
Abstract
The use of emergency departments for non-emergent issues has led to overcrowding and decreased the quality of care. Telemedicine may be a mechanism to decrease overutilization of this expensive resource. From April to September 2020, we assessed (a) the impact of a multi-center tele-urgent care program on emergency department referral rates and (b) the proportion of individuals who had a subsequent emergency department visit within 72 h of tele-urgent care evaluation when they were not referred to the emergency department. We then performed a chart review to assess whether patients presented to the emergency department for the same reason as was stated for their tele-urgent care evaluation, whether subsequent hospitalization was needed during that emergency department visit, and whether death occurred. Among the 2510 patients who would have been referred to in-person emergency department care, but instead received tele-urgent care assessment, one in five (21%; n = 533) were subsequently referred to the emergency department. Among those not referred following tele-urgent care, 1 in 10 (11%; n = 162) visited the emergency department within 72 h. Among these 162 individuals, most (91%) returned with the same or similar complaint as what was assessed during their tele-urgent care visit, with one in five requiring hospitalization (19%, n = 31) with one individual (0.01%) dying. In conclusion, tele-urgent care may safely decrease emergency department utilization.
Introduction
In recent years, emergency departments (EDs) have experienced a dramatic increase in visits for non-emergent conditions.1–3 This is due, in part, to long wait times for outpatient appointments, limited after-hours care at physicians’ offices, and other barriers to accessing care. While many health care systems have implemented telephone-based nursing (RN) advice programs to reduce the burden of non-emergent care on EDs, recent evidence has found that remote triage programs often fail to reduce ED or primary care utilization. 4 In the early 2000s, urgent care (UC) centers and retail clinics grew in number in hopes to decrease the use of EDs for non-emergent conditions, 5 with recent studies suggesting that UC centers located near EDs can reduce the use of these resources. 6 Because virtual care is widely recognized as a means of increasing access to care, increasing patient satisfaction, and reducing costs to patients,7–10 hospitals and health care systems have begun exploring virtual UC platforms as one mechanism to optimize the use of EDs.11–14
The coronavirus disease 2019 (COVID-19) pandemic has further impacted how health care systems provide non-emergent care. In order to decrease vulnerable populations and providers from exposure to coronavirus, many EDs have adapted virtual platforms as a means to screen low-risk patients and preserve personal protective equipment. 15 Moreover, telemedicine has the capacity to improve ED flow, decrease congestion, and improve utilization patterns of this expensive resource. While there is a growing body of data examining the use of telemedicine in emergency and UC settings, the extent to which telemedicine can reduce ED utilization is not clear. 11 Moreover, among recently published studies, many are performed at single institutions or on small patient populations.12–14
As the largest integrated health provider in the United States, the Veterans Health Administration (VA) provides care for over 9 million enrolled Veterans. In March 2020, the VA made a dramatic nationwide shift from primarily providing in-person care to telemedicine-based care due to the pandemic. Recognizing the need for rapid assessment of non-emergent clinical scenarios, the VA initiated a tele-UC (TUC) program into a Veterans Integrated Service Network (VISN) with the goal of providing virtual-based clinical assessments for patients seeking non-emergent care. 1 The objective of this study was to describe the impact of a multi-center TUC program on ED referral rates patterns which, to date, is yet to be described.
Methods
Program overview
Starting in April 2020, the VA implemented a multi-center TUC program in VISN 21, a network of seven facilities located in California, Nevada, and the Pacific Islands. The goal of the program was to provide non-emergent care through a variety of virtual formats as a means of maintaining access to care while decreasing both patient and providers’ exposure risk during the COVID-19 pandemic. The TUC program was implemented during Weekends (Saturday and Sunday), Holidays, Evenings and Nights (WHEN) hours (4 p.m.–12 a.m.)—periods when outpatient clinics are closed, when VA EDs have less staffing and resources, and patients have greater difficulty accessing care for acute complaints.
Participants
The sample included all callers during the WHEN time periods who would otherwise have been referred to the ED by the telephone advice nurse but instead were referred to the TUC provider (Figure 1). Individuals with potential life-threatening complaints (e.g. new chest pain or shortness of breath, sudden stroke-like symptoms), major trauma or hemorrhage, and psychosis or homicidal ideation were excluded from TUC assessment and were advised to seek immediate emergency care. Nurses at the Clinical Contact Center are equipped with Triage Expert Dual Purpose (TEDP) software© (DSHI Systems) that uses a computerized triage algorithm that provides a structured workflow for >850 symptoms and injuries. 16 Questions within the algorithm guide the telephone advice nurse through a chief complaint-driven medical history with an evidence-based algorithm making disposition recommendations for the optimal time interval in which to be seen and recommended location of care (ED, UC, clinic, dentist, or home). Those who met the appropriate criteria were given the opportunity to be evaluated by an on-call TUC provider (physician or nurse practitioner). This provider could confirm or revise the disposition and/or decide the need to perform a video or telephone-based assessment. Individuals who declined to participate in a TUC assessment were advised to follow up in person to the recommended location based on the triage algorithm. Referral to the TUC program was non-random as this could only occur during the after-hours when the TUC service was staffed and only if the telephone advice nurse chose to present the case to the TUC provider.
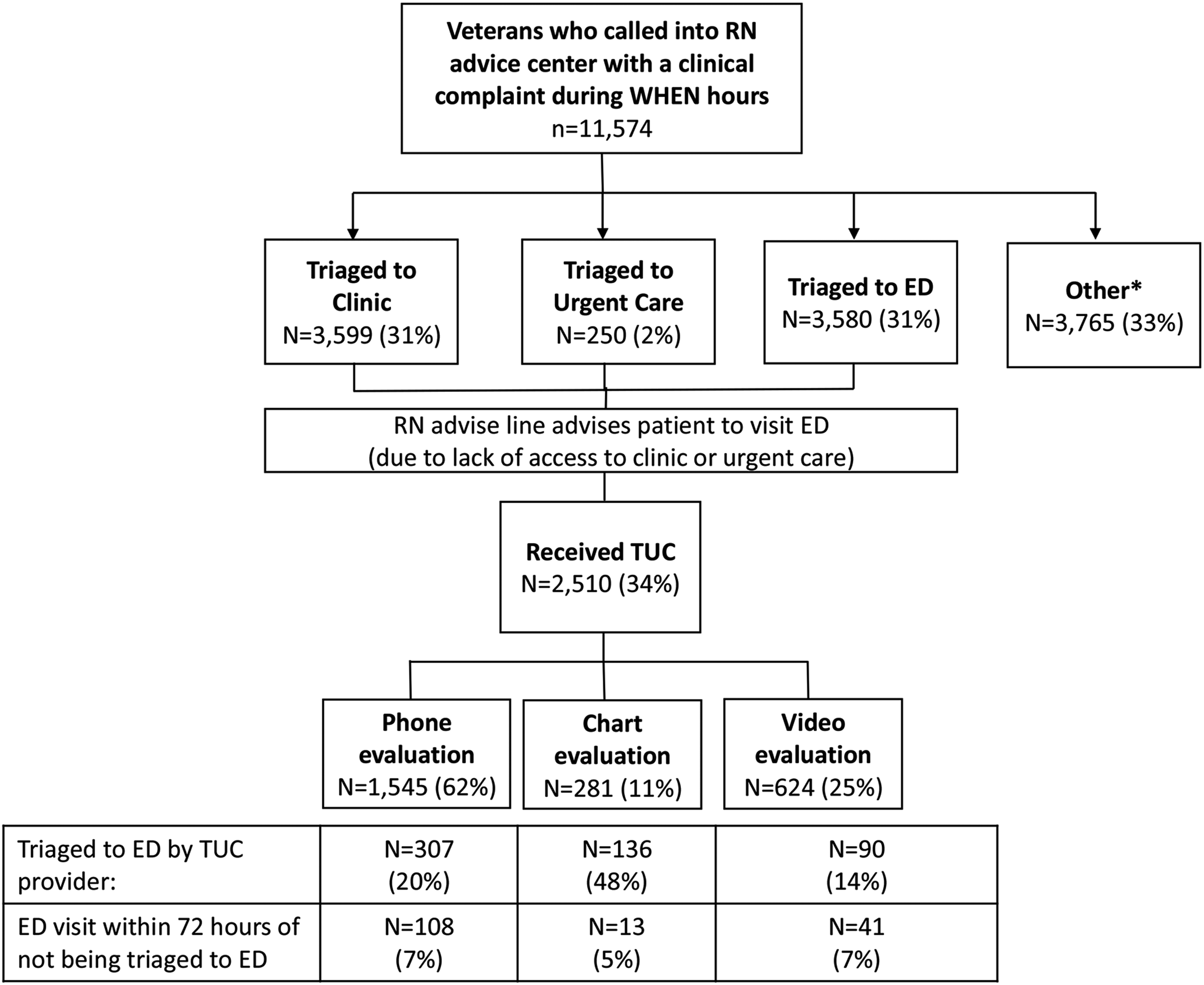
Flow diagram of tele-urgent care program.
Intervention
Individuals whose disposition recommendation was either ED, UC, or clinic appointment within a time frame that could not be met due to hours of operation (e.g. clinic appointment within 12 h on a Sunday morning) were offered TUC assessment. Note, prior to implementation, all individuals provided with these recommendations would be advised to be seen in the nearest ED. Communication between the telephone advice nurse and the TUC provider was done through instant messaging and an online tracking board. Providers utilized one of three assessment modalities: (a) video-based visits, (b) telephone-based visits, or (c) chart review. Providers were urged to use video visits whenever possible—which were performed using VA Video Connect—a video-based platform that allows providers to interact with patients through their mobile devices or computer. 17 If the individual consented to a video visit, the provider texted or emailed a weblink to a virtual medical room where the provider and patient could meet. Those who could not access a mobile device or computer, or who favored a telephone visit, were assessed through telephone evaluation. Chart review consisted of times in which information conveyed by the telephone advice nurse was sufficient to confirm or revise a disposition following chart review by the TUC provider.
Data sources
All data were obtained from the electronic medical records and the VA Corporate Data Warehouse–a national repository of electronic health records from visits to any VA facility. 18 Extracted data included patient demographics, chief complaint, the facility catchment area of each case, and the modality of interaction (video, telephone, or chart review only). Individuals who were missing these data (2.4%; n = 60) were excluded from analysis.
Analytic plan
We analyzed utilization patterns over a six-month period between April and September 2020. To assess whether the TUC was decreasing ED referral rates, we examined the proportion of cases that were referred to the ED following TUC evaluation during the six-month time period. To assess safety, we determined the proportion of callers who had a subsequent ED visit within 72-h of TUC evaluation when they were not referred by the TUC provider to the ED. Among these cases, we then performed individual chart review to assess: (a) if patients presented to the ED for the same reason as was stated for their TUC evaluation; (b) if subsequent hospitalization was needed during that ED visit; and (c) if death occurred during that hospitalization. This study was approved by the San Francisco VA institutional review board.
Results
During the six-month assessment, 11,574 individuals called into the RN advice line with a clinical symptom complaint during WHEN hours. Among the 2510 patients who were eligible and received TUC assessment, the average age was 63.3 (±16.7) years and most were male (87%, 2176). The most common chief complaints were musculoskeletal (21%), upper respiratory (15%), skin complaints (12%), or gastrointestinal (12%) in nature. Similar proportions existed among each modality, though video assessment was used more frequently for skin evaluations and had a younger average age than telephone or chart review assessment (Table 1).
Characteristics of individuals who received tele-urgent care assessment.
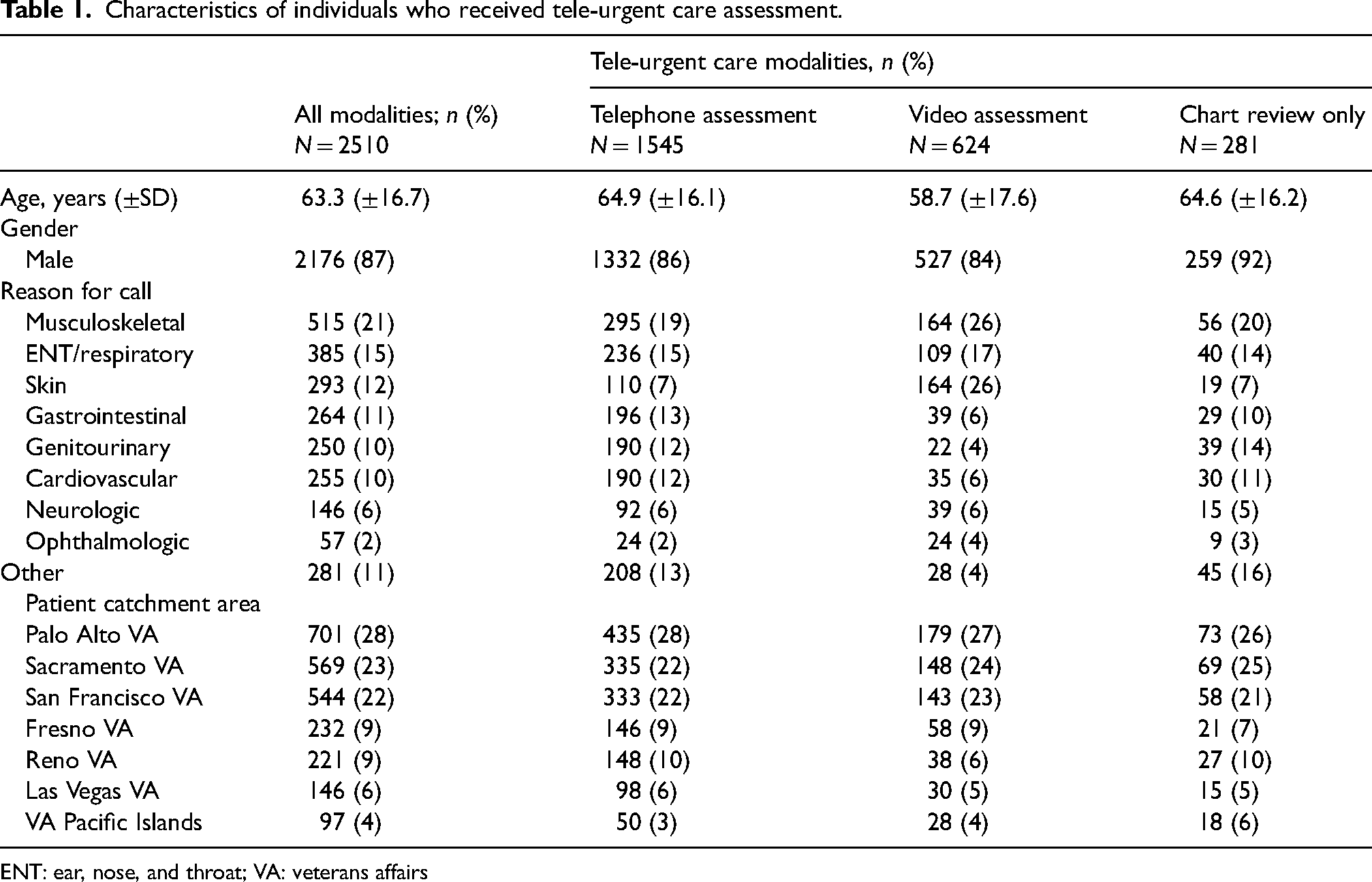
ENT: ear, nose, and throat; VA: veterans affairs
Among those who called with a clinical complaint, one-third (32%) were resolved to no further intervention (home), a dental clinic, or to future follow-up in a clinical setting. Approximately two-thirds of all calls were advised to be seen in a clinic (31%; n = 3599) or were triaged to the ED (31%; n = 3580), while a small number (2%; n = 250) were triaged to an UC. Among these combined 7429 individuals triaged to be seen by a medical provider, one-third (34%; n = 2510) received TUC assessment. Of these individuals, most were assessed through telephone evaluation (62%; n = 1545), followed by video evaluation (25%; n = 624) and chart review (11%; n = 281) (Figure 1).
In assessing ED referral rates, one in five individuals (21%; n = 533) who were seen by TUC required subsequent in-person ED assessment. Among the three assessment modalities, chart evaluation had the highest ED referral rate (48%; n = 136), followed by telephone (20%; n = 1545), and video evaluation (14%; n = 90). Among individuals who were not referred to the ED following TUC assessment, 1 in 10 (11%; n = 162) had a visit to the ED within 72-h of TUC assessment. Chart review revealed that among these individuals, most (91%) returned with the same or similar complaint as what was assessed during their TUC visit. Additionally, a chart review found that one in five of these individuals required hospitalization (19%, n = 31), with only one death (0.01%) that did not appear related to the admission method.
Discussion
In this assessment, we found that a multi-center, virtual tele-UC program appears to safely reduce non-emergent ED referral rates. Among the different virtual care modalities used, video-based assessment appeared to lead to the largest reduction in referrals, though was only used a quarter of the time. As hospitals and health care systems address ED overcrowding and overutilization, as well as the stresses of the COVID-19 pandemic, virtual care assessment and triage may be viable tools to decrease the unnecessary use of EDs—one of the most expensive resources in health care systems costs. While previous work has explored the use of telemedicine in the UC setting, most published studies are single-center in nature, recruit patients over short periods of time, and are not performed in an integrated health care system like the VA.11–14 This assessment highlights several important characteristics in the implementation of a multi-center TUC program.
First, our findings suggest that video visits may lead to fewer ED referral rates compared to all other modalities. While there are few studies that assess for potential differences between telephone and video-based virtual visits, our findings may support greater use of video-based assessment as a primary modality for virtual interaction. Our findings are consistent with prior work, which found that video-based care may be a superior assessment modality compared to telephone-based care—as previous studies have shown it to improve diagnostic accuracy and reduce readmissions rates compared to telephone-based care. 19 Second, our study demonstrates the safety of virtual TUC as a means of triaging non-emergent patients—as only 1 in 10 individuals who were assessed by TUC returned to the ED within 72-h, and only one in five of those required hospitalization. These findings are comparable to hospitalization rates in similar populations (e.g. adults >60 years) when patients are assessed in person. 20 While health care systems have found that virtual care can be an efficient, cost-effective way to deliver care, ensuring that it does not put patients at undue risk remains important. To date, there is limited high-quality evidence that virtual care does not harm patients or achieves the same or better clinical outcomes as traditional care. 21 These findings may suggest that TUC assessment for non-emergent settings does not place patients at higher risk of subsequent hospitalization than traditional, in-person care. We believe these findings should be validated in future studies that include larger samples and robust risk adjustment to account for the differences in the individuals who were evaluated by the different telemedicine modalities.
We note that while video was the preferred modality, only 25% of all TUC visits were completed through this method. This is consistent with previous research that finds telephone-based visits to be more common than video-based visits. 10 This may be occurring for a number of reasons including skepticism among patients and providers regarding the benefits of video-based care 22 and less complexity and fewer barriers with telephone-based care compared to video-based care—which requires a digital device with a camera and access to broadband internet. Additionally, although the VA had implemented virtual care prior to the pandemic, most video-based care was being provided by mental health providers, while there was little uptake among specialties who heavily rely on physical examination. 10 Finally, this may reflect providers’ choice in providing care over the telephone based on the clinical situation. We would highlight that the proportion of individuals who had a follow-up ED visit after either telephone or video-based TUC assessment were the same (7%), indicating that both modalities appear to offer similar quality of care.
Several challenges in implementation existed. Initially, proper staffing for the TUC was difficult as many providers had variable experience in acute medicine, UC, or ED triage. Due to these differences, there was noted variability in assessment and care provided to TUC patients in the early stages of implementation. To address this, providers with experience and knowledge with TUC provided one-on-one training to clinicians. While initially, this training was time-intensive, providers have since become more familiar and comfortable with TUC assessments and care. To further address this, weekly meetings were established to troubleshoot and address issues or barriers providers were experiencing. Additionally, technological issues (e.g. ability to use the VA’s video-based platform, connectivity, etc.) were pervasive in the early months of implementation; though, as the VA technological infrastructure was strengthened over the course of the pandemic, such issues have largely resolved.
Our assessment has limitations. First, our findings may lack generalizability outside the VA, which is a large integrated health care system that allows nationwide access to patient’s electronic medical records, potentially making virtual visits and triage easier for providers. Second, we were unable to assess whether patients visited a non-VA ED following TUC assessment; thus, our findings may underestimate the failure rate of TUC. Third, this was a non-randomized assessment that did not control for underlying factors that could predispose an individual for higher ED use—thus, unexplained confounding likely exists. Fourth, we did not assess population differences between those who experienced TUC and those who did not. Finally, this assessment was performed during the pandemic, when case-mix may have been different than non-pandemic periods, thus potentially affecting the efficacy of the intervention.
In conclusion, a telemedicine-based evaluation of non-emergent care appears to safely decrease ED referral rates in a large integrated health care system. Virtual-based platforms may offer an effective and safe mechanism to decrease ED overcrowding and should be investigated further. As hospitals and health care systems look to integrate virtual-care modalities into ED and UC settings, further work should focus on potential barriers to providing video-based care and the overall cost-effectiveness of such programs.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Dr Wray was supported by a Veterans Health Affairs Health Services, Research & Development Career Development Award (CDA 19-349-3).