
Abstract
Introduction
Telehealth is an applicable, acceptable, cost-effective, easily accessible, and speedy method for pregnant women. This study aimed to examine the impact of telehealth applications on pregnancy outcomes and costs in high-risk pregnancies.
Methods
Studies were selected from PubMed, Science Direct, Web of Science, EBSCO, Scopus, and Clinical Key databases according to the inclusion and exclusion criteria from January to February 2021. Cochrane risk-of-bias tools were used in the quality assessment of the studies.
Results
Four observational and eight randomized controlled studies were included in this meta-analysis (telehealth: 135,875, control: 94,275). It was seen that the number of ultrasound (p < 0.01) and face-to-face visits (p < 0.01), fasting insulin (p < 0.01), hemoglobin A1C before delivery (p < 0.01), and emergency cesarean section rates (p = 0.05) were lower in the telehealth group. In the telehealth group, the women's use of antenatal corticosteroids (p = 0.03) and hypoglycemic medication at delivery (p = 0.03), the total of nursing interventions (p < 0.01), compliance with actual blood glucose measurements (p < 0.01), induction intervention at delivery (p = 0.003), and maternal mortality (p < 0.001) rates were higher. Two groups were similar in terms of the use of medical therapy, total gestational weight gain, health problems related to pregnancy, mode and complications of delivery, maternal intensive care unit admission, fetal-neonatal growth and development, neonatal health problems and mortality, follow-up, and care costs.
Discussion
Telehealth and routine care yielded similar maternal/neonatal health and cost outcomes. It can be said that telehealth is a safe technique to work with in the management of high-risk pregnancies.
Introduction
Pregnancy is a critical period in a woman's life, one in which she experiences a range of physical, mental, and social changes. When the mother and/or fetus are at high risk of pregnancy or birth complications, the period is defined as high-risk pregnancy. 1 High-risk pregnancy necessitate closer monitoring and multidisciplinary care. 2 In February 2020, the World Health Organization (WHO) announced that coronavirus disease 2019 (COVID-19) had broken out in 2019, declaring that the disease was rapidly spreading throughout the world. 3 During the period of the pandemic, face-to-face visits created a risk for pregnant women and health professionals in terms of exposure to the virus, becoming a source of anxiety and eventually leading to an increased use of telehealth services at many hospitals. Data can be found in many studies on the use of telehealth applications in high-risk obstetric care over the period of the pandemic.4,5 Under the circumstances, the matter of implementing telehealth applications in caring for cases of high-risk pregnancy is an important issue that must be evaluated.
High-risk pregnancy can be caused by chronic health problems such as diabetes or high blood pressure, also by infections, complications stemming from previous pregnancies, or from other issues that may emerge during a current pregnancy. 2 About 22% of pregnant women are beset by some kind of high-risk condition. 6 Women going through a high-risk pregnancy may have a need for special monitoring, care, or treatment for a safe and healthy pregnancy and delivery. The type of health service needed depends not only on certain risk factors, but can also change according to the general health condition of the mother and fetus. 2 The management of a high-risk pregnancy then may need an individualized and innovative approach. 7 One of these innovative approaches is “telehealth,” which is being increasingly employed in recent years.8–11 Researchers have reported in their studies that telehealth is an applicable, acceptable, cost-effective, easily accessible, and speedy method to use in the monitoring and treatment of pregnant women at high risk.1,8,12
Telehealth has a long history behind it, but the technique began to take hold at the end of the 1980s in parallel with the advances in digital communication and the development of low-cost computers. 11 Today, telehealth is being used more and more in the monitoring and management of high-risk pregnancies, especially in the case of women with diabetes or high blood pressure.13–15 It is observed that telehealth is not only used in developed states, but also in low or middle-income countries as a technique that caters to prenatal care in rural areas where access to care is limited. 16 With the emergence of the COVID-19 pandemic, telehealth found widespread attention, particularly in the area of antenatal care. Indeed, many international health organizations have recommended the heightened use of telehealth applications for pregnant women and health professionals providing health services with an eye to reducing transmission of the virus during the pandemic.3,17–19 Besides the COVID-19 pandemic, other natural disasters and infectious pandemics are likely to reoccur in the future, although the time of occurrence cannot be predicted. Telehealth has a critical role in emergency response in such pandemic situations.20,21
Evidence suggests that the use of telehealth can be equivalent or more clinically effective when compared to usual care in medical disciplines. 22 Among the health disciplines, risky pregnancy monitoring is one of the areas where telehealth is widely used. There are many international studies of different research designs that probe into the use of telehealth in the monitoring and treatment of women with high-risk pregnancies.8,23–25 It has actually been seen that due to the COVID-19 pandemic, the use of telehealth applications in the monitoring and care of high-risk pregnancies has increased substantially in antenatal health services. It is for this reason that the need arose for a strong evidence-based examination of the effectiveness of telehealth, and this became the basis for the planning of the present study. The data obtained are expected to contribute to the improvement of antepartum care services as well as to the accumulation of knowledge in the national and international literature.
Aim and research questions
The aim of the study was to examine the impact of telehealth applications on pregnancy outcomes and costs in high-risk pregnancies. The research question to be answered was, “What is the impact of telehealth applications on maternal, neonatal health outcomes and costs in cases of high-risk pregnancy?”
Methods
In conducting our study and preparing our report of this systematic review and meta-analysis, we followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA). 26 The protocol of this systematic review and meta-analysis was registered on the PROSPERO database (Trial Registration Number: CRD42021241115). To keep the risk of bias under control during the study, two researchers carried out the literature search, selection of articles, data extraction, and quality assessment of the included articles independently. In the case of disagreement on any matter, all of the researchers were brought together for a discussion and a final consensus. At the same time, prior to the start of the research, all of the authors participated in a pilot study for each stage of the study to concur on a road map to follow. During the study, no situation requiring deviation from the protocol was encountered and the study was terminated in line with the protocol entered into PROSPERO database.
Eligibility criteria
We included in our study accessible full texts of articles published in English and Turkish over the period 2016–2021. The following criteria were considered (PICOS) in selecting the studies to be included in the research:
Participant (P): Pregnant women are at high risk. The women recruited into the study displayed the following criteria for high-risk pregnancy: (1) obstetric risk (e.g. multigravida, multiple pregnancies, early or later-age pregnancy, placental location anomalies, miscarriage, early membrane rupture, and bleeding), (2) medical conditions (e.g. diabetes mellitus, hypertension, preeclampsia, epilepsy, anemia, cardiac diseases, deep vein thrombosis, asthma, thyroid diseases, and obesity), (3) infectious diseases (e.g. HIC, hepatitis A, hepatitis B, rubella, varicella, and COVID-19), (4) genetic disorders (e.g. hemoglobinopathy, congenital defect in previous birth, familial history of genetic disease, and uterine anomaly), (5) behavioral risks (e.g. use of alcohol, electronic nicotine or cigarettes, opioid, cocaine or similar drug addiction), and (6) lack of social support (e.g. domestic violence, deficiency in health services).17,27
Intervention (I): Telehealth methods: These are interventions through communication tools such as smartphones, computers, two-way videos, wireless devices, tracking devices, and other tools such as emails, speaking and message delivery systems.28–30
Comparison (C): Routine care.
Outcomes (0): Primary outcomes were prenatal care and follow-up, additional health problems related to pregnancy, type of delivery, labor interventions, complications at birth, admission to the intensive care unit, maternal mortality, birth weight, outcomes of fetal-neonatal growth and development, neonatal health problems, admission to the neonatal intensive care unit or special care nursery, neonatal mortality, absenteeism at work, follow-up, and care costs. The secondary outcomes were the gestational week when the insulin therapy was started, the use of medical therapies, diet and weight gain, compliance and blood glucose measurements, the management of asthma.
Study design (S): Randomized, controlled, experimental, quasi-experimental, and observational studies with control groups (retrospective, cohort, and case–control) were included.
Studies that did not define two-way interactions between healthcare personnel and pregnant women as well as traditional and systematic reviews were excluded.
Search strategy
The literature search for this systematic review was carried out over the period January–February 2021 on the PubMed, Science Direct, Web of Science, EBSCO, Scopus, Clinical Key, and Ulakbim databases. The keywords used were “high risk pregnancy” and “telehealth.” Additionally, to reach more studies, the reference lists of systematic reviews carried out on the included articles and other previous systematic reviews were checked.
Study selection
The selection of possible studies to be included was made after repeats appearing in the scan of the literature were removed, and on the basis of headings, abstracts, and full texts.
Data extraction
A data extraction instrument developed by the researchers was used to obtain the study data. With this data extraction tool, data on the place and year of the study, year of publication, research design, sample size, mean age of mothers, type and mode of telehealth applications, the effects of telehealth on maternal and neonatal health, and costs in the studies included in the systematic review and meta-analysis were obtained.
Evaluation of the methodological quality of the studies
The quality of the articles in randomized controlled studies were assessed with Version 2 of the Cochrane Risk-of-Bias tool for randomized trials (RoB-2) 31 and in observational studies with the Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I). 32
Data analysis
The meta-analysis was performed using Review Manager 5.4 (The Nordic Cochrane Center, Copenhagen, Denmark) for the data analysis. Heterogeneity between studies was assessed using Cochran's Q test and Higgins’ I², with I² greater than 50% considered to indicate significant heterogeneity. Accordingly, when I² was greater than 50%, the random effect results, and if the value was less, the fixed effect results were considered. The odds ratio (OR) was calculated for categorical variables, mean difference (MD) and standardized mean difference (SMD) were calculated for continuous variables. MD or SMD along with corresponding 95% confidence interval (CI) were pooled for continuous variables appropriately, according to whether the outcomes were measured by the same scales or not. All tests were calculated from two-tailed tests, and a p-value of less than 0.05 was considered statistically significant.
Results
Search results
At the beginning, the results of the scan yielded 2463 records from the databases and 11 from additional scans, a total of 2474 records. With the exclusion of the records that were repeats, the review carried out according to heading and abstract yielded the full texts of 39 articles. Following the examination of the full texts, 12 articles were taken into the meta-analysis (Figure 1).
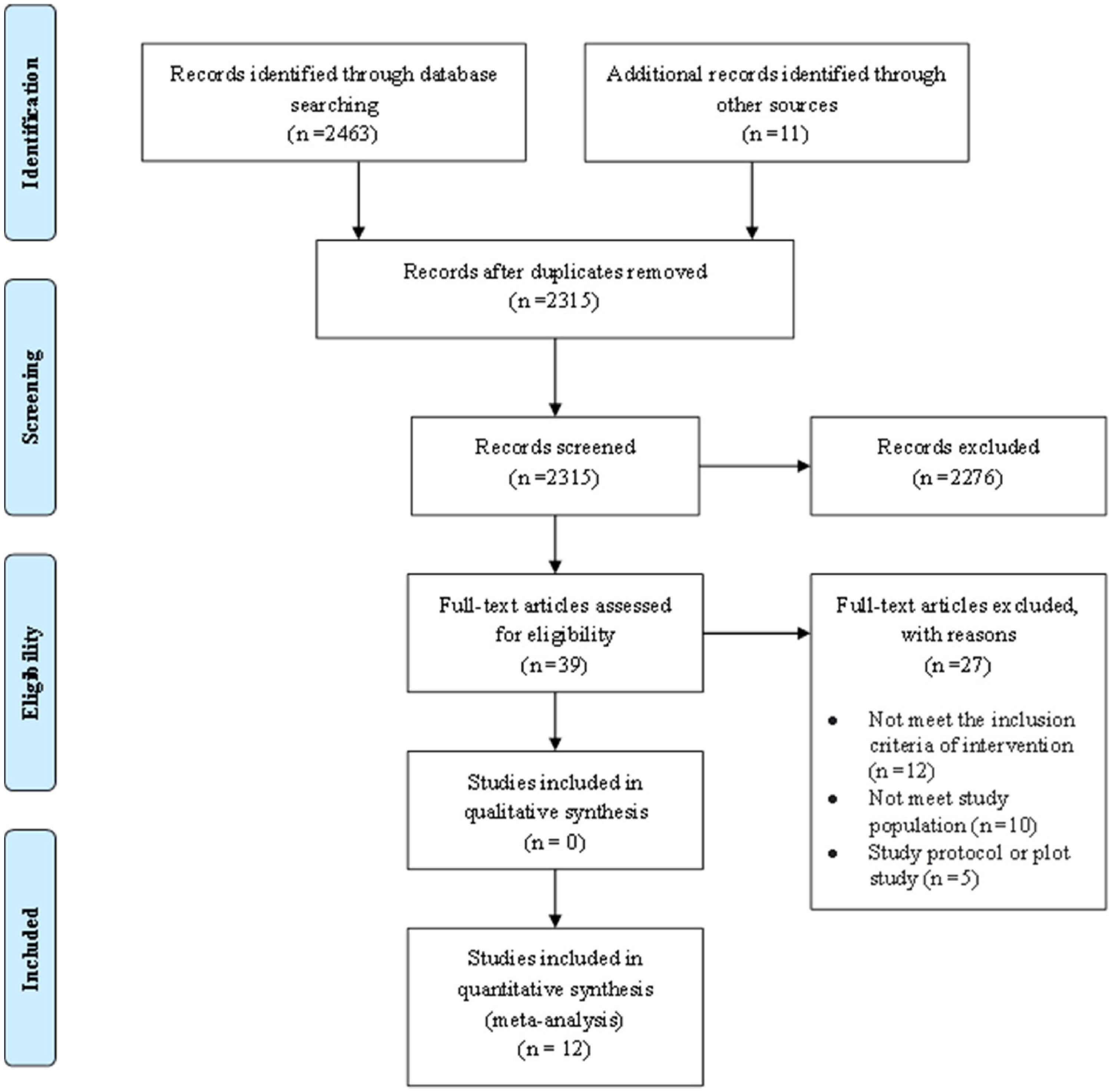
PRISMA flow diagram.
Study characteristics
All of the studies (n = 12) had been published in English. Eight of the articles were randomized controlled experimental studies, four were observational (quasi-experimental with controls, retrospective cohort, and case–control) studies. It was noted that the study data had been collected over the period 2012–2018 and published over the period 2016–2020. It was reported that the studies had been conducted in China (n = 3), the United States (n = 1), Australia (n = 2), United Kingdom (n = 1), Canada (n = 1), the Netherlands (n = 1), Israel (n = 1), Spain (n = 1), and Saudi Arabia (n = 1) (Table 1).
Characteristics and main findings of the studies included in the systematic review and meta-analyses.

APGAR: activity – pulse – grimace – appearance – respiration; FPG: fasting plasma glucose; GDM: gestational diabetes mellitus; GWG: gestational weight gain; IOM: Institute of Medicine; LGA: large gestational age; NST: non-stress test; NICU: neonatal intensive care unit; PPG: postprandial plasma glucose; RCT: randomized control trial; SGA: small gestational age.
High-risk groups: Scar uterus, hepatitis B virus, miscarriage, BMI ≤ 18, BMI ≥ 25, age ≥ 35 years old, diabetes, normal< ALT< 100 IU, hypothyroidism is required medication, anemia.
From among the studies included in this analysis, eight were reported to be carried out with women with gestational diabetes mellitus,24,33–39 two with women with multiple diseases (chronic hypertension, history of preeclampsia, or maternal cardiac or kidney disease, scarred uterus, hepatitis B virus, miscarriage (natural, artificial) ≥2 times, body mass index (BMI) ≤ 18, BMI ≥ 25, age ≥ 35 years old, diabetes, normal< ALT< 100 IU, medication-required hypothyroidism, and anemia),7,40 one with women with asthma, 41 and one with overweight or obese women. 42
The types of telehealth methods reported to have been used in the studies included in this systematic review and meta-analysis were smartphone applications in seven,7,24,33,35,37,39,41 a web-based platform in four studies34,36,38,40 and telephone call sessions in one study. 42
The total volume of the sampling consisted of 230,150 studies (telehealth: 135,875, control: 94,275). Sample size in the telehealth groups varied from 27 33 to 134,884, 7 and in the control groups from 29 34 to 93,465 7 (Table 1).
Quality assessment results of the studies
Four of the articles included in the review were evaluated with the ROBINS-1, eight with the RoB-2 tools. A high level of bias was found in three of the randomized controlled studies,34,37,38 “some concerns” regarding bias were seen in another three of the studies,33,35,42 and a low bias risk was observed in two studies24,41 (Figure 2). Observers reported serious risk of bias in two studies7,40 and moderate risk of bias in another two studies36,39 (Figure 3).
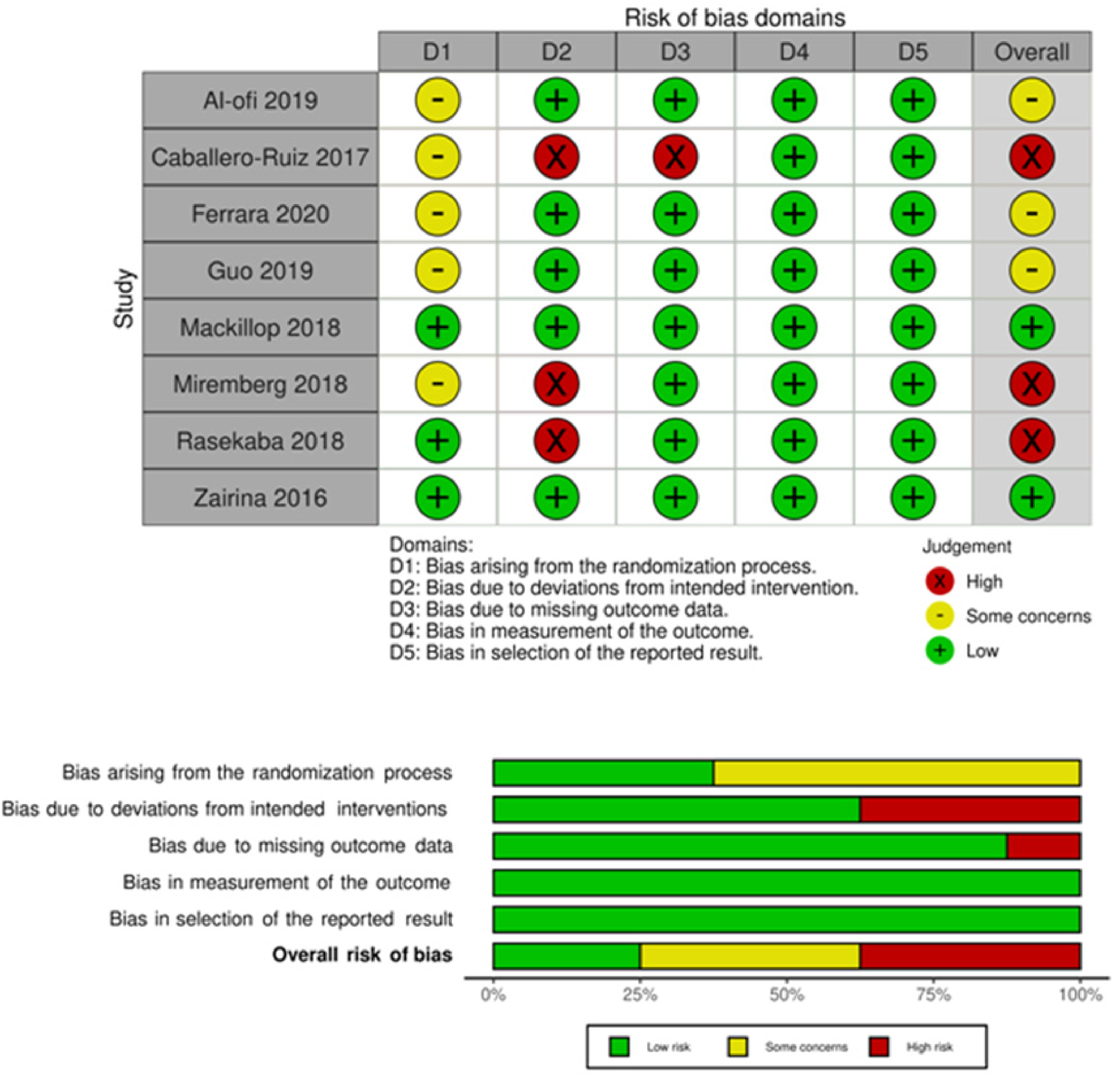
Risk of bias domains: ROB-2.
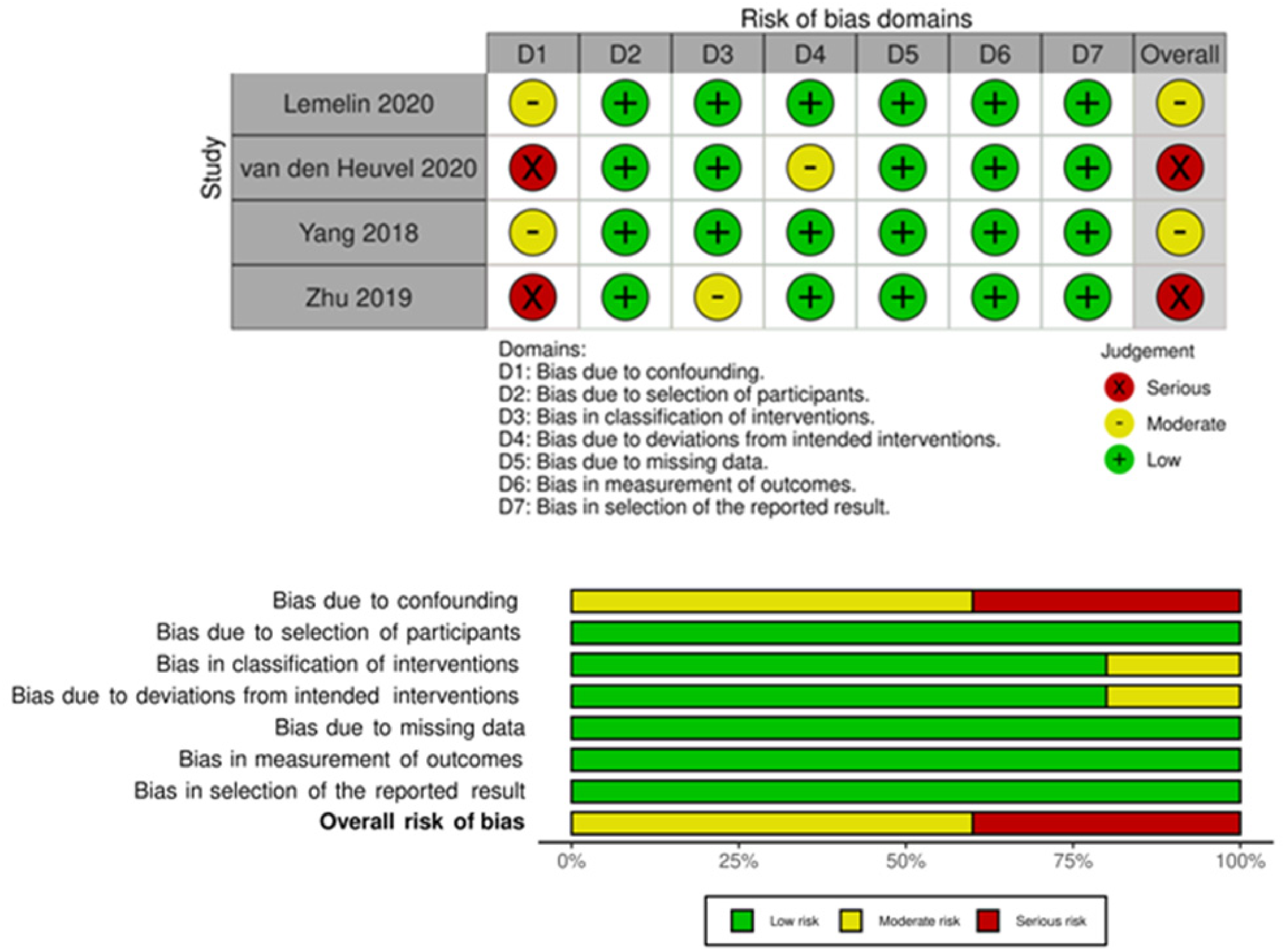
Risk of bias domains: ROBINS-1.
Results of the meta-analysis
Effect of telehealth on the use of medical therapy
The authors of one of the studies reviewed 34 reported that the difference between the telehealth and control groups was not statistically significant in terms of the gestational week when insulin therapy was started (MD: 1.45, 95% CI:−1.64 to 4.55, Z = 0.92, p = 0.36). In five studies, the authors reported results from the use of medical therapy.24,34,36,37,40 The pooled results of the studies indicated no significant difference between the groups in terms of the use of medical therapy (OR: 1.17, 95% CI: 0.82 to 1.68, Z = 0.86, p = 0.39). In the subgroup analysis according to the type of medical therapy, it was found that the difference between the use of antenatal corticosteroids (OR: 2.20, 95% CI: 1.07 to 4.54, Z = 2.13, p = 0.03) and hypoglycemic medication at delivery (OR: 0.51, 95% CI: 0.28 to 0.95, Z = 2.14, p = 0.03) was statistically significant (Figure 4a–b).
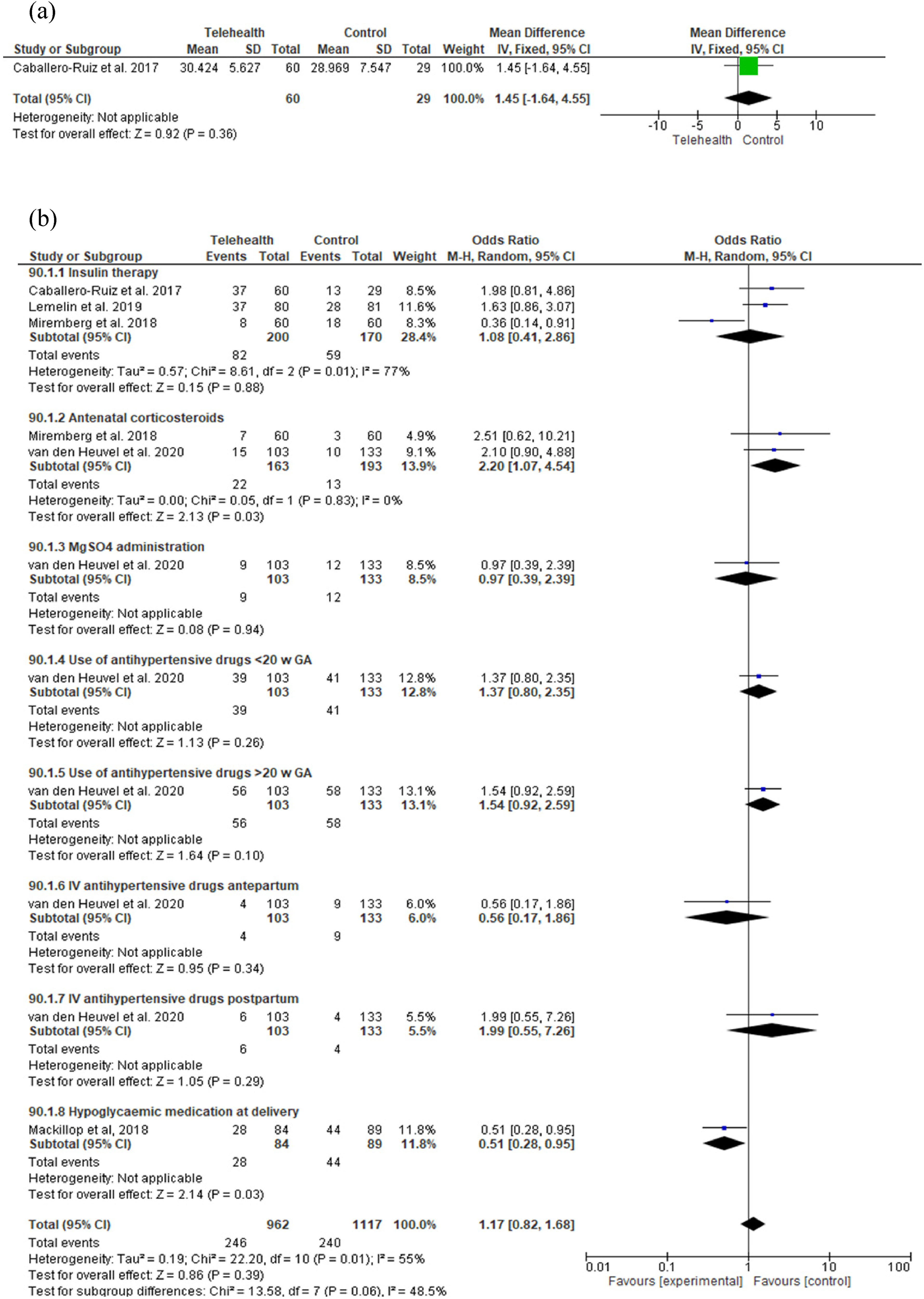
Meta-analysis results on the effect of telehealth on the use of medical therapy: (a) Gestational week when the insulin therapy was started and (b) use of medical therapy.
Effect of telehealth on prenatal care and follow-up
The effect of telehealth on the number of face-to-face visits was examined in five studies.24,34–36,40 When the pooled results were compared with the control group, the mean number of face-to-face visits in the telehealth group was seen to be significantly less (MD: −2.09, 95% CI: −2.98 to −1.19, Z = 4.57, p < 0.01). In another study, 36 it was reported that there was a significant difference between groups in terms of the number of nursing follow-ups by telephone (MD: 1.90, 95% CI: 1.48 to 2.32, Z = 8.85, p < 0.01) and the total number of nursing interventions (MD: 9.40, 95% CI: 8.69 to 10.11, Z = 26.04, p < 0.01); there was however no difference in terms of the number of nonstress test (NST) visits. The authors of another study 40 reported that the number of ultrasounds taken in the telehealth group was statistically and significantly less than in the control group (MD: −1.10, 95% CI: −1.82 to −0.38, Z = 3.00, p < 0.01). The authors of another two studies reported one or more instances of a need for emergency obstetric care.36,40 According to the results of the meta-analysis, there was no significant difference between the two groups in terms of the number of instances in which emergency obstetric care was received (Figure 5a–g).
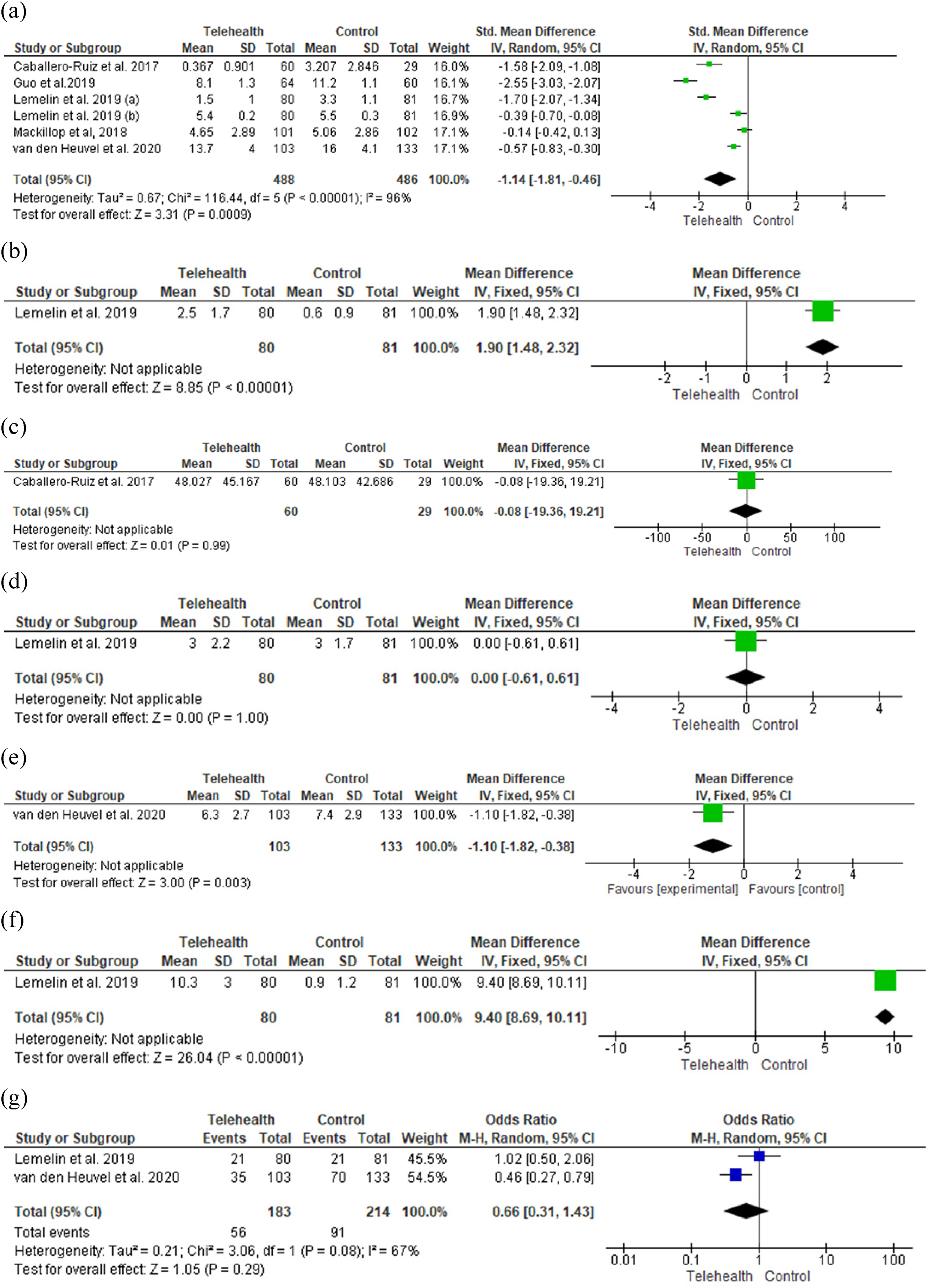
Meta-analysis results related to the effect of telehealth on prenatal care and follow-up: (a) Number of face-to-face visits, (b) number of nursing follow-up(s) by telephone, (c) the global time (Tglo) devoted to patients considering also face-to-face visits, (d) visits for NST, (e) total number of ultrasound assessments, (f) total of nursing interventions, and (g) patients with ≥1 visit to the OB emergency.
Effect of telehealth on diet and weight gain
In five studies examined in the systematic review and meta-analysis, results had been reported on the effect of telehealth on weight gain and diet during pregnancy.24,35–37,42 The pooled results indicated no difference between groups in terms of weight gain after treatment, excessive weight gain weekly and during pregnancy, and total gestational weight gain. On the other hand, in the telehealth group, it was determined that the probability of weekly weight gain being below the Institute of Medicine (IOM) criteria was 2.83 times greater and this was observed to be statistically significant (OR: 2.83, 95% CI: 1.50 to 5.34, Z = 3.22, p < 0.01) (Figure 6a–e).
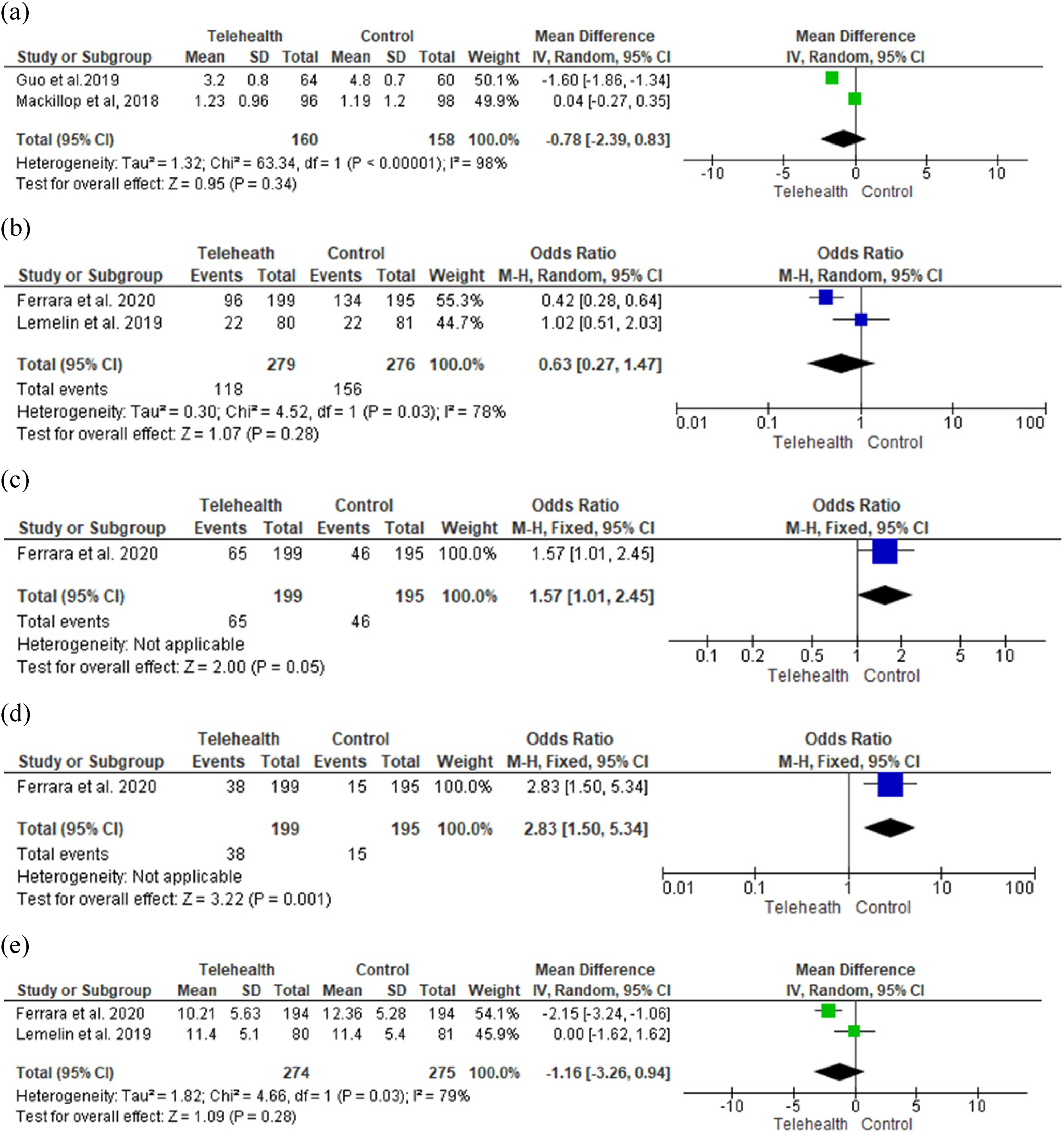
Meta-analysis results related to the effect of telehealth on diet and weight gain: (a) Weight gain after treatment, (b) excessive weight gain weekly and during pregnancy, (c) meeting IOM weekly rate or total during pregnancy of gestational weight gain, (d) below IOM weekly rate of gestational weight gain, and (e) total gestational weight gain (kg)—among all women.
Effect of telehealth on compliance and blood glucose measurements
Two studies included in our study contained reports of compliance and blood glucose results.35,37 The pooled results of these studies showed that the telehealth intervention had a positive and statistically significant impact on compliance and actual blood glucose measurements (MD: 15.86, 95% CI: 10.92 to 20.79, Z = 6.30, p < 0.01). Again, the number of blood glucose measurements was examined in two studies,24,34 mean fasting plasma glucose in three studies,33,39,42 fasting insulin in one study, 42 and hemoglobin A1C (HbA1C) before delivery in another. 35 The pooled results showed that the telehealth and control groups were similar in terms of the number of blood glucose measurements and mean fasting plasma glucose levels, but it was seen that telehealth produced a reducing effect on fasting insulin and levels of HbA1C before delivery (respectively, MD: −9.30, 95% CI: −14.95 to −3.65, Z = 3.22, p < 0.01; MD: −0.60, 95% CI: −0.69 to −0.51, Z = 13.02, p < 0.01) (Figure 7a–e).
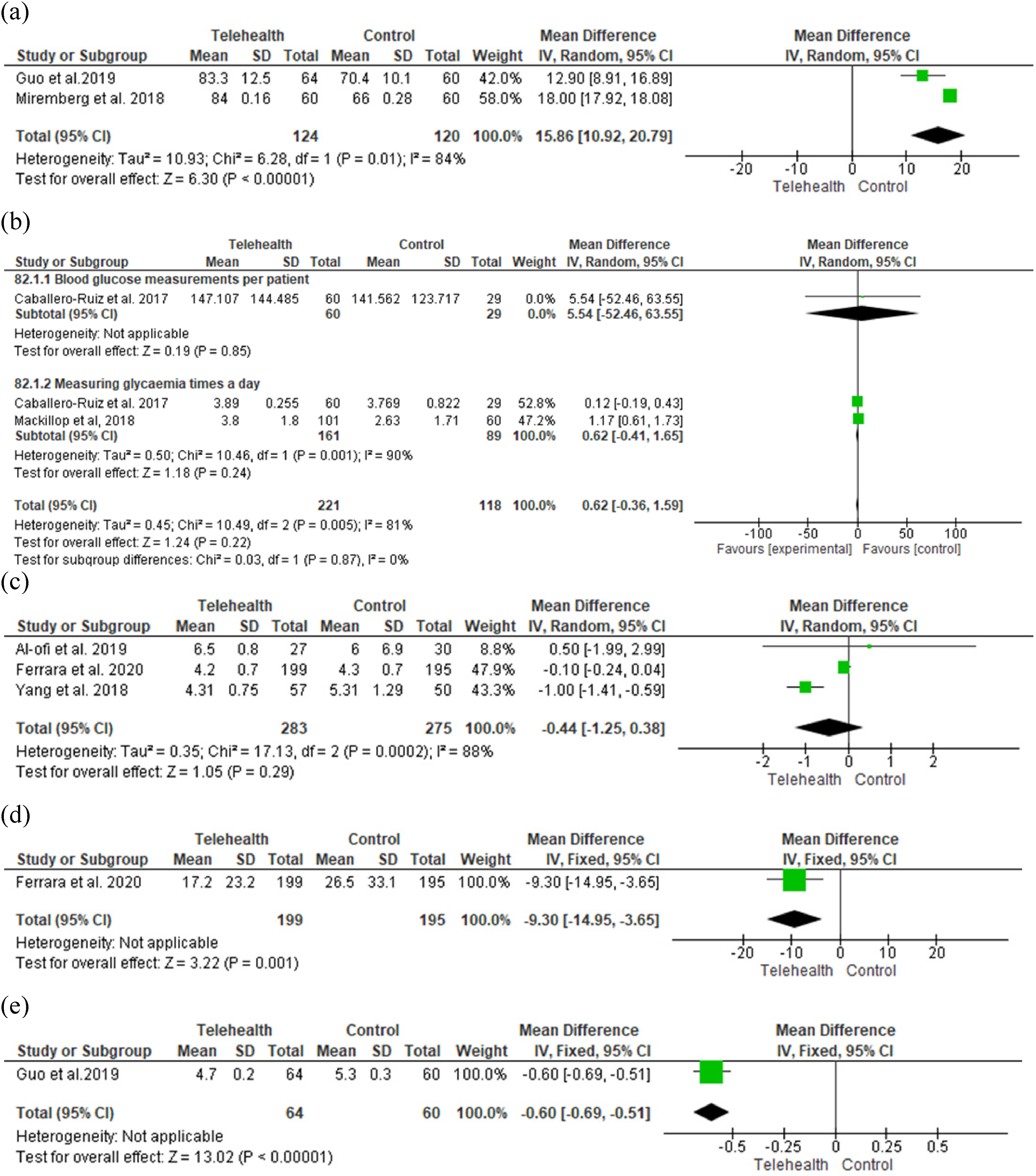
Meta-analysis results related to the effect of telehealth on compliance and blood glucose measurements: (a) Compliance (%): The actual blood glucose measurements/instructed measurements X 100, (b) number of blood glucose measurements, (c) the mean fasting plasma glucose, (d) fasting insulin change, and (e) hemoglobin A1C (HbA1C) before delivery.
Effect of telehealth on additional health problems related to pregnancy
The authors of seven studies in this systematic review and meta-analysis24,36,37,39–42 reported additional health problems related to pregnancy (hypertension or preeclampsia or eclampsia and gestational diabetes mellitus). The subgroup analysis carried out to observe the effect of telehealth applications on additional health problems related to pregnancy revealed that the telehealth and control groups were statistically similar (OR: 0.89, 95% CI: 0.65 to 1.22, Z = 0.73, p = 0.46) (Figure 8).
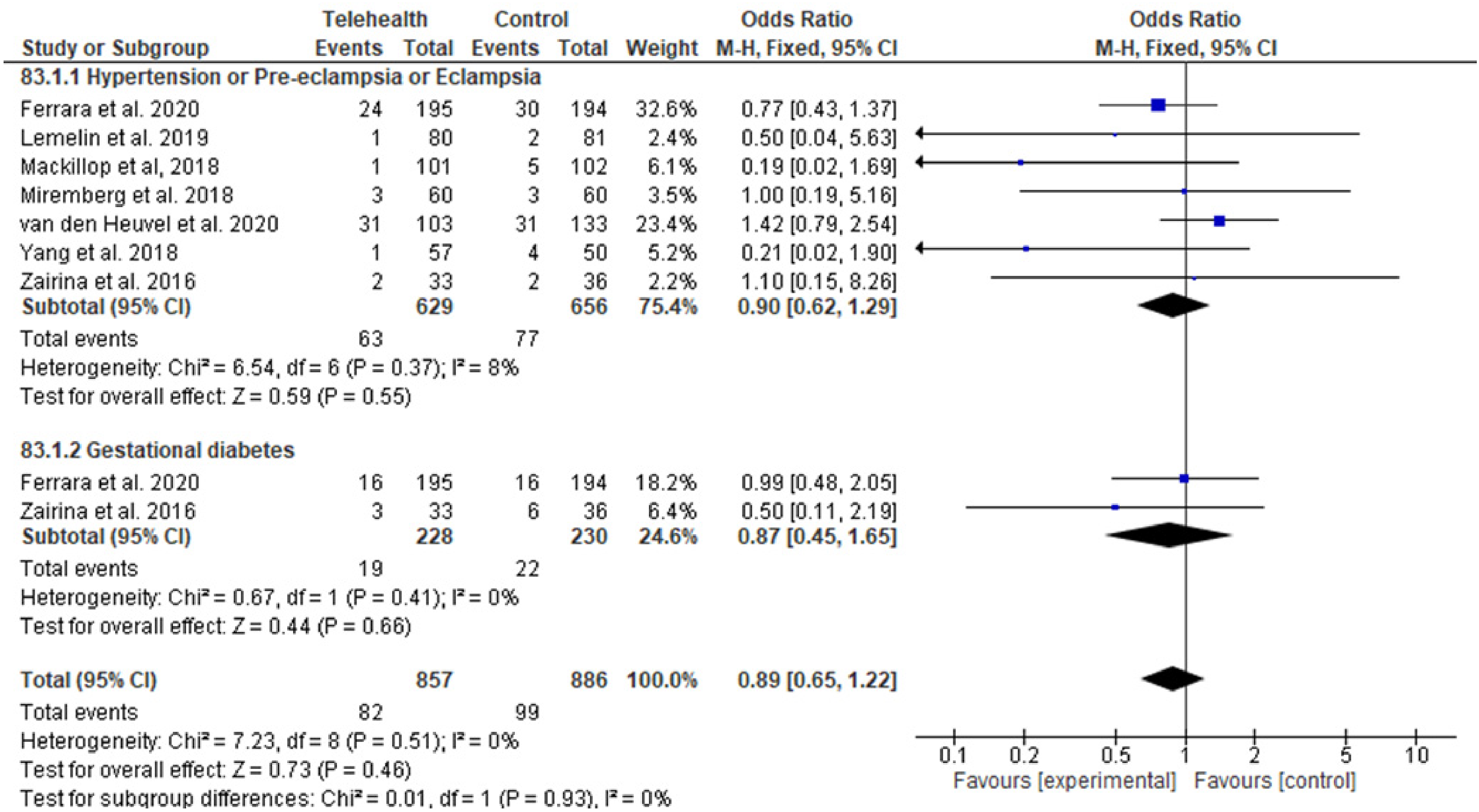
Meta-analysis results related to the effect of telehealth on additional health problems related to pregnancy.
Effect of telehealth related to the management of asthma
We reviewed in this study the impact of the telehealth application on asthma control and the quality of life in pregnant women with asthma. 41 Based on this, it was found in the meta-analysis that telehealth had a positive impact on asthma control and quality of life in the 3rd and 6th follow-up months (respectively, MD: −0.26, %95 CI: −0.30 to −0.23, Z = 14.86, p < 0.001; MD: 0.46, %95 CI: 0.41 to 0.51, Z = 18.82, p < 0.001) (Figure 9a–b).
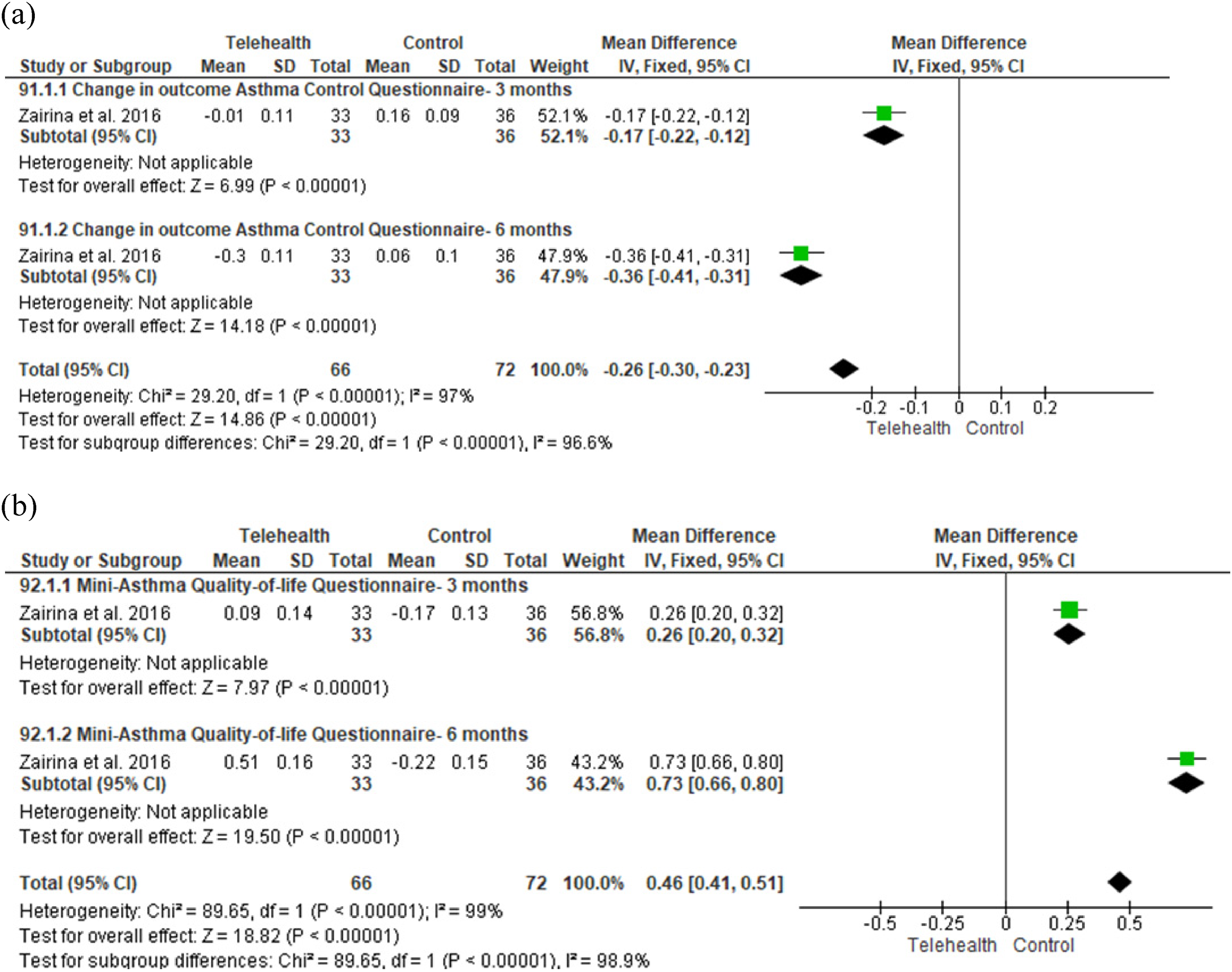
Meta-analysis results related to the effect of telehealth on the management of asthma: (a) Change in outcome Asthma Control Questionnaire—3 and 6 months and (b) Mini-Asthma Quality-of-Life Questionnaire—3 and 6 months.
Effect of telehealth on maternal birth outcomes
Five circumstances were found in this systematic review and meta-analysis that revealed the impact of telehealth interventions on maternal birth outcomes. In nine studies included in the meta-analysis, results had been reported about cesarean, primary, and emergency cesarean section delivery modes.24,35–42 The analysis revealed that there was no difference between the telehealth and control groups in terms of delivery mode but that emergency cesarean rates were statistically and significantly reduced in the telehealth group (OR: 0.54, 95% CI: 0.29 to 1.00, Z = 1.95, p = 0.05).
The results reported in seven articles about birth interventions (e.g. labor induction, labor intervention, and episiotomy) were included in the meta-analysis.24,35–37,39–41 The pooled results showed that the women in the telehealth group were subjected to 1.56 times the labor interventions experienced by the other women; this difference was statistically significant (OR: 1.56, 95% CI: 1.18 to 2.06, Z = 3.12, p = 0.002). In the subgroup analysis, it was seen that while the intervention of induced labor occurred 1.94 more times in the telehealth group (OR: 1.94, 95% CI: 1.26 to 2.99, Z = 3.01, p = 0.003), instrumental labor and episiotomy interventions were similar in both groups.
In six studies included in the meta-analysis, the authors reported labor complications in the form of shoulder dystocia, major perineal trauma, premature rupture of membranes, and postpartum hemorrhage.24,35–37,39,41 The analysis based on these outcomes showed that there was no statistical difference between the telehealth and control groups as far as labor complications were concerned (OR: 1.09, 95% CI: 0.61 to 1.94, Z = 0.29, p = 0.78).
The authors of one study reported that the use of telehealth applications had resulted in maternal admission into the intensive care unit. 24 According to the results of this study, no similarity was found between telehealth and control groups in terms of maternal admission into the intensive care unit (OR: 0.99, 95% CI: 0.06 to 16.05, Z = 0.01, p = 0.99). In another study, results were reported on the impact of the telehealth application on maternal mortality. 7 In the calculations made based on this study, it was seen that maternal mortality was 8.82 times higher in the telehealth group (OR: 8.82, 95% CI: 6.19 to 12.58, Z = 12.04, p < 0.001) (Figure 10a–e).
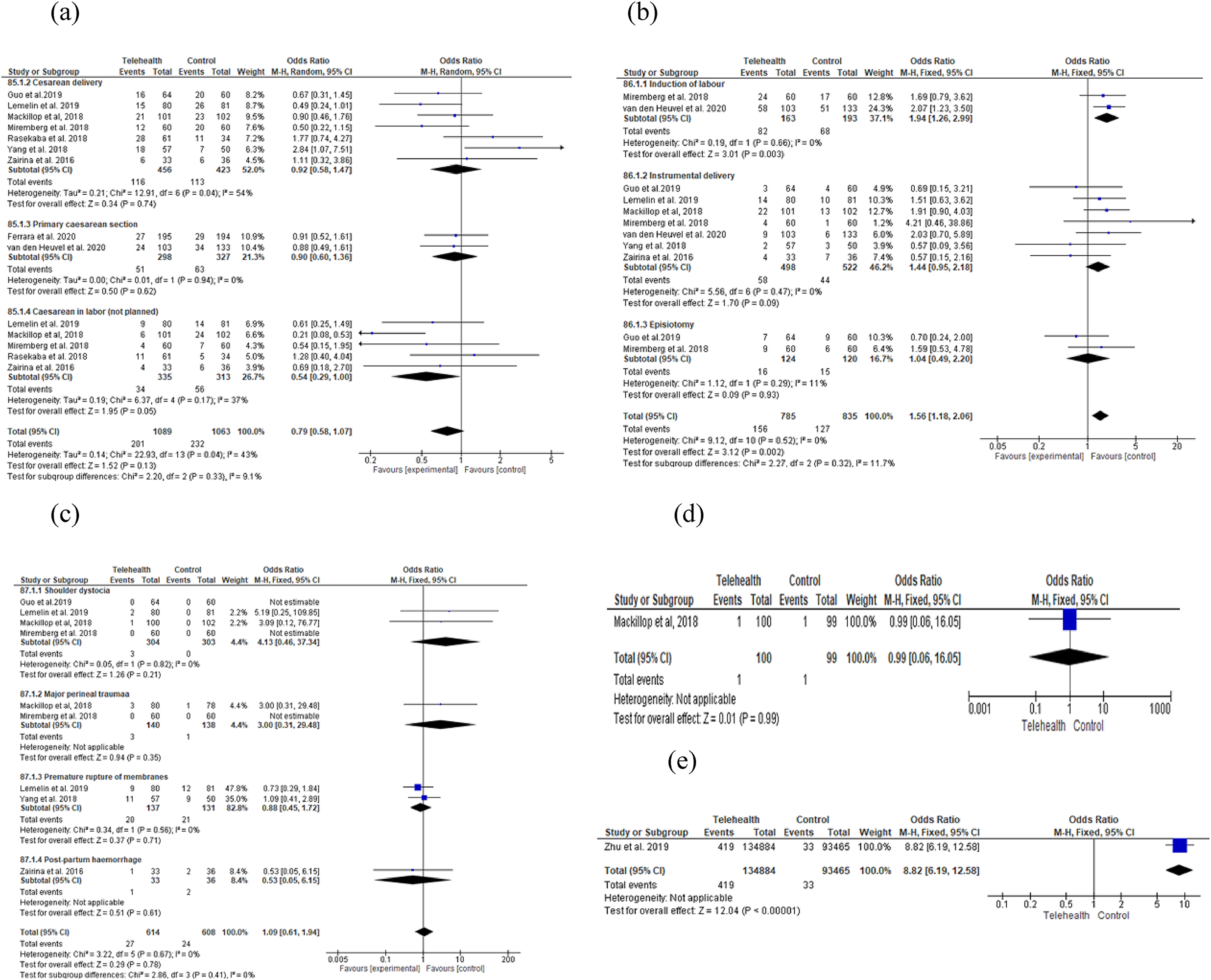
Meta-analysis results related to the effect of telehealth on maternal birth outcomes: (a) Type of delivery, (b) intervention of labor, (c) complications at birth, (d) admission to ICU, and (e) maternal mortality (/100,000).
Effect of telehealth on neonatal outcomes
In this systematic review and meta-analysis, we found five circumstances related to the impact of telehealth interventions on neonatal outcomes. In seven studies, the authors reported results on the birth weight of neonates.24,36–41 The pooled results of these studies demonstrated that there was no significant difference between the telehealth and control groups in terms of neonatal birth weight (MD: −12.14, %95 CI: −72.66 to 48.38, Z = 0.39, p = 0.69). In the meta-analysis of the results of eight studies,35–42 it was found that the telehealth and control groups were similar in terms of the variables of large for gestational age (LGA), low birth weight, small for gestational age (SGA), intrauterine growth restriction (IUGR), and fetal macrosomia (OR: 0.98, 95% CI: 0.78 to 1.24, Z = 0.15, p = 0.88).
In eight studies included in the meta-analysis,24,35–37,39–42 the authors reported results on neonatal health problems and the 5th-minute APGAR score being below 7, as well as on preterm birth, respiratory distress syndrome, hyperbilirubinemia, and hypoglycemia. The pooled results showed that the telehealth and control groups were statistically similar in terms of health problems appearing in the neonate (OR: 0.88, 95% CI: 0.66 to 1.18, Z = 0.84, p = 0.40). In another seven studies, the authors reported results on admission to the neonatal intensive care unit (NICU) or the special care nursery.24,36–41 The pooled results pointed to a similarity between the telehealth and control group in terms of admission to the NICU or to the special care nursery (OR: 0.75, 95% CI: 0.45 to 1.24, Z = 1.12, p = 0.26). In another study, it was reported that there was no significant difference between the telehealth and control groups in terms of neonatal mortality (OR: 0.69, 95% CI: 0.17 to 2.77, Z = 0.52, p = 0.60) (Figure 11a–e). 7
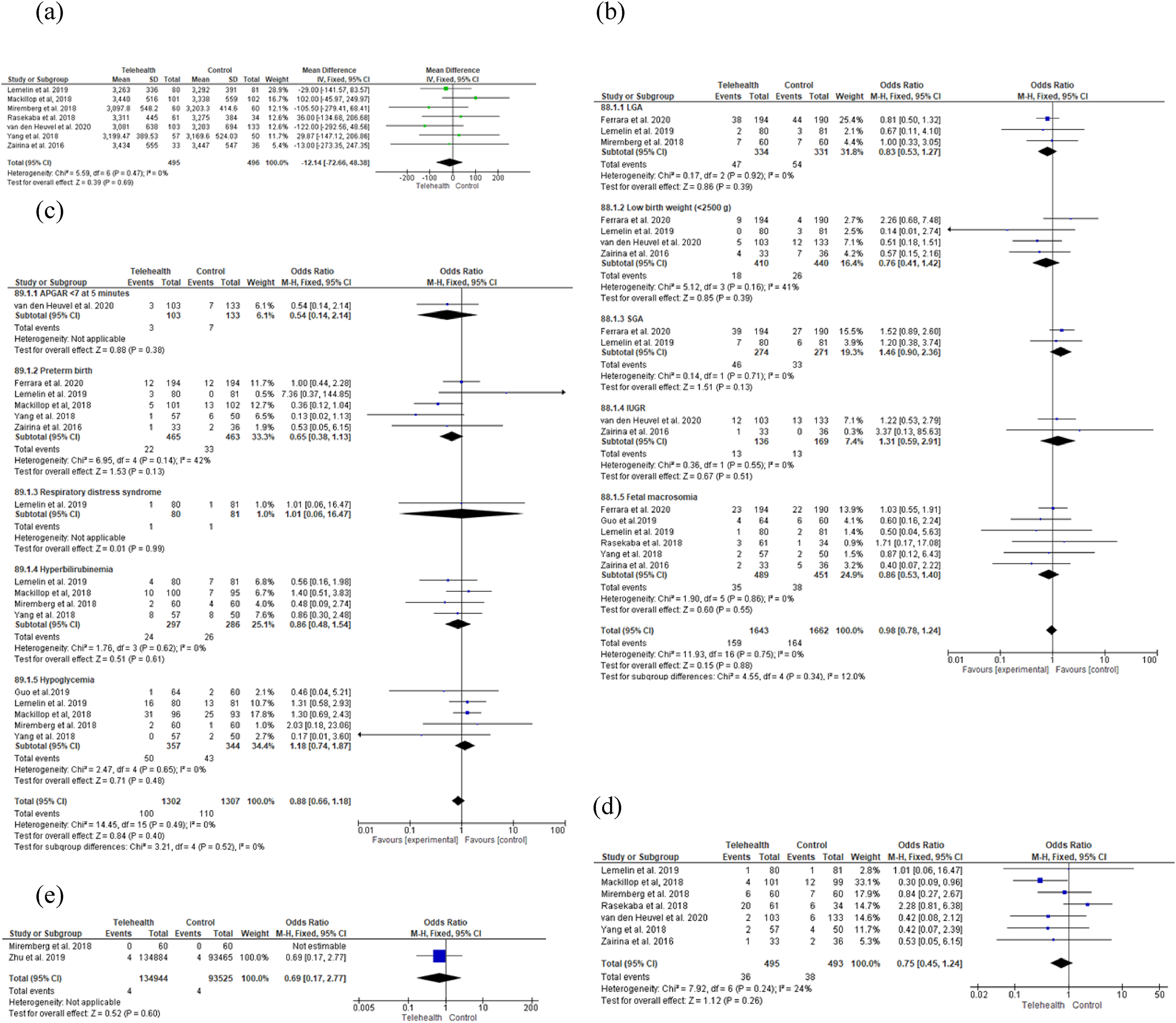
Meta-analysis results related to the effect of telehealth on neonatal outcomes: (a) Birth weight, (b) outcomes on the fetal-neonatal growth and development, (c) neonatal health problems, (d) admission to NICU or special care nursery admission, and (e) neonatal mortality.
Effect of telehealth on costs
The author of one study reported on the impact of telehealth applications on not work absenteeism. 36 In the calculations made based on this study, it was found that there was less absence from work in the telehealth group compared to the controls (MD: −1.00, %95 CI: −1.83 to −0.17, Z = 2.38, p = 0.02). Two studies contained results on face-to-face, unplanned and planned appointments, and the total care cost of pregnancy and labor; it was reported that the telehealth and control groups were similar in terms of these variables (Figure 12a–b).24,38
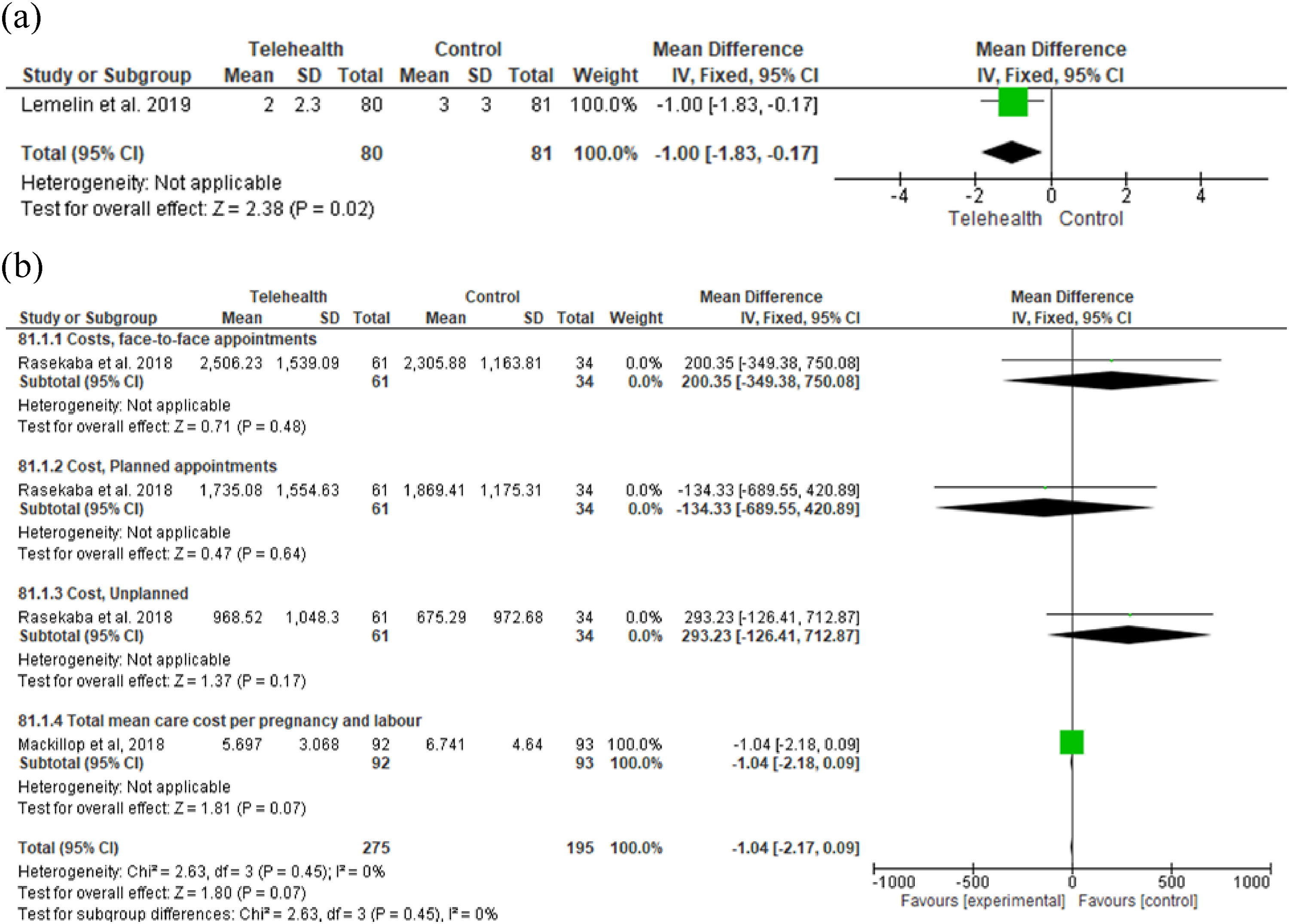
Meta-analysis results related to the effect of telehealth on costs: (a) Absenteeism at work and (b) follow-up and care costs.
Discussion
We identified in our study the impact of telehealth applications on pregnancy outcomes and costs in cases of high-risk pregnancy. We found that telehealth interventions had a positive impact on maternal/neonatal health as well as on costs. Our results are important in that they indicate that modern technology can be used in the management of high-risk pregnancies.
Our meta-analysis revealed that when the effect of telehealth on the gestational week in which insulin therapy was started and the use of insulin in pregnancy, the administration of magnesium, the use of antihypertensive therapy in the form of antihypertensive or intravenous antihypertensive therapy before and after gestational week <20 were compared to routine care, it was seen that the effects were similar, and that telehealth reduced the use of hypoglycemic therapy during labor. Similarly, a Cochrane systematic review has also indicated that the use of telehealth does not have an impact on insulin therapy during pregnancy. 43 These findings are important in that they indicate that the impact of telehealth in high-risk pregnancy is similar to what is achieved with routine care. On the other hand, this meta-analysis reveals that there were more cases of using antenatal corticosteroids in the telehealth group. This may be explained by the fact that the study was conducted with a population of pregnant women who were already at high risk regardless of the telehealth intervention.
We found in the meta-analysis that the telehealth intervention significantly reduced the average number of face-to-face and ultrasound visits, increased the number of nursing follow-ups by phone and the total number of nursing interventions, but did not have an effect on NST visits and receiving emergency obstetric care. Similarly, it has been reported in previously published meta-analyses and systematic reviews that telehealth applications reduce the number of face-to-face examinations during pregnancy.44,45 It was also found in this meta-analysis that telehealth reduced the number of ultrasounds. This finding might be explained by the fact that pregnant women benefiting from telehealth services apply to the hospitals less. In fact, the WHO does not recommend routine ultrasound scans. 28 It is believed that conducting a fewer number of ultrasounds does not have an adverse effect on maternal or fetal health. We found in our meta-analysis that telehealth did not affect the women's diet program, or their weight gain, either weekly on over the course of the pregnancy. It was seen however that telehealth increased the likelihood of weekly weight gain below the IOM criteria. Similarly, in another meta-analysis of 21 studies, the researchers reported that women receiving support gained less weight with telehealth applications during pregnancy compared to women without support. 46 These findings show that the use of telehealth in pregnancy may be useful in terms of improving women's adoption of a healthy lifestyle that includes weight control and healthy eating.
The authors of studies conducted in recent years have reported that telehealth is beneficial in the management of gestational diabetes mellitus (GDM) and that pregnant women are better able to achieve awareness and adaptation to treatment.38,47,48 Our meta-analysis is consistent with literature that reveals that telehealth increases the adaptation of pregnant women to glucose monitoring. The study also indicates that telehealth reduces levels of fasting insulin and pre-labor HbA1c, but does not affect the number of glucose measurements and the level of fasting plasma glucose. It is reported in another systematic review and meta-analysis that the use of telehealth during pregnancy reduces HbA1C and fasting blood glucose levels.10,14,49,50 These findings are important in that they demonstrate that telehealth can be of benefit in the management of disease in women with GDM.
We found in this systematic review and meta-analysis that the telehealth and control groups were similar in their status of also having hypertension or preeclampsia or eclampsia or developing gestational diabetes mellitus. In a systematic review on this topic, it was reported that a telehealth intervention was an effective method in controlling and preventing disease in pregnancy. 45 Chan and Chen 51 reported in their meta-analysis that telehealth was effective in improving the physical health of pregnant women, including in terms of keeping GDM under control. Based on these findings, it can be said that besides having an impact on existing maternal health issues, telehealth is also effective in terms of risk management.
We found in our study that telehealth has a positive effect on asthma control and quality of life in the 3rd and 6th follow-up months. No systematic review or meta-analysis was encountered in the literature on the impact of telehealth on asthma control. However, our findings support reports on the potential benefit of internet or mobile phone app-based health interventions compared to routine care in adults52,53 and children with asthma. 54 According to these results, it can be said based on the positive effects of telehealth on asthma control that pregnant women with asthma can safely use telehealth in monitoring their asthma.
It was seen in this systematic review and meta-analysis that telehealth reduced emergency cesarean rates but was not effective in primary and total cesarean childbirth. Similarly, Li et al. 55 reported in a meta-analysis performed to look into whether technology-supported lifestyle interventions improved maternal/fetal outcomes of women with gestational diabetes, that there was no significant difference between the groups in terms of cesarean rates. Again, in the meta-analysis by Ming et al., 10 the authors reported that the telehealth and the control group were similar in terms of cesarean rates (50% in the telehealth group; 45.0% in the controls). Similar results were revealed in the Cochrane systematic review by Raman et al. 43 In another meta-analysis, the authors reported that telemedicine interventions reduced the risk of cesarean delivery in women with GDM. 14 Besides pertaining to telehealth, these results could also have been a consequence of the approaches to mode of delivery in the areas where the study was conducted.
We observed in our study that in general, labor interventions and in particular, the use of labor induction were more common in the telehealth group, but instrumental labor and episiotomy interventions were similar in both groups. Li et al. 55 reported similar outcomes regarding instrumental labor in their meta-analysis. On the other hand, Raman et al. 43 revealed in their Cochrane systematic review that there was no significant difference between the telemedicine and control groups in terms of operative vaginal birth and induction of labor. The discrepancy in the reports on the effect of telehealth on labor interventions may be related to the differences in the characteristics of the cohorts (e.g. age, parity) or the methods used for intrapartum care and monitoring. According to these results, it can be said that evidence is still unclear about the effect of telehealth applications on labor intervention in high-risk pregnancy but that telehealth may increase the use of induction in labor.
Our meta-analysis results showed telehealth and control groups were similar in terms of labor complications such as shoulder dystocia, major perineal trauma, preterm rupture of the membranes, postpartum hemorrhage, and admission into the maternal intensive care unit. Raman et al. 43 reported similar results in their Cochrane systematic review. In their meta-analysis of eight studies (150 women), another group of authors reported one case of shoulder dystocia. 10 Contrary to these findings, Xie et al. 14 demonstrated in their meta-analysis that telemedicine interventions statistically and significantly reduced premature rupture of the membranes in women with GDM. This indicates that there is no increase in labor complications that may lead to maternal mortality in the telehealth group. Because of this, it might be said that telehealth can safely be used in prenatal care services provided to pregnant women at high risk.
Based on the results of the study by Zhu et al., 7 it was noted that the maternal mortality rate was higher in the telehealth group. Contrary to this finding, Snoswell et al. 56 demonstrated in their systematic review results of 24 meta-analyses that telehealth did not increase mortality rates on five overarching medical disciplines (cardiovascular, neurology, pulmonary, obstetrics, and intensive care). Since this finding is based on the results of only one study in our review, it is clear that more research is necessary.
We found in our meta-analysis that both telehealth and control groups were similar in terms of the variables of neonatal birth weight, LGA, low birth weight, SGA, IUGR, and fetal macrosomia. In another Cochrane systematic review, the authors reported that telemedicine and control groups were similar in terms of large-for-gestational age, fetal macrosomia, small-for-gestational age, and birthweight. 43 Another two meta-analyses carried out on this topic revealed reports of similar findings concerning neonatal birth weight and LGA.10,55 Based on these findings, in terms of the parameters of fetal-neonatal growth and development, it can be said that telehealth interventions are similar to standard care and follow-up.
In our study, we found that the telehealth and control groups were similar in terms of neonatal health issues such as the 5th-minute APGAR score being below 7, preterm birth, respiratory distress syndrome, hyperbilirubinemia, and hypoglycemia, and admission to the NICU or special care nursery. Raman et al. 43 reported similar results in their Cochrane systematic review. In their meta-analysis, Ming et al. 10 reported that telehealth and controls were similar in terms of admission to the NICU and neonatal hypoglycemia. Again in a similar fashion, Li et al. 53 demonstrated that telehealth and control groups were similar in terms of rates of preterm labor, neonatal hypoglycemia, fetal macrosomia, and admission to the NICU. In their meta-analysis, Xie et al. 14 reported that telemedicine interventions reduced the risks of macrosomia, neonatal hypoglycemia, and preterm birth, but both groups were similar in terms of admission to the NICU, or of neonatal jaundice or neonatal acute respiratory distress syndrome.
In this study, the telehealth group and the controls were found to be similar in terms of neonatal mortality. Similarly, Raman et al. 43 revealed in their Cochrane systematic review that there was no significant difference between the telemedicine and control groups in terms of stillbirth and neonatal death. Since we could find only one study 7 on the effect of telehealth on neonatal mortality, our meta-analysis results lead us to believe that there need to be more studies conducted with larger sample groups.
We determined in this study that telehealth caused an interruption of work, but did not affect the outcomes of face-to-face, unplanned and planned appointments, and total care costs of pregnancy and labor. Similarly, Raman et al. 43 in their Cochrane systematic review reported that the telemedicine and control groups showed similarity in terms of the number of face-to-face hospitals or professional health visits, but that the telemedicine group displayed a reduced number of unscheduled face-to-face visits. At the same time, Perez-Ferre et al. 57 reported on the costs of telehealth interventions, stating that telemedicine caused individuals to become more conscientious, which resulted in lower costs for the health system due to the decline in the utilization of professional health services. Based on these results, it can be said that telehealth applications may cut costs in the prenatal care of pregnant women at high risk, thus making a positive contribution to the healthcare system.
Strengths and limitations of the study
The strengths of this systematic review and meta-analysis included the fact that a comprehensive search strategy was used, the review encompassed an expansive geography (e.g. America, Asia, and Australia), brought into focus current issues, and involved an ample number of pregnant women. The results analyzed included various pregnancy risk groups, were collected from different telehealth applications, and were treated from a wide perspective that covered maternal, fetal ,and cost effects, all adding to the strengths of the study and reinforcing the outcomes. At the same time, since most of the studies examined were high in homogeneity, our study gains significance through the strength of the evidence. However, the fact that this study covered only those articles published in English constitutes a limitation. On the other hand, since most of the sample of research articles included in this study was made up of pregnant women with GDM, only a limited diversity of risk groups was represented. Also, because maternal and neonatal mortality rates were reported in only one article, the results limit the level of evidence presented by the meta-analysis.
Conclusions
In this systematic review and meta-analysis, (1) the telehealth group was found to display lower results in terms of the number of ultrasound and face-to-face visits, fasting insulin, HbA1C before delivery, emergency cesarean rates, absence from work; (2) the telehealth group was found to display higher results in terms of the use of antenatal corticosteroids and hypoglycemic medication at delivery, the number of nursing follow-ups by telephone, the total of nursing interventions, the probability of weekly weight gain that was lower than IOM criteria, compliance with actual blood glucose measurements, asthma control and improved quality of life in the 3rd and 6th follow-up months, labor induction interventions, and maternal mortality; and (3) the groups were similar in terms of the gestational week when the insulin therapy was started, the use of medical therapy, NST visits and receiving emergency obstetric care, weight gain after treatment, excessive weight gain weekly and during pregnancy, and total gestational weight gain, number of blood glucose measurements and mean fasting plasma glucose levels, additional health problems related to pregnancy, mode of delivery, instrumental labor and episiotomy interventions, labor complications, admission into maternal intensive care unit, neonatal birth weight, outcomes of fetal-neonatal growth and development, neonate health issues, admission to the NICU or special care nursery, neonatal mortality, follow-up, and care costs.
The results of this research and the recommendations of international health organizations3,17,18 show that health providers and administrators can use telehealth as a safe method in the monitoring and care of pregnant women at high risk, thus contributing to the improvement of antepartum care services. At the same time, it might be suggested that randomized controlled studies are conducted on the effects of telehealth on different risk groups during pregnancy, which would lead to systematic reviews and meta-analyses that would provide stronger evidence.
Footnotes
Author’s contribution
Study design: GGÖ, DA, ZK. Data collection: GGÖ, DA, ZK. Data analysis: GGÖ, DA, ZK. Study supervision: ZK. Manuscript writing: GGÖ, DA, ZK. Critical revisions for important intellectual content: ZK. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Not applicable as this is systematic review.