
Abstract
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has resulted in a widespread adoption of telehealth (phone and video consultations) in cancer care worldwide. The aim of this study was to determine patient satisfaction with telehealth consultations with their medical oncologist at a tertiary cancer centre in Sydney, Australia.
Methods
Patients who attended a routine telehealth appointment at the medical oncology outpatient clinic were recruited to complete a questionnaire containing 16 items, each on a 5-point Likert scale regarding satisfaction levels in various aspects of telehealth and their willingness to continue telehealth after the pandemic. Patients were also invited to provide suggestions for improvement.
Results
In total, 150 patients were invited to participate, and 103 valid questionnaires were returned. Median age was 63 years (range: 25–90), 49% of patients were male, 63% of patients had advanced cancer and 81% were on active treatment. In total, 95% of participants indicated that they were satisfied (score ≥4) with telehealth. 82% of participants preferred to continue telehealth consultations after the coronavirus disease 2019 pandemic, but ideally with a mix of telehealth and in-person consultations. Phone appointments (vs. video, p < 0.002), patients with advanced cancer (vs. early, p < 0.036) and pre-chemotherapy/immunotherapy/targeted therapy treatment reviews (vs. follow-up appointments, p < 0.001) were significantly associated with a willingness to continue telehealth.
Discussion
Patients were overwhelmingly satisfied with telehealth during the study period and were willing to continue telehealth for some appointments beyond the coronavirus disease 2019 pandemic. More research into the effectiveness, safety and implementation of telehealth to compliment traditional face-to-face services for patient-centred cancer care is required.
Introduction
Telehealth is defined as the delivery and facilitation of health and health-related services including medical care, provider and patient education, health information services, and self-care via telecommunications and digital communication technologies. 1 Uptake of this model of care in Australia has historically been in rural populations to facilitate access to specialists, reduce time and travel expenses for patients and allow access to multiple remote sites in one session. 2
The coronavirus disease 2019 (COVID-19) outbreak has officially declared a pandemic by the World Health Organisation on March 11, 2020. This has presented new challenges particularly in the management of cancer patients who are often immunosuppressed and are at a higher risk of developing complications including pneumonia, respiratory failure and even death. 3 The Australian government introduced a temporary telehealth scheme on March 30, 2020 to enable subsidised access to medical appointments conducted via telephone or videoconference to all patients regardless of location. To reduce the risk of exposure to the virus for both patients and doctors, there has been a rapid shift away from traditional face to face appointments and uptake of telehealth in the delivery of cancer care in both metropolitan and rural settings. 4 Telehealth has been widely adopted by physicians, and cancer societies worldwide have released guidelines in support of bolstering telemedicine services, reducing clinic visits and switching to subcutaneous or oral therapies where possible. 5
Delivering treatment using remote supervision and telehealth consultations has previously been shown to be a safe model of delivering quality care in rural cancer care settings, and recently there has also been a further expansion in utilising telehealth to conduct clinical trials through the implementation of the Australasian Teletrial Model.6–8
Patient satisfaction is also essential for telehealth to be a viable mode of service delivery. Satisfaction with healthcare is closely related to improved patient engagement and treatment compliance in a multitude of different clinical settings. 9 Several studies measuring patient acceptability with telehealth in cancer services have been conducted however almost all have been in rural settings. 10 To our knowledge, there has been limited evaluation of patient satisfaction for telehealth cancer services in medical oncology services delivered in the metropolitan setting, as this mode of delivery has traditionally not been subsidised. The aim of this study was to determine the proportion of patients who were satisfied to have their consultation with their medical oncologist conducted through video-conferencing or phone call, and the proportion of patients willing to continue telehealth after the COVID-19 pandemic.
Methods
Patients were recruited from the medical oncology outpatient clinic at Chris O’Brien Lifehouse in Sydney, Australia following routine clinical appointments. A paper-based questionnaire was provided after verbal consent. Inclusion criteria were patients aged ≥18 years old, proficient in reading English, diagnosed with early or advanced cancer and had a telehealth consultation (video or phone call) with their treating medical oncologist between 01/03/20 and 01/09/2020. Video consultations were conducted using Attend Anywhere®, a web-based video-conferencing tool. If the patient had phone or video consultation, they were sent a participant information sheet, a copy of the survey and a reply paid envelope in the mail. If the patient was recruited face to face (but the patient previously had a telehealth consultation), the participant information sheet and survey was provided at the time of the consultation.
Each questionnaire was individually coded to be re-identifiable for the purposes of linking survey responses to the electronic medical record to collect demographic, staging and treatment information, and results were de-identified for analysis. For appointment type, pre-treatment appointments were classified as those on active treatment including chemotherapy, immunotherapy or targeted therapy requiring regular monitoring of toxicities. Follow-up appointments were classified as those patients on active surveillance or endocrine therapy.
Questionnaires addressed (i) the type of consultation undertaken (video or phone), (ii) primary language spoken at home, (iii) time taken to travel to the hospital for a face to face consultation and (iv) 16 statements regarding satisfaction levels in various aspects of telehealth (Supplementary Material 1). Responses to each statement were recorded on a 5-point Likert scale with 5 indicating strong agreement and 1 indicating strong disagreement. Question 17 allowed for free text input regarding any aspects of telehealth consultations that patients felt could be improved.
The first 15 questions were adapted from a previous survey of patient satisfaction conducted by Sabesan et al. 11 in Townsville, Queensland for ease of comparing responses to a regional Australian setting, with hospital names and terminology changed as required, and questions that were not relevant to the metropolitan setting were removed. The final question was added in the context of the COVID-19 outbreak to assess whether patients were willing to consider telehealth consultations beyond the pandemic for some of their appointments.
This research was approved by the St Vincent's Health Network, St Vincent's Hospital Human Research Ethics Committee (2020/ETH01559).
Statistical analysis
Descriptive statistics were used to summarise patient characteristics and survey responses. Quantitative data was analysed using SPSS 25. For statistical analysis, this study took the responses and reduced the dimension of the ordered dependent variable to a binary variable (agree and strongly agree were classified as agreeing with the statement, and all other responses were classified as disagreeing with the statement). Pearson's chi-squared test was used to analyse results and p < 0.05 was considered statistically significant. Qualitative responses to the final question requesting feedback from patients was analysed using content analysis. The free text content was reviewed, a list of recurring themes was generated and the final coding framework was applied to data. Descriptive statistics were used to summarise the frequency of each code.
Results
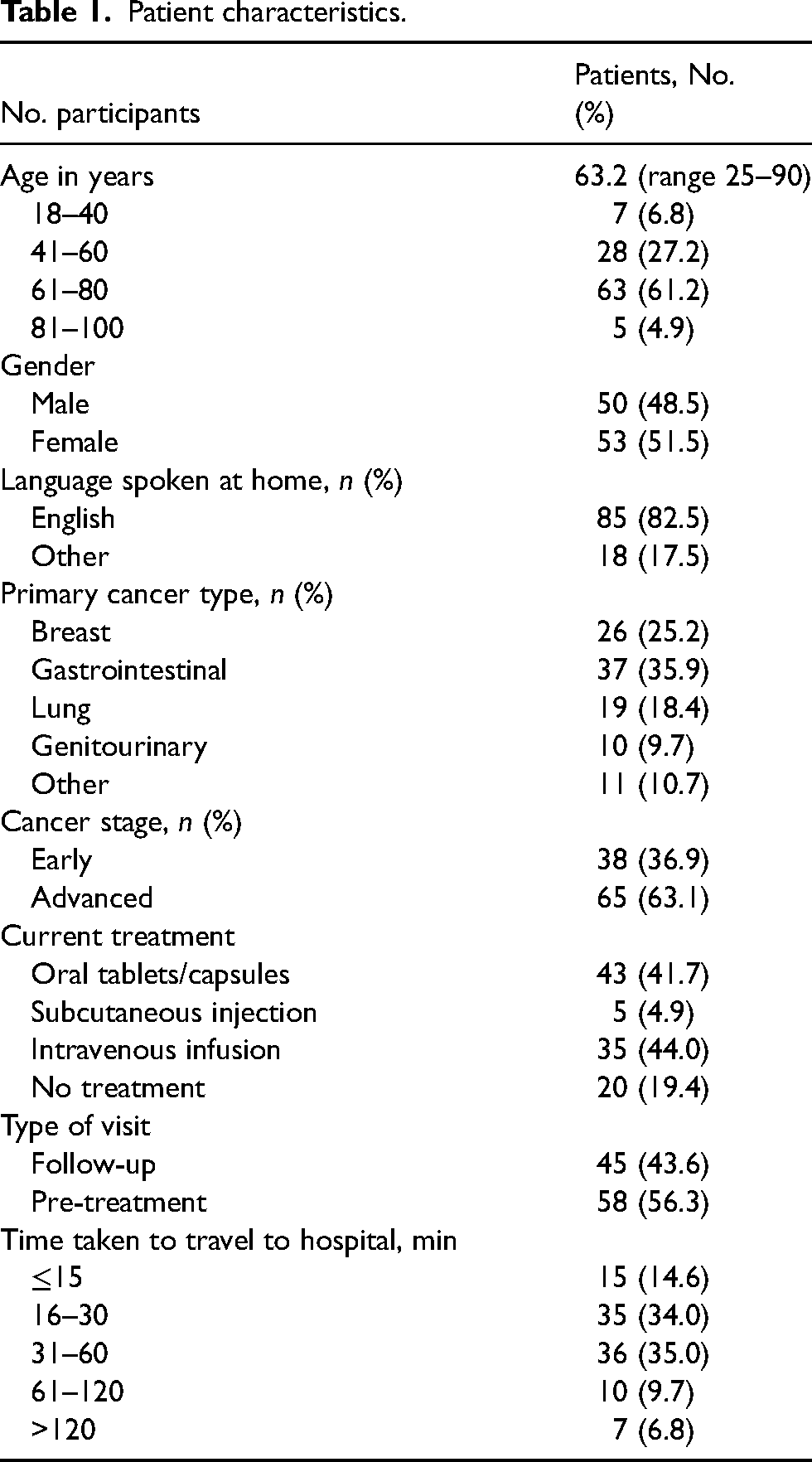
A total of 150 patients were invited to participate between March to September 2020, and 103 valid surveys were returned (response rate = 68.7%). Demographic details of the patients are summarised in Table 1. The majority of patients spoke English as their primary language. Patients’ responses to the questionnaire statements are shown in Figure 1. In total, 95.1% of participants indicated that they were satisfied with their video or phone consultation. Except for question 9, the majority of responses to questions were in agreement or strong agreement with the score of 4 or more on the Likert scale. For question 9, 49% of patients indicated that they felt it was important for the specialist to perform a physical examination. In question 10, 68% of patients indicated that they preferred to have another phone or video consultation rather than travel to hospital. In Question 16, 82.3% of patients indicated that they would consider continuing phone/video consultations after the COVID-19 pandemic if this was an option for some of their appointments. Patient responses to suggestions for improvement are shown in Table 2.
Patient characteristics.
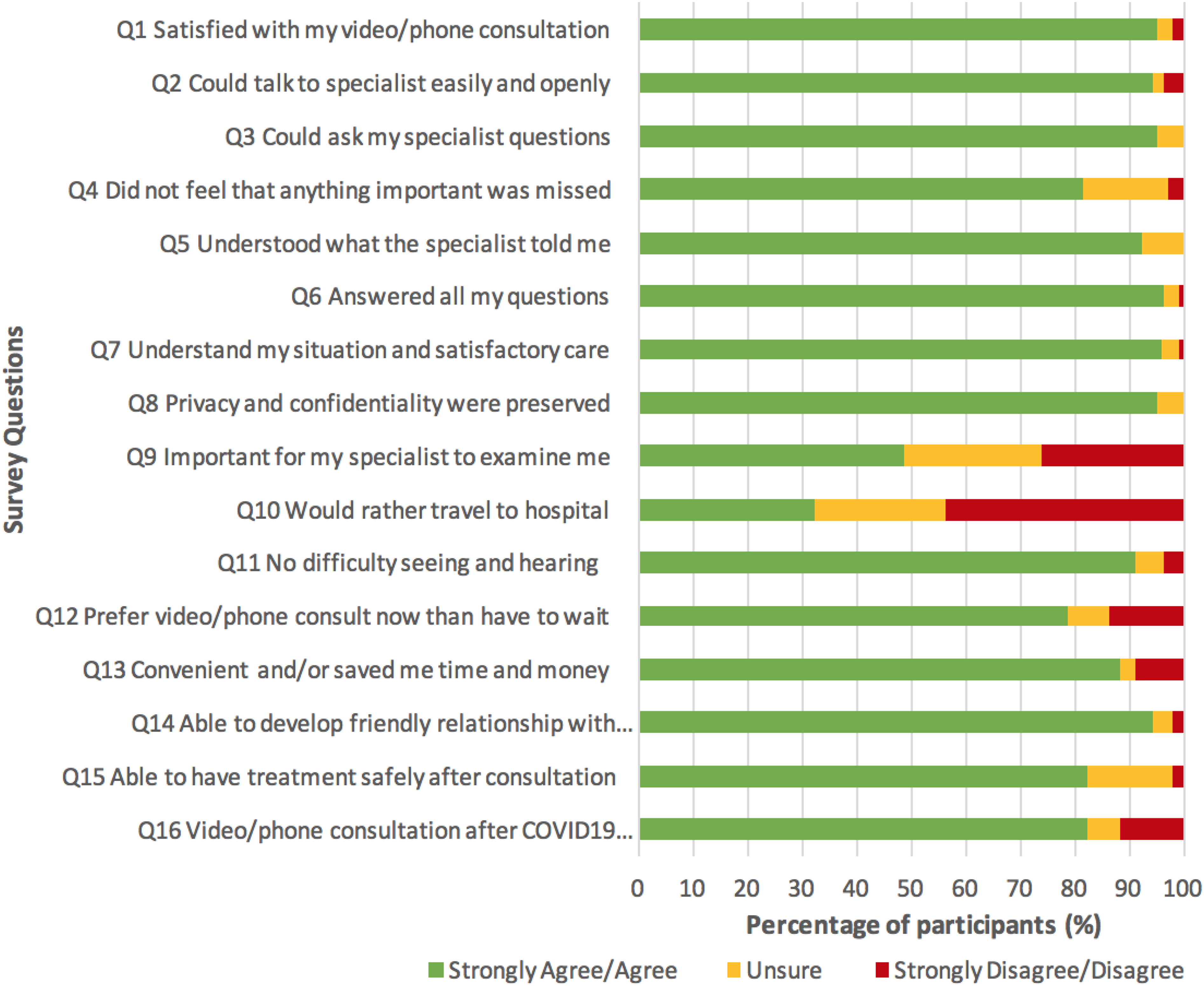
Response to satisfaction statements by participants.
Single factor Chi-squared analysis of patient willingness to continue telehealth post-pandemic.
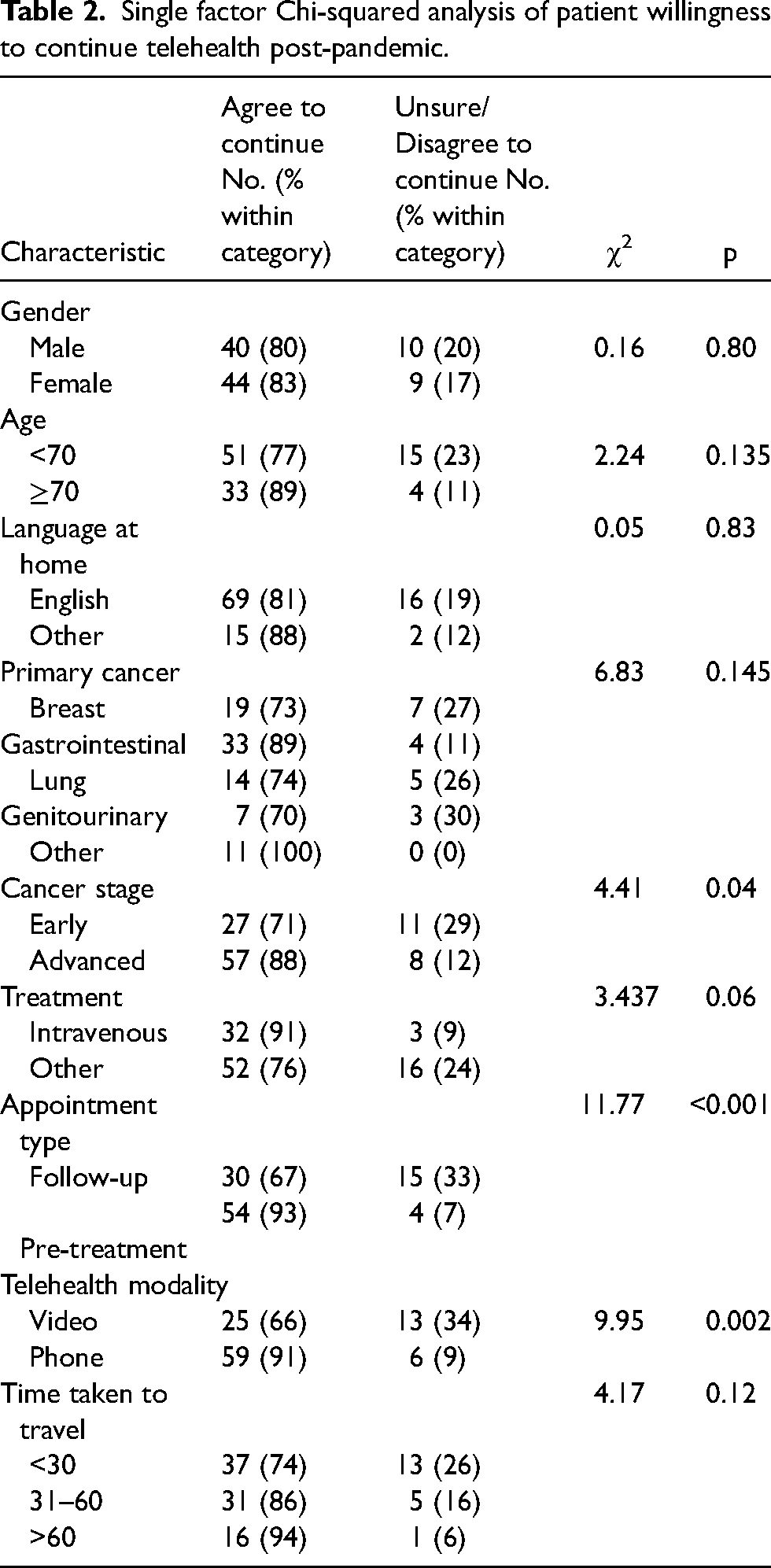
Analysis of patient willingness to continue telehealth beyond COVID-19
To explore the factors affecting patient willingness to continue telehealth beyond the COVID-19 pandemic, patient characteristics were included in the analysis as independent variables against agreement to Question 16 (Table 3). The results showed phone appointments (vs. video, p < 0.002), patients with advanced cancer (vs. early, p < 0.036) and pre-chemotherapy/immunotherapy/targeted therapy reviews (vs. follow-up appointment not requiring active monitoring of toxicities, p < 0.001) were significantly associated with a willingness to continue telehealth after the pandemic.
Descriptions of suggestions for improvement were provided by 43 respondents, with the frequency of overarching themes and sub-themes with example quotes a .
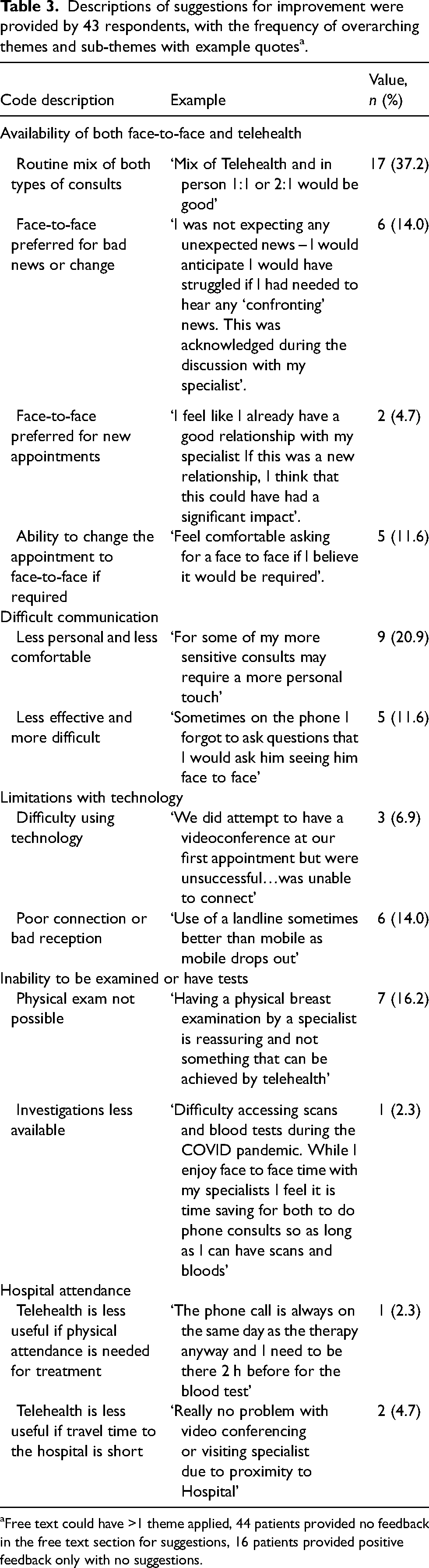
Free text could have >1 theme applied, 44 patients provided no feedback in the free text section for suggestions, 16 patients provided positive feedback only with no suggestions.
Discussion
There has been a rapid adoption of telehealth across all health services internationally, as part of the emergency response to the COVID-19 pandemic. 12 The expansion of telehealth in routine cancer care has allowed medical oncology consultations to continue during the pandemic allowing patients access to treatment but reducing their potential exposure to infection and oncologists to maintain involvement regardless of their physical location. Whilst telehealth consultations were formally supported with broad funding arrangements through the Australian Medicare Benefits Schedule in 2011, overall telehealth uptake has been slower than expected. 13 The COVID-19 pandemic has resulted in a heightened awareness of telehealth among clinicians, patients, and society overall, although further work is required to ensure sustainability in both metropolitan and rural settings beyond the pandemic. 14
Patient satisfaction with a telehealth supported model of care at a rural centre by Sabesan et al. 11 and our study has demonstrated similar results in the metropolitan setting. Survey results indicated that almost all patients were satisfied with their telehealth consultations during the study period, felt comfortable during their consultation and that most patients were willing to continue telehealth beyond the COVID-19 pandemic for some of their appointments. Those with advanced cancer were more willing to undergo telehealth beyond the COVID-19 pandemic. This may be due to the reduced travel required that can be difficult for those with symptoms of advanced cancer and less interruption to personal and family life, as well as a burden on caregivers. Caregiver satisfaction was not directly examined in this study, however it is well known that caregivers are regularly involved in consultations and decision-making in cancer care. 15 Increased patient satisfaction with telehealth may be related to reduced dependence on caregivers for transport, particularly when travel may be difficult for those symptomatic with advanced cancer. 16 Furthermore, telehealth can facilitate triadic involvement of caregivers in the consultation, that should be actively encouraged even if they are unable to travel to attend the appointment with the patient.
Those patients undergoing pre-treatment reviews were more willing to continue telehealth and this may be due to more appointments and regular contact with their medical oncologist, compared to those on active surveillance or endocrine therapy who typically have fewer appointments and only have a routine appointment once or twice a year.
Interestingly, patients undergoing phone appointments were more willing to continue telehealth than those undergoing videoconferencing. This may be due to technical difficulties with the videoconferencing technology with an impact on communication that can arise if sound or vision quality is poor due to internet connectivity and lack of bandwidth. Lack of infrastructure, information technology resources and organisational support have been identified as key barriers to overcome going forward for scaled implementation of telehealth via video consultations. 17
Most patients felt that they saved time and/or money with their telehealth consultation, however, longer time taken to travel to appointments was not significantly associated with a willingness to continue telehealth beyond the pandemic. Similarly, there was no difference between those patients who were required to travel to the hospital to have the intravenous treatment and those patients on no treatment or treatment via alternative routes of administration (such as oral tablets), who could potentially have treatment in the community without a visit to hospital.
The perceived need for a physical examination continues to be a concern for some patients, with almost half of the surveyed patients reporting that they feel a physical examination by the specialist is important. This concern is consistent with the Townsville study that reported 76% of patients proposing that an examination is a necessary part of the consultation. 11 Most patients felt that treatment could be safely delivered after their telehealth appointment. The safety aspect of delivering chemotherapy via remote supervision has been previously demonstrated in the regional setting with chemotherapy being delivered without compromising safety. 6 Telehealth has been shown to be safe, and equivalent or at times, more clinically effective than usual care in certain contexts and specialities, however more studies are required specifically in the cancer care setting.18,19
Not all consultations may be ideal for telehealth and the most common theme for suggestions provided by patients in our study was to have both telehealth and face-to-face appointments available. Clinicians have also suggested this previously, acknowledging that telehealth does not need to be used exclusively, but rather as an adjunct to usual modes of care delivery. 17 Even in the metropolitan setting, when face to face attendance to a cancer centre is not feasible for the patient, this could be overcome by collaborating with local health professional. Consultations that may not be ideal for telehealth include new consultations when a patient is not known to their specialist, when difficult news is being delivered or when patients are acutely unwell and require immediate intervention.
A limitation to this study includes the recruitment period, which was during the time Sydney was experiencing COVID-19 outbreaks when satisfaction with telehealth may have been higher than normal due to patient concerns regarding infection risk. Most patients spoke English at home and the use of telehealth with interpreters for those from culturally and linguistically diverse backgrounds needs to be further explored. Furthermore, all patients surveyed were follow-up or pre-treatment appointments, were often on established treatment plans, and had previously seen their oncologist in person and established some rapport.
Conclusion
Our survey indicated that metropolitan patients were overwhelmingly satisfied with telehealth during the study period and were willing to continue telehealth beyond the COVID-19 pandemic in certain situations and particularly for pre-treatment reviews. Although telehealth is not appropriate for all patients or all types of consultations, as we move out of the pandemic more research into the effectiveness, safety and implementation of telehealth to compliment traditional face-to-face services for patient-centred cancer care is required.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This research was approved by the St Vincent's Health Network, St Vincent's Hospital Human Research Ethics Committee (2020/ETH01559).