
Abstract
Introduction
Group engagement is an important component of video-based telehealth interventions, yet this construct remains understudied. In the present study, we applied a multidimensional conceptualization of group engagement in two video-based telehealth interventions that either aimed to reduce fear of hypoglycemia or diabetes distress in parents of children with type 1 diabetes. We examined variability in group engagement across parents and assessed the relationship between parents’ level of group engagement and their treatment outcomes.
Methods
Twenty-nine parents participated in one of two manualized, closed-group, telehealth interventions and completed outcome measures pre- and post-treatment. We behaviorally coded telehealth sessions based on six dimensions of group engagement using the Group Engagement Measure (inter-rater reliability = 0.94). We examined correlations between group engagement dimensions, parent psychosocial well-being, and child hemoglobin A1c. Further, we examined independent sample t-tests to assess differences between treatment groups.
Results
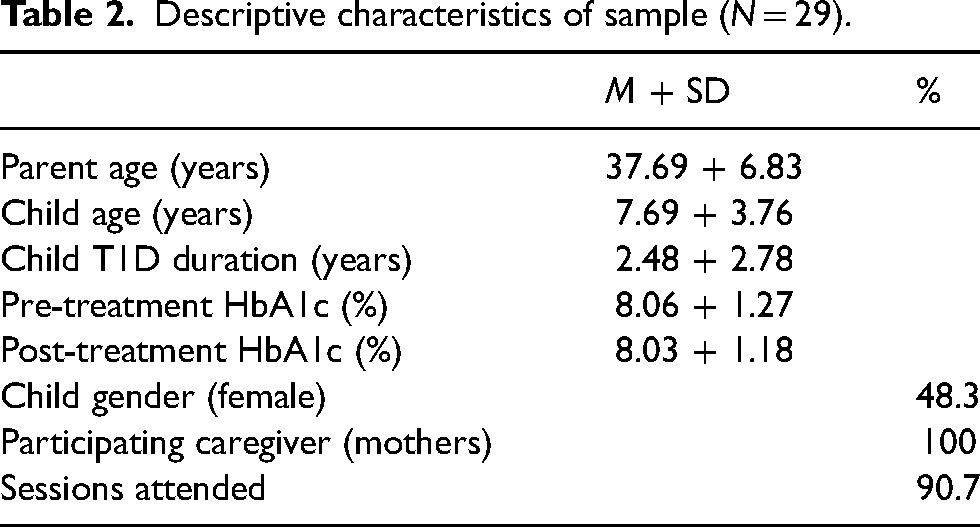
Mean parent age was 37.69 ± 6.83 years, mean child age was 7.69 ± 3.76 years, and mean child hemoglobin A1c was 8.06 ± 1.27% (41.4% had a hemoglobin A1c <7.5%). Parents who spent more time attending to other group member's issues, reported lower hypoglycemia fear at post-treatment, and parents who showed more active support of the group leader's purpose/goals during the session also reported fewer depressive symptoms at post-treatment.
Discussion
We identify several dimensions of group engagement that are associate with improved parent psychosocial and child hemoglobin A1c outcomes. Intervention designs that use group engagement to guide treatment planning or inform treatment-related decisions in video-based telehealth interventions could help families achieve more optimal treatment outcomes.
Introduction
Group engagement is an important, but potentially understudied, component of success for group-based interventions. Group engagement reflects a multidimensional construct that includes participants’ session attendance, relationships with other group members, therapeutic alliance with the group leader, and effort applied to addressing their presenting issues.1–3 Indeed, in support of this multidimensional characterization of group engagement, previous studies have found a link between group members’ sense of belonging and their attendance at group sessions. 4 Further, there is evidence that participants’ perceptions of the group dynamic affect the probability they will attend future sessions, particularly if they feel their level of group engagement is commensurate with the group. 5 While researchers have applied a multidimensional measurement of group engagement to interventions delivered within in-person settings, to our knowledge no study has yet attempted this for interventions delivered via telehealth in children with diabetes. This represents an important gap in the literature that needs to be solved; applying a multidimensional measurement of group engagement to telehealth-delivered interventions could uncover new evidence supporting the roles session attendance, group dynamics, and therapeutic alliance also play in promoting the success of telehealth-delivered interventions.
To begin to fill this gap, the present study seeks to measure and evaluate group engagement in two telehealth-based interventions our team developed for parents and caregivers of children with type 1 diabetes (T1D). Parents and caregivers of children with T1D report difficulties with adequate social support and experience high levels of stress, which is associate with increased symptoms of depression and anxiety.6–9 Parents may also report moderate to high levels of diabetes distress and fear of hypoglycemia,10–12 which may negatively impact their quality of life13,14 and their child's glycemic levels. 15 To address parents’ hypoglycemia fear, our research group developed the Reducing Emotional Distress to Childhood Hypoglycemia in Parents (REDCHiP) intervention. REDCHiP is a manualized, closed-group, telehealth intervention that uses principles of Cognitive Behavioral Therapy (CBT) to reduce parents’ fear and use of maladaptive avoidance behaviors and increase their use of adaptive coping strategies. In addition, during REDCHiP sessions, parents review T1D education, learn age-appropriate behavioral parenting strategies, and learn how to problem-solve challenges with T1D management. 16 The REDCHiP intervention takes 13 weeks to complete and delivers the treatment content via a combination of seven groups and three individual sessions. In a previous report, our research group found preliminary evidence supporting REDCHiP's efficacy for reducing parents’ hypoglycemia fear both after treatment and at a three-month follow-up assessment. 17
To address parents’ feelings of diabetes distress, our research team developed the Cognitive Adaptations to Reduce Emotional Stress (CARES) intervention. CARES is a manualized, closed-group, telehealth intervention designed for parents of school-aged children with T1D. The CARES intervention includes 8 or 12 weekly group sessions and uses principles from CBT and mindfulness to teach parents how to identify unhelpful thoughts, feelings, and behaviors specific to T1D. Parents also learn to use behavioral activation to manage their negative thoughts and feelings related to T1D. Our preliminary results suggest CARES can help parents to achieve significant reductions in their feelings of diabetes distress. 18
Specifically, in the present study, we tested the hypothesis that we would find support for applying a multidimensional conceptualization of group engagement in a telehealth setting (i.e. we would see the variation in parents’ dimensions of group engagement) and that we would find associations between parents’ level of group engagement and their treatment outcomes.
Methods
Study design
Although we include data originating from two interventional studies, the present study uses an observational design.17,18 It is important to note that neither intervention included an intentional manipulation of group engagement and one of our goals in the present study is to examine how group engagement relates to the self-report measures we collected as part of testing these interventions within a telehealth context.
Participants
For the original pilot projects, we recruited parents and caregivers of children with T1D from an endocrinology department at a large pediatric hospital system in the Midwest United States. Eligibility criteria included parents who were English speaking and had a child who (1) was between the ages of 1 and 12 years, (2) had a confirmed diagnosis of T1D for greater than 6 months, and (3) was prescribed intensive insulin therapy using multiple daily injections or continuous subcutaneous insulin infusion.
Procedures
The local Institutional Review Board approved all procedures before family enrollment to either treatment group. Parents provided written informed consent for their own participation, as well as consent for their child. Before either treatment group began, parents completed several measures on a tablet during their pre-treatment study visit and their child provided a finger-prick blood sample to measure hemoglobin A1c (HbA1c). Families repeated these procedures after their treatment group ended. Parents either participated in a pilot trial of REDCHiP or CARES and group leaders were masters-level graduate students enrolled in a doctoral clinical psychology program. If a parent did not attend a treatment session the group leader scheduled a make-up session with the individual participant to ensure they were exposed to the same intervention content as the other participants. Group members joined the telehealth session from their residence and the group leaders join from their office.
As part of the intervention trials, we set up the telehealth platform so each parent could always be seen during sessions, and we recorded sessions to code for treatment fidelity. To code group engagement for the present study, we selected one group session with full group attendance, from each intervention cohort. While previous recommendations suggest that closed treatment groups typically stabilize after the third session,( 1 ) we selected a group session that occurred towards the end of each treatment cohort to code for group engagement. We opted to do this because the REDCHiP intervention includes three individual sessions that occurred in the middle of treatment, and we wanted to account for this difference when considering group stabilization. The two independent coders for this study (authors ADM and SRP) have a background in psychology and extensive experience in video-based behavioral coding across multiple projects.19–21 Before coding sessions, our team first discussed the dimensional coding system to identify behaviors consistent with each dimension of the Group Engagement Measure. The two coders then independently watched each group session, and qualitatively documented which behaviors and interactions mapped onto each group engagement dimension using a participant-specific coding sheet based on the Group Engagement Measure. Per protocol, the coders watched each session several times and coded only one participant's behavior each time. They met weekly to discuss coding challenges and any new behaviors they attributed to each group engagement dimension. The coders considered both the frequency and quality of behaviors when assigning a numerical value to each item from the Group Engagement Measure.
Behavioral coding
Group engagement
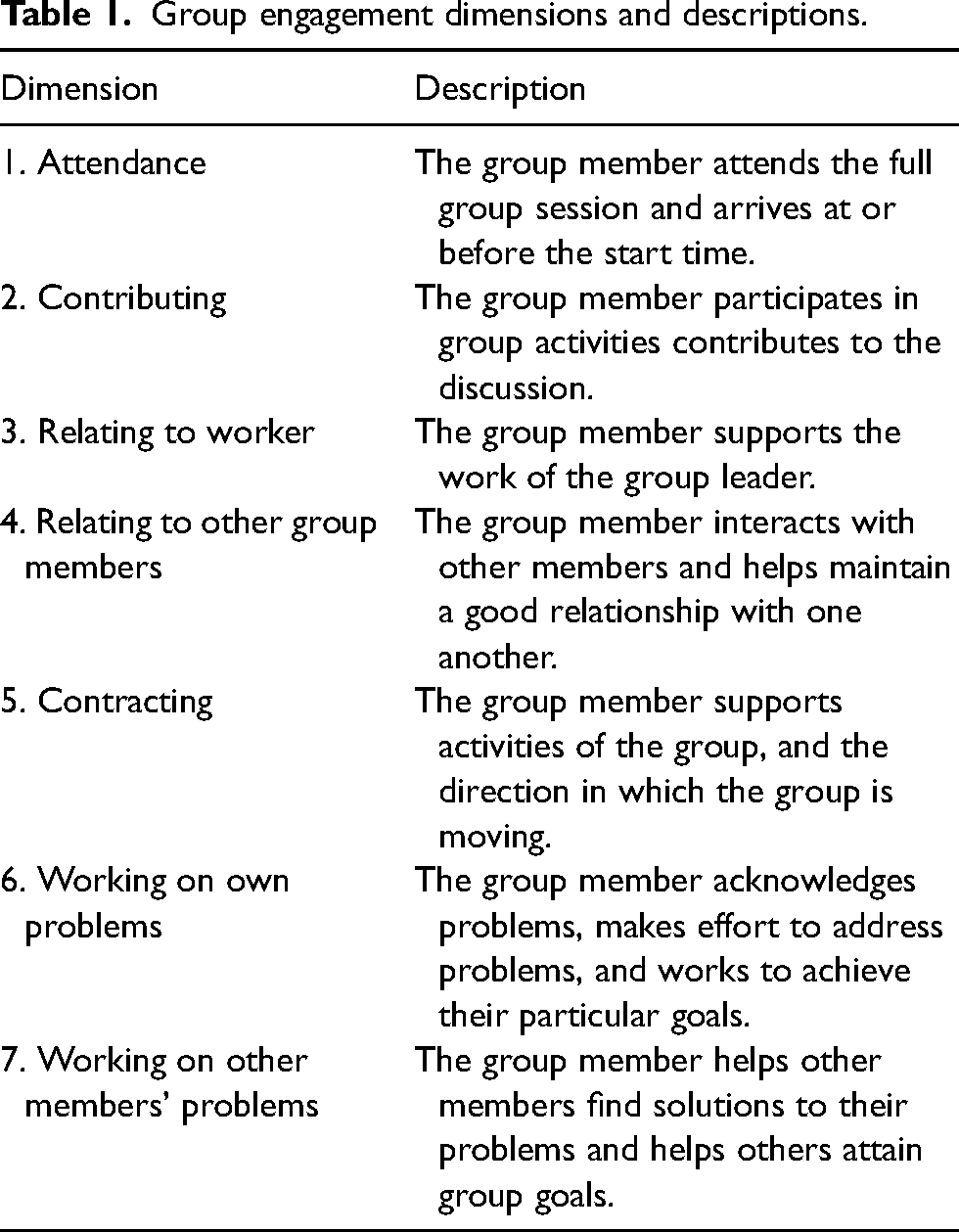
We used the Group Engagement Measure to code individual behavioral characteristics for each participant in select video-taped sessions. 1 This 27-item measure and coding system was developed to assess the engagement of an individual group member across seven dimensions of group engagement: Attendance, Contributing, Relating to Group Worker, Relating with Group Members, Contracting with the Group Service, Working on Own Problems, and Working on Other Group Members’ Problems. See Table 1 for descriptions of each group engagement dimension. Both coders rated each group member's interactions within the group session on a 5-point Likert scale (i.e. 1 = “Rarely or none of the time,” 2 = “A little of the time,” 3 = “Some of the time,” 4 = “A good part of the time,” and 5 = “Most or all of the time”) with higher scores indicating higher group engagement. There were 11 group cohorts in the REDCHiP trial and nine group cohorts in the CARES trial. Ultimately, our team coded 10 group sessions across all intervention cohorts (four REDCHiP and six CARES) including four randomly chosen sessions to double code for inter-rater reliability.
Group engagement dimensions and descriptions.
Parent-reported measures
Fear of hypoglycemia
Parents either completed the 25-item Hypoglycemia Fear Survey for Parents (HFS-P) 22 or the 26-item Hypoglycemia Fear Survey for Parents of Young Children (HFS-PYC) 23 based on the child's age. Both measures assess anxiety regarding the negative consequences of hypoglycemia and the behaviors parents may engage in to keep their child from experiencing hypoglycemia. Parents rated how frequently each statement is true for them on a 5-point Likert scale (e.g. from “Never” to “Very Often”) with higher scores indicating higher fear of hypoglycemia. Internal consistency for the HFS-P was 0.87, and for the HFS-PYC was 0.95.
Symptoms of depression
Parents completed the Center for Epidemiological Studies Depression Scale Revised (CESD-R) 24 . This 20-item measure assesses the frequency of depressive symptoms over the previous 2 weeks with higher scores indicating more depressive symptoms. Internal consistency for the CESD-R was 0.91.
Diabetes distress
Parents completed the Problem Areas in Diabetes Survey-Parent Revised (PAID-PR) 14 . This 18-item measure assesses negative emotions experienced by parents of children with T1D and parental worries about the future. Parents rated the degree to which each item is a problem for them on a 5-point Likert scale (e.g. from “Not a problem” to “Serious Problem”) with higher scores indicating more distress. Internal consistency for the PAID-PR was 0.88.
Child measure of glycemic control
HbA1c
Each child provided a finger-prick blood sample to measure his/her HbA1c at pre- and post-treatment. We analyzed children's HbA1c levels in a single laboratory using automated high-performance liquid chromatography, with measurement methods reliable to Diabetes Control and Complications Trial (DCCT) standards (Reference range 4.0–6.0%; Tosoh 2.2, Tosoh Corporation, San Francisco, California; 22) 25 .
Data analysis
We analyzed the intra-class correlation (ICC) between the scores of two coders to assess inter-rater reliability. We used descriptive statistics for the group engagement measure to examine for variation in the different dimensions of group engagement, which might support the use of a multidimensional measure of group engagement in a telehealth setting. To examine how parents’ group engagement scores may relate to their treatment satisfaction and treatment outcomes, we used Pearson correlations. We also used Pearson correlations to relate parents’ group engagement scores to their child's HbA1c. Lastly, we used independent sample t-tests to examine for differences between the CARES and REDCHiP treatments based on each group engagement score.
Results
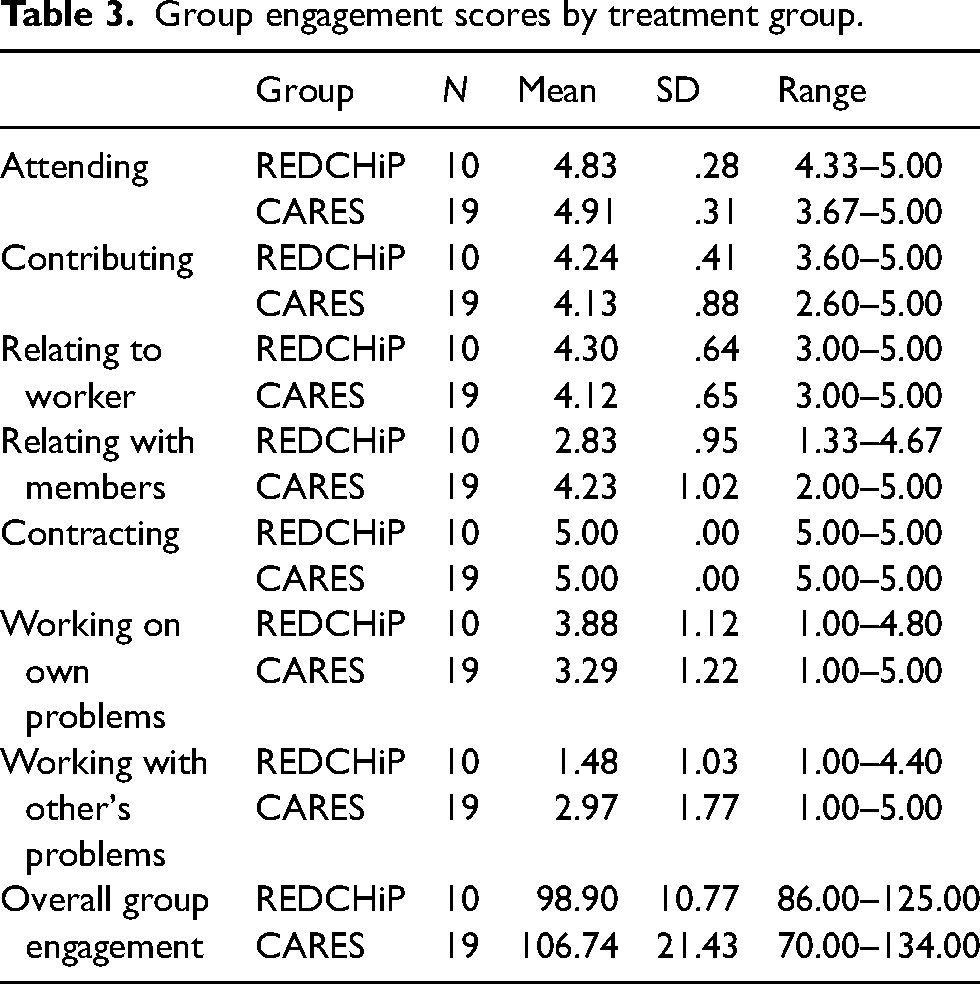
In the present analyses, we included data from 29 parents who participated in one of 10 treatment groups, with an average group size of three parents. A total of 19 parents participated in a CARES group and 10 parents participated in a REDCHiP group. The average parent age was 37.69 ± 6.83 years, and the average child age was 7.69 ± 3.76 years. At baseline, average child HbA1c was 8.06 ± 1.27% and 41.4% of children had an HbA1c < 7.5%, which was the recommended glycemic target at the time of these pilot trials. 22 Across both treatment groups, participants attended 90.7% of the treatment sessions at the scheduled day and time. See Table 2 for additional demographic information. The ICC between both coders was 0.94, indicating strong inter-rater reliability of the Group Engagement scores. Table 3 lists descriptive statistics for each Group Engagement score across each treatment group. Notably, these analyses suggest variation in all but parents’ Contracting scores. Because there was no observed variability in parents’ Contracting scores, we did not include this dimension in the subsequent analyses.
Descriptive characteristics of sample (N = 29).
Group engagement scores by treatment group.
Correlations. We examined the relationship between the Group Engagement scores and parent's age, child's age, and the number of times the parents rescheduled sessions during their time in treatment. We observed significant correlations that suggested parents older in age were more likely to have higher Attending (r = 0.37, p = 0.04), Contributing (r = 0.43, p = 0.02), Working on Other's Problems (r = 0.57, p = 0.001), and overall Group Engagement (r = 0.52, p = 0.004) scores. We also observed that parents with older children were more likely to have higher Relating to Member (r = 0.44, p = 0.02) and Working on Other's Problems (r = 0.38, p = 0.04) scores. Lastly, we observed that the parents who had higher attendance rates to scheduled sessions were more likely to have higher Contributing (r = 0.41, p = 0.03), Relating to Worker (r = 0.42, p = 0.02), Working on Other's Problems (r = 0.44, p = 0.02), and overall Group Engagement (r = 0.46, p = 0.01) scores.
We then examined the relationships between the Group Engagement scores and child HbA1c as well as parents’ report of treatment satisfaction, symptoms of depression, fear of hypoglycemia, and diabetes distress. Our results suggested that higher Attending scores related to lower HbA1c values both before (r = −0.48, p = <0.01) and after treatment (r = −0.47, p = 0.04). Similarly, higher Contributing scores related to lower HbA1c values both before (r = −0.47, p = 0.01) and after treatment (r = −0.47, p = <0.01). We saw that higher Relating to Worker scores related to lower depressive symptoms after treatment (r = −0.37, p = 0.04). Lastly, we saw that higher Attending scores related to lower fear of hypoglycemia scores both before (r = −0.39, p = 0.03) and after treatment (r = −0.46, p = 0.01), while higher Working with Other's Problems related to lower fear of hypoglycemia scores after treatment (r = −0.38, p = 0.04). Interestingly, we did not observe significant correlations between any group engagement scores and parents’ report of diabetes distress or treatment satisfaction. See Table 4 for the correlation r coefficients.
Pearson correlation of group engagement scores and other study measures.
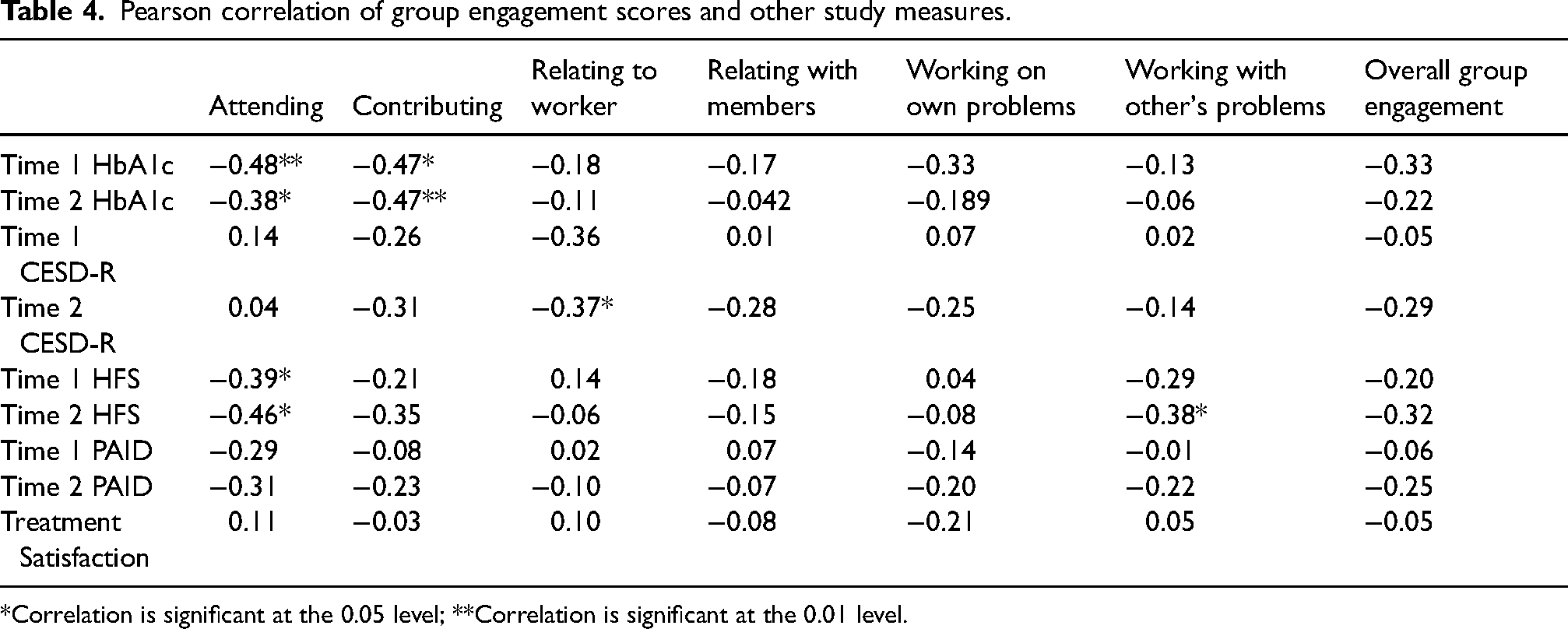
*Correlation is significant at the 0.05 level; **Correlation is significant at the 0.01 level.
T-tests. When comparing parents who participated in REDCHiP (n = 10) versus CARES (n = 20), we observed a significant difference in parent's Group Engagement scores: Relating with Members t(23) = −3.59, p = <0.01, and Working with Other's Problems t(23) = −2.44, p = 0.02, with the CARES groups demonstrating higher Relating with Members and Working with Other's Problems scores.
Discussion
The present study is, to the best of our knowledge, the first to apply a multidimensional measure of group engagement in a telehealth setting specific to families of children with T1D. For our analyses, we used data from two parent-focused telehealth interventions for families of children with T1D. In support of our first hypothesis, descriptive statistics for our group engagement measure showed variability in parents’ scores for all but the Contracting dimension. This finding offers further support for a multidimensional conceptualization of group engagement and suggests this measurement approach may also be possible to use in a video-based telehealth setting. Moreover, while we found significant positive associations between parents’ attendance to group sessions and their overall group engagement score, contribution to the discussion, support of the group leader, and participation in helping others to find solutions to personal challenges, these were only moderate associations, suggesting using group attendance as a single factor measure of group engagement might miss other group engagement behaviors in a video-based telehealth setting. Interestingly, the results of the study suggest that parents older in age, who have older children, and who attend sessions regularly are more likely to have higher select Group Engagement scores. A priori, we had not hypothesized that demographic variables would relate to parents’ group engagement scores. This finding suggests that future studies may consider demographic differences when targeting strategies to improve group engagement or evaluating the effectiveness of those strategies across different demographic groups.
In partial support of our second hypothesis, we found a negative association between parent Group Engagement scores and child HbA1c. Specifically, these results suggest children were more likely to have lower HbA1c values both pre- and post-treatment if their parents attended the full group session and contributed to the group discussion. It is possible our use of telehealth, which enabled parents to participate from home, helped them to attend group sessions in full, thereby allowing them to receive a larger treatment dose and to achieve a better outcome with respect to their child's HbA1c. We also found that parents who spent more time working on other group member's issues reported lower fear of hypoglycemia at post-treatment. Because we set up our telehealth platform so that parents could see each other during sessions, it is possible this helped parents to contribute more openly to the group discussion and to help each other to achieve treatment goals, which enabled better short-term outcomes.
Another interesting finding that may support our second hypothesis is the negative association between parents’ Relating to Worker scores and their post-treatment depressive symptoms. Specifically, our results suggested that parents who showed more active support of the group leader's purpose/goals during the session also reported fewer depressive symptoms at post-treatment. To the extent our Relating to Worker scores reflects a measure of the therapeutic alliance between parents and the group leader, this finding builds upon previous research which demonstrates an association between positive psychotherapeutic outcomes in traditional in-person treatments and group members’ therapeutic alliance and cohesion.23,24 Indeed, the therapeutic alliance between a therapist and individual is particularly important as meta-analyses suggest a consistently moderate association between therapeutic alliance and a person's treatment outcomes with few other moderating variables. 25 Further, there is evidence supporting the importance of the association between therapeutic alliance and a person's treatment outcomes even within the context of internet-based interventions involving a remote therapist. 26 Here, we offer new data suggesting the association between therapeutic alliance and a person's treatment outcomes also may extend to group-based telehealth interventions. Thus, as clinical telehealth services continue to grow, our results, coupled with these earlier studies, may highlight the importance of attending to the therapeutic alliances during telehealth treatment delivery and measuring these outcomes as part of clinical care. Several measures are available and easy to administer in a clinic setting. 27
Lastly, the results of the present study suggest interesting differences between treatment groups (REDCHiP vs. CARES) such that group members in the CARES treatment related with other group members and discussed their issues during the sessions more often than REDCHiP group members. These differences may be explained by the different focus of these two interventions. The REDCHiP intervention contained more psychoeducation content and included individual problem-solving sessions. These two factors could have limited REDCHiP group member opportunities to relate to each other during group sessions. Indeed, having the option of an individual session may have encouraged some parents to wait to discuss a specific concern or issues during an individual session versus sharing these during a group session. Further, the CARES intervention promoted additional discussion related to increasing group members’ coping skills, and group leaders encouraged families to provide positive feedback and additional suggestions if group members encountered barriers to implementing their coping strategies each week. Future telehealth interventions seeking to increase group engagement may consider planning specific discussion points throughout each treatment session and reserving time for each member to contribute to the discussion. Other models of telehealth intervention development also suggest co-designing intervention content with caregivers to promote connectiveness. 28 Lastly, the group leader should play an active role in facilitating discussion and drawing connections between group members’ responses to promote cohesion and inter-group member discussion.
The results of the present study offer several recommendations for future video-based telehealth research and clinical application of assessing group engagement. First, researchers and clinicians should consider objectively measuring group member engagement when delivering treatment via telehealth. We believe the results of our study demonstrate that an objective multidimensional measure of group engagement could help to guide group leaders in their clinical decision-making and group management. Moreover, once the group is established and stable, objectively assessing group engagement could provide important information on which group members may need additional prompting to join group discussions or which group members may benefit from increased connectiveness to other group members via a telehealth platform. Second, future researchers and clinicians should consider if a multidimensional measure of group engagement could help inform when to adapt or intensify treatment for group members. For example, with an objective measure of group engagement, it might be easier to identify group members who are not comfortable participating in a group format and might benefit from additional one-on-one check-in sessions with the group leader or different treatment modalities altogether. Evidence-based treatments exist for a range of behavioral and psychosocial concerns, however not every treatment is appropriate for every person. In this way, measuring group engagement could be an important factor to consider when a clinician is deciding if group therapy would be beneficial for a certain family. Third, with repeated measures of group engagement across a group cohort, it may be possible to modify group procedures or a group leader's interaction style to try to improve group engagement in near real-time, which might help to maximize treatment outcomes for participants. For example, one study significantly increased adolescent group engagement during a substance use treatment group by specifically targeting and intervening on group engagement factors within sessions. 29 Fourth, researchers should explore drivers of group engagement to understand what traits may modify one's group engagement score. For example, differences among specific personality traits or levels of education across group members could uncover important differences between members who score across the spectrum on group engagement. Finally, measuring group engagement could be another important variable to assess in comparative effectiveness trials for telehealth-delivered group interventions versus traditional in-person group interventions.
The overwhelming pivot to telehealth-based care during the COVID-19 pandemic will likely continue to shape the healthcare system. While previous research demonstrates feasibility, efficacy, and satisfaction with telehealth modalities,30–32 future studies must now examine how we can continue to improve telehealth-based care and address barriers to telehealth sustainability. 33 Specific to diabetes care, adults have viewed telehealth appointments as useful during the ongoing pandemic, and many plans to continue telehealth appointments in the future. 34 In pediatric T1D care, children and adolescents who use devices (i.e. insulin pumps, continuous glucose monitors) can collect and share health data remotely with their healthcare team for effective telehealth-based care and treatment recommendations. Of course, telehealth-based pediatric T1D care does not present without challenges, such as insurance coverage for telehealth visits, privacy and security of videoconferencing platforms, stable internet connections, and follow-up communication after video appointments. 35 However, we would propose that the present study demonstrates a need for follow-up research to examine how engagement may impact the efficacy of telehealth-based care when addressing both physical and mental health needs.
Strengths and limitations
This study is novel in its examination of group engagement in two parent-focused telehealth interventions. Another strength of this study is its use of an objective, multidimensional measure of group engagement and the high level of reliability the two coders achieved with their group engagement measure. However, there are some limitations to note when interpreting the results. First, this study did not include a self-report measure of group engagement for parents to complete. It is possible parents’ self-perception of group cohesion or therapeutic alliance could relate to their treatment outcomes independent of any objective measure of their engagement and yield important information to guide treatment development. Thus, future studies may consider including a subjective measure to capture each group member's perception of group cohesion or a qualitative aim to collect a more in-depth assessment of parents’ group experience. Second, the present sample was small and demographically homogeneous. While the participants were representative of the recruiting clinic, the results may not generalize to all individuals and therefore it may be important to examine group engagement in video-based telehealth treatments delivered more broadly. Third, the results of the present study represent a secondary analysis of two pilot interventions and as such the researchers did not power these pilot projects to specifically examine for treatment effects due to parents’ group engagement. Therefore, it is possible that the present study is under-powered to detect other associations between parents’ group engagement during our video-based telehealth interventions and their treatment outcomes.
Conclusion
The results of the present study provide new evidence suggesting that attendance, group dynamics, and therapeutic alliance, the multidimensions of group engagement, are important not only in in-person interventions, but also in interventions conducted via telehealth. In the future, researchers and clinicians may consider objectively measuring group member engagement when delivering treatment via telehealth and using group engagement to guide treatment planning or inform treatment-related decisions. Telehealth services and the use of videoconferencing platforms became the prominent treatment delivery method during the global COVID-19 pandemic and may continue to improve our ability to provide effective therapy services to children and their families well into the future. Ultimately, researchers and clinicians should consider group engagement an important factor to assess and incorporate in their treatment planning as telehealth and videoconferencing remain service delivery options for treatment groups.
Footnotes
Declaration of conflicting interests
ADM and SRP have no conflicts of interest to declare. MAC is the Chief Medical Officer of Glooko and provides research support to Abbott Diabetes Care and Dexcom.
Funding
This work was supported by the National Institute of Diabetes and Digestive and Kidney Diseases (grant numbers R01-DK100779 & R01-DK118514).