
Abstract
Background
During the COVID-19 pandemic, we identified a gap in adequate discharge counseling for COVID-19 patients in the Emergency Department. This was due to high patient volumes and lack of patient education regarding a novel disease. Medical students were also restricted from clinical areas due to safety concerns, compromising their clinical experience. We piloted a novel program in which medical students served as virtual discharge counselors for COVID-19 patients via teleconference. We aimed to demonstrate an impact on patient care by examining the patient bounce back rate as well as assessing medical student education and experience.
Methods
This program was piloted in a tertiary care Emergency Department. Medical student volunteers served as virtual discharge counselors. Students were trained in discharge counseling with a standardized protocol and a discharge script. Eligible patients for virtual discharge counseling were 18 years old or greater with a diagnosis of confirmed or suspected COVID-19 and no impediment precluding them from participating in a telemedicine encounter. Counseling was provided via secure teleconference in the patient's preferred language. Counseling included diagnosis, supportive care with medication dosing, quarantine instructions, return precautions, follow up, and time to ask questions. Duration of counseling was recorded and medical students were anonymously surveyed regarding their experience.
Results
Over an 18-week period, 45 patients were counseled for a median of 20 min. The 72-hr ED revisit rate was 0%, versus 4.2% in similarly-matched, not counseled COVID-19 patients. 90% of medical students believed this project increased their confidence when speaking with patients while 80% indicated this was their first telemedicine experience.
Conclusion
Our pilot discharge program provided patients with an extensive discharge counseling experience that would not otherwise be possible in an urban ED setting and demonstrated benefit to patient care. Medical students received a safe clinical experience that improved their communication skills.
Introduction
The first wave of the COVID-19 pandemic hit New York City beginning in February 2020. During this time, Emergency Departments (EDs) were overwhelmed with high-acuity patients, as well as those who were discharged with a new diagnosis of COVID-19. During this time period, there were an estimated 203,000 confirmed cases in New York City. 1 According to The Joint Commission, approximately 80% of adverse medical events occur during care transitions, including to home. State data suggest that only 47% of New Yorkers receive adequate information about care following discharge. 2 This gap in discharge education was further amplified during the pandemic with many well and worried patients who required extra counseling on a new and dangerous diagnosis. At the same time, due to safety concerns, medical students were displaced from clinical duties in hospitals, which compromised their clinical experience. During the COVID-19 pandemic, we identified a simultaneous gap in both ED COVID-19 patient discharge counseling, as well as medical student patient interaction.
Both telemedicine and discharge counseling have been identified as areas for educational growth within the medical school curriculum. In particular, telemedicine underwent a rapid expansion during the COVID-19 pandemic; however, medical training has lagged in incorporating this rapidly growing field into the curriculum. A study in 2017 found that only 10.4% of medical schools in France had telemedicine education in their first year, and only 4% of schools integrated telemedicine into their clinical training. 3 In the US, approximately, 25% of allopathic medical schools integrated telemedicine into their preclinical curriculum and almost half into their clinical training in 2016. 4 A recent survey from the Alliance for Clinical Education (ACE) noted that the biggest barriers to incorporating telemedicine in a medical school curriculum were a lack of technology delivery mechanism and administrative concerns, such as compliance with laws. 5 Despite initial gains in the usage of telemedicine during the early parts of the pandemic, analyses have shown that it has since declined, with some attributing this to the lack of prior training with telemedicine or lack of established workflows. 6 In addition, the vast majority of medical students have no formative education in discharge counseling, yet will be expected to perform this task during their careers. We piloted a novel program in which medical students served as virtual discharge counselors for COVID-19 patients via remote tele-conference. To our knowledge, our pilot study is the first to incorporate telemedicine as a modality to teach and perform discharge counseling.
The goals of this COVID-19 virtual discharge counseling pilot quality intervention were: augment patient education and experience upon discharge via dedicated discharge counseling time by medical students; decrease COVID related return visits; reduce provider tasks as it pertained to discharge counseling to allow clinical staff to focus on high acuity patients during a pandemic; improve medical student core competencies (interpersonal and communication skills, patient care and medical knowledge); provide students with a safe clinical experience and introduce them to the rapidly growing field of telemedicine.
Methods
Setting
NYU Langone Brooklyn Hospital is a tertiary care referral center and a community hospital affiliate of NYU Langone Health. It is located in the diverse urban area of Sunset Park, Brooklyn and serves as a level I trauma center.
Study population
Eligible patients for virtual discharge counseling were ED patients that were 18 years of age or greater who were being discharged from the ED with a diagnosis of confirmed or suspected COVID-19. Patients also had no impediment precluding them from participating in a telemedicine encounter.
Medical student volunteers from NYU Grossman School of Medicine participated in this pilot study. MS2-MS4 student volunteers were utilized who had already participated in at least one clinical clerkship.
Intervention
Medical students were trained with a standardized protocol and provided with a thorough and prepared discharge script for COVID-19 counseling, which can be found in the supplementary material accompanying the online article (methods supplement). This seven-page illness script contained critical discharge elements: explanation of diagnosis, educational content (including instructions for supportive care and isolation), supportive care medication dosing, return precautions, follow-up, and the ability for patients to ask questions.7,8 The script also included a “frequently asked questions” section to which students could refer.
Medical students were notified by nurses or providers via secure chat once patients were ready to receive discharge instructions. The nurse or provider would then move a designated iPad (Apple Inc., Seventh generation, Cupertino, CA) into the patients’ room. The discharge counselor would call into the iPad via secure (HIPPA-compliant) video conference (Cisco Jabber, Cisco Systems, Inc., San Jose, CA). Counseling included previously identified critical discharge elements.7,8 Counseling was provided in the patient's preferred language utilizing either in-person or conference call-in certified language interpreters. Discharge counseling was documented in the patient's EHR (Epic Systems Corporation, Verona, WI) by the student. This workflow is shown in Supplemental Material S2.
Measurements
After discharge counseling was complete, patient demographics, counseling duration time, and language spoken were recorded by the medical student for each encounter in a HIPAA complaint data repository (REDCap, version 12.0.19, Vanderbilt University, Nashville, TN). Additionally, students also documented whether patients asked any additional questions which were not listed in the discharge script.
After the pilot, participating medical students (n = 16) were anonymously surveyed regarding their experience utilizing a Likert scale of 1–5, with one indicating they strongly disagreed with the statement and five indicating they strongly agreed. Questions were targeted at assessing perceived improvement in interpersonal and communication skills, medical knowledge, patient care as well as program preparation/support and service orientation.
Data analysis
Duration of counseling times and bounce back rate comparison was analyzed via the Kruskal–Wallis test, with post-hoc pairwise application of the Mann–Whitney U test with Bonferroni correction. Bounce back rate was compared among counseled and non-counseled patients who were matched with a diagnosis of COVID or confirmed COVID same language and patient age.
Institutional review board approval was not required for this pilot quality improvement activity. Authors of this study had no conflicts of interest.
Results
Over an 18-week period from May 2020 to September 2020, 45 patients with a diagnosis of COVID-19 or suspected COVID-19 were counseled. The average patient age was 44 years old. 44% of patients identified as female and 56% identified as male. A total of twenty second through fourth year medical students at NYU Grossman School of Medicine voluntarily chose to participate as discharge counselors. 60% of the volunteer medical students identified as female and 40% identified as male. Eligible patients for virtual discharge counseling were 18 years of age or greater with a diagnosis of confirmed or suspected COVID-19 and no impediment precluding them from participating in a telemedicine encounter.
The median counseling time duration was 20 min (range: 7–39 min). 58% of patients were English speaking; 35% were Spanish speaking; and 7% spoke other languages (Arabic, Cantonese, and Mandarin). The median times for discharge counseling in English, Spanish, and other languages were 16 min, 23 min, and 18 min, respectively (p = 0.015) (Figure 1). Discharge counseling in Spanish took significantly longer than English (p = 0.017). The 72-h ED revisit rate in counseled patients was 0%, versus 4.2% in similarly-matched, non-counseled COVID-19 patients.
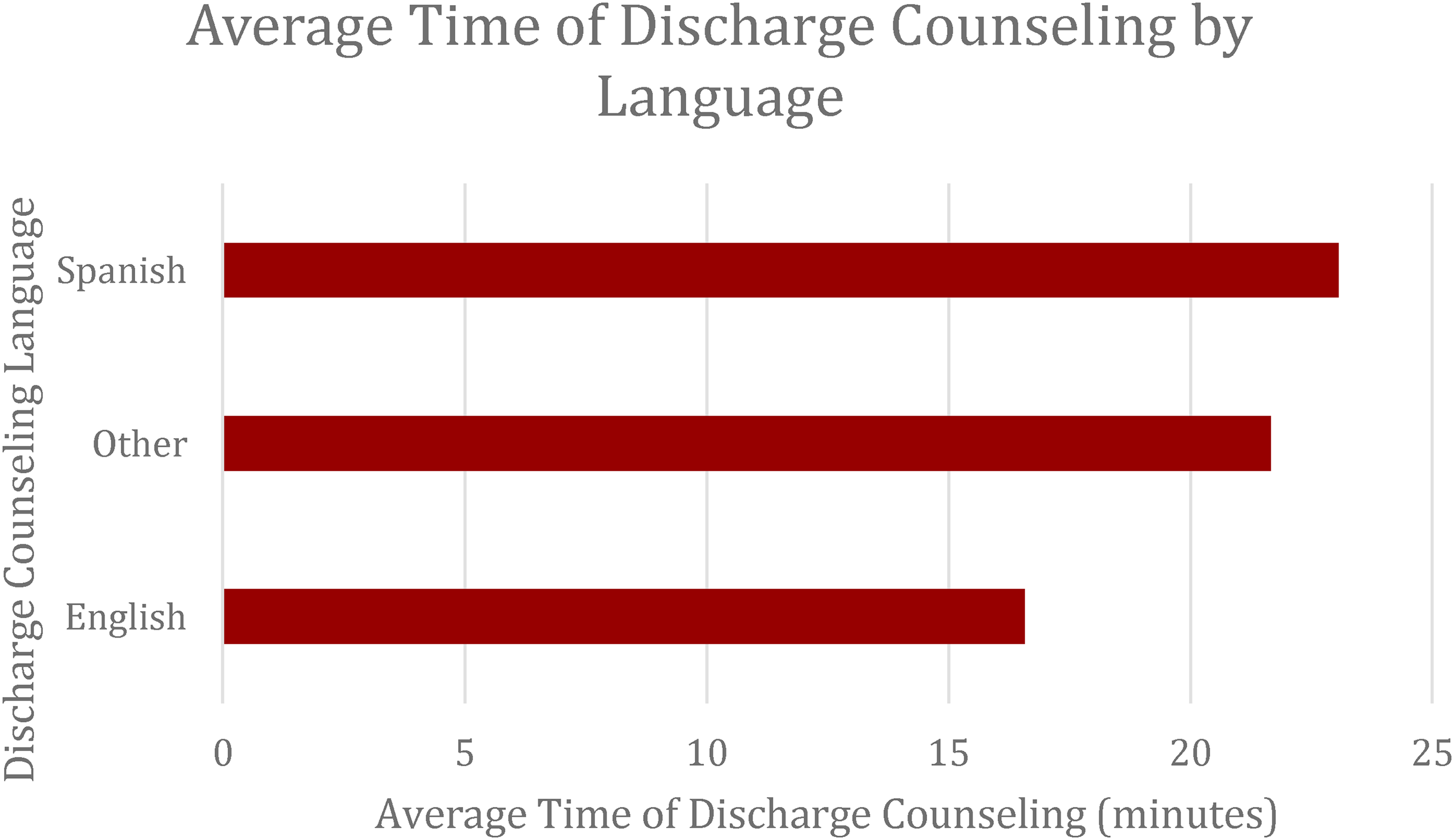
Average discharge counseling time by language of patients who were discharged counseled.
Medical students (n = 16) participating in this pilot study were anonymously surveyed regarding their experience with a 63% response rate. Overall, students believed this project increased their confidence when speaking with patients (90% strongly agreed or agreed) and that it was a worthwhile experience (100% strongly agreed or agreed). Lastly, 80% strongly agreed that they would volunteer again, and similarly, 80% indicated that this was their first telemedicine experience (Figure 2).
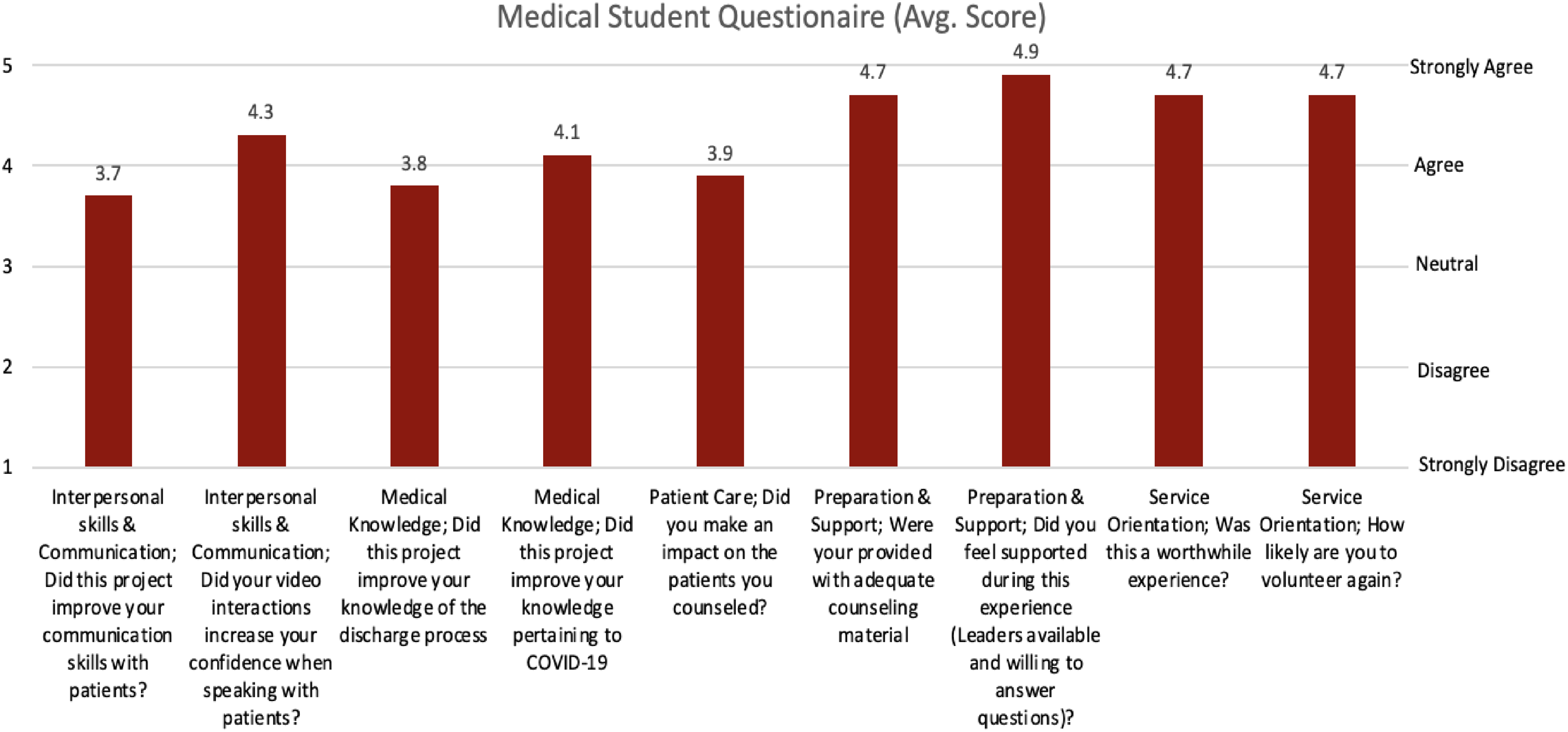
Average response to learning goals of medical student.
Discussion
This pilot study utilized medical students as virtual discharge counselors during the initial wave of the COVID-19 pandemic, thereby providing both patients and medical students with an enriched discharge counseling experience. We were able to ensure both patient and student safety by limiting in-person interactions via remote counseling, offloading tasks from ED staff to allow them to focus on acute patients, and provide high-quality dedicated discharge counseling to our patients.
As the hospital is located in a diverse urban environment (Brooklyn, NY), the predominant counseling languages were English (58%) and Spanish (35%), with patients counseled in Spanish requiring significantly longer counseling duration than English speaking patients (23 min versus 16 min, p = 0.015). Prior studies have found that limited English proficiency (LEP) patients have higher odds of difficulty with understanding a medical situation and confusion regarding medication use, 9 demonstrating the need for allowance of longer counseling duration for LEP patients. During our pilot, we provided patients with a median of 20 min of discharge counseling time. In one prior study which examined 477 audio tapes of ED discharge encounters, the average duration time was substantially lower (4 min). 10 We postulate that the reason for this difference is likely two-fold: our pilot utilized medical trainees who received specific training and instructions on the core elements of discharge counseling, an area generally underemphasized in medical training. Moreover, the students who participated in our pilot were solely dedicated to discharge counseling, affording them more time to do so, while busy emergency department staff must balance competing priorities (goal conflict), particularly during a pandemic. Additionally, only 34% of those discharges in the study by Vashi and Rhodes discussed ED return precautions, and only 22% provided the patient with an opportunity to confirm their understanding of the discharge instructions. 10 Our pilot study, with significantly longer discharge counseling times unencumbered by competing pressures, was able to consistently address each of these vital aspects of discharge counseling.
One of the goals of this pilot study was to decrease patient bounce backs to the ED. One reason that patients may return to the ED is due to a lack of understanding of their discharge instructions; this may have been especially amplified during a pandemic with heightened patient anxiety coupled with limited time resources to dedicate to counseling. In our pilot study, counseled patients had a 0% ED 72-h bounce-back rate as compared to 4.2% with similarly matched, non-counseled COVID-19 patients thereby demonstrating the impact of dedicated counseling.
It was equally as important to provide students with an enriching clinical experience at a time during which they were otherwise prohibited from clinical practice. From our pilot study, anonymous student surveys demonstrated that this discharge counseling program both increased their confidence in speaking with patients as well as improved their medical knowledge pertaining to COVID-19. Students felt well supported during this program, and felt it was a worthwhile experience and would volunteer again (Figure 2). Prior studies out of the United Kingdom have found no significant difference in medical students’ perceived usefulness and the ability to learn when comparing face-to-face clinic visits versus video telemedicine clinic visits. 11 This underscores the value of our medical student telemedicine pilot study during the initial wave of the COVID pandemic and the value of continued incorporation of telemedicine teaching into medical school curriculums.
While basic concepts such as taking a patient's history are fundamentally taught early in medical school, more advanced concepts such as answering patient questions and discharge counseling require a higher level of medical comprehension and skill acquisition. While discharge counseling is a vital skill for clinicians, there is a paucity of literature on formal medical school education regarding this topic. One study at Boston University School of Medicine, demonstrated that out of the five critical elements of discharge counseling, 78% of medical students only discussed two or fewer of these elements while observed by a supervising physician. 12 Furthermore, these results were obtained after a brief introduction to discharge counseling thereby demonstrating the need for this skill to be incorporated into medical school didactics. Our study leveraged telemedicine not only to practice critical elements of discharge counseling but also to introduce students to the growing field of telemedicine. A prior study by Smith and colleagues noted several factors contributing to a lack of telemedicine growth prior to the pandemic: clinician unwillingness to adopt telemedicine, complexity of implementation and perception of telemedicine ineffectiveness. 13 By exposing trainees to telemedicine early through our simple discharge counseling model with positive patient and student interaction, these future physicians can move forward with the knowledge and experience to incorporate telemedicine into their future clinical practices.
Limitations
Our pilot study had several limitations: A relatively small number of patients counseled (n = 45), as well as discharge counselors (n = 16). Given this sample size, our decreased revisit rate, though statistically significant, may be influenced by other confounding factors. Our medical student questionnaire was only administered post-discharge counseling; thus, we only have cross-sectional information and cannot quantitatively gauge improvement in skill. We were also unable to collect objective patient satisfaction data. A large barrier to this was contacting patients after their discharge, as surveys administered by their discharge counselor may have produced bias. We presume that if a patient has a roughly 20-min face-to-face counseling interaction with an open forum for questions, then their understanding of their disease as well as overall satisfaction with the discharge process would improve. Future studies should focus on objective patient surveys regarding information retention and satisfaction.
Conclusion
Our novel discharge program was centered on patient-driven education and improvement of the discharge process. Limited English proficiency and limited health literacy barriers were addressed. Through our pilot study, patients were able to receive extensive discharge counseling in their preferred language, which would not otherwise be possible in an urban ED setting amidst a pandemic, or even routine ED operations. In addition, our pilot program demonstrated a mechanism in improving clinical efficiency during a pandemic by offloading discharge tasks to medical students who were otherwise restricted from direct patient care. This innovative solution offered a safe clinical experience for medical students whose education was adversely compromised by COVID-19 and served as an introduction to the rapidly growing field of telemedicine. We also established the feasibility of quickly train clinical novices, demonstrating that this experience improved their self-perceived communication and clinical skills. Due to its success, this program was scaled across three additional ED sites, and ten additional counseling diagnoses were added. The program accrued over 40 medical student participants and has proven to be sustainable and scalable.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X221149227 - Supplemental material for Piloting a novel medical student virtual discharge counseling process in the time of the COVID-19 pandemic
Supplemental material, sj-docx-1-jtt-10.1177_1357633X221149227 for Piloting a novel medical student virtual discharge counseling process in the time of the COVID-19 pandemic by Victoria Leybov, Joshua Ross, Silas W Smith, Amber Ciardiello, Sana Maheshwari, Christopher Caspers, Ian Wittman, Christopher Kuhner, Stephen Stark, and Nancy Conroy in Journal of Telemedicine and Telecare
Supplemental Material
sj-docx-2-jtt-10.1177_1357633X221149227 - Supplemental material for Piloting a novel medical student virtual discharge counseling process in the time of the COVID-19 pandemic
Supplemental material, sj-docx-2-jtt-10.1177_1357633X221149227 for Piloting a novel medical student virtual discharge counseling process in the time of the COVID-19 pandemic by Victoria Leybov, Joshua Ross, Silas W Smith, Amber Ciardiello, Sana Maheshwari, Christopher Caspers, Ian Wittman, Christopher Kuhner, Stephen Stark, and Nancy Conroy in Journal of Telemedicine and Telecare
Footnotes
Acknowledgements
Audrey Bree Tse-Tanzanillo, MD
Masahsi Rotte, MD
May Li, MD
Catherine Jamin, MD
Robert Femia, MD
Harita Reddy, MPH
Joanna Watterson, MD
Viraj Lakdawala, MD
Anup Chitnis, MD
Staci Mandola, RN
Author contributions
VL, NC, CC, and IW conceived and designed the quality intervention. VL, JR, NC, AC, SM, and CK implemented the interventions. VL and NC supervised the conduct of the quality intervention. VL, JR, and SWS acquired and managed the data. SWS analyzed and interpreted the data. VL, JR, NC, AC, SM, CK, CC, IW, SS, and SWS provided administrative, technical, or material support. JR, VL, and SWS drafted the manuscript, and all authors contributed substantially to its revision for important intellectual content. VL, JR, and SWS take responsibility for the paper as a whole.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Financial support
No funding was received for this work. For work outside of the scope of the current study, SWS is supported by grant funding from the National Institute of Biomedical Imaging and Bioengineering (NIBIB1R01EB024539 - 01A1) and the National Institute on Drug Abuse (1R61DA049265-01) to the New York University Grossman School of Medicine.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.