
Abstract
Introduction
Telemedicine when properly implemented can be used to facilitate consultations from physicians with little or no burn experience by providing access to qualified physicians in burn care to reduce the workload in emergency departments or elsewhere. In this study, the role of telemedicine in the management and triage of pediatric burn patients admitted to the emergency department of a tertiary care hospital is investigated.
Methods
This cross-sectional study was conducted between 1 January 2019 and 31 December 2020 and a total of 210 patients were enrolled in the study. Patients were initially evaluated in the emergency room by a pediatrician and consulted by an experienced burn specialist using lesion images. An in-person assessment of the patients was performed by another burn specialist according to the clinical decision made via telemedicine. The data of both assessments and clinical data of the patients were examined.
Results
The mean age of our patients was 3.35 ± 3.7 years. Most of the burns were scalds with hot liquids (71%). After the consultations, 73 patients were discharged from the emergency room. The rest were decided as follow-up at the burn outpatient clinic (n = 99) or hospitalization (n = 35) and in-person assessment was performed for these patients. The inter-rater reliability value for “clinical decision” was almost perfect (Cohen's kappa value is 0.923). Also, the level of concordance between the two assessments was very high for burned total body surface area (interclass correlation coefficient = 0.999).
Conclusion
In the management and triage of pediatric burn patients admitted to the emergency department, telemedicine and in-person examination resulted in almost perfect agreement in terms of clinical decision and total body surface area. Legal arrangements and regulatory changes are essential to support the safe and wide adoption of telemedicine, which is a reliable method in emergency room settings.
Introduction
Telemedicine (TM) is the use of telecommunication technologies to provide medical information and services. The evaluation of burns needs experience. The burned total body surface area (TBSA), burn depth, age, and weight of the patient are important aspects that the emergency physicians should evaluate for further management of the patient. Burns are typically cutaneous and visible injuries except for burns that occurred with electrical current. Hence, in most instances, they can be evaluated accurately and quantified as to both extent and depth by visual examination. 1
Many physicians receive little or no training in burn evaluation or management. This can lead to serious errors in burn evaluation, triage, transfer to burn center, and the treatment of the patient.1–5 TM helps diagnosis and treatment by enabling information exchange from a distance which is a great clinical decision support for the emergency physician.
The width and depth of the wound are evaluated once the patient is transferred to an emergency room. An appropriate fluid resuscitation is initiated by opening vascular access when needed. In first-degree burns, moisturizing creams are sufficient; the wound does not need to be covered. In second-degree burns, the wound is closed with gauze impregnated with paraffin or oily cream. 6 Almost 40% of interventions performed in a health institution were found to be inappropriate in the first treatment of burn patients. 6 TM fills the gap in meeting the need for specialized burn care even in locations where it may be logistically impossible.1,3,7–9 TM and the use of smartphones in the medical field have contributed significantly to the diagnosis, need for referral, treatment, and follow-up of patients especially in limited-resource environments.8,10–12 Furthermore, the global spread of coronavirus disease 2019 (COVID-19) affected health care providers worldwide. In the current COVID-19 crisis and future outbreaks, we do not know yet implement TM to optimize pediatric health care delivery.13–18
Initially, videoconferencing was used for consulting burn patients. The system required fixed rooms between two centers equipped with necessary devices and trained staff. The counterparts performed the consultation at the time of appointment.19,20 A TM system should capture an image, temporarily store it, send this image to a remote location, and view it without loss of resolution. A smartphone has all these properties.
Mobile applications are getting popular in burn treatment by the widespread smartphone usage. 1 In some studies, applications which are specially designed for burn assessment are used, but their availability is limited to care providers who are in the project.2,4,9 Recently, WhatsApp (WhatsApp LLC, Menlo Park, California), which is an instant messaging application that allows smartphone users to exchange text, image, video, and audio messages for free, is gaining popularity among health care providers because of low cost, availability, and ease of use.7,10,11
In this study, we aimed to evaluate the use of smartphones, WhatsApp, and TM in the management of pediatric burn patients admitted to our emergency service.
Materials and methods
This cross-sectional study was conducted between January 1, 2019 and December 31, 2020 in the pediatric emergency unit and burn center of a tertiary care hospital. A total of 210 patients were enrolled in the study. Among them, three intubated patients with the critical clinical condition were excluded from the study.
Initial evaluation and treatment were carried out in the emergency unit by the same pediatrician throughout the study. After the patient was stabilized an informed consent was obtained from the parents of the patients for imaging of the burn lesions implementing that all data were subject to the current laws for data protection. Burned body parts and lesions were visualized by the same pediatrician who evaluated the patient, paying attention to protect the privacy of patients. A smartphone (iPhone 7) with a 7-megapixel (f/2.2) front camera was used to take photographs. Photographs were taken in a well-lit room in photo mode with no filters and no flash activation. No rulers or other objects were used. These images together with additional information such as etiology of the burn, gender, age, and weight of the patients were transmitted by WhatsApp. Two burn specialists were involved in the study. One of them examined the images on the smartphone (iPhone 8) with no adjustment or program. The TBSA and the clinical decision for each patient were reported. There were three kinds of decisions and the patients were divided into three groups according to these decisions. In the first decision, the patients were discharged from the emergency unit (after their burn care, prescription, and follow-up advice) for treatment by primary care facilities or at home. The second decision is follow up of the patient at the outpatient clinic of the burn center and the last decision is the hospitalization of the patient. The patients in the second and third decision groups were examined face-to-face by the other physician specialized in burn care. The results of the face-to-face examination were also reported for further analysis.
Approval was obtained from the local ethics committee of our hospital for the study (date October 24, 2018/decision no. 300).
Statistical analysis
Statistical Package for Social Sciences 20.0 for Windows (SPSS 20.0) was used for the analysis of the data. Variables were checked for normal distribution. As the data did not distribute normally, Kruskal–Wallis test was used for comparison of the continuous variables, whereas χ2 test was used for comparison of the categorical variables between groups. An interrater reliability analysis was performed to determine the consistency of “clinical decision” using the kappa statistic, whereas interclass correlation coefficient (ICC) was used to analyze the concordance of TBSA among raters of the face-to-face examination and evaluation with WhatsApp. Categorical measurements were given as a number (n) and percentage (%), continuous measurements as mean ± SD, and median (min–max).
Results
The mean age of the patients was 3.35 ± 3.7 years. Among them, 48.3% were male (n = 100) and 51.7% were female (n = 107). Most of the burns were scalds with hot liquids (71%) and there was a substantial amount of contact burn patients (19.3%). The rest were flame burns (n = 15, 7.2%) and five of them were categorized as others (2.4%).
There were 73 patients in the first decision group. The mean age of these patients was 3.51 ± 5.2 years. The percentage of burned TBSA was 1.67 ± 0.9. Most of the burns were scalding (n = 39, 53.4%) followed by contact burns (n = 27, 37.8%). The rest were flame (n = 4, 5.5%) and other burns (n = 3, 4.1%). The percentage of burned TBSA was higher in groups 2 and 3. Scald burns were still the main etiology for burns but the percentage of flame burns was higher especially in group 3. The demographic and clinical data of the patients based on groups are given in Table 1. The results of group 1 are based on TM assessment and the results for groups 2 and 3 are based on the face-to-face assessment in this table.
Demographic and clinical data of the study population based on groups.
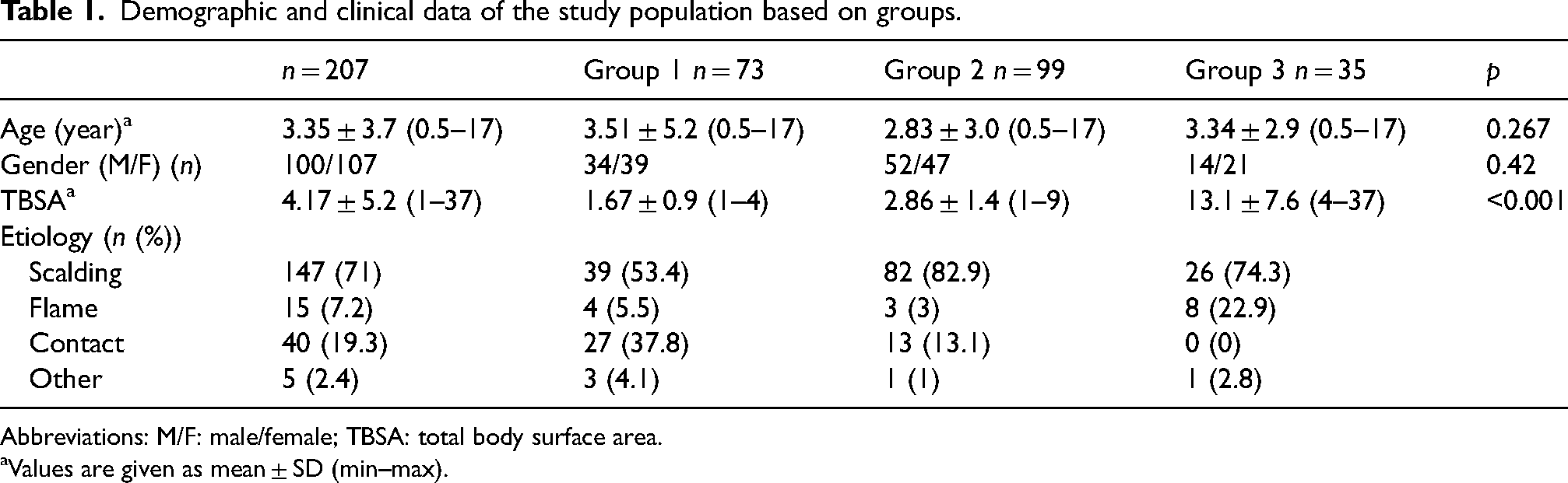
Abbreviations: M/F: male/female; TBSA: total body surface area.
Values are given as mean ± SD (min–max).
The final decision was made based on the face-to-face assessment. Two patients decided by WhatsApp as follow up of the patient at the outpatient clinic (group 2) were moved to the hospitalization group (group 3) after the face-to-face assessment as they turned out to be third-degree burns in the latter assessment. Also, two patients with burns to the hands and fingers were moved from group 3 to group 2 after an in-person assessment as they could be handled without hospitalization. The burn etiology for these patients was scalding so the data regarding the etiology remained the same between groups 2 and 3. The clinical data of patients in groups 2 and 3 according to the TM and face-to-face assessment is presented in Table 2.
The clinical data of patients in groups 2 and 3.
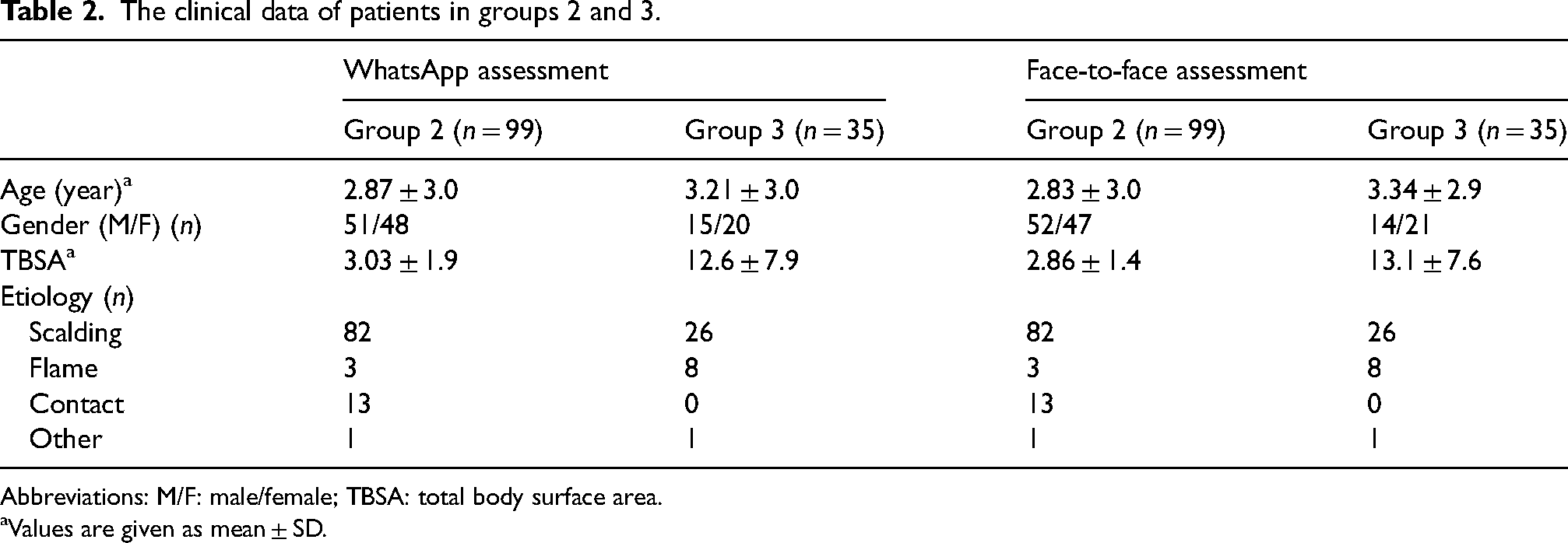
Abbreviations: M/F: male/female; TBSA: total body surface area.
Values are given as mean ± SD.
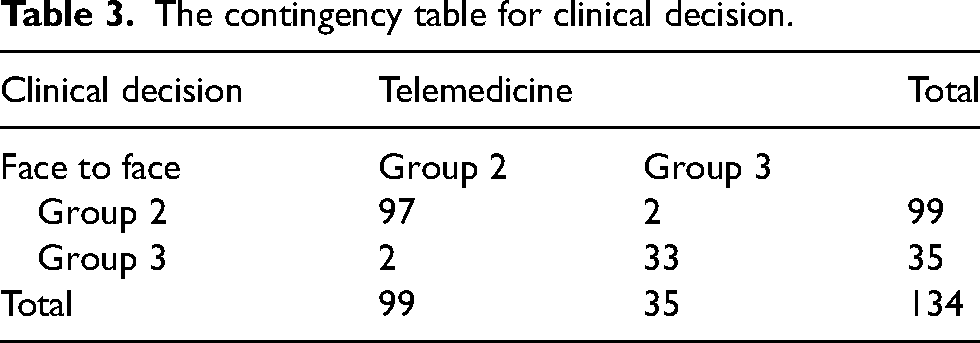
In group 1, the decision was made only with TM. Whereas in groups 2 and 3, two different methods of assessment were used namely TM and face-to-face examination each performed by a different physician. The interrater reliability value for “clinical decision” was almost perfect (Cohen's kappa value is 0.923) for groups 2 and 3 comparing these two methods. The level of concordance between the two assessments was very high for TBSA (ICC = 0.999) (Tables 3 and 4).
The contingency table for clinical decision.
Interrater reliability and concordance values of assessments by face-to-face examination versus telemedicine group.

Abbreviation: TBSA: total body surface area.
Cohen's kappa.
Interclass correlation coefficient.
Seventy-three patients (35.3%) were discharged from the emergency room. No problem was seen in the recovery period of these patients. Two patients in group 2 were hospitalized due to delayed epithelization and grafting was performed for the closure of their remaining burn lesions.
Discussion
We have evaluated the role of TM in the management and triage of pediatric burn patients admitted to an emergency room in this study. We found that 35.3% of patients can be managed without face-to-face assessment by a burn specialist. There was a high concordance for TBSA evaluation between WhatsApp and face-to-face assessment of the burn lesion and almost perfect agreement in “clinical decision.” Our findings support that triage of pediatric burn patients admitted to the emergency room can be managed safely with the use of TM.
Emergency departments of tertiary care hospitals are intensively working with health care providers and inappropriate transfers add to their workload. This is more pronounced in pediatric burns as there is a lack of training among emergency physicians in the evaluation and management of burns.2,6 This leads mostly to overestimation of the burn size and thereby unnecessary transfers.3,4,7,11,12
The COVID-19 pandemic has challenged the health care systems worldwide. The outbreak rapidly transformed the health care system to virtual health where possible by integrating TM. There is an ongoing process of optimizing digital approaches to health care systems, applying the changes to patient care, and providing the safety of health caregivers as well. Also, the COVID-19 outbreak and other possible future pandemics force the system to this adaptation.13,21–23
The number of burn centers is limited and these centers serve a large region. Eliminating burn patients for transfer to a burn center will help to reduce the workload of transfer services and the emergency departments. Different TM techniques were used to achieve this goal. Videoconferencing was once used with high patient satisfaction and travel savings.19,20 With the widespread use of smartphones, work on this issue has also accelerated.7,10–12,23
In our study, 35.3% of patients were discharged from the emergency department after assessment by TM only. Most of these patients were scalds and contact burns with a burned TBSA of <5%. These patients would have been referred to the outpatient burn clinic if they were not evaluated with TM. We did not use any mobile phone application designed for burns in the study. A smartphone application designed for burns (Burn App) was used by Carmichael et al. 4 in their study. They hypothesized that the use of this Burn App could improve triage decisions particularly in cases of burns with 1–10% TBSA. In their study, 33% of patients with intermediate-size burns were down-triaged by using this burn application. There are similar other studies with 24.5% and 38% down-triage results.3,7 We studied mainly the accuracy of decision making rather than the impact of TM on down triage of burns and there was an almost perfect agreement with a Cohen's kappa value of 0.923 even in patients with TBSA > 10%.
In a similar study, the authors examined the diagnostic accuracy of a TM tool for the triage of acute burn patients. They found a high intra-observer concordance as 0.94 comparing TM consultation and the gold standard of an in-person consultation. In this study, the use of TM was able to detect that 83% of the patients could have been managed on an outpatient basis. 2 In our study, there were no tools or special applications for burn used either but a high concordance was achieved at the same time. Similar to their findings, 82.1% of our patients could be managed on an outpatient basis in our study. Each of the specialist physicians evaluating the results had at least 5 years of experience. Better results can be obtained by evaluating the images of burn lesions by experienced experts or by a group of experts to reduce the interobserver bias.
In a review article about the impact of TM on diagnosis and clinical management of rural trauma patients, only four of 187 articles reported the impact of TM on a diagnosis. Study findings suggested that the use of TM may improve patient diagnosis and streamline the process of transferring patients but the use of TM had minimal impact on mortality and complications in rural trauma patients. 23 There is a need for randomized clinical trials to validate these findings as the authors suggest. They also conclude that the application of TM also has great potential to enhance the education of providers at rural facilities.
In the current study, we have evaluated the clinical decision for pediatric burn patients made by TM and face-to-face assessment. In this study, a personal assessment of the pediatrician working in the emergency department who performed the initial evaluation and treatment of the patients admitted to the emergency department was not included. This can be considered as a limitation of the study as we could not demonstrate the experience gained from consultation with TM throughout the study period. Also, the lesion images could be assessed by physicians with different levels of experience in burns and a ruler could be used when capturing an image, which can be considered as other limitations of the study.
In the future, TM will play a greater role in delivering pediatric health care when it is accessible, available, and appropriate to address the problem. 13 The legal aspect of the TM should be revealed by laws and regulations. 1 There are various mobile phone applications used in burns for diagnosis, triage, transfer, and consultation.2,4,24 There is also the implementation of TM programs and protocols in pediatric burns and emergencies.3,5,12,22 The applications and TM programs should be standardized and guidelines should be updated. In this way, the results can be comparable and the guidelines and applications can contribute to physicians working in the emergency by increasing their experience and confidence.
Conclusions
Evaluation of pediatric burn patients and making a clinical decision with TM is a reliable and feasible method in emergency room settings. Making legal arrangements and regulatory changes are essential to support the safe and wide adoption of TM. The impact of TM on quality of burn care and contribution of knowledge to physicians working in the emergency issues to be addressed in future studies.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.