
Abstract
Introduction
With a recent resurgence of the 2019 coronavirus disease (COVID-19) cases globally, an increasing number of healthcare systems are adopting telemedicine as an alternative method of healthcare delivery in a bid to decrease disease transmission. Continued care of orthopaedic patients in the outpatient setting during the coronavirus disease of 2019 era can prove challenging without a systematic workflow, adequate logistics, and careful patient selection for teleconsultation. The aim of this paper is to describe our single-centre experience with the application of telemedicine in our orthopaedic practice, and its effectiveness in maintaining outpatient follow-up of orthopaedic patients.
Methodology
We describe our centre's telemedicine model of care for orthopaedic patients on the outpatient follow-up – which includes workforce assembly, population health and target patients, logistics and communications, and overall workflow – with roles and responsibilities of involved people portrayed in detail.
Results
Feedback from both patients and orthopaedic surgeons reflected high satisfaction rates with care provided, noting minimal communication and clinical barriers compared to face-to-face consultations. Whilst not without limitations, our protocol allowed for rapid adoption of telemedicine in line with a national-wide initiative to digitize healthcare.
Discussion
The implementation of teleconsultation services at our orthopaedic centre has provided an effective method of healthcare delivery while enforcing social distancing measures – which proves vital in combating the spread of COVID-19 and ushering in a new normal.
Introduction
The outbreak of the coronavirus disease 2019 (COVID-19) pandemic has led to significant disruption in healthcare services across the world, with various organizations striving to develop systems with calculated risks of disease transmission via means of early detection, isolation, and intervention. While the advent of vaccinations and social distancing/isolation measures initially resulted in the gradual flattening of the incidence curve,1,2 several countries have reported a resurgence of COVID-19 cases3–5 – highlighting an urgent need to reinforce avoidance of unnecessary human exposure to prevent a second, or even third wave of disease. As such, various orthopaedic associations across the world (American Academy of Orthopedic Surgeons, British Orthopaedic Association, Australian Orthopaedic Association) have urgently advocated the use of telemedicine during the COVID-19 pandemic in a bid to prevent disease transmission without hindering the provision of services to orthopaedic patients.6–8
Telemedicine, defined as the delivery of healthcare services (i.e. diagnosis, treatment, disease prevention, research, education) from a remote location using telecommunication technology, has rapidly gained traction during the COVID-19 pandemic.9,10 With advancements in telecommunication technology and improving health literacy, employment of telemedicine has become more widespread – with various medical and surgical specialities reporting promising results from their telemedicine services.11–13 Due to the large proportion of patients who attend the orthopaedic outpatient clinic at our centre, the use of telemedicine to review repeat visit patients was paramount in maintaining social distancing and reducing overcrowding in outpatient clinics, thereby preventing disease transmission. Indirectly, telemedicine also granted better access to patients who were unable to attend face-to-face orthopaedic care for non-COVID-19 related reasons, namely inaccessibility of clinic location and time constraints.
In this paper, we describe our orthopaedic centre's telemedicine model of care which details a protocol and workflow to provide telemedicine services for orthopaedic patients across various subspecialties in the COVID-19 era. The aim of this paper is to encourage orthopaedic surgeons and services to implement telemedicine services during this pandemic.
Model of care
Guided by a nation-wide effort to improve population health literacy and digitalize healthcare, systematic adoption of telemedicine revolves around certain key elements to ensure satisfactory delivery of care to patients. Implementation of telemedicine at our centre entailed awareness of availability and limitations of logistics and communication capabilities, appreciation of people involved (members of workforce such as orthopaedic surgeons & IT support staff, patients and their carers) and their respective roles and responsibilities, and development of a standardized workflow for teleconsultation. Primary objectives of adoption of telemedicine by our centre included (1) seamless integration of telemedicine into routine care, (2) improving patient awareness of telemedicine, access to treatment services, and compliance towards functional recovery, (3) education and training of workforce in utilization of telemedicine, and (4) optimization of resources to overcome manpower and technological constraints.
Workforce
Developing a skilled workforce that is competent in the delivery of telemedicine is critical for ensuring optimal treatment of patients off-site. 14 The rapid adoption of telehealth across Singapore during this COVID-19 pandemic generated new demands for healthcare providers, support staff, and IT specialists to obtain the necessary skills to deliver teleconsultation services. 15 While telehealth is not a foreign concept to local practitioners, most orthopaedic surgeons and support staff were not trained to deliver telemedicine – thus necessitating the need for e-training. In March 2020, the Ministry of Health (MOH) Regulation Group introduced an online course and guidelines for doctors/dentists on designing and delivering telemedicine services, with a focus on prioritizing patient safety and welfare. Orthopaedic surgeons from our centre that underwent the above telemedicine course were taught specifics on clinical standards and outcomes, understanding human resources, organizational considerations, and technology and equipment relevant for telehealth support. Technical support and training were also provided to selected IT and support staff to facilitate the use of telemedicine, such as the use of Zoom videoconferencing, management of secure data and telecommunications equipment, and patient communication. The aforementioned accredited training schemes – designed to upskill healthcare providers and relevant staff – provide qualifications for recognized training in telemedicine delivery, ensuring a competent workforce that is confident in providing telemedicine support.
Population health and target patients
The rapid adoption of telemedicine and mobile-medicine rests heavily on improving population health awareness, and acceptance of telemedicine by both healthcare providers and patients alike. 16 With a consistently declining old-age support ratio, healthcare is made more proactive to guide patients in managing their well-being at a national level. 17 Promotion of healthcare services is done via a multifaceted approach: widespread adoption of telehealth is combined with the use of assistive technology and robotics in healthcare, advent of HealthHub – a digital portal for Singaporeans to access medical records and useful health information, and the Healthy 365 application which promotes healthier lifestyles.
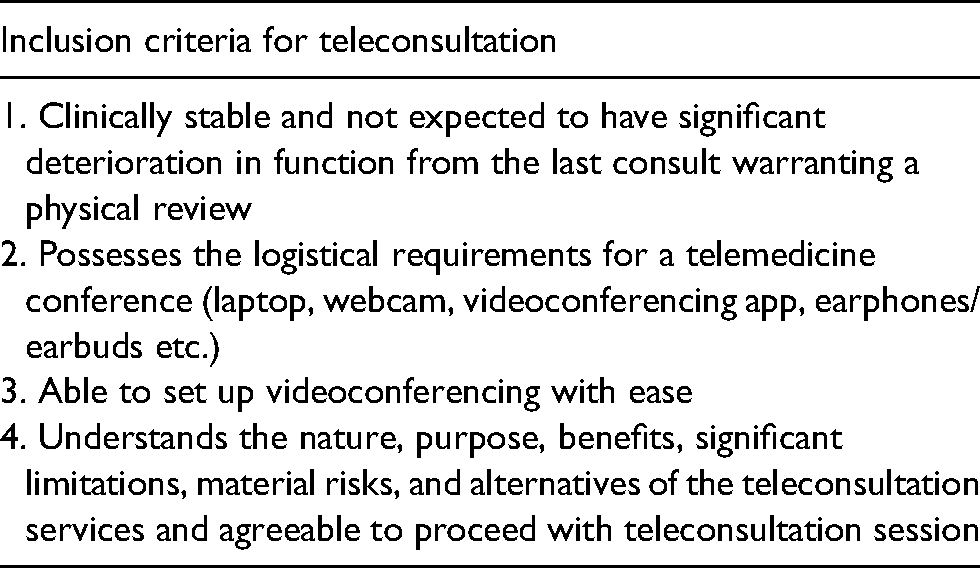
The adoption of telemedicine by our orthopaedic centre was met with challenges on patient selection. Certain limiting factors (from both patient and healthcare provider alike) resulted in a need for a careful selection criterion of patients suitable to attend teleconsultation appointments. Patients selected for teleconsultation were pre-determined in either (1) a physical consult prior to discharge as a hospital inpatient, (2) a physical consult during a prior outpatient review, or (3) via phone contact after their case has been reviewed by the attending surgeon and deemed suitable for teleconsultation. In our centre, clinically appropriate reasons for follow-up via teleconsultation included routine follow up (short/medium/long-term), interval review for post-operative follow-up, imaging review, and preoperative counselling. The inclusion criteria for teleconsultation at our centre are highlighted in Table 1.
Inclusion criteria for teleconsultation.
Logistics and communications
Ensuring a smooth teleconsultation rests on the secure sharing of patient data while ensuring personal data protection, involving meticulous logistical planning to facilitate better communication with the patient off-site (Online Appendix 1). Prior to the teleconsultation appointment, patients are notified by clinic staff on the necessary preparation to ensure appropriate set-up for the consult – including a mobile device/computer with adequate internet connection which can allow for videoconferencing via the Zoom meeting application, a room spacious enough to allow visualization of the patient in full, and brochure/video instructions on self-performed examination appropriate to the orthopaedic subspecialty.18–22 For the healthcare provider, videoconferencing was performed in a private clinic setting to ensure privacy. As Singapore's healthcare system has been internet separated since 2018 due to cybersecurity concerns, this necessitated the need for two platforms: A hospital-approved laptop with videoconferencing capabilities and an adequate internet connection, and a second platform that is internet separated (desktop computer) with electronic medical records. Both platforms are connected via HDMI cable and dongles to enable screen sharing of relevant radiological images and test results. Our surgeons utilized an electronic medical records system EPIC (Verona, Wisconsin) with secure access to the patient's biodata, medical history, relevant investigations (biochemistry/pathology results, imaging via PACS system), which also provided a platform to record patient information during teleconsultation sessions.
During teleconsultation, clinical aids were provided to the patient to better understand their clinical condition, namely the Visual Analogue Score chart, body diagrams, and plastic anatomical models. Relevant investigations such as imaging and laboratory results are shared with the patient via screen share with the use of annotation tools as appropriate. At the end of the teleconsultation session, e-medications, e-referrals, and follow-up appointments are ordered and dispatched accordingly. Medical certificates and reports are printed in PDF and password protected before they are emailed to the patient. If necessary, additional radiographic investigations could be ordered for patients to undergo prior to subsequent review. Educational materials were also sent to the patient via secure mail at the end of the session.
IT governance and security are provided by in-house support staff trained in the secure management of patient data and linked connections between healthcare providers and patients. Access to patient records is strictly limited to the healthcare provider, requiring secure login to the electronic patient records system under data monitoring.
Workflow
After the initial recruitment phase, patients are notified of the details of their teleconsultation session – including the timing of appointment and consultant in charge (Figure 1). The surgeon then proceeds to vet the patient's case, radiographic scans, and other relevant investigations at least 1 day prior to the teleconsultation session. The patient is also sent a reminder of their appointment timing with a video-URL link one day before by clinic staff. On the actual day of teleconsultation, a clinic room is prepared by support staff with relevant logistics as detailed above, with audio and video links established between surgeon and patient. The conduct of teleconsultation session then begins with confirming the identity of the patient via two patient identifiers (e.g. full name, identification number). Teleconsultation is then performed via starting with a brief on teleconsultation flow to the patient, obtaining subjective and objective information, assessment and impression, and finally execution of management plans. Clinical assessment was performed via virtual examinations relevant to the subspecialty.18–22 Investigations such as imaging and laboratory results are shown to the patient via the use of share-screen and annotation. Explanation of the patient's conditions/pathology is performed using the aforementioned clinical aids (Online Appendix 2).
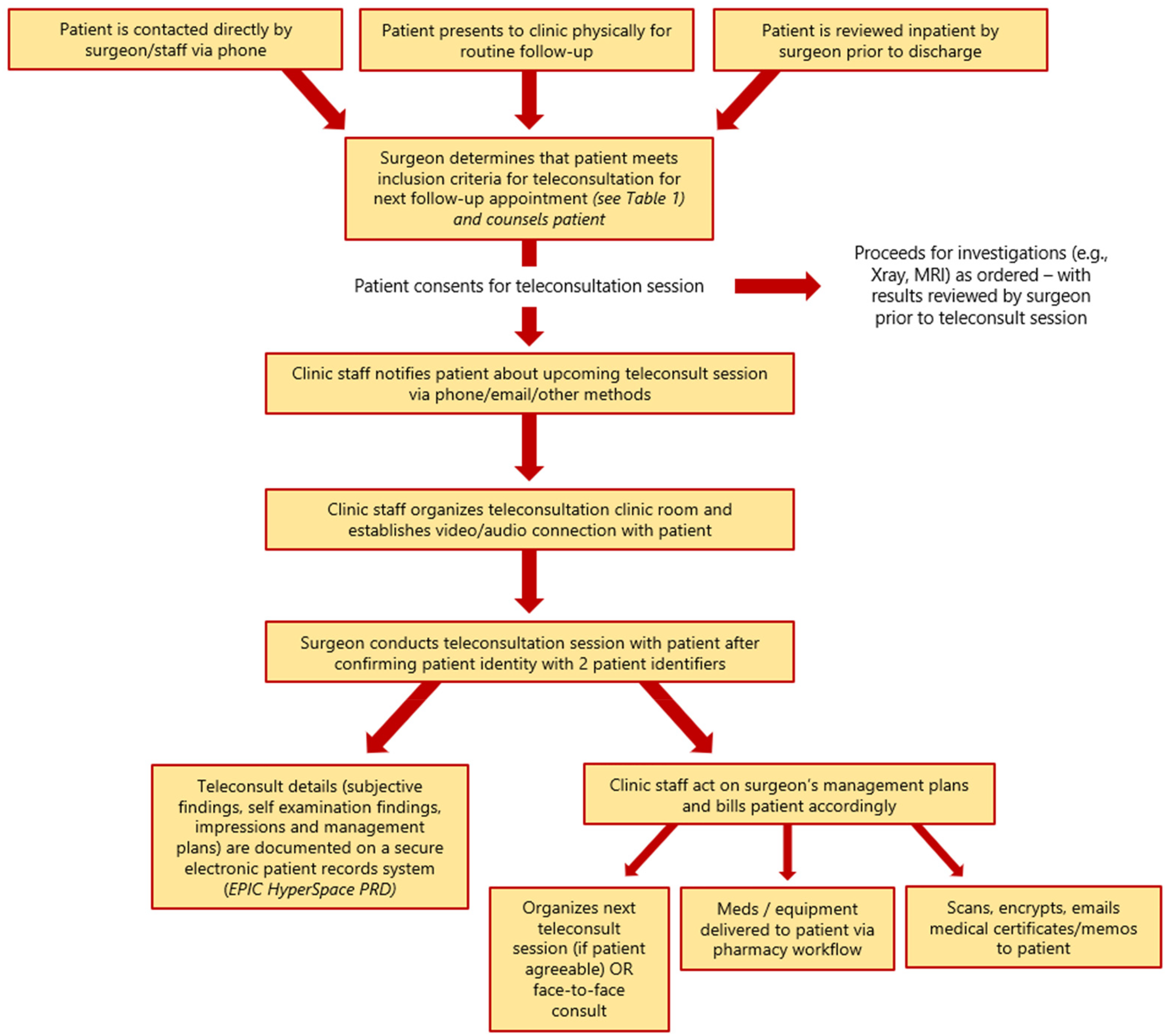
Orthopaedic surgery teleconsultation workflow.
Upon completion of the above, the clinic staff assists with the organization of the next teleconsultation session, delivery of medications or equipment to patient's location, and scanning – encrypting - emailing medical certificates and/or memos to the patient. Relevant investigations done after teleconsultation can be tracked by patients online via HealthHub. For patients who are deemed not to require to follow up by their orthopaedic surgeon, direct eReferrals are made to their primary healthcare provider of choice (family doctors/general practitioners) to ensure the continuation of care – with communication channels kept open should patients require re-referral back to their attending orthopaedic surgeon. Patients and surgeons who are agreeable are also sent electronic surveys after the appointment to obtain feedback on their telemedicine experience.
Results
A total of 364 patients (200 females) with a mean age of 56.4 years old attended orthopaedic teleconsultation sessions conducted by 23 orthopaedic surgeons across six subspecialties (hand, shoulder & elbow, spine, hip & knee, foot & ankle, general-orthopaedics) between July 2020 to April 2021. A list of patient diagnoses and reasons for follow-up via teleconsultation are included in Table 2. In all, 168 patients rejected teleconsultation services (Figure 2), with a vast majority citing a preference for physical consultations (n = 113). Of note, six patients rejected teleconsultation services due to security concerns of videoconferencing in their respective military bases. Over the 9 months, 127 patients initially planned for teleconsultation sessions had their sessions cancelled for reasons such as improvement in symptoms, inability to set up videoconferencing equipment, no-show, and doctor's request – the latter of which included reasons such as surgeon's request for physical consultation after vetting relevant investigations, or interval worsening of symptoms requiring a physician consult.
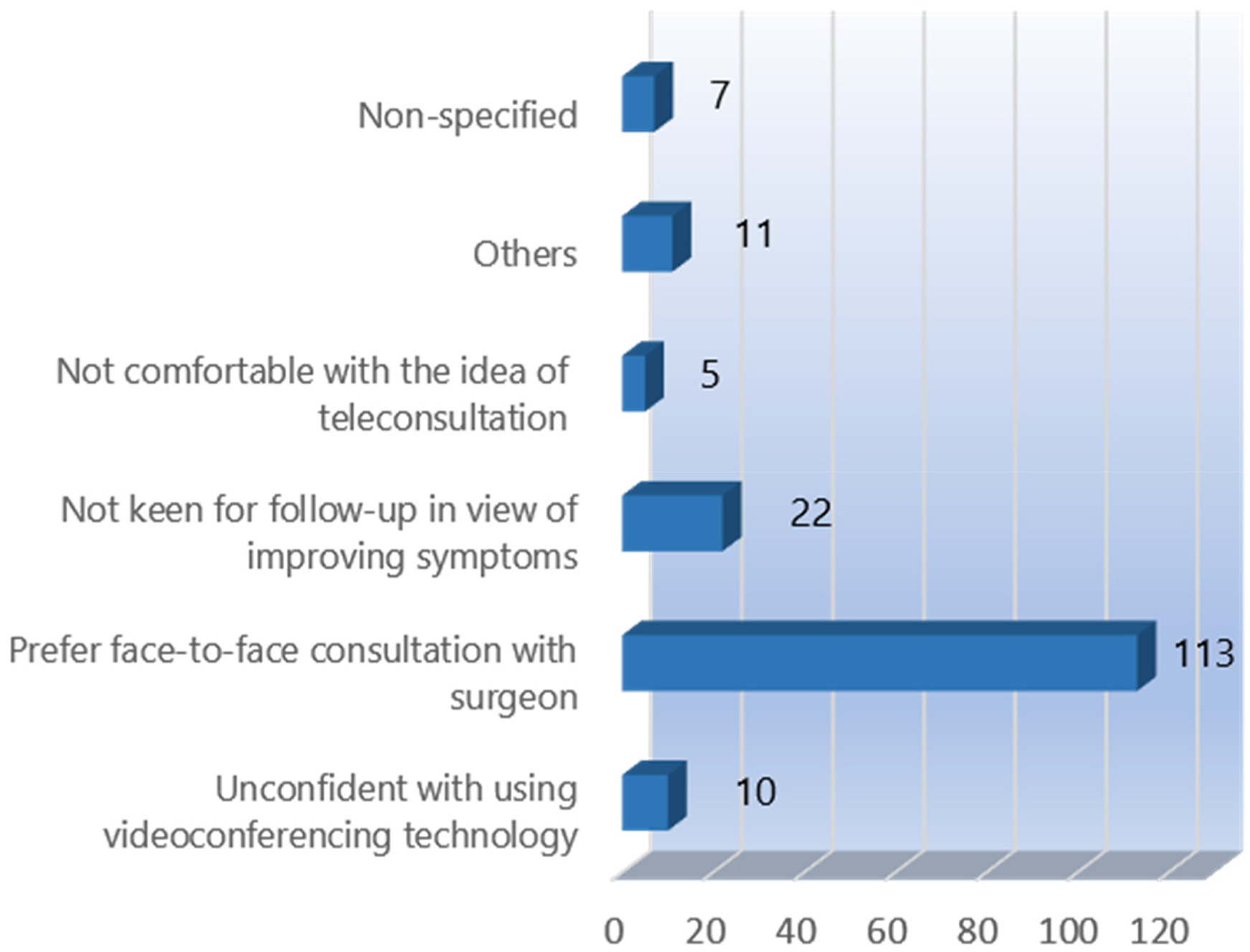
Reasons for rejection of telemedicine consultation.
Common key diagnoses and reasons for follow-up of patients who underwent teleconsultation.
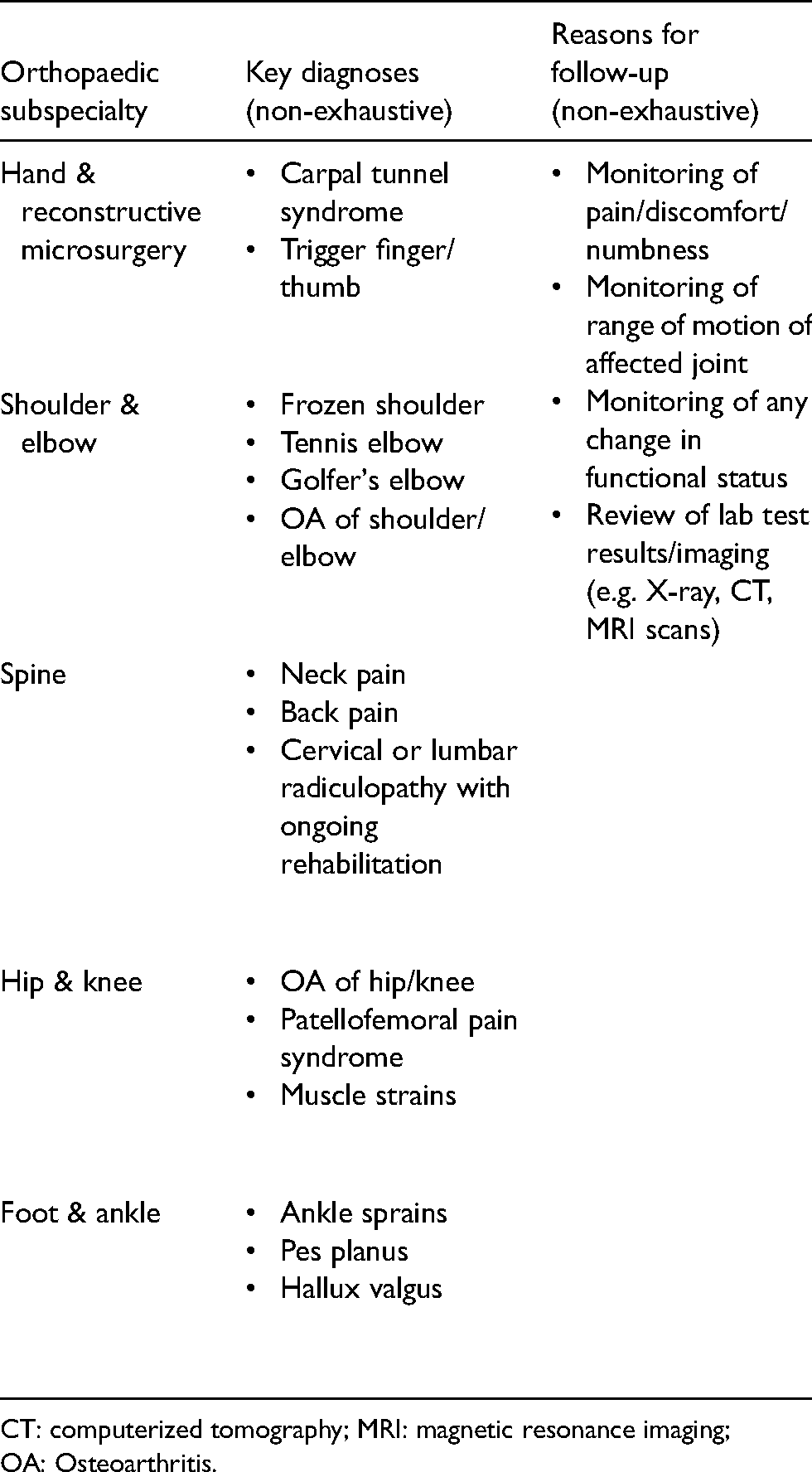
CT: computerized tomography; MRI: magnetic resonance imaging; OA: Osteoarthritis.
Discussion
With the recent resurgence in COVID-19 cases across various continents, healthcare institutions around the world are battling new strains of COVID-19 viruses by adopting improved workflows and restructuring organizations to mitigate the spread of infection.23,24 Advancements in network capabilities and population health awareness have led to adaptation to this new normal via the use of telemedicine, which has proven to be a viable method of communication between doctor and patient.6,7,13 Rapid adoption of telemedicine across various specialities and different countries have shown promising results, with reported high satisfaction rates reflecting its potential to provide quality care for patients whilst effectively decreasing outpatient work burden and minimization of disease transmission.25,26
Overall, teleconsultation services provided by our centre were well received by both patients and healthcare providers alike. Feedback suggests that telemedicine is an effective medium to follow-up with patients who meet our inclusion criteria, with a vast majority of patients reporting their teleconsultation experience to be similar to a face-to-face consultation. This was attributable to minimal disruption in patient-doctor communication, clinical assessment, and execution of treatment measures despite the patient being off-site – key domains evaluated in our study. Surgeons from the present study have reported minimal challenges in conducting the virtual physical examination safely – allowing for an adequate understanding of the patient's condition and rendering of appropriate treatment. In its infancy, telemedicine practitioners struggled with limitations of not being able to physically examine their patients, relying primarily on patients’ reported symptoms and visual inspection over videoconferencing to formulate their diagnoses.18,27,28 The advent of virtual examinations of different joints19–22 – which were reported to be effective and enabled clinical decision-making – has negotiated what was once a critical obstacle in clinical assessment.
Orthopaedic surgeons from our centre have highlighted that clinical assessment of their patients via teleconsultation was usually as effective as a face-to-face consultation – in part due to careful selection of stable patients with non-complex conditions. Patients with conditions expected to improve with a course of non-operative treatment (Table 2), or on routine review for abatement of symptoms, were found to be appropriate for teleconsultation provided they were clinically stable with no red flag signs/symptoms. Additionally, our surgeons also found that patients on follow-up for review of investigations (e.g. magnetic resonance imaging scans, histology results from excision biopsies, blood tests/bone mineral density scans etc.) in teleconsultation settings were largely similar to face-to-face appointments, with no hindrance to taking appropriate follow-up actions. In view of the above, the authors highly suggest consideration of the aforementioned groups of orthopaedic patients for teleconsultation over face-to-face appointments. Currently, our centre does not recommend teleconsultation follow-up for first visit patients or immediate post-operative patients, due to the importance of a physical consultation.
The benefits of telemedicine for populations facing difficulties in accessing healthcare have been long established in rural areas and developing countries across the globe.29–32 However, the adoption of telemedicine in cosmopolitan systems such as ours has also brought other advantages aside from mitigating the spread of infection. Patients who have personal or work commitments have given feedback that teleconsultation has helped them save travelling and waiting time while allowing them the comfort of having teleconsultation without physical barriers. Additionally, patients who have difficulties arranging for transportation to a hospital or are unable to leave their current environment have found teleconsultation to be a suitable alternative to a face-to-face consult – which may have been cancelled should there be a no-show. Streamlined workflows for delivery of medication/equipment/relevant correspondence to patients have allowed for a fuss-free method of rendering treatment off-site, with patients praising the avoidance of long waiting times at the pharmacy and minimisation of human contact. From the healthcare provider's point of view, a transition from face-to-face consultation to teleconsultation was a relatively smooth process, with specialists quickly adapting to the virtual physical examination and executing their management plans remotely. Should an urgent consult be required – teleconsultation can be rapidly set up in any room with a viable internet connection and necessary logistics.
Despite our centre's encouraging experience, teleconsultation is not without its shortcomings. The majority of patients who rejected teleconsultation services cited a preference for a face-to-face consult, highlighting perceived potential differences in social interaction/dynamics and rapport building between the two methods. 33 To mitigate this, the authors suggest surgeons/clinic staff to build rapport with the patient during the initial recruitment phase – in particular, explaining how the patient has met the inclusion criteria for teleconsultation, the teleconsultation procedure, and reassurance that telemedicine consultation does not result in a poorer standard of care compared to a face-to-face consult. In our single-centre experience, both patients and healthcare providers have cited technical issues in setting up teleconferencing equipment. However, these issues were often faced only during pilot consults, with subsequent teleconsultations experiencing less technical difficulty. The authors suggest that surgeons and clinic staff be proficient in the usage of teleconferencing hardware and software, with clear instructions given to patients on how to set up videoconferencing equipment so as to avoid technical difficulties during the consultation. With improvements in technological advancements and health awareness, even patients limited by their technology literacy may eventually be suitable candidates for teleconsultation.
Limitations
Despite telemedicine being limited in its application on certain patients, our single-centre experience has given us valuable insight into the challenges of telemedicine which are being addressed continuously. With an ever-increasing number of patients planned for orthopaedic teleconsultations sessions in the upcoming months, constant improvement to the telemedicine workflow will allow for better services to be provided to our patients. While teleconsultations may not be suitable for clinic first-visit patients due to the lack of physical examination and assessment of existing records/results, it significantly alleviates the outpatient burden given the large percentage of patients on follow-up.
Conclusion
Combating the resurgence of the COVID-19 infection necessitates augmentation of clinical practice to prevent transmission of disease. The use of telemedicine in our orthopaedic practice has shown effectiveness in the continuing clinical management of follow-up patients off-site while avoiding unnecessary human exposure. The authors hope that our positive experiences with telemedicine can encourage orthopaedic centres worldwide to adopt similar strategies in this new normal.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X211041011 - Supplemental material for Telemedicine use in orthopaedics: Experience during the COVID-19 pandemic
Supplemental material, sj-docx-1-jtt-10.1177_1357633X211041011 for Telemedicine use in orthopaedics: Experience during the COVID-19 pandemic by Brian Z Chin, Nazrul Nashi, Shuxun Lin, Kevin Yik, Gamaliel Tan and Fareed HY Kagda in Journal of Telemedicine and Telecare
Supplemental Material
sj-docx-2-jtt-10.1177_1357633X211041011 - Supplemental material for Telemedicine use in orthopaedics: Experience during the COVID-19 pandemic
Supplemental material, sj-docx-2-jtt-10.1177_1357633X211041011 for Telemedicine use in orthopaedics: Experience during the COVID-19 pandemic by Brian Z Chin, Nazrul Nashi, Shuxun Lin, Kevin Yik, Gamaliel Tan and Fareed HY Kagda in Journal of Telemedicine and Telecare
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.