
Abstract
Background
With the rapid increase in telehealth use during the COVID-19 pandemic, concerns have been raised about the potential for exacerbating existing healthcare disparities in marginalized populations. While eliminating barriers such as transportation and time constraints, telehealth may introduce barriers related to technology access. With little known about the patient experience accessing telehealth during the COVID-19 pandemic, this study seeks to understand the barriers and facilitators to telehealth use as well as interventions that may address them.
Methods
We conducted qualitative interviews with parents of pediatric patients of a primary care clinic in a diverse community during the study period of March–May 2021. The interviews explored barriers and facilitators to telehealth during the COVID-19 pandemic. Interviews were balanced across language (Spanish and English) as well as across visit type (in-person vs. telehealth). Recruitment, collection of demographic information, and interviews were conducted by telephone. The conversations were recorded and transcribed. Once thematic saturation was achieved, the data were analyzed using a modified grounded theory approach.
Results
Of the 33 participants, 17 (52%) spoke English and 16 (48%) spoke Spanish. A total of 17 (52%) had experienced a telehealth encounter as their first visit during the study period while 16 (48%) had an in-person visit. Five themes were identified: (1) a recognition of differences in technological knowledge and access, (2) situational preferences for telehealth versus in-person visits, (3) avoidance of COVID-19 exposure, (4) convenience, and (5) change over time. English-speaking patients expressed greater ease with and a preference for telehealth, while Spanish-speaking participants expressed more technological difficulty with telehealth and a preference for in-person visits. Suggested interventions included informational tutorials such as videos before the visit, technical support, and providing families with technological devices.
Conclusion
In this study, we examined patient and family perspectives on pediatric telehealth during the COVID-19 pandemic. Implementation of the suggested interventions to address barriers to telehealth use is essential to prevent further exacerbation of health disparities already experienced by marginalized populations.
Keywords
Introduction
Telehealth use in ambulatory medical care has been steadily increasing and has grown particularly rapidly during the COVID-19 pandemic.1–5 This rapid growth of telehealth during the pandemic was a key component of healthcare delivery as telehealth enabled ongoing access to care for many patients while also reducing the potential for viral transmission.
Legitimate concerns have been raised, however, regarding the potential for telehealth to worsen existing healthcare disparities. 6–8 The technology may introduce additional barriers for patients with limited English proficiency, with lower health literacy or digital literacy, or with limited access to devices or broadband connectivity. This effect has been termed “the digital divide.”9,10 Importantly, these barriers may affect both access to and efficacy of telehealth. 11 In contrast, however, telehealth could also reduce barriers to care by eliminating the need for transportation and associated costs of an in-person visit. A few studies have examined the transition to virtual care during the pandemic and its effect on healthcare access for underserved populations.12–14 However, the experience of this change by patients and families has been more difficult to capture. 15
Given how little is known about the experience of patients and families accessing telehealth during the COVID-19 pandemic, the goal of this work is to better understand barriers and facilitators to telehealth use among pediatric patients, and specifically to compare barriers and facilitators between English- and Spanish-speaking parents. While telehealth as a term can refer to multiple forms of remotely delivered technologically facilitated care, this study focuses on virtual visits occurring through online videoconferencing or phone.
Methods
Between March and May 2021, we conducted a qualitative (in-depth interview) study with a purposive sample of parents of patients from a pediatric primary care clinic affiliated with an academic medical center located in a diverse community. Interviewees were parents of children who had received care in the clinic prior to initiation of the study and were selected to balance across language (English vs. Spanish) and telehealth use (in-person vs. telehealth visit). We chose to use in-depth qualitative interviews to identify the range of opinions and new ideas and concepts. Interview questions were designed to examine barriers and facilitators to telehealth and develop novel, patient-centered ideas for interventions (Supplementary Table 1). While we use the term telehealth in this manuscript, the interview guide referenced telemedicine visits as we felt this term would be most understandable to patients. Team members (GC, AA) were trained in qualitative interviewing by researchers with extensive prior qualitative experience and training (MSK, AC), and underwent practice interviews prior to beginning the study. In addition, transcripts were reviewed and interview feedback was provided after early interviews to improve quality.
There is no standard accepted sample size for qualitative research, but most papers report thematic saturation at around 6–12 interviews for a group of individuals with similar demographic characteristics or characteristics of interest. 16 We aimed to interview individuals in the following groups: (English-speaking with in-person clinical visit, English-speaking with telehealth visit, Spanish-speaking with in-person clinical visit, and Spanish-speaking with telehealth visit) until thematic saturation was reached in each group.
Due to the ongoing COVID-19 pandemic, telephone recruitment and consent were used. Potential participants were called by a bilingual member of the study team (GC, AA) and underwent a verbal informed consent process. Participants completed a brief demographic survey prior to the interview. Interviews focused on barriers and facilitators to telehealth use, and on the experience of receiving care during the COVID-19 pandemic. All interviews were recorded and professionally transcribed. A coding tree was developed based on the interview guide and was refined with input from the entire team. Transcripts were coded by two independent members of the research staff (GC, AA) with differences resolved by consensus. Coding and theme development were ongoing throughout the study process, with changes to the coding tree and interview guide as themes were identified. Analyses used a modified grounded theory framework, 17 and thematic saturation was identified by consensus. Coded data from English-speaking and Spanish-speaking participants were organized by theme in a matrix to facilitate the comparison of responses. This research was approved by the Partners Human Research Committee, and was performed and presented in accordance with the consolidated criteria for reporting qualitative research (COREQ) checklist. Where quotations are included from Spanish speakers to preserve meaning to the greatest degree possible, the original Spanish is presented with an italicized English translation.
Results
There were 33 participants, of whom 17 (52%) preferred English and 16 (48%) preferred Spanish. A total of 17 (52%) had experienced a telehealth encounter as their first visit during the study period and 16 (48%) had an in-person visit. The demographics of the study cohort are shown in Table 1, with differences in educational attainment and insurance status between the language groups. Of note, some English-speaking participants identified as Hispanic/Latinx.
Demographic information of study participants by language group.
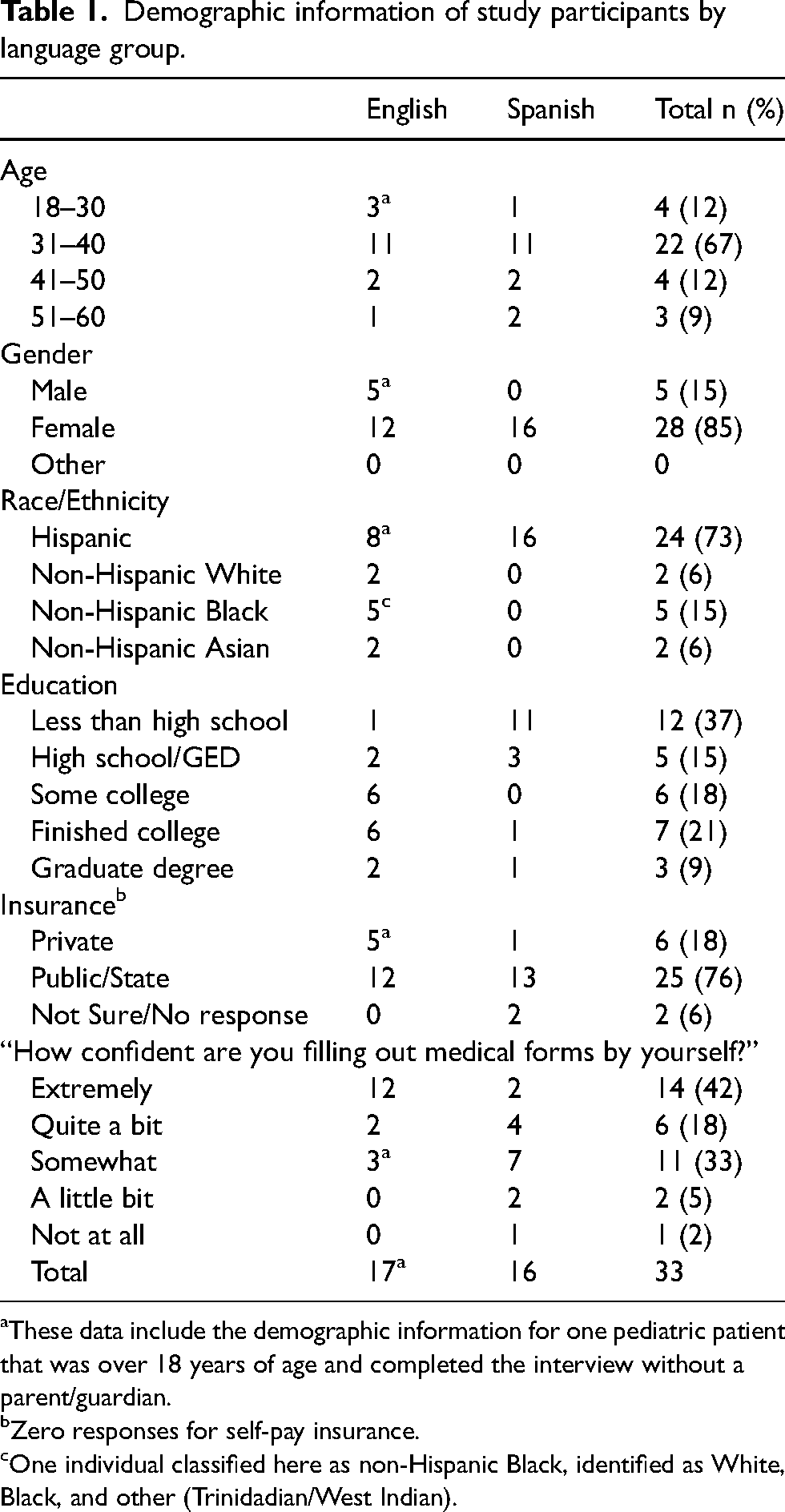
These data include the demographic information for one pediatric patient that was over 18 years of age and completed the interview without a parent/guardian.
Zero responses for self-pay insurance.
One individual classified here as non-Hispanic Black, identified as White, Black, and other (Trinidadian/West Indian).
There were five main themes that were identified from our interviews, along with several recommendations from participants about how to improve telehealth access. The themes were: (1) a recognition of differences in technological knowledge and access, (2) situational preferences for telehealth versus in-person visits, (3) avoidance of COVID exposure, (4) convenience, and (5) change over time. Overall, English-speaking patients more often mentioned the advantages of virtual visits, whereas Spanish-speakers more commonly discussed the advantages of in-person visits.
Recognition of differences in technological knowledge and access
Participants described technological challenges around connectivity, access, and knowledge. English-speaking participants tended to describe hypothetical barriers or challenges that might affect other individuals: “I think the biggest issue is more of like the technology barriers. Not everyone wants to adapt or I know it's hard to adapt to be able to use the technology as best as they can for telemed especially.” Several participants commented on how older individuals may struggle more with virtual visits. Interestingly, one participant highlighted the physician‘s challenges with the telehealth system: “And then, at the appointment, I logged in, and they put me in a waiting room, and I kind of just waited for the doctor to come in. And then he was a little fumbly with the Zoom or accessing the Zoom which, again, I understand. I think it's a learning curve for some of the older generation, so I didn't have a problem with that.”
While some Spanish-speaking participants expressed similar sentiments, others reported needing assistance from their children or extended family to connect to virtual visits “Yo casi no sé mucho meterme en cosas así pues en los teléfonos o sobre una computadora, yo nunca la he usado … Sí, necesito siempre la ayuda de mis hijas.” (I almost don‘t know much about going into those things like telephones and computers, I have never used them…I always need the help of my daughters.) Additionally, some Spanish-speaking participants suggested that limited literacy may serve as a barrier to the use of telehealth: “Pero donde ya me explica el doctor cómo es, cómo uno entra y todo pues, ya sentí más fácil, en el caso mío que sé leer, pero en el caso de personas que no saben leer es muy difícil para ellas.” (But where the doctor already explained how it is, how you enter and everything, I felt it was easier, in my case where I know how to read, but in the case of others who don‘t know how to read, it‘s much more difficult for them.)
Situational preferences
The discussion around situational preferences was similar across language groups, with parents describing the importance of an in-person exam for specific conditions or for obtaining services such as vaccines, “Because like I said, she has a breathing disease, and they used to hear her lungs. It's something that they cannot do through the telehealth. And also, they always check in the oxygen levels, and they do a breathing test every time that we go. So they do a multiple things that they cannot do through the telehealth.” Additionally, communication was often described as being better through in-person visits, such as “Porque siento yo que mirándolo físicamente-- le voy a dar la experiencia cuando he visitado al [redacted]. Ahí, “¿quiere traductor?” -me dice-, “sí", te ponen ahí a una persona. Y yo los estoy mirando, y ellos si me ven que yo tengo una duda, ellos me dicen: “¿Qué no entiende? ¿O qué no entendió?". Yo les explico, entonces vuelven ellos a decir lo que yo quiero que ellos me digan o lo que yo quiero dar a entender.” (Because I feel that looking at him physically —I’m going to give you an experience of when I visited [redacted] there. “Would you like an interpreter?” they asked. “Yes.” They put this person there. And I am looking at them and they see that I have doubts, they ask, “What don‘t you understand? Or what didn‘t you understand?” I explain so then they say again what I want them to tell me or what I want to understand.) In addition, some participants commented that mental health visits were easier via telehealth: “But thus far, I really do-- I see the benefit for sure. I’m not sure about the more hands-on healthcare, but when it comes to psychiatry, I can say that telemedicine is a very good option, at least one that benefits me. If anything, it made me feel more comfortable to share my symptoms just because I’m at the comfort of my own home, and so I’m more inclined to open up rather than being in the place where I know that I am sick because of the hospital environment. So I guess being comfortable really helps with that.”
Avoidance of COVID-19 exposure
Both English- and Spanish-speaking parents emphasized the importance of telehealth visits for keeping their children safe from COVID-19 exposure, “Back then, we were so scared to go, especially to go to the hospital, and I was trying to keep them at home, especially not to risk my daughter.”
Convenience
The convenience of virtual visits was discussed by both groups, such as “Y a veces, cuando es así, cita personalmente, hago el esfuerzo, porque casi siempre las pido por la tarde, porque yo trabajo; entonces, yo corro para allá, para el hospital. Pero cuando es virtual se me hace muy bien, porque ya yo estoy en la casa, ya estamos explicándole a la doctora o ella nos explica a nosotros cómo es acerca de la cita.” (And sometimes, when it‘s like that, an in-person appointment, I make an effort because I almost always ask for them in the afternoon because I work. So then I run over there, to the hospital. But when they are virtual I feel like they are very good, because I am in my home, already explaining to the doctor or she is explaining to me what the appointment will be like.) However, convenience was more frequently mentioned by English-speakers, including: “I do not think that people have to be doing all this traveling and going into [Hospital] and whatever. I just don't think it's necessary. But for something like a follow-up, I don't see why it's necessary for somebody to be going all the way into the city. I just think that's just ridiculous.”
Change over time
Both groups reported being skeptical of telehealth in the early stages of the pandemic, but that the method became more acceptable to them over time (Table 2).
Themes and illustrative quotes.
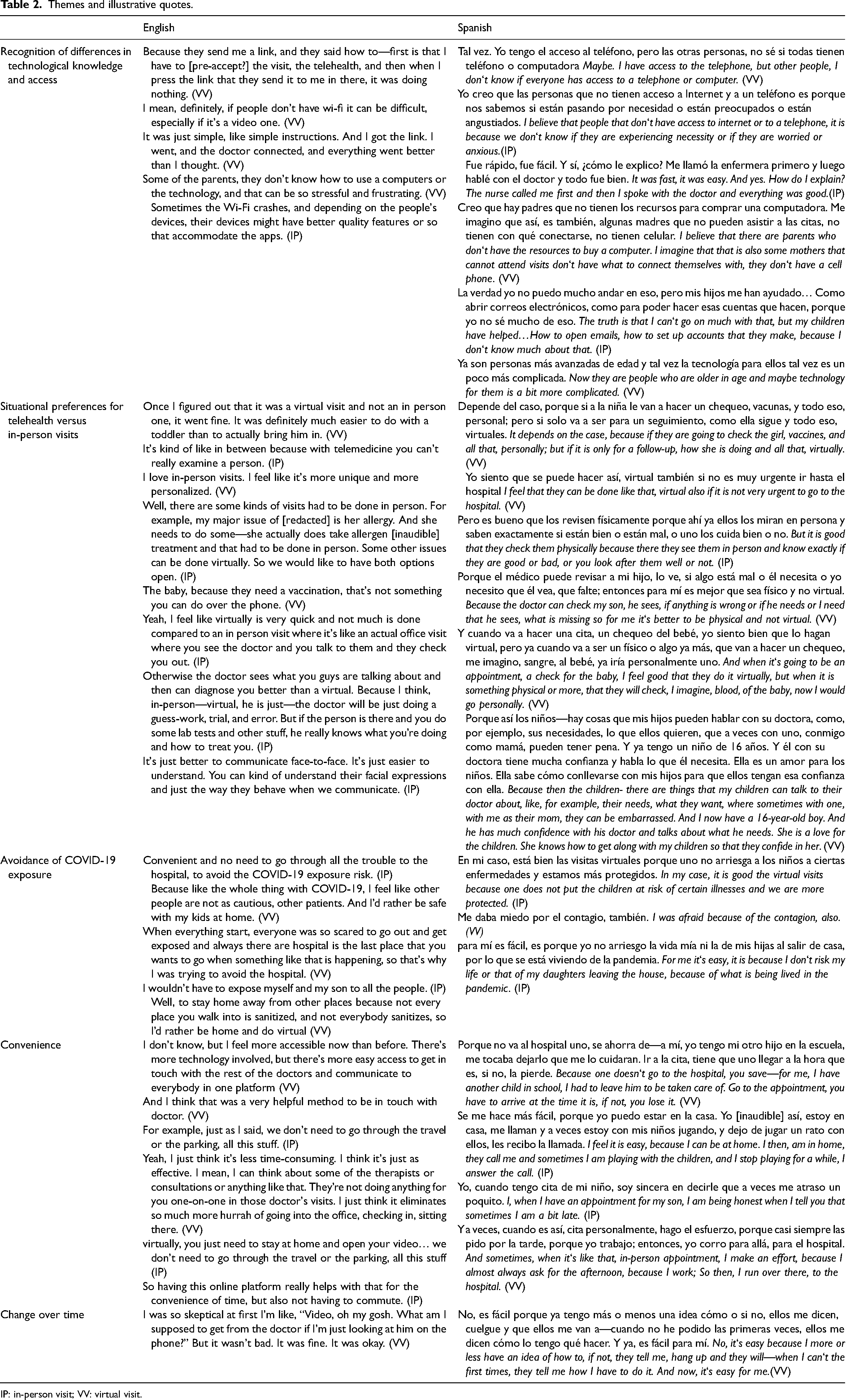
IP: in-person visit; VV: virtual visit.
Recommendations
Participants made several recommendations for improvements to telehealth delivery systems. Recommendations included phone and technical support, including detailed instruction on the use of the platform via phone call with video tutorials and step-by-step instructions. Participants recommended simplifying the process wherever possible: “Oh, a tutorial to find and to tell you where things are in the app or the website. Because if I see it on the website, it's different on a computer than on my app on the cell phone, you know what I mean? It's just different. You just have to take your time to do it, and not everybody has the time to sit down and navigate their way to learn it again.” Both language groups also requested notifications and appointment reminders, and discussed strategies for helping individuals navigate potential financial barriers to telehealth access, such as, “Maybe notifying people of free public wi-fi and just having maybe videos to show people how to do it correctly.” Several Spanish-speaking participants commented on the importance of having a Spanish-speaking provider: “No, mi preferencia fuera siempre la misma: que fuera en mi idioma.” (No, my preference would always the same: that it be in my language.)
Suggested solutions included providing detailed training and technical support for families accessing telehealth services, with video options: “Like sometimes they send you a video like how-- I know I have done that before. Like they’ll send you a video on how to do it before you actually have to do it. So whenever you’re confirming the appointment-- because usually, you get the message about the appointment when they call. Add to that message the video on how they have to do it so that when it's time for them to do it, they’re ready. They already know what they have to press and how it works,” as well as reminders. It is important to remain cognizant of language preferences when developing some of the previous interventions like video tutorials, 20 a concern that arose in English-speaking families as well. “If it's in multiple languages, yes. Or I find a lot of the, let's say, people-- my husband, for example, he's from Honduras and a lot of them, even though they’re young, in their 30s, they don't understand that type of technology because in their country they may not have it like that. So I don't know, unless it's in other languages and maybe if it's quick.”
Some Spanish-speaking families suggested that the clinic assist families without resources by allowing them to borrow technology similarly to what is being done by some schooling systems. “Sí hay métodos de ayudar, como las escuelas ahorita, que, para que los niños no asistieran a la escuela les obsequiaron una computadora mientras ellos regresan. Y están usando esa computadora, porque, creo que hay padres que no tienen los recursos para comprar una computadora. Me imagino que así, es también, algunas madres que no pueden asistir a las citas, no tienen con qué conectarse, no tienen celular. Y ayudándoles, que todos colaboremos a ver quién necesita un iPad o un teléfono, aunque sea.” (There are ways to help, like schools right now, to assist children schools are presenting students with computers until they return. And they are using the computers, I believe, because their parents don‘t have the resources to buy a computer. I imagine that this would also help mothers who cannot attend appointments because they cannot connect themselves, they do not have phones. And helping them, that we all collaborate to see who needs an iPad or phone at least.) (Table 3).
Recommendations and improvements.
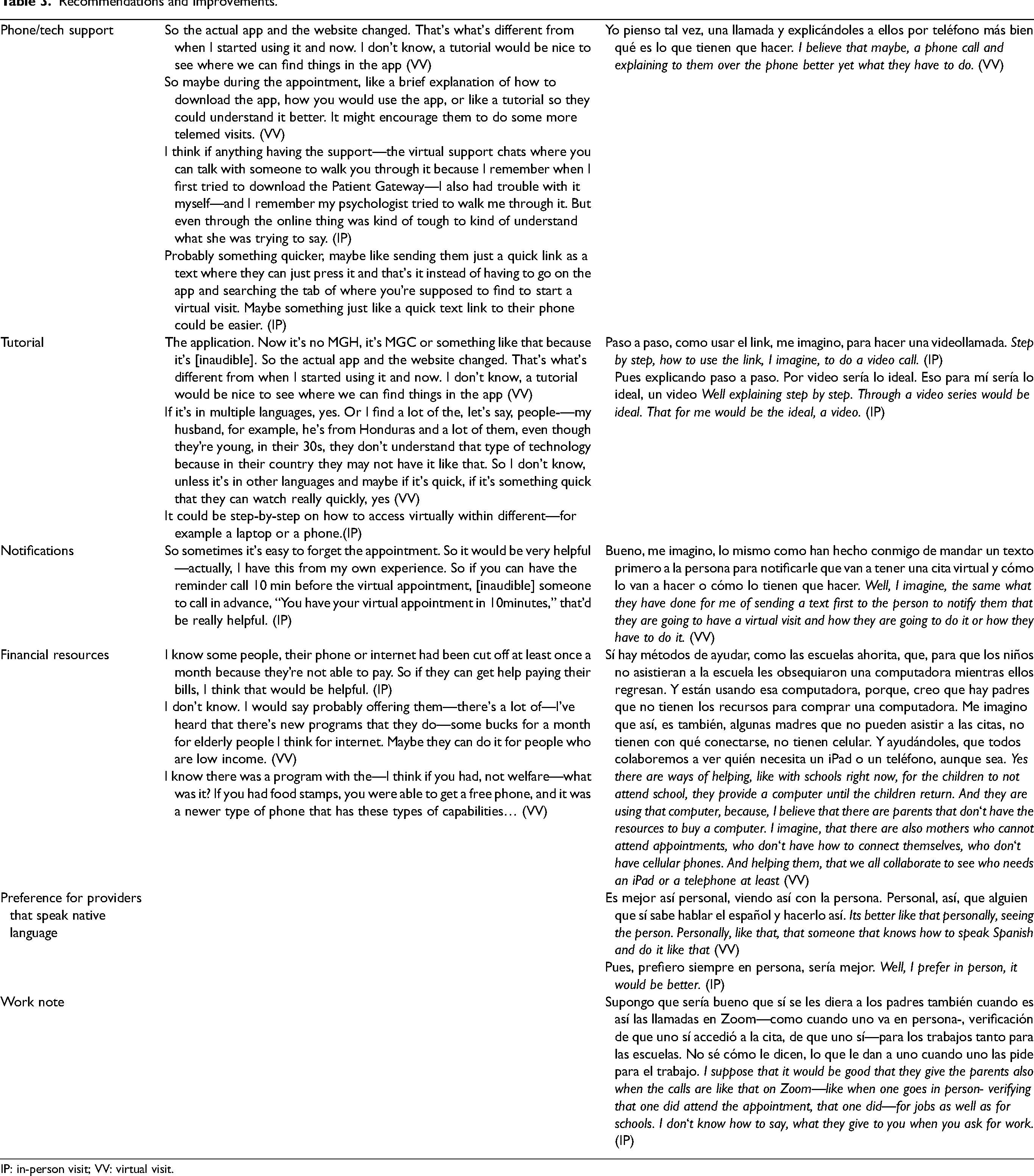
IP: in-person visit; VV: virtual visit.
Discussion
In this study, parents identified five themes around telehealth access: (1) a recognition of differences in technological knowledge and access, (2) situational preferences for telehealth versus in-person visits, (3) avoidance of COVID exposure, (4) convenience, and (5) change over time. Overall, English-speaking parents were more positive about telehealth, more likely to discuss barriers as hypotheticals rather than lived experience, and more likely to describe convenience as an important facilitator. Spanish-speaking parents, in contrast, described more challenges around technology access, and a stronger preference for in-person visits for both clinical and communication-based reasons. Both groups were similar in their discussion of the advantage of avoiding COVID-19 exposure and becoming more comfortable with virtual visits over time. Participants faced barriers at individual (e.g. limited literacy), structural (e.g. affordability of Wi-Fi), and institutional (e.g. telehealth portal not easily available in Spanish) levels.
Large-scale survey and chart review-based research demonstrates racial/ethnic disparities in access to telehealth during the COVID-19 pandemic.2,6,18 This study provides urgently needed user-centered insights into possible mechanisms behind these disparities. 19 Our Spanish-speaking participants echoed findings from other studies with respect to internet/data access barriers for individuals with limited English proficiency. 18 Spanish-speaking parents’ need for assistance from younger family members to access telehealth appointments is an important finding with implications for the design of technical support.
Additionally, participants emphasized the importance of addressing the financial challenges that serve as a barrier to telehealth access and increasing knowledge about available assistance programs. Finally, participants strongly preferred providers who could speak their language, and Spanish-speaking parents often preferred in-person visits even when their telehealth provider also spoke Spanish.
Although not frequently mentioned in our interviews, audio-only telehealth visits may also help to reduce technology-related barriers to participation,20,21 but may increase the feeling that something is missed without an in-person exam or even the opportunity to conduct a video physical exam. Previous work has found that Hispanic and Spanish-speaking patients were less likely to use video visits, and more likely to have phone-only telehealth visits during the initial stages of the COVID-19 pandemic. 12
Limitations
The study has several potential limitations. We interviewed only parents who spoke either English or Spanish and so these findings may have limited generalizability to the experience of families speaking other languages, specifically those with non-Roman alphabets who may face additional struggles using patient portal systems to access telehealth services. We also interviewed families over the phone and so were limited to those who had telephone access. Additionally, the clinic from which we recruited participants has a high rate of bilingual clinicians and so many of our Spanish-speaking patients have Spanish-speaking providers for their children at baseline, potentially reducing the barriers to communication they faced interacting with the clinic providers. Additionally, as with all interview studies, our work may be subject to social desirability bias where the interview participants did not want to criticize provided services to someone who was perceived as a representative of the service provider (hospital), despite an introduction that made it clear that the research team was separate from the provision of clinical care. Finally, while we describe the variation in themes across linguistic groups, this is not a prevalence sample and the groups differ in educational attainment and other baseline characteristics; the study is designed only to describe the range of potential themes but not the number of people with each opinion or idea.
Conclusion
In this study, we examined patient perspectives of telehealth during the COVID-19 pandemic. The qualitative interviews highlight individual, structural, and institutional barriers as well as facilitators of telehealth use. English-speaking participants expressed a greater ease with as well as a preference for telehealth while Spanish-speaking participants expressed more technological difficulty with telehealth and a preference for in-person visits. Suggested interventions included providing informational tutorials such as videos prior to the visit and technical support during the visit should issues arise, as well as providing technological devices to those without. Utilization of interventions to address barriers to telehealth use is essential to prevent further exacerbation of health disparities.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.