimise treatment plans for their patients. The potential savings to the healthcare system from Dermatology ECHO have been established through a small pilot study and need to be evaluated further, 27 but medical errors are known to be a financial burden on healthcare. A 2017 study demonstrated the projected costs of misdiagnosis of lower extremity cellulitis to be $195 million to $515 million in the United States annually. 28 In addition, many patients with cutaneous manifestations of systemic diseases in emergency departments or inpatient settings are often misdiagnosed and/or mismanaged by PCPs, 29 further adding to the financial burden caused by inaccurate and delayed diagnoses.
The ECHO model educates multiple providers at once, efficiently addressing these knowledge deficiencies and ideally improving future patient care. While not yet assessed in Dermatology ECHO, this teaching modality has been successful in increasing competency in the subjects of endocrinology, mental health, and hepatitis C among participants.30–32 Based on these studies, this model will also likely increase competency among Dermatology ECHO participants as well.
Limitations
This study is limited by its small sample size and regional exclusivity making generalisation difficult. Additionally, participants had varying years of experience and exposure to dermatology prior to participation in Dermatology ECHO. While this study addressed the potential need for such a programme, it did not evaluate the efficacy of its educational model or cost-effectiveness. Since most of the participating providers practice in clinics other than the University of Missouri Health System (UMHS) outpatient clinics and therefore are not connected to the UMHS electronic medical records system, we were not able to verify implementation of recommendations from ECHO sessions. This will need to be addressed in a future study.
Conclusions
This project demonstrates a knowledge gap that exists among PCPs in both the diagnosis and treatment of skin conditions. We believe this model is the ideal solution to improving competency in the field of dermatology as it efficiently educates multiple providers at once while simultaneously improving patient outcomes. Our results also indicated that 60 providers observed Dermatology ECHO, and 12 (20%) provided case presentations. Challenges with time commitment may prevent providers from presenting cases. However, informal feedback from participants, as well as from a number of PCPs joining the sessions, suggests the cases selected were relevant. As this model is especially applicable to providers who practice in rural areas of lower socioeconomic status where access to expert dermatologic care is very limited, more efforts should be done to educate administrators on the benefits of providing time to PCPs to submit their cases for ECHO discussion. Now that the utility and impact of Dermatology ECHO has been established, more research needs to be conducted into the long-term outcomes of its educational interventions.
Footnotes
Acknowledgements
We would like to acknowledge Karen Edison, M.D. and Rachel Mutrux for their leadership and support in Dermatology ECHO, as well as the staff members of the Show-Me ECHO project for their assistance with data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.