
Abstract
Telehealth can effectively increase access to specialist care and reduce the need for travel. The Geri-Connect service was established in 2017 to support people living in residential aged care facilities in regional Victoria, Australia. Using the Model for the Assessment of Telemedicine, an evaluation of the Geri-Connect service identified service activity patterns and factors associated with uptake. Service activity from 2017 to 2020 and 10 semi-structured, key stakeholder interviews were captured and analysed. Between 2017 and 2020, video consultations were provided to 53 residential aged care facilities. Sustained growth (over 178%) and strong stakeholder acceptance highlight the effectiveness of this telegeriatric service. Four recommendations provide opportunities to further enhance service delivery including: implementation of an integrated health information system; systematic evaluation of service impact on stakeholders and residents, auditing and subsequent provision of targeted training; and regular auditing of software and hardware. Additionally, the need to augment fixed room hardware with mobile telehealth systems would increase access for residents with mobility problems. Dedicated personnel of the centralised team are best suited to implementing the recommendations. Whilst the provision of routine telehealth services into residential aged care facilities is challenging, the Geri-Connect service demonstrates that telehealth can be effectively provided to residential aged care facility residents needing specialist geriatric care.
Introduction
Pressures on health systems (e.g. COVID-19, ageing population, geographical spread) demand innovative approaches to meet the changing needs of the population. 1 Telehealth can deliver health services across distances via information technology increasing access to care for vulnerable populations.2,3
Telehealth has increased access to geriatric care for older adults where mobility problems and the need to travel precludes specialist support.3,4 An ageing population and growth in residential aged care 5 demands flexible access to geriatric care. 6 In Australia, residential aged care facilities (RACFs) are audited to promote safety and quality care. 5 The 2020 Australian Royal Commission into Aged Care Quality and Safety recommended increased use of telehealth in RACFs. 7 While commenting on the value of existing RACF telehealth services, it also highlighted the need to address service gaps wherein RACFs without telehealth should become telehealth capable.
Establishing a large scale telegeriatric service can be a substantial undertaking. Bendigo Health's Geri-Connect service is a successful geriatric medicine telehealth model, established in 2017, to improve equity and quality of care to aged care consumers across a regional district in Victoria, Australia. A clinical nurse coordinator works with general practitioners (GPs) and RACFs to triage residents for geriatric review. Video consultations between geriatricians and residents (supported by RACF staff and often including family) result in care management plans disseminated to the GP. At the time of publication, the Medicare-funded Geri-Connect service was offered into 58 RACFs. In 2020, an independent service evaluation reported on the implementation and ongoing delivery of the Geri-Connect service. The recommendations put forward aimed to support service optimisation and expansion. While some success factors will be outlined in this paper, to be of maximum use for a broader audience (i.e. similar health services), the paper focuses on a subset of the key recommendations aimed at service sustainability and expansion.
Method
The Model for the Assessment of Telemedicine (MAST), 8 a robust telehealth evaluation framework 9 guided the evaluation. Table 1 shows the MAST indicators and evaluation methods used in the full evaluation. Geri-Connect service activity data (from 2017 to 2020) were analysed to investigate the growth and reach of the service. Semi-structured interviews with key stakeholders provided staff perspectives on the utility and barriers. Ethics exemption (Ref: 2021/HE001698) was received from The University of Queensland human ethics department.
MAST indicators and evaluation methods.
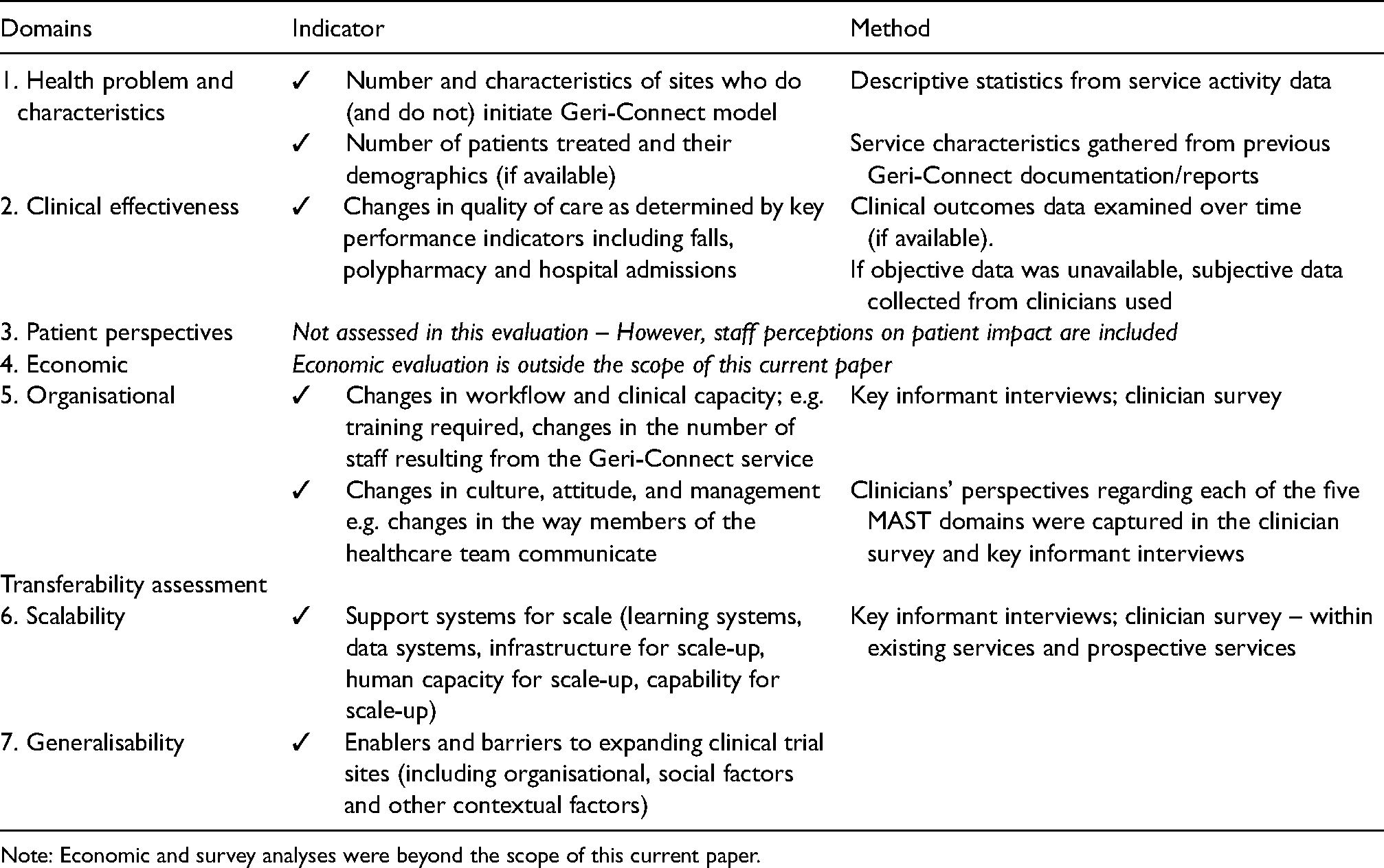
Note: Economic and survey analyses were beyond the scope of this current paper.
Quantitative – service activity data
Activity data collected by the telegeriatric service team as part of routine service delivery was obtained and analysed using descriptive statistics.
Qualitative – stakeholder interviews
Bendigo Health provided a list of staff involved with the service. The evaluation team reviewed the list and carried out purposive sampling to ensure the inclusion of services with both high and low adoption of telehealth. To ensure confidentiality, consenting interviewees’ names were known only to the independent evaluation team. Between July and November 2020, 10 phone interviews (ranging between 15 to 40 min; M = 24.7 min), were recorded, transcribed, deidentified and analysed. An inductive thematic analysis, as guided by Braun and Clarke, 10 generated themes. However, the broad MAST domains meant that most themes fit within the domains. Four peer debriefing sessions were held throughout the analysis between Authors HH and MT and a research assistant.
Results
Interview participant demographics
All interview participants were female, ranging between 31 to 66 years old (M = 49.2 years). Years of experience working with older adults ranged from 3 to 30 + years (M = 18.8 years). Staff interviewed ranged in experience in using the Geri-Connect service from eight months to four years (M = 2.5 years). Finally, the number of patients they supported to use Geri-Connect per month ranged between 1 and 4 (M = 3).
Overall results
The results presented in this paper align with three MAST domains: health problem and characteristics of the service; clinical effectiveness; and organisational impacts. Themes that did not fit within the domains were included in the original evaluation report but were more specific to internal Geri-Connect staff processes and procedures. Lacking generalisability, they have been excluded from this paper's results.
Domain 1 – service addressing the health problem
In 2015/2016 regional hospitals in the Bendigo Health district identified the need to increase access to geriatric medicine services for the region's older population. Between January 2017 and September 2020, a total of 1935 video consultations were carried out by a team of seven geriatricians and trainee registrars assessing over 1103 patients across 53 RACFs.
Staff interviews highlighted how Geri-Connect addresses a clinical need and is more efficient at times than in-person services. For instance, the inclusion of clinicians, patients, carers and GPs in the video consultations enabled more efficient communication and processes to support patient care: The information that we get from the geriatrician via Geri-Connect is information that we normally, that prior to that we would not have had access to. Unless the GP had put a referral in … and that's always been probably where the biggest gap has been you know trying to get the GP to make ongoing referrals, but now we can sort of bypass that, go straight through Geri-Connect who then put the referral letter and review straight to the GP with just the changes. BEN6
Domain 2 – clinical effectiveness and patient safety
Need for an integrated electronic reporting system
The initial aim to assess the clinical effectiveness of Geri-Connect by examining hospitalisation, falls and polypharmacy data could not be carried out. Unfortunately, variation in data collection between RACFs prevented examination of these clinical key performance indicators (KPIs).
Staff discussed the need for an integrated information management system to monitor KPIs across sites. Although, the Geri-Connect team collaborated with RACFs to establish smooth reporting and administration processes, system constraints often meant a reliance on different software systems and paper-based reporting. These were barriers to regular reporting. ‘Initially [the paperwork] was fairly daunting, but now we've got into some routine’. BEN9
Clinical effectiveness and safety
Staff provided numerous examples indicating the clinical effectiveness and safety of the Geri-Connect service. These fell under the categories of:
the multidisciplinary inter-service nature of the consultations; reduced polypharmacy as a result of regular clinical and medication reviews and; reduced patient transport to external clinical facilities or hospitals (clinical effectiveness, safety).
Patient-centred service
Consistently, staff described Geri-Connect as patient-centred because it:
is readily accepted by patients; allows representation of family members and patient advocacy within multidisciplinary discussions and; reduces the need for travel to clinical facilities (comfort and convenience).
Need for mobile telehealth units
During implementation, the Geri-Connect team collaborated with the RACF to assess technology requirements for effective video consultations. The Geri-Connect team emphasised the need for bedside telehealth consultations and, suggest mobile telehealth units. However, budget constraints meant that some RACFs predominantly had fixed room systems. Some RACF staff commented on the limitations of fixed room systems as barriers to service, especially for residents with mobility problems. Examples included: bariatric patients and patients who do not leave their rooms; and where mobility chairs are too wide to fit through doorways to the fixed system room. Finally, where space was limited, a clinician using the room prevented access to other staff. Hence, some staff advocated for mobile systems such as mobile video units or even handheld devices (e.g. tablet computers).
Domain 5 – organisational aspects
A growing service
As mentioned above, there has been sustained growth of the Geri-Connect service since its inception (see Figure 1 for the monthly figures). Full-year comparisons (between 2017 and 2019) show a 178% growth in the number of video consultations. The impact of service implementation and growth on workflow and staffing was highlighted in the interviews.
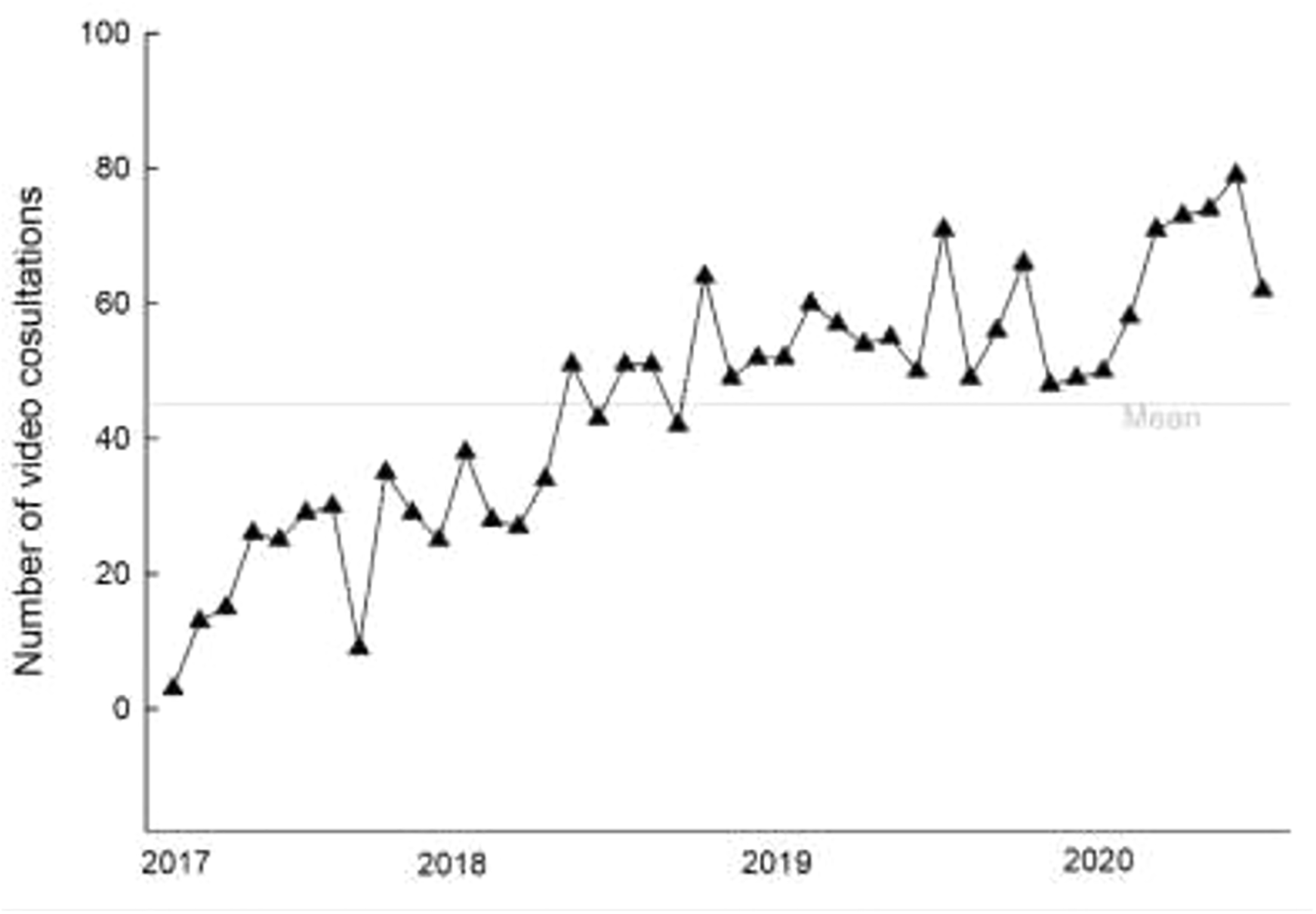
Monthly video consultations (January 2017 to September 2020).
Staff benefits
Overall, RACF staff reported that Geri-Connect held great value for them, with one staff member discussing a positive change in work culture as a result of the service. Specifically, staff emphasised the positive impact that Geri-Connect has had on the workforce as a result of:
upskilling; increased feelings of being listened to and appreciated and; increasing the meaningfulness and value of their work.
Need for audit of training requirements
Interviews also revealed varying levels of confidence, skill and readiness to adopt the service. There was substantial disparity in the amount of training that staff had undertaken and varying perceptions of how much training was needed. These results indicate the need to resource regular skills auditing and subsequent targeted training: The younger staff members seem to just pick it up in five seconds, the older ones are a bit hesitant … [Most now, since COVID-19] have worked out how to use telehealth BEN4 Maybe they need to talk to some of us that are using it to see if that helps. Put their fears aside. … there's nurses that are older than me, that this is really hard for them to get their head around. BEN1
Effective communication strategies
RACF staff expressed the need to improve communication processes (e.g. referral letters, medical information) between services, including GP clinics. Some staff noted inconsistencies in GP adoption of the service and variation in their communication responsiveness. Specifically, delays in the transfer of information impacted on RACF staff workload and influenced service effectiveness. Established communication guidelines and an integrated information management system could enhance communication: We have a couple of GPs that are amazing. They take on all the information. They implement just about 99% of the recommendations. … [Yet others] I see that they feel it as a challenge to their own level of expertise. And they just say, No, I'm not doing it. BEN1 Maybe the process of the getting the GP on board … Some doctors, of course, are very quick, some take a little bit longer depending if they’re, you know, coming into the service often. BEN8
Centralised management team
A small, central Geri-Connect team has collaborated with RACFs to drive service implementation and expansion. A dedicated central team is needed for service sustainability and continual improvement and therefore requires a continued funding base. Scheduling video consultations, the clinical nurse coordinator assesses technology and clinical staff availability. The availability of RACF staff has been a challenge and a common reason for delays in the consultation process.
Five RACF staff discussed the difficulty of finding someone who had capacity to coordinate Geri-Connect at a local level. In some RACFs ad-hoc systems of finding someone with capacity means that uptake success is reliant on the existence of telehealth champions. It is recommended that dedicated (and funded) RACF staff support the coordination of service delivery and monitor reporting at a local level: “Management has to support it or they've got to nominate someone to do it or whatever, a couple of, you need a couple of people really. We've got two people. We both sort it out.” BEN3
“I think that would definitely have to be the NUM or someone in a similar role, that wasn't needed on the floor … Yeah. I think you need that extra person to do it properly.” BEN10
Discussion
The current study highlights the successful uptake of a telehealth geriatric service that addresses the clinical needs of older adults in regional RACFs. Regardless of whether a service is in the initial stages of implementation or expanding (as with the Geri-Connect service), the recommendations put forward in this paper underpin a number of logistical factors to promote sustainability. Specifically, four recommendations were generated from an analysis of service activity and staff interviews.
Recommendation 1. Streamlined integrated information system
Several findings (e.g. incomplete data sets; need to enhance communication between services; recommendation to audit workflow impacts on staff and training) point to the need for an integrated multi-site information management system. Incomplete data sets are a common issue where human input is required. 11 Ideally the information system facilitates streamlined data reporting and is integrated within existing systems to incorporate: service activity, key performance measures, patient records, appointment scheduling, and staff training records. Such a system aims to overcome fragmented multiple (often paper-based) systems which may be labour intensive and not practically useful when planning service development. Evidence shows that when systems are easy to use and interoperable 1 there is potential improvement in quality and timeliness of data 12 and increased quality of care. 13 Such a system could support the remaining recommendations outlined below.
Recommendation 2. Effective feedback mechanisms and change management processes
This study shows that with increased activity there is a need to increase and change workflows which needs to be undertaken in consultation with stakeholders. In part the Geri-Connect service has been successful because of this consultation during implementation. It underpins the importance of regular auditing of workflows and staff feedback to determine the impact of implementation (or expansion) on service users. Regularly assessing the needs of service users (all stakeholders including staff) through routine feedback mechanisms allows targeted support of changed workflows to reduce burden. Auditing human resource demands enable a targeted approach to funding additional support where needed. Addressing changes in workflow and workload supports clinical outcome performance and may ultimately improve service sustainability. 1
The current study showed variation in service uptake and communication practices by GPs. Comprehensive stakeholder engagement in terms of routine needs assessment can address barriers and enablers to uptake. 2 Further, assessing the feasibility of standardised processes and workflows (including referral templates, record-keeping) may increase the efficiency of information transfer. Establishing standardised communication expectations can facilitate smooth service administration, efficiency of information sharing and reduce the burden on RACF staff. Previous research has demonstrated the need for effective communication strategies and systems to manage telehealth services as routine.2,14
Recommendation 3. Tailored training programme
A comprehensive audit of training needs can assess stakeholder confidence and skills using telehealth. Targeted regular upskilling in telehealth can address gaps in knowledge and confidence and promote consistent telehealth service delivery. 1 Regular training audits capture the needs of new staff training, reinforce skills if someone is an infrequent user, and allows updating of information (e.g. new technology) and processes. Training audits to support staff can improve service sustainability. To improve confidence in service, training should highlight service effectiveness (clinical, cost and time effectiveness). 1
Recommendation 4. Auditing of software and hardware
Appropriate technology when delivering telehealth services improves equitable access to health care. Routine auditing of the videoconferencing hardware and software systems within each facility should be undertaken to ensure clinical suitability. Residents of aged care facilities would benefit from mobile systems to improve ease of use for patients with mobility issues. 15 Technology audits should also be guided by usability and acceptability factors and consider evolving technology.15,16 For instance, opportunities to incorporate remote patient monitoring as well as video consultations can potentially enhance the quality of care and lead to more responsive patient management.
Sustaining and enhancing an effective service
Sustaining a telehealth service and further enhancement of service requires substantial investment. Staff interviews showed a preference for a larger centralised team to manage the service and dedicated funded personnel (champions) within the RACFs to coordinate Geri-Connect consultations. In collaboration with the RACF personnel, the centralised team would continue to focus on maintenance (existing sites with high activity), upscaling (existing sites with low to moderate activity); and expansion (new sites), considering the above recommendations. As previously mentioned, although these recommendations originated from the Geri-Connect service development and evaluation, they may be generalisable to other similar health services.
Limitations
The MAST recommends the evaluation of telehealth services across seven domains. A more comprehensive evaluation would incorporate patient perspectives and external stakeholder interviews (e.g. GPs). However, the current scope of the evaluation and limited engagement opportunities due to the COVID-19 pandemic precluded this data collection. More complete data could have provided further information on clinical effectiveness and service impact on workload and workflows. However, this limitation resulted in an important finding and subsequent recommendation that can support more effective data collection (i.e. the integrated electronic system).
Conclusion
The Geri-Connect service is a successful model of care considered by involved stakeholders to be effective and patient-centred. Its successful uptake highlights an innovative way to meet the demands of geriatric care in regional areas.
Footnotes
Acknowledgements
Thank you to all Bendigo Health and RACF staff who gave their time to participate in the evaluation.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Marc Budge and Ms Jacinta Probert who are employed by Bendigo Health were responsible for conceptualisation of the research, support with data collection and overall review of the manuscript. However, the evaluation and reporting of findings were performed independently by the authors from the University of Queensland.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Bendigo Health.