
Abstract
Introduction
In Queensland, Australia, the public hospital system has used telehealth for almost three decades. Although telehealth activity has been growing consistently, there are substantial variations across geographic regions. We explored factors which contribute to this variation in telehealth adoption.
Methods
This was a multi-method comparative study of two matched metropolitan health services and two matched rural health services. The health services were matched according to the number of providers and hospitals but had different rates of telehealth use. Comparative rates of telehealth visits were analysed using descriptive statistics. Qualitative data was obtained from 63 semi-structured interviews with telehealth administrators, clinicians and senior managers involved in telehealth policies and procedures. Data were analysed using a framework analysis.
Results
The metropolitan health service that had more telehealth use had greater investment in telehealth, higher population referral areas, highly developed communication strategies and understanding of the value proposition for telehealth, and reported fewer information technology and administration systems difficulties. In rural health services, telehealth activity was influenced by onboarding processes, clinician willingness to practice, strategic challenges and primary care activity.
Discussion
Telehealth adoption can be influenced by funding, cross-organisational strategic policies and a multi-faceted approach to address clinician reluctance to use telehealth.
Introduction
Telehealth has been used extensively for several decades in Australia, mainly because of the challenges associated with distance, a widely dispersed population and the centralisation of specialist health services in metropolitan areas. 1 However, despite the strategic intention to increase telehealth adoption and expansion, 2 prior to COVID-19 telehealth was used for only a small proportion of all clinical services.3–5 Understanding the factors which may influence telehealth uptake would enable the development of targeted strategies to drive telehealth adoption.
Advantages of telehealth for patients and healthcare providers have been well documented.1,6,7 For patients, these potential benefits include improved access to healthcare, reduced need for travel, greater convenience and lower personal expenses.6,8 For organisations, telehealth can reduce demand on emergency services and length of hospital stay, improve the quality of clinical services and clinical outcomes, and support multi-disciplinary care particularly for the management of chronic and complex conditions.6,9–11 In addition, telehealth provides valuable learning and professional development opportunities for health providers.6,12
The evidence concerning the adoption of telehealth is multifaceted. Factors such as the lack of evidence for clinical and cost-effectiveness, training, health provider protocols, and changes in workflows have all been highlighted.4,13,14 However, factors which support telehealth adoption and sustainability are not as well understood. Clinician’s acceptance or willingness to use telehealth is a primary driver. 4 New services require a clear vision and the support of managers and clinicians. 1 Once developed, services must be flexible, able to respond to key stakeholders needs and require new procedures and processes including ways to cope with technology problems. 1
Another key factor is how telehealth is implemented and the process that is used during deployment and roll-out of new telehealth systems. These change-management processes are often less frequently reported in telehealth literature. 15 A recent systematic review identified 16 strategies that have been applied when implementing telehealth services. 15 However, not all contexts are similar and therefore the same implementation process may not work in all of them. Understanding the factors which are of key importance to successful implementation may help with a more nuanced understanding for success. Furthermore, understanding is warranted of what strategies would increase adoption and expansion once telehealth is deployed. To support this, comparing organisations of similar size, location, implementation processes and context would be useful.
Therefore, to investigate factors associated with differences in the adoption and expansion of telehealth services, this study compared two matched metropolitan health services and two matched rural health services. Each pairing had differing levels of telehealth activity. This study sought to identify the main drivers of different telehealth adoption processes to facilitate evidence-informed decisions which promote telehealth uptake and change in the health service.
Methods
Setting
Queensland is the second largest state in Australia (area approximately 1,727,000 km2) with a population of around 5 m. 16 In contrast to the rest of Australia, Queensland’s population is relatively decentralised, with more than half of its population living outside its capital city, Brisbane. To support the dispersed population’s healthcare the Queensland Health (QH) Department established a videoconference network 20 years ago, and now connects more than 200 hospital and community facilities throughout the state. The majority of the QH videoconsultation services are delivered via the Telehealth Portal, which is coordinated through the QH Department’s Telehealth Support Unit.
The QH Department is made up of 16 Hospital and Health Services (HHSs). Service level agreements are negotiated between the QH Department and each HHS. Patients who require a specialist appointment may be referred to a Queensland Health staff specialist – at the nearest location, which often means travel to a larger metropolitan facility. Alternatively, the patient may be referred to a privately practising specialist. In this circumstance, the patient may incur additional out of pocket fees charged by the private specialist, whereas there is no charge for a public appointment with a staff specialist.
Over a four-year period, from 2013–2014 to 2016–2017, A$30.9 m was invested into telehealth services by the Queensland Government, to encourage the expansion of telehealth services within Queensland. Although there has been strong overall growth in telehealth during this time, the rates of adoption and expansion are different across the state.
Study design
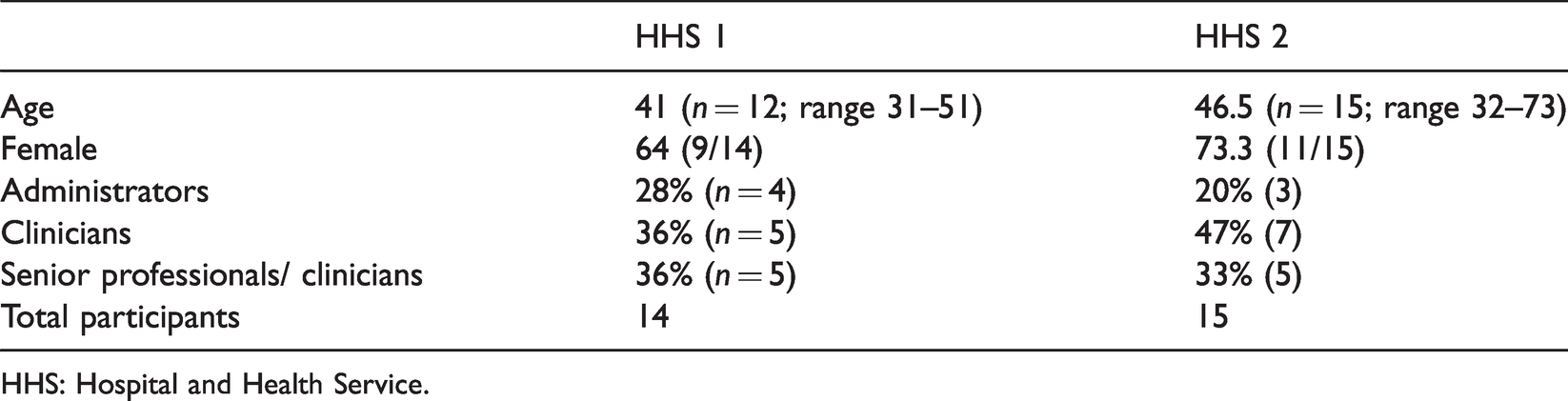
To understand factors affecting adoption and expansion, we used a multi-method comparative case study approach with two matched metropolitan HHSs and two matched rural HHSs. Initial scoping of telehealth activity in 16 HHSs identified two metropolitan HHSs (predominately telehealth service providers) and two rural HHSs (predominately telehealth recipients) who have similar profiles in terms of numbers of hospitals, population served and geographical area for rural HHSs (Table 1) – but different levels of activity. Ethical approval was obtained (HREC/2019/QMS/54871) as well as governance approval for each organisation and informed consent from all participants.
Matched Hospital and Health Service (HHS) characteristics.

Data collection and recruitment
Monthly telehealth services data that is routinely collected was obtained from the QH Telehealth Support Unit and used for the quantitative analysis.
For qualitative data, a purposive sampling technique and snowballing were used to identify potential participants. 17 Senior telehealth staff at each HHS identified potential participants for semi-structured interviews. Criteria included experience or knowledge of telehealth at a senior manager, clinician or administrator level. Once identified, participant information and consent forms were sent by email. In total, 92% (n=58) of interviews took place in-person at the participant’s location, 6% by videoconferencing and one by phone. Researchers (AB, LJC, AS and AM) conducted interviews in rural areas as a group and individually. Metropolitan interviews were conducted by AB and a research assistant (MT). In rural areas snowballing was used to identify others who met the criteria. Recruitment and interviewing continued until data saturation was reached.
Interviews lasted approximately 45–60 min. In some cases, interviews were conducted in groups when senior members of staff requested that their team members were included in the interview. Interview questions focused on the service model, technology, operations, adoption, outcomes and impact for organisations and patients, as well as ways to innovate for an increase in telehealth adoption. Questions were adapted as required for the three types of roles. For example, senior managers were asked about strategic barriers to adoption, whilst administrators were asked about workflow barriers. All interviews were recorded and field notes were taken during each interview.
Data analysis
Telehealth activity data were analysed using descriptive statistics. Recordings of the semi-structured interviews and focus groups were used in conjunction with research team field notes 18 made from the interviews to develop contemporaneous notes for each interview. Deductive analysis was undertaken using the adapted Telehealth Pathways Framework 19 in NVivo to manage and code the data. 20 Each organisation was coded separately for first stage coding after which hierarchical categories were revised. During the second stage, coding sub-categories were developed to provide more in-depth understanding. These categories were the same for metropolitan and rural health services except for 'adoption' which included education and process sub-categories for rural services. To enhance credibility, coding was discussed between researchers until consensus was reached. 21
Results
Metropolitan organisations
Levels of activity
In 2018–2019 HHS 1 performed 12,796 teleconsultations of which 74% were medical and the remaining were nursing and allied health services. HHS 2 performed 5843 service events of which 84% were medical and the remaining were nursing and allied health services. Although there were multiple hospitals within each matched pair, HHS 2 had 93% of their telehealth performed at one hospital whereas, HHS 2 had two major hospitals providing telehealth consultations – comprising 77% and 20% respectively of all activity.
Figure 1 illustrates outpatient telehealth services (excluding mental health) from 2013/2014 to 2018/2019. The growth rate for the initial 3 years was relatively similar for both HHSs but a substantial increase in activity for HHS 1 took place in 2016/2017.
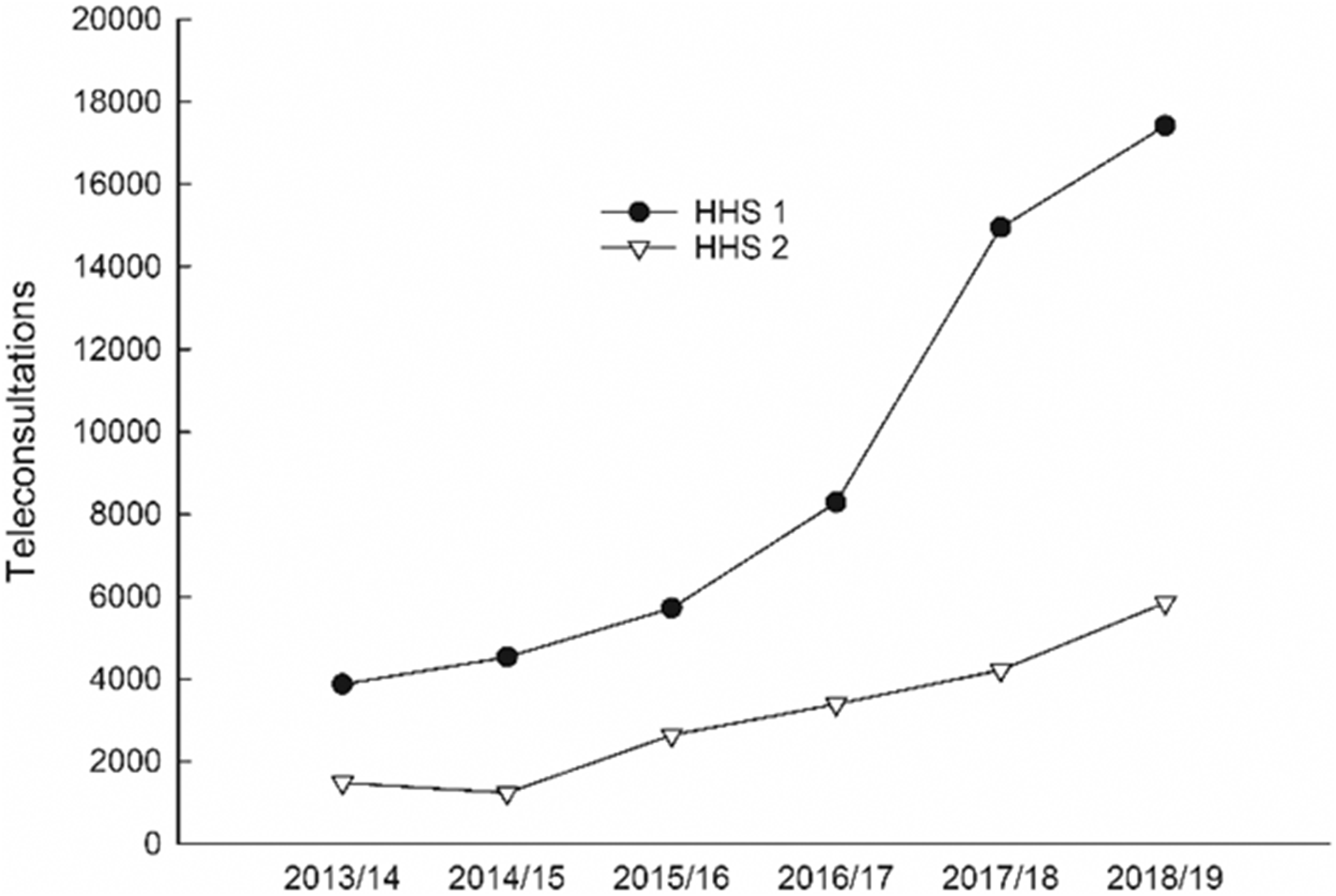
Outpatient telehealth service events by metropolitan Hospital and Health Services (HHSs) for years 2013/2014–2018/2019.
Figure 2 outlines the medical specialities which performed more than 100 consultations per year. Of the 34 medical specialties, nine are the same in both HHSs. In HHS 1 there were nine additional services and seven in HHS 2.
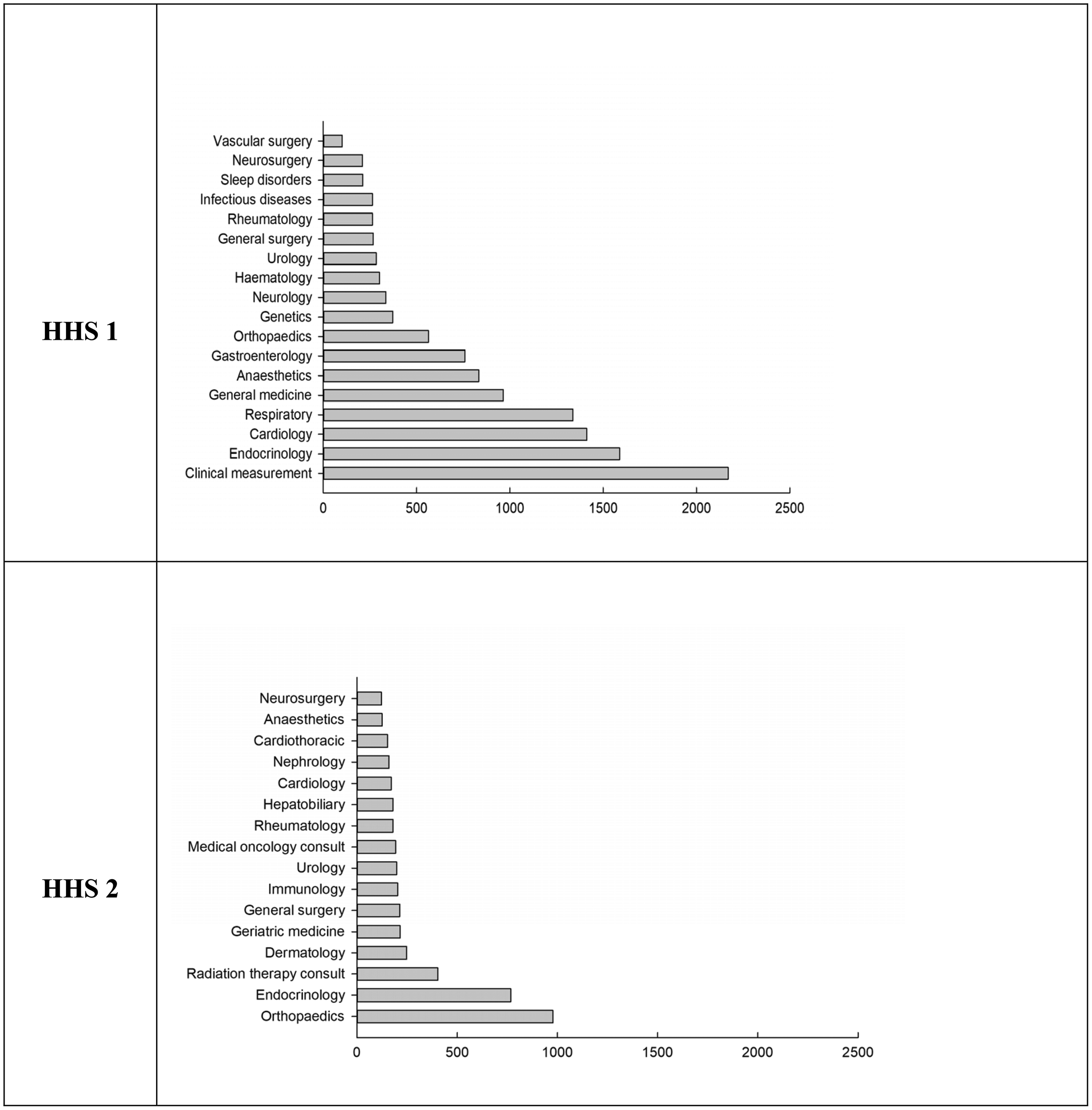
Comparison of telehealth activity between each metropolitan Hospital and Health Service (HHS) by medical specialty (>100 consultations per year) for year 2018–2019.
For allied health and nursing consultations, HHS 1 had nine different disciplines using telehealth for more than 100 consultations per year, whereas HHS 2 had four disciplines at this level of activity. HHS 1 had a statistically significant higher proportion of services provided by nursing and allied health compared to HHS 2 (Figure 3).
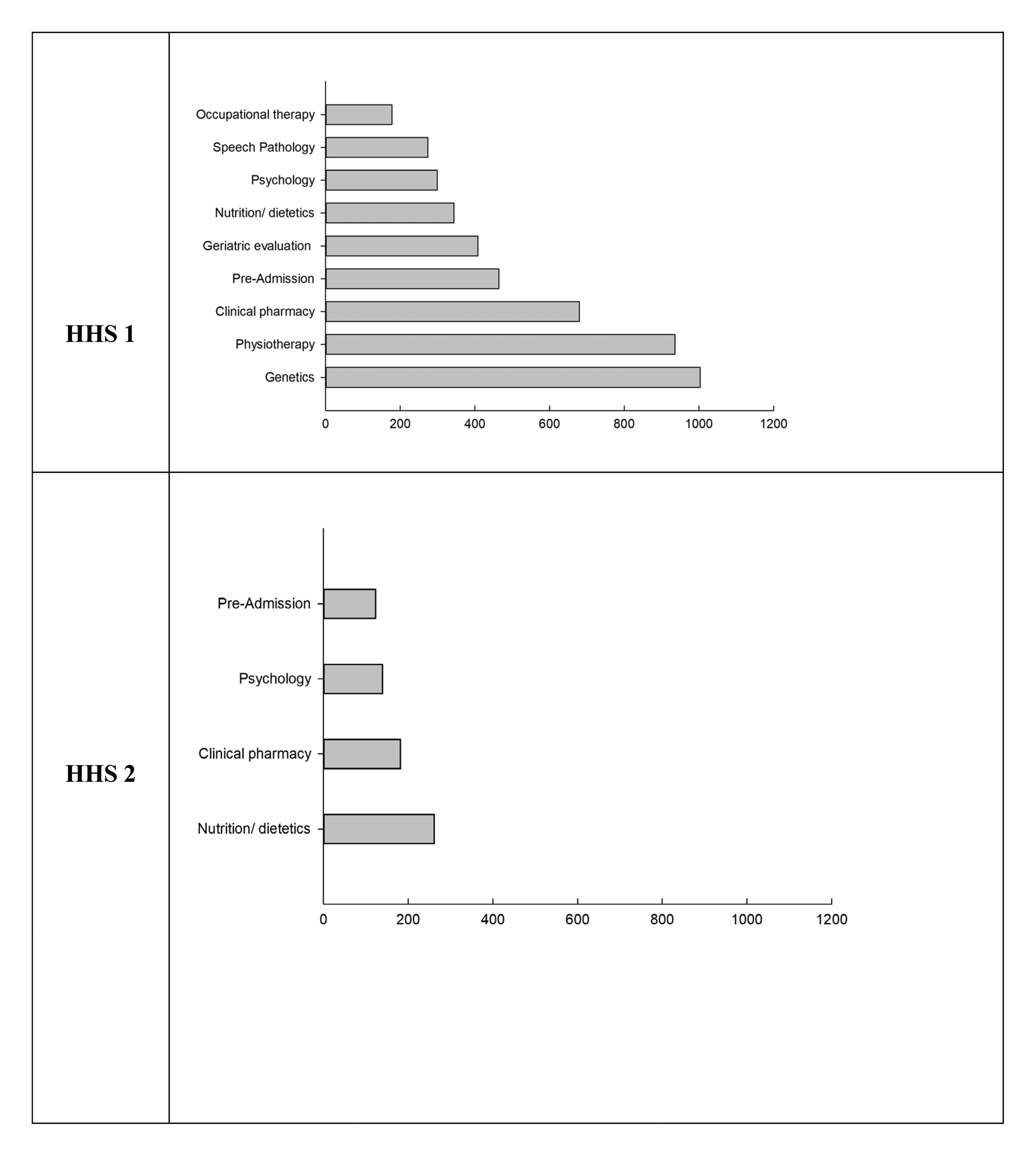
Comparison of telehealth activity between each metropolitan Hospital and Health Service (HHS) by nursing and allied health providers (>100 consultations per year) for year 2018–2019.
Catchment areas of telehealth patients
In general, HHS 1 has more telehealth referrals from coastal areas compared to HHS 2 (Figures 4 and 5), particularly from the highly populated Sunshine Coast and Central Queensland coastal areas. For HHS 2, referrals were more likely to come from sparsely populated regions in Western Queensland. The high activity between HHS 2 and the north west of the state is due to specific service level agreements, not natural referral catchment areas.
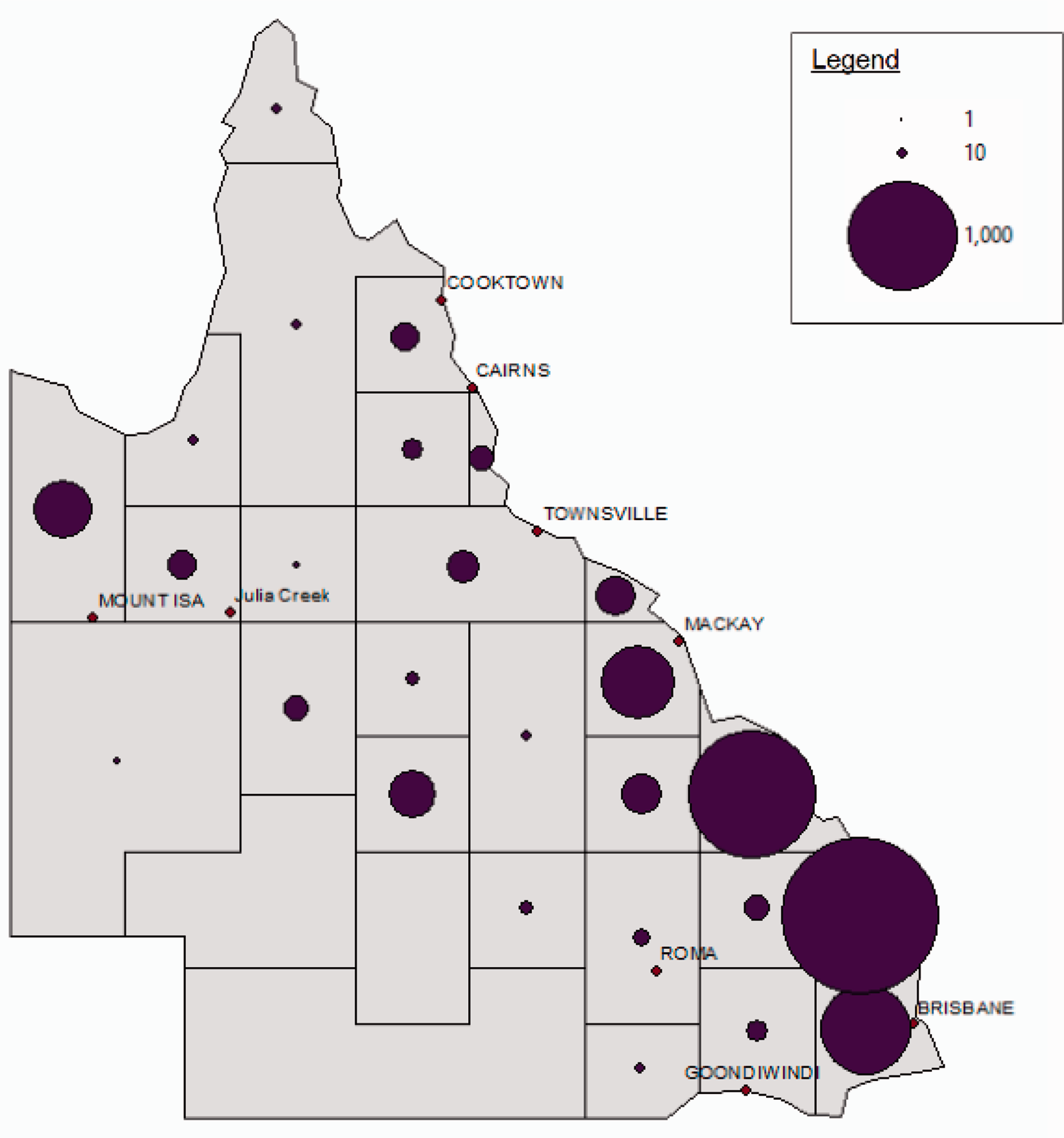
Catchment area of telehealth patients for Hospital and Health Service 1 for year 2018/2019.
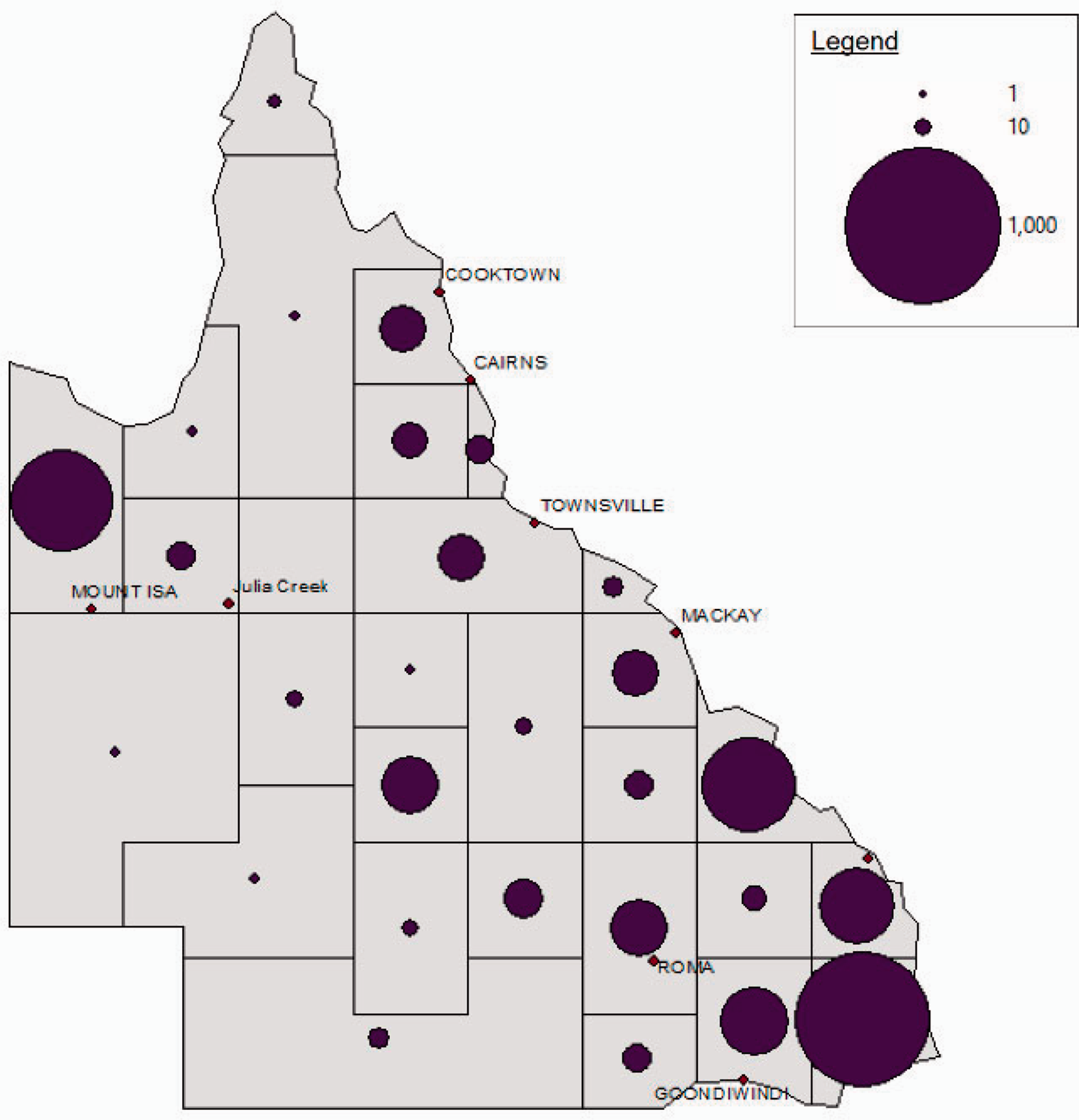
Catchment area of telehealth patients for Hospital and Health Service 2 for year 2018/2019.
Key variables between metropolitan organisations
In total, 29 participants took part in the interviews. Table 2 provides participants characteristics.
Participant characteristics in metropolitan organisations.
HHS: Hospital and Health Service.
Levels of investment
Participants in HHS 1 reported higher levels of investment in telehealth services compared to HHS 2. For example, in 2016/2017 HHS 1 received significant seed-funding (>A$1 m) to expand clinical measurement (use of technology to diagnosing aiding or treating patients), its most active telehealth service. However, a significant barrier to expanding telehealth services in HHS 2 was the cost of providing telehealth capacity using existing computers. One of our issues is actually getting access to the technology, so the technology comes at a cost. It’s not provided for free, so every time you want to set up a computer with a telehealth-enabled consultation room or whatever, that comes at a cost of roughly about $700. So, if you’re working at an outpatient area that has, let’s say, 10 consult rooms, you’re still looking at $7000 to telehealth-enable them, which in current budgetary restraints that can still be problematic. When you have [hospital name] who are only just starting to do telehealth, and their outpatients base has something like 30 consultation rooms, that’s a considerable expense to telehealth-enable them. (Participant 3)
Clinician understanding of the value proposition
Participants at HHS 1 consistently reported the difficulties patients had when travelling from rural areas to attend in-person consultations. They were cognisant of the effect the journey had, not only on the patient but also on the companion or caregiver who accompanied them. They were aware of the cost, and the emotional and physical toll of travelling. This understanding led to a desire to find a solution that met the needs of the rural HHS rather than a fixed model of care. If that procedure can be done at their local facility, to stop them having to travel all that distance, well then that’s what we should be implementing. Because, when these people have to travel, it’s not, you know, they drive 50 km from Ipswich to Brisbane, it is 1000 km, it’s a flight. It’s stop business, down tools, they’re farmers, so everything stops, their revenue goes nowhere, their family come with them, it’s a huge expense to them and the health facility. I don’t think our metropolitan clinicians understand the complexities of what occurs in those rural areas. They don’t go there and so; they don’t fully understand and have not listened. That’s where we have flipped it on its head and listened to them and said, how can we help you; these are some of the models. When we sit down with them, we go, these are all the different ways we can do it. Then they were, we like that, a bit of that and a bit of that and a bit of that, and we go, okay, and we customise it for them based on their knowledge and complexities. (Participant 20)
Communicating the benefits of telehealth
The ability of telehealth staff to communicate the benefits of telehealth to stakeholders was considered highly important for telehealth adoption. In HHS 1 the telehealth staff had high visibility within the organisation and were often located in areas with other hospital staff assisting information to be easily diffused. In addition, there was a higher level of awareness of telehealth throughout the organisation which may be in part be due to the significant funding received. In contrast, the telehealth staff in HHS 2 were located with less incidental opportunity to engage with clinicians and disseminate telehealth information.
IT administration systems
A key difference between the two HHSs is the administration and scheduling of telehealth appointments. HHS 1 has a centralised outpatients service and private practice specialist suites with dedicated administrators organising telehealth appointments across a number of specialties as well as some departments organising their own appointments. For some regular telehealth clinics to run at full capacity, any available appointments are filled with suitable patients who are within the organisation’s catchment area. Patients who are suitable for a telehealth appointment are routinely identified by clinicians. There hasn’t been a lot of in-district [inter-organisation] but there has been circumstances where patients cannot physically get here or transport or financial situation [so they are seen]. Also depends on the referral numbers, sometimes they’re really low and sometimes they come in an influx and they are really high. This impacts on whether we can open it up to more [in district] patients… It also depends on the hospital waitlists and whether hospitals offer services… this all plays a role if the clinician offers the service. (Participant 27)
Rural organisations
In total 34 participants took part in the semi-structured interviews (Table 3).
Participant characteristics in rural organisations.
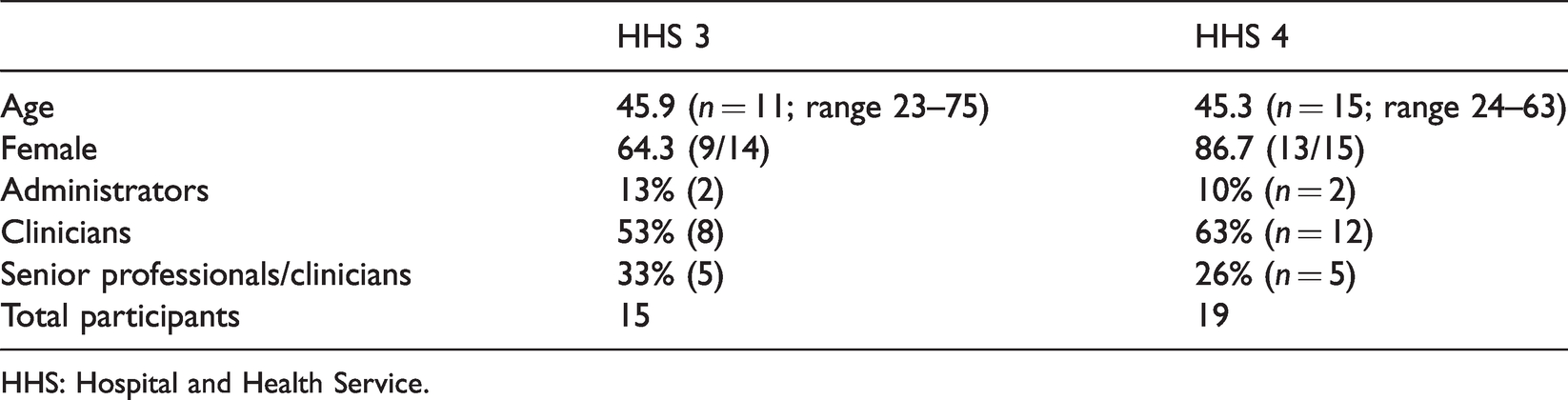
HHS: Hospital and Health Service.
Levels of activity
Both HHS 3 and HHS 4 were predominantly recipients of telehealth activity with HHS 3 having almost double the amount of telehealth activity compared to HHS 4 in years 2018/2019. (Figure 6). A number of high-volume services accounted for this difference such as remote chemotherapy, clinical measures and orthopaedic fracture clinics.
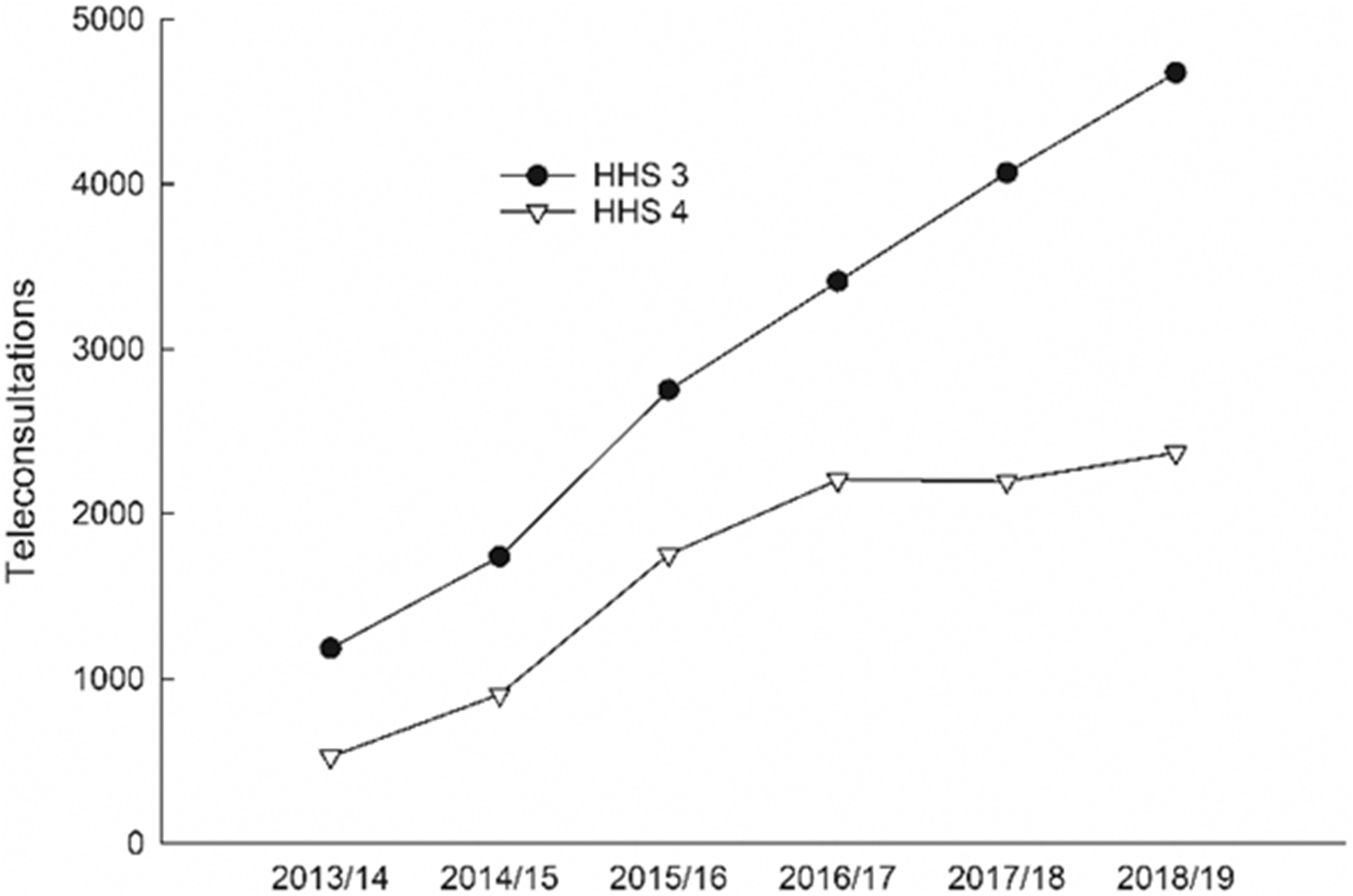
Recipient telehealth service events by rural Hospital and Health Services (HHSs) for years 2013/2014–2018/2019.
At a service level, there were similar levels of recipient services (n=44 and 49) and provider services (n=20 and 18) across the rural HHSs. For recipient services (Figure 7), eight were available in both services (circulatory, oncology, endocrinology primary healthcare, nephrology, general surgery, general medicine and orthopaedics). For provider services (Figure 8), five were the same in both organisations (endocrinology, general medicine, pre-admission, gynaecology and general surgery).
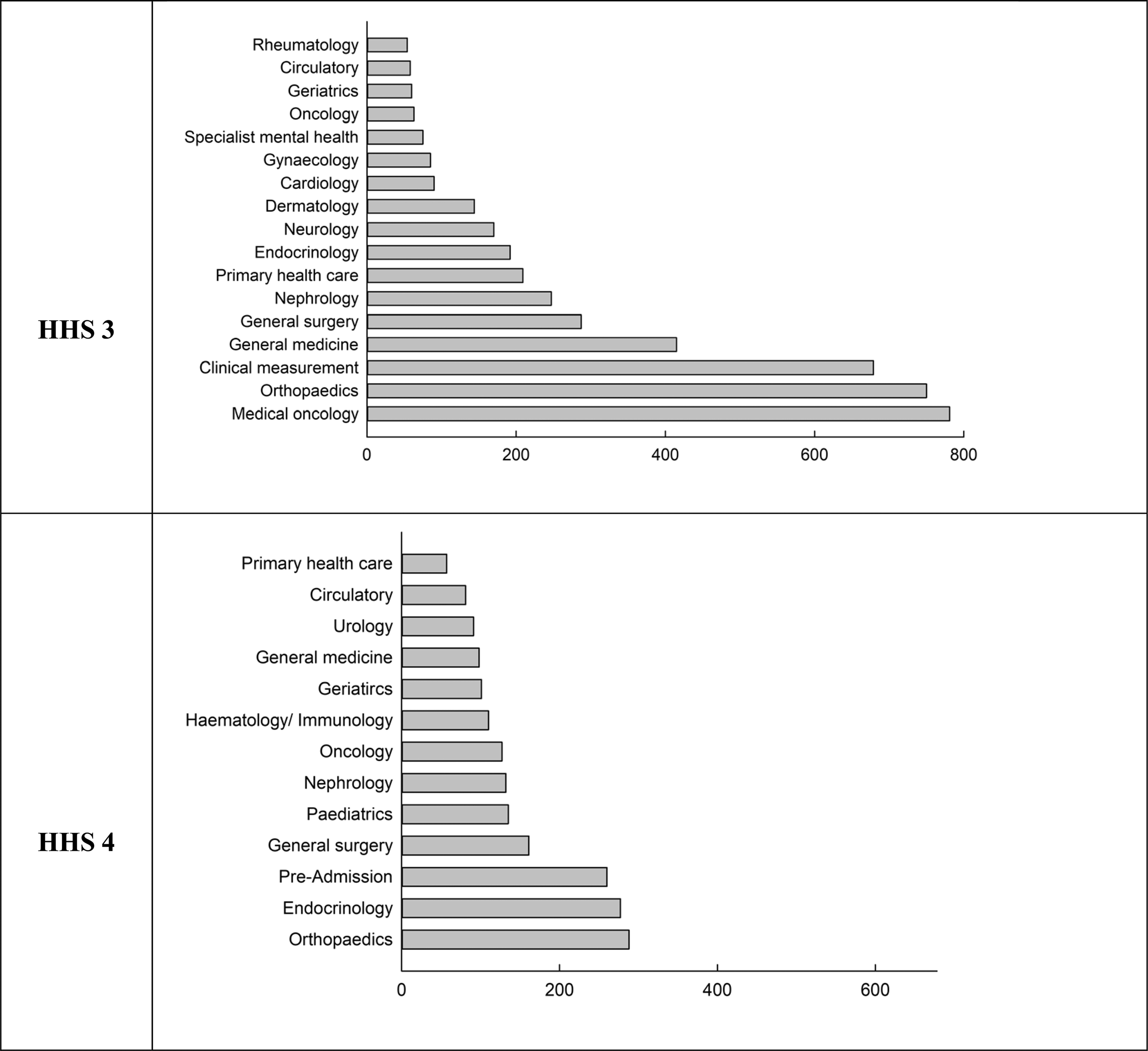
Comparison of recipient telehealth activity (>50 consultations per year) between rural Hospital and Health Services (HHSs) by service for year 2018–2019.
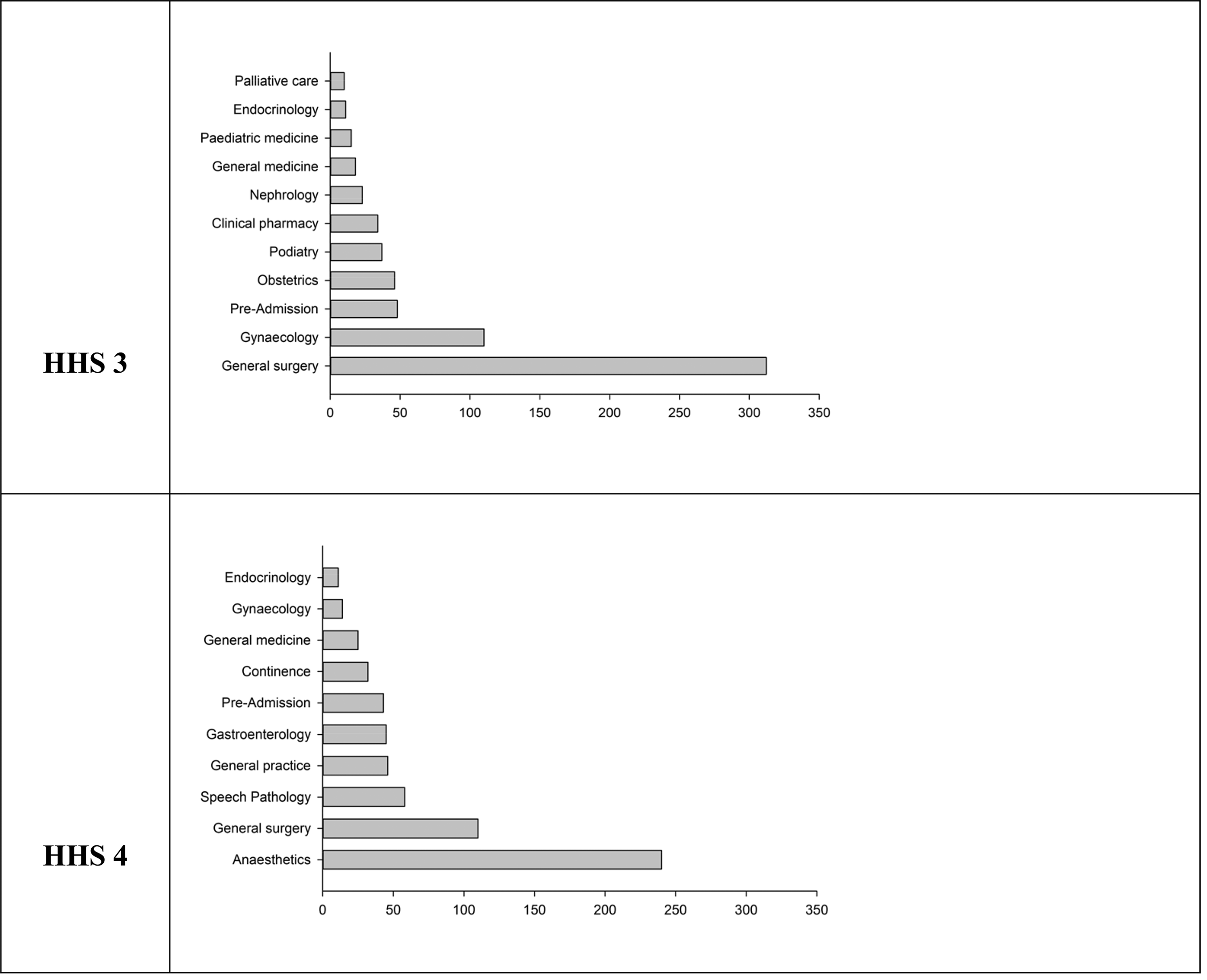
Comparison of provider telehealth activity (>10 consultations per year) between rural Hospital and Health Services (HHSs) by service for year 2018–2019.
Key variables between rural organisations
On-boarding process for clinicians
All external providers of telehealth services are required to be credentialled by each HHS. Credentialing is the process of establishing practitioners qualifications and legitimacy for providing health care. HHS 4 reported a significant amount of telehealth coordination and administration time being used to credential practitioners, leaving very limited time for service development. The credentialing process was a barrier for private specialists to provide consultations by telehealth with participants reporting that rather than completing the process, many specialists would conduct a telehealth appointment with the patient at their general (medical) practitioner surgery instead. One of our biggest barriers is doctors agreeing to be credentialed, particularly private doctors. Every appointment needs to be checked to see if the doctor is credentialed, if not a credentialing request is sent – even if they are a QH doctor, they need credentialing and some are really offended by this. [Also] at some stage the credentialing expires… If the doctor doesn’t reply to the credentialing request and we have to cancel the appointment so then they run down to the GP who will do it because they don’t have credentialing… that’s a problem. (Participant 42)
Clinician willingness to perform telehealth
Clinician reluctance to change practice at both at inter- and intra-organisation level was reported in both HHSs, but at a far greater level in HHS 4. HHS 4 reported great difficulty in getting clinicians at metropolitan provider sites to use telehealth compared to HHS 3. In particular, private specialists often refused to undertake appointments including follow-up appointments by telehealth. In addition, there was limited drive or impetus for clinicians to support telehealth appointments within their own service and explore change management. If you don’t have the doctors that will do it [telehealth] – that is where it is blocked. If you cannot get the doctors on board in metropolitan areas to do the service, our hands are tied and that is what makes it hard. (Participant 50) [We need to be] improving the motivations and uptake of clinicians and services outside of the [rural HHS area]. Connectability is so easy there is really is no excuse for not using telehealth. There is a lot of push back from specialists particularly private specialists – they don’t give you an answer why they can’t do it, I think they are so stuck in their ways of making people come to them. (Participant 54)
Strategic challenges
Both organisations were supportive of telehealth but reported a range of challenges in driving its use forward. There were more structural barriers identified in HHS 4. These included out of area providers not wanting to undertake telehealth appointments, clarity on out-of-catchment area referrals and service development.
Telehealth activity in primary care
In HHS 4 the barriers created by the credentialing process for specialists to perform telehealth activity in the public hospital appears to have pushed telehealth activity into private practice primary care. Therefore, telehealth activity is taking place within the area but is not captured in the data presented in this study. One general practitioner (GP) reported performing on average 10 telehealth consultations a week with haematologists and additional consultations with other specialists. In contrast, telehealth activity in primary care was not reported in HHS 3.
Discussion
This was a multi-methods case study comparing two matched metropolitan organisations and two matched rural organisations with differing levels of telehealth activity within the public hospital system. It sought to identify key characteristics between the matched organisations that are potentially modifiable to increase adoption of telehealth.
For metropolitan organisations, key differences in supporting telehealth uptake were, levels of investment for service delivery, referral catchment areas which were more densely populated, booking and administration systems, communicating telehealth’s benefits and clinician’s understanding of the value proposition. For rural organisations, key differences in telehealth activity were affected by on-boarding processes, clinician resistance, strategic barriers and telehealth activity in primary care.
Clinician adoption
A key theme across both metropolitan and rural organisations centred on clinicians' willingness to undertake telehealth consultations. 4 In metropolitan organisations telehealth services were delivered by 34 medical specialties, of which only nine were the same in both organisations. When both metropolitan services offer in-person specialist services in a particular discipline but only one offers the service via telehealth then this would suggest that clinician preference is driving telehealth rather than clinical necessity.
Although there is a strategic vision for digital health in Queensland, 22 there are currently no quantifiable targets set for volume or saturation of telehealth services. The decision on whether to perform telehealth or not remains a decision made by the clinician. In light of COVID-19 and the rapid increase in telehealth activity, setting targets for the number of consultations may now be more acceptable.
In metropolitan organisations, higher activity occurred when the benefits of telehealth were well communicated and understood by clinicians. Rural organisations reported a significant barrier with clinicians in metropolitan areas. Many metropolitan clinicians are not always aware of the impact on patients when travelling long distances to attend appointments. Being able to motivate clinicians to adopt telehealth and challenge their resistance to clinically appropriate telehealth consults is important. Fully articulating the value proposition for rural patients is necessary – the burden of travel such as the physical strain, the amount of time, overnight stays, different modes of travel, requiring a companion and the impact on the companion such as taking time off work or arranging care for dependents or farming responsibilities.
Encouraging, persuading and articulating the benefits for the patient is a soft skill and an important change management mechanism 23 that has not received much attention within the telehealth literature. Overcoming clinician resistance to deliver consultations which are appropriate for telehealth could learn from public health behaviour change theories. For example, The transtheoretical stages of change model provides a framework to explore barriers to change and provide tailored information to move people through the change process.24,25 For example, if a clinician is in a precontemplative stage of change and not interested in using telehealth, messages that improve their understanding of the benefits for patients and how other services have successfully used telehealth would be more effective to change their perception rather than providing information on how to deliver a telehealth consult. Although primarily used to elicit changes in patient’s health behaviours, the stages of change model may be beneficial in changing clinician willingness to practice. The model emphasises that change is a process that requires nuanced messages and information at different stages of the change process. 24
Organisational strategic decisions
Research on telehealth has mostly focused on patient outcomes, cost-effectiveness or technical feasibility. 26 Less research has concentrated on an organisation’s role in supporting service development. 27 A clear organisational vision supports successful telehealth implementation.28–30 In our study, the majority of factors influencing activity were at an organisational level: levels of investment, referral areas, strategic challenges and onboarding processes. There would appear to be some tension between the organisation strategic policy to support telehealth with underlying policy necessary for telehealth implementation.
Activity increased following a significant level of investment in telehealth services. Activity was also higher when telehealth capacity was across two tertiary centres compared to just one centre. Investment in telehealth is vital to secure widespread use. Funding streams need to be long-term and focused on both infrastructure and personnel. Without strategic commitment from organisations and governments to fund the development and growth of telehealth services, adoption and expansion will be contained. 31
Referral routes, booking and administration systems and processes influenced activity level differences. Changes in usual care workflow are required to implement telehealth.32,33 Logistical factors associated with the delivery of telehealth services, such as scheduling and administration can take longer than in-person consultations. 34 Scheduling software differed between organisations resulting in using emails and phone calls to organise appointments. A lack of access to a shared electronic medical record resulted in clinicians and administrators collating health information from several systems to prepare for an appointment. Previous research has shown that a shared electronic medical record is a key factor positively affecting the adoption of telehealth. 35 Efficiency gains could be made by ensuring technology integrations work across organisations. In addition, cost savings could be made if processes which took significant time, such as credentialing, were statewide rather than by individual organisations.
This study has several limitations. First, this work was undertaken prior to the current COVID-19 crisis and the impetus and context for using telehealth has now changed.31,36,37 However, to support the sustainability of telehealth’s rapid adoption and ensure it is embedded into usual care, the issues identified in this study will require addressing. 38 Second, for the referral catchment areas, we were unable to report data per capita because each HHS receives out-of-area referrals and therefore using the population data for each area would be misleading. Third, the scope of this study does not include telehealth related to mental health, which is substantial, as it does not fall within the remit of Clinical Excellence Queensland who commissioned the research.
Conclusion
Telehealth has an important role in supporting a broad range of health services, and its adoption is influenced by specific factors at individual and organisational levels. To support telehealth expansion, organisations need strategic intention, a clear vision, a change management plan and dedicated funding. This study highlights the need to view telehealth adoption from a ‘whole of system’ perspective, as factors which improve adoption and expansion transcend organisational boundaries.
Footnotes
Acknowledgement
We thank Ms Monica Taylor (MT) for expert support on this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.