
Abstract
Introduction
Shortage of ear, nose, and throat specialists in public hospitals can result in delays in the detection and management of otitis media. This study introduced a new hospital-based telehealth service, named the Ear Portal, and investigated its role in improving access to specialist care.
Methods
The study included 87 children (aged 6 months to 6 years) referred to a tertiary children's hospital due to otitis media-related concerns. A specialist multidisciplinary team met fortnightly to review pre-recorded data and provide care plans.
Results
The service resulted in a median waiting time of 28 days to receive a diagnosis and care plan by the multidisciplinary team, compared to a mean waiting time of 450 days for a reference group receiving standard healthcare services. Most children (90.3%) received bilateral ear diagnosis. Normal findings were found in 43.9%. However, the majority required further ear, nose, and throat with or without audiology face-to-face follow-up due to a diagnosis of middle-ear disease, unknown hearing status, or concerns not related to ears. The mean time required for clinical assessments completion by research assistants and multidisciplinary team review was 37.6 and 5.1 min per participant, respectively.
Discussion
Children in the Ear Portal service received a diagnosis and care plan in a median of 28 days, which is within the clinically recommended timeframes. With sufficient clinical information, this service can provide faster access to specialist care than the standard healthcare pathway. The service can reduce the time required by the specialist to provide a diagnosis and care plan which may help increase the specialists’ capacity.
Introduction
Middle ear infection, also known as otitis media (OM), is one of the most prevalent childhood diseases, affecting around 80% of children by the age of 4 years, 1 and 26.8% of children can experience recurrent episodes of OM by the age of 3 years. 2 OM is known to be the main cause of conductive hearing loss (HL) in children. 3 As such, children with recurrent and persistent OM may be more likely to encounter developmental delays.4–9 Prolonged OM episodes can increase the chances for developmental delays to persist in the long term. 9 They may also lead to extracranial complications (e.g. mastoiditis) or intracranial complications (e.g. meningitis). 10 Timely diagnosis and management are therefore important, to avoid these consequences.
Access to specialist ear-health services is, however, limited globally, 11 resulting in delays in the detection and management of OM. In Australia, the limited number of specialists has been shown to be a barrier contributing to reduced access to outpatient services in hospitals. 12 Therefore, children referred to ENT outpatients clinics in public hospitals can suffer lengthy waiting times before they receive care, resulting in delays in the diagnosis and management of OM.13–15 In Western Australia, where the present study was conducted, waiting times for an initial appointment in the ENT outpatient clinic have been reported to be up to two years in public hospitals. 16 Previous studies have looked at alternative hospital-based services to improve access to ENT specialist clinics, including the utilization of advanced audiology-led services.13–15,17,18
Others have shown the effectiveness of telehealth in improving access for patients living in remote and rural areas to ear-health services.19–23 Telehealth has been also shown to be an effective intervention for reducing waiting times to access different outpatient specialist services including ENT. 24 Telehealth has recently gained global recognition since healthcare provision became more restricted amid the outbreak of COVID-19, with outpatient consultations being one of the main settings where telehealth was most commonly implemented. 25
Whilst employing telehealth to expedite access to ENT specialists for patients living in rural and remote was the focus of previous studies, telehealth may also help improve access to ENT specialists in metropolitan areas where current service provision is also limited. Therefore, we created a new hospital-based telehealth service, named the Ear Portal, which was designed to improve access to specialist ear-health services and facilitate timely diagnosis and management for children with OM-related concerns. The present study described this service and investigated its effectiveness in reducing waiting times. The time taken to test children and asynchronously review their results by a multidisciplinary team (MDT) was also assessed. It was hypothesised that the service will improve children's access to specialist ear-health services by reducing waiting times for receiving care within the clinically recommended timeframes compared to the standard healthcare pathway and increase in the use of specialists’ time.
Methods
Ear Portal study
Recruitment in the Ear Portal study commenced in June 2020. Participants recruited in the study were allocated to one of three cohorts according to the date they were placed on the hospital's ENT outpatient clinic waiting list. Cohort 1 included children who had been on the waiting list for < 6 months. Cohort 2 included children who had been on the waiting list for > 6 months and did not have an appointment booked in the ENT outpatient clinic, while cohort 3 included children who had been waiting the longest and already had a standard care ENT outpatient appointment booked. Children were recruited in three different cohorts to compare the medical and developmental outcomes of children encountering different waiting times. For the purposes of the present study, children in cohorts 1 and 2 were included in the analyses as one group which was referred to as the ‘Ear Portal group’, while cohort 3 was referred to as the ‘Standard Healthcare group’ in the following sections.
Inclusion criteria
Eligibility criteria included children aged between six months and six years who were on the Perth Children's Hospital (PCH) ENT outpatient clinic waiting list for their initial appointment (i.e. not previously referred or seen in public or private ENT clinics) and live in the greater metropolitan region (within a 60 km radius) of Perth, Western Australia. Children had to be referred due to recurrent or persistent OM, or due to caregiver's concerns regarding the child's hearing, speech and/or language development. Informed consent was provided by the caregiver prior to participation in the study.
Exclusion criteria
Children were excluded if they were triaged by the hospital as a ‘category 1’ referral, (i.e. requiring urgent medical intervention), or had a complex medical history (e.g. craniofacial abnormalities) that required regular face-to-face follow-ups.
Recruitment
Participants were identified and recruited regularly from the ENT outpatient waiting list at PCH. Opt-out notification letters were mailed to caregivers of all eligible children. These letters provided information on the study and an invitation for participation. Following a two-week opt-out period, the Ear Portal team contacted the caregivers to discuss the study, confirm the children's eligibility, and obtain pre-consent. An Ear Portal appointment was then booked on a day chosen by the caregiver. A copy of the written consent form was emailed to caregivers to read the details and ask questions before appointments. Written consent was signed by caregivers on the day of the appointment. Figure 1 illustrates the process of recruitment and assessment of all children.
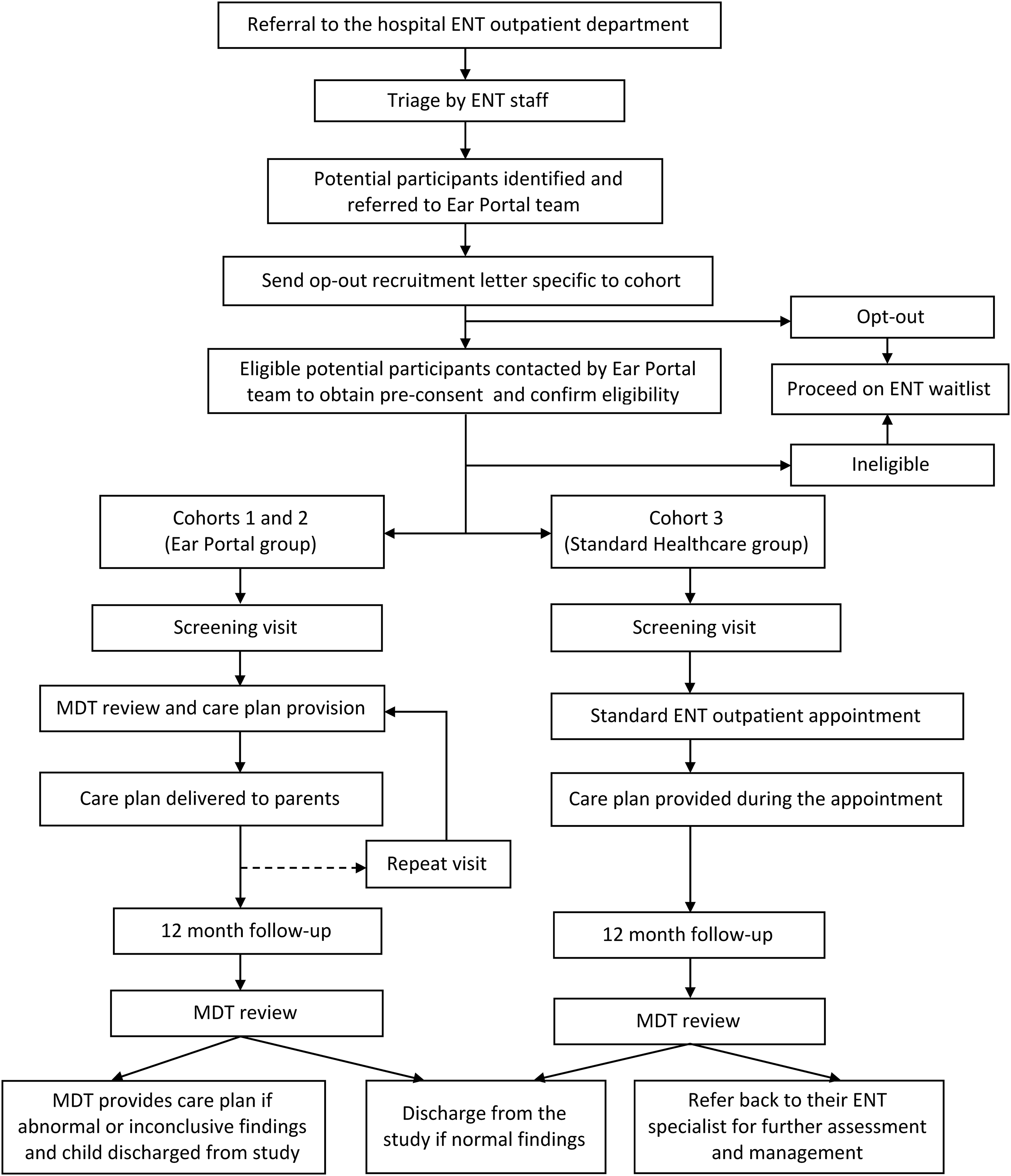
Flowchart of the Ear Portal recruitment, assessment, and care plan provision processes.
Equipment
The equipment used in this study was selected based on its portability and ease of administration by trained non-clinicians. Video otoscopy was conducted using the HearScope app version 2.0 (HearX Group, Pretoria, South Africa), to collect still images and/or recordings of the tympanic membrane (TM) and ear canal. Hearing screening (air-conduction only) at 25 dB at 500, 1000, 2000 and 4000 Hz was attempted in all children who were able to provide responses, using the HearScreen app (HearX Group, Pretoria, South Africa). The HearScreen app is calibrated to international standards and validated for paediatric use.26–28 Both apps were installed in a 4.7-inch screen Samsung Galaxy A3 smartphone (2017) connected to video otoscopy and headphone attachments. To assess the middle ear function, single probe tone (226 Hz) tympanometry and wideband tympanometry (WBT) were used, while distortion product otoacoustic emissions (DPOAE) between 1 and 6 kHz were performed to assess cochlear function. Titan Middle Ear Analyzer (Interacoustics, Denmark) was used to perform tympanometry, WBT and DPOAE.
Questionnaires
During the appointment, a case history of the child was completed with the caregiver to obtain information on demographic, general medical history, OM-specific history and treatment, family history and an economic assessment. Children's listening and language skills were screened using the Parent-Evaluated Listening and Understanding Measure (PLUM) and the Hear and Talk Scale (HATS) (National Acoustic Laboratory, Australia). The PLUM provides information about a child's listening behaviour in daily life, while HATS provides information about a child's hearing and talking abilities at home. 29 Caregivers also completed the Otitis Media-6 (OM-6), a widely used OM-specific quality of life questionnaire. 30 All questionnaires are parental-reported questionnaires.
Screening visit
All children attended a screening visit in the PCH research clinic, where the aforementioned assessments and questionnaires were conducted. Children were examined by research assistants from the Ear Portal team. Some research assistants were non-clinicians who were trained on how to use the equipment and save results by study audiologists, others were qualified audiologists. Research assistants were only responsible for collecting data. To ensure equal service provision, interpretations of findings and recommendations were only provided to caregivers after the results were asynchronously reviewed by the MDT.
The Ear Portal MDT, which included an ENT consultant or registrar, ENT clinical nurse specialist, audiologist and a research assistant usually met fortnightly to discuss the findings and provide individualised care plans for children in the Ear Portal group. An Ear Portal team member then contacted the caregiver for care plan delivery. The MDT was informed if the caregiver raised further concerns. Children in the Standard Healthcare group followed the same procedure during the screening visit, prior to their outpatient appointment at PCH. However, their results were not reviewed by the MDT. Instead, their care plan was provided during their outpatient appointment.
12-month follow-up visit
All children were scheduled for a 12-month follow-up visit, using the same procedure of the screening visit. Caregivers also completed a satisfaction questionnaire regarding the Ear Portal service. The MDT asynchronously reviewed the findings of all children. For the Ear Portal group, the MDT provided care plans for children with abnormal results before being discharged from the study. Children in the Standard Healthcare group with abnormal findings were re-referred to their ENT consultant for further action. All children with normal findings were discharged from the study and hospital.
Repeat visit
Repeat visits took place when recommended by the MDT or when requested by caregivers before the 12-month follow-up visit. Repeat visits involved the same screening visit procedure and MDT review detailed previously and were only offered to the Ear Portal group.
Present study
The present study included children in the Ear Portal group who completed their screening visit and received a care plan from the MDT between June 2020 and June 2022. Waiting times of the Standard Healthcare group were compared to those of the Ear Portal group.
Ethics
Ethics approval was obtained from Child and Adolescent Health Service, the Western Australian Aboriginal Health Ethics Committee and The University of Western Australia Human Research Ethics Committee. The study was prospectively registered on the Australian New Zealand Clinical Trials Registry (ACTRN1269000039189p).
Analysis
The characteristics of study participants and the ear diagnoses of children in the Ear Portal group as determined by the MDT were summarised using descriptive statistics. Outcome variables of the study included waiting time to assessment (from pre-consent to screening visit) and waiting time to review (from screening visit to MDT review) for children in the Ear Portal group. The overall waiting times for the Ear Portal group (from pre-consent to care plan provision to caregivers) and the Standard Healthcare group (from referral to the hospital to the face-to-face ENT outpatient appointment) were also assessed. The time required to complete the screening visits and the MDT review was examined. Outcome variables were summarised using mean and standard deviation (SD) for normal distributions, and median and interquartile range (IQR) for asymmetric distributions. Outliers related to waiting time outcome variables were identified and investigated. The statistical analysis was conducted using SPSS, version 28.0.
Results
Characteristics of the study population
Between June 2020 and June 2022, 369 recruitment opt-out letters were sent to caregivers of eligible children. Of those, 282 were not enrolled in the study due to various reasons including caregiver unable to be contacted (39.7%) or declined participation (10.6%), the child was receiving or had received specialist care (e.g. privately) (20.6%), had a complex medical history (7.1%), was enrolled without meeting the eligibility criteria (6.0%), or did not receive a care plan before June 2022 (7.5%). A total of 87 children were eligible for inclusion in the analysis; 82 children in the Ear Portal group and five children in the Standard Healthcare group.
The mean age of eligible children was 3.2 years (SD = 1.9; 50.6% females). Eighteen children were triaged by the hospital staff as category 2 (‘semi-urgent’) referrals and 69 as category 3 (‘not urgent’) referrals. Most children in the Ear Portal group (90.3%) received a bilateral diagnosis by the MDT. Bilateral normal findings were found in 43.9% (Table 1). The most common middle ear pathologies were bilateral OME (19.5%) and bilateral AOM with intact TM (9.8%). The ear diagnosis was unknown for seven children in both ears (8.5%) and one child in one ear (1.2%), due to poor reliability of results (e.g. lack of child's compliance). Table 2 summarises the audiological findings of the Ear Portal group which were used by the MDT to make ear diagnoses. These results in addition to the information from the developmental and case history questionnaires were also used to make clinical decisions and care plans. These included: audiology plus ENT face-to-face follow-up (39.0%), ENT face-to-face follow-up (32.9%), Ear Portal repeat visit (11.0%), waitlist for surgery (6.1%), discharge from care (6.1%) or referral to GP for management (4.9%). MDT decisions for ENT face-to-face follow-up only were based on caregivers’ concerns not related to ears (e.g. obstructive sleep disorder symptoms), while decisions for audiology plus ENT face-to-face follow-up were based on a diagnosis of middle-ear disease or the lack of sufficient hearing screening and/or other audiological results collected during the screening visit.
Ear-related diagnoses of children in the Ear Portal group as determined by the MDT.
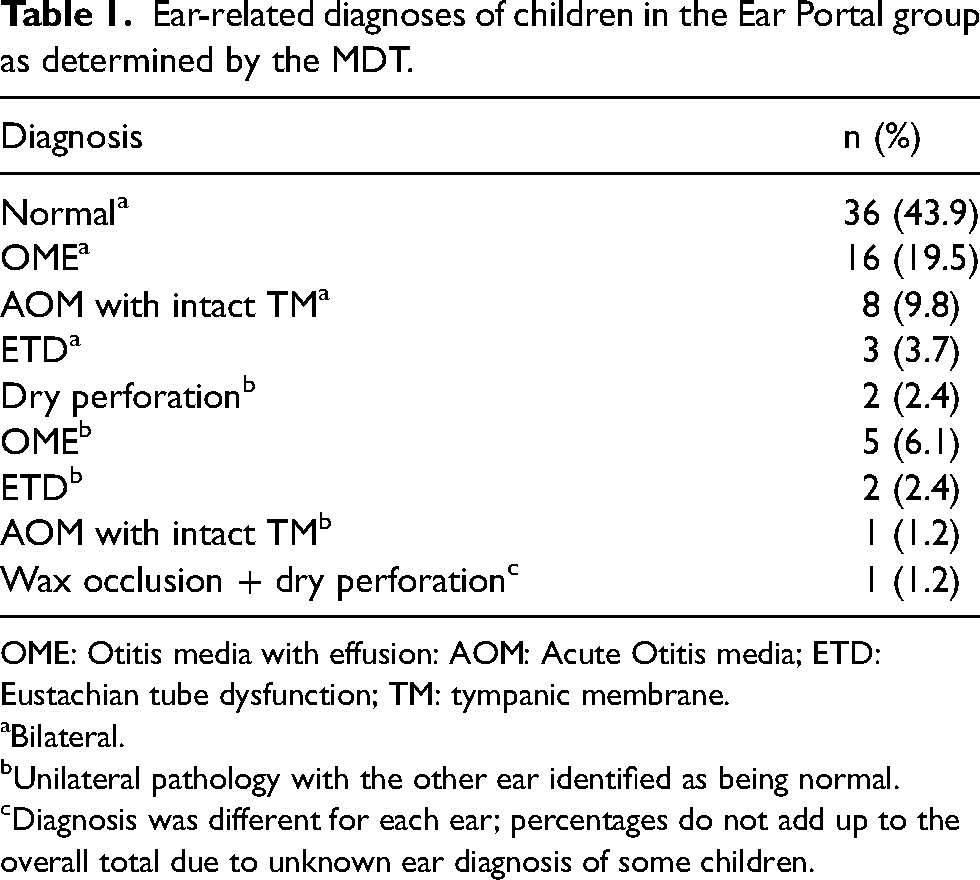
OME: Otitis media with effusion: AOM: Acute Otitis media; ETD: Eustachian tube dysfunction; TM: tympanic membrane.
Bilateral.
Unilateral pathology with the other ear identified as being normal.
Diagnosis was different for each ear; percentages do not add up to the overall total due to unknown ear diagnosis of some children.
Frequencies of the audiological findings of the Ear Portal group.
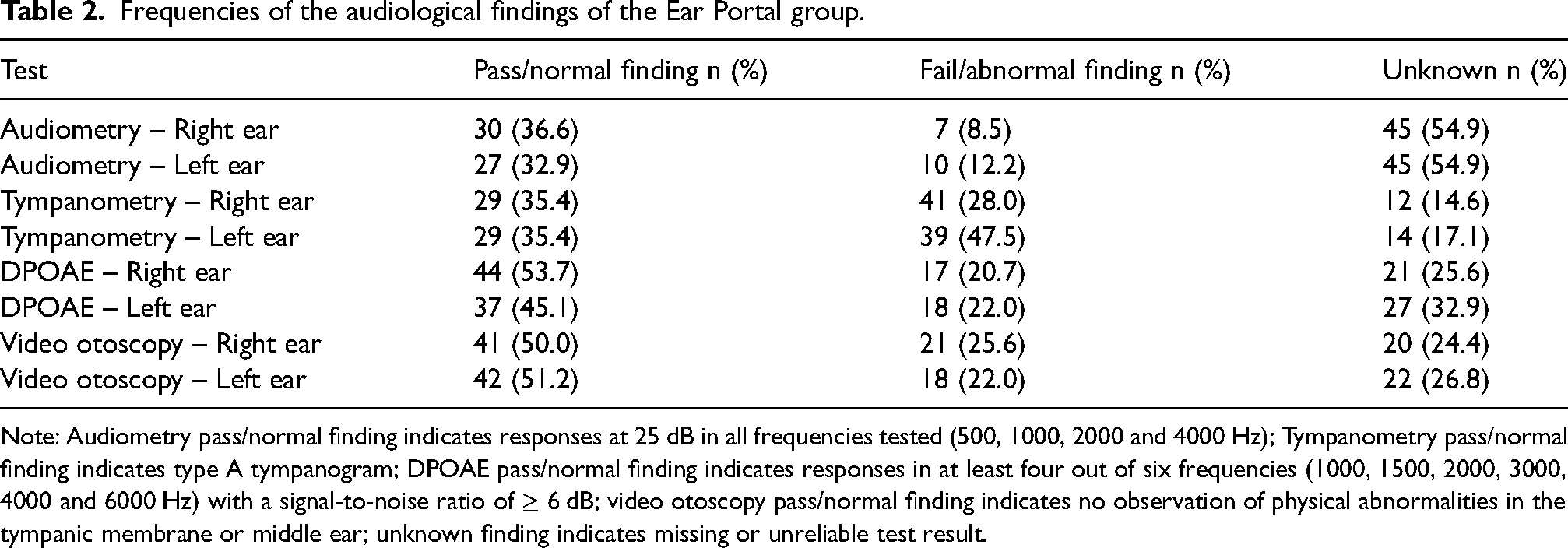
Note: Audiometry pass/normal finding indicates responses at 25 dB in all frequencies tested (500, 1000, 2000 and 4000 Hz); Tympanometry pass/normal finding indicates type A tympanogram; DPOAE pass/normal finding indicates responses in at least four out of six frequencies (1000, 1500, 2000, 3000, 4000 and 6000 Hz) with a signal-to-noise ratio of ≥ 6 dB; video otoscopy pass/normal finding indicates no observation of physical abnormalities in the tympanic membrane or middle ear; unknown finding indicates missing or unreliable test result.
All children who were discharged from care had bilateral normal findings. Others with bilateral normal findings were scheduled for ENT face-to-face follow-up due to concerns not related to ears (51.6%), ENT plus audiology face-to-face follow-up due to concerns regarding hearing, speech, and/or language when hearing results were unavailable (16.1%), Ear Portal repeat visit due to incomplete or unreliable audiometric results (9.7%), or referred to GP for management (6.5%). Diagnoses and care plans of the Standard Healthcare group were unavailable as they were provided during their ENT outpatient appointments.
Waiting times
The median waiting time to assessment was 14 days (IQR = 21), while the median time to MDT review was 8 days (IQR = 8) (Figure 2). The median overall waiting time of the Ear Portal group was 28 days (IQR = 19.8), while the mean overall waiting time for the Standard Healthcare group was 450 days (SD = 211.4) (Figure 3). Nearly all children (98.8%) in the Ear Portal group received care within the clinically recommended timeframes for their triage category (i.e. category 2 = 90 days category 3 = 365 days) compared to only 20% of children in the Standard Healthcare group who were seen within these timeframes.
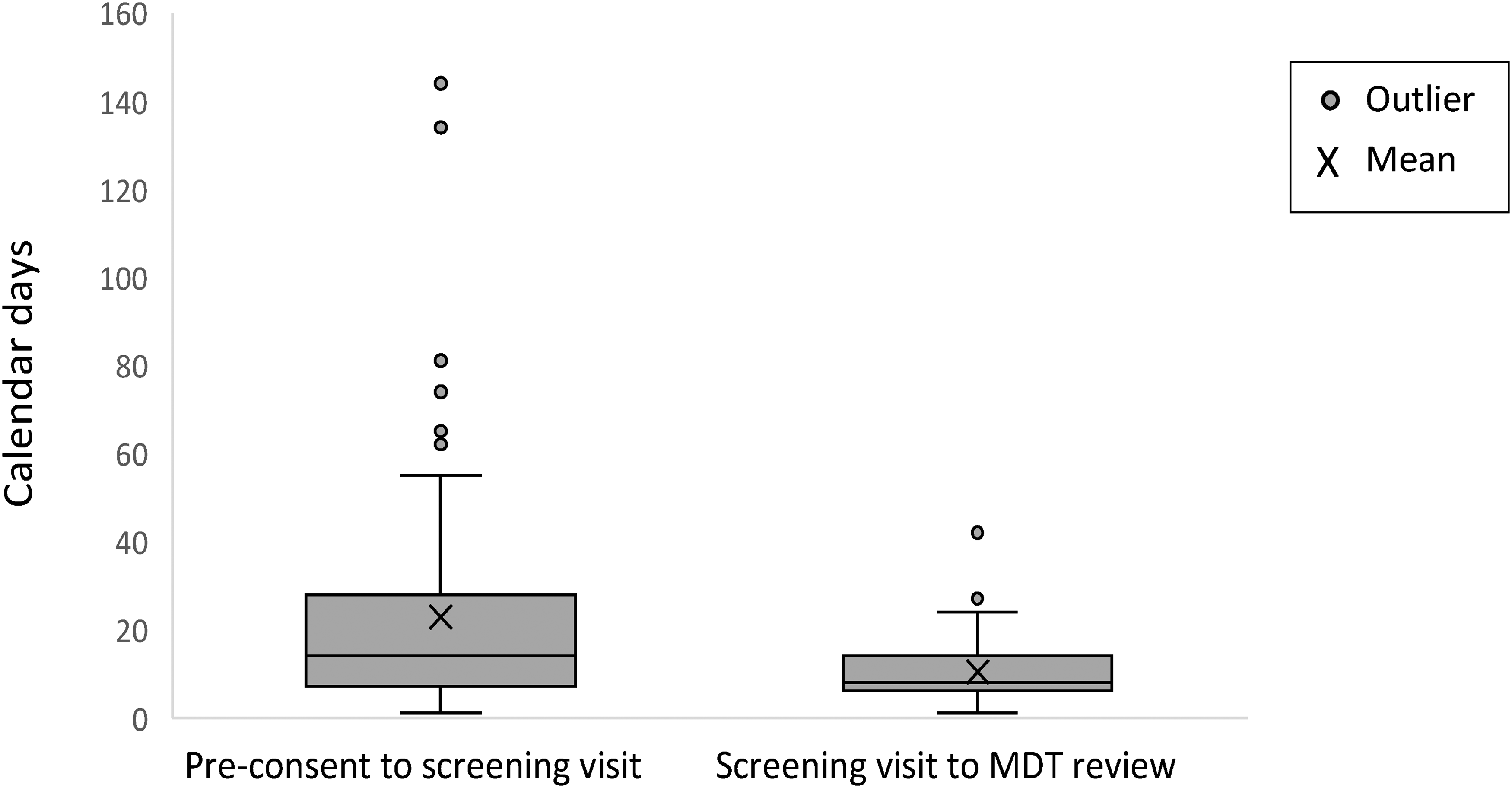
Ear Portal group waiting times to screening visit and multidisciplinary team (MDT) review.
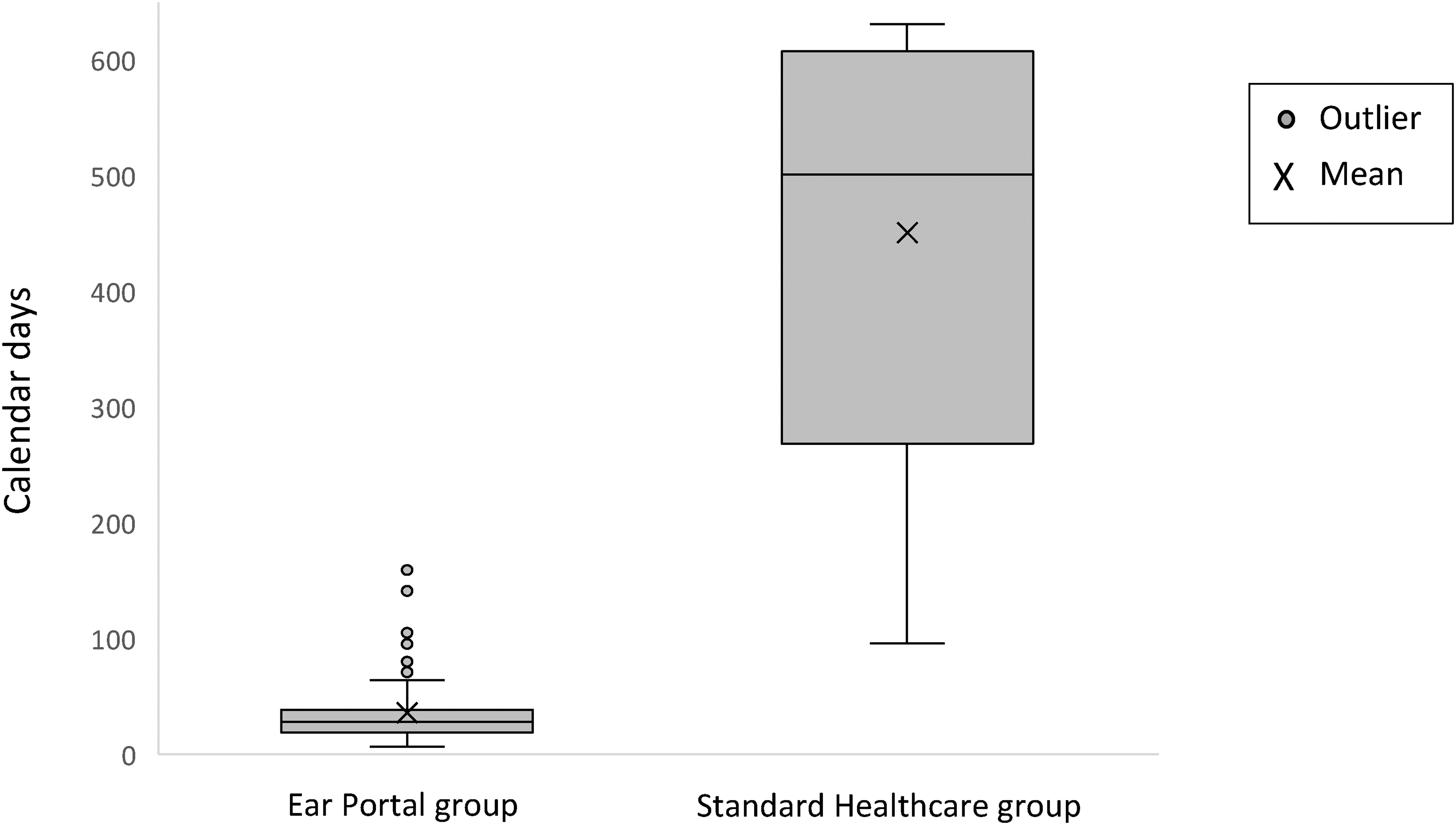
Overall waiting times of the Ear Portal group and Standard Healthcare group.
Screening visits were usually offered to caregivers of children in the Ear Portal group on the next working day (Figure 2). However, these appointments were booked based on caregivers’ preferences, broadening the range of waiting times to assessment (1–57 days) and overall waiting time (6–64 days).
We identified 19 outliers related to waiting times in the Ear Portal group. These outliers were investigated to identify the possible causes for extended waiting time to assessment (n = 7; range = 62–144 days), waiting time to MDT review (n = 4; range = 27–44 days), and the overall waiting time (n = 8; range = 71–159 days). Causes of outliers were classified into three categories: caregiver-related delays (e.g. choice of later dates; n = 15), staff-related delays (e.g. staff unavailability; n = 1), and holiday-related delays (e.g. Christmas holiday; n = 4).
Time required for the screening visit and MDT review
The mean time for the screening visit completion in the Ear Portal group was 37.6 min (SD = 8.3) per participant. The mean and maximum times for MDT review were 5.1 min (SD = 1.7), and 10 min per participant, respectively (Table 3).
Completion time for a screening visit and MDT review (in minutes).
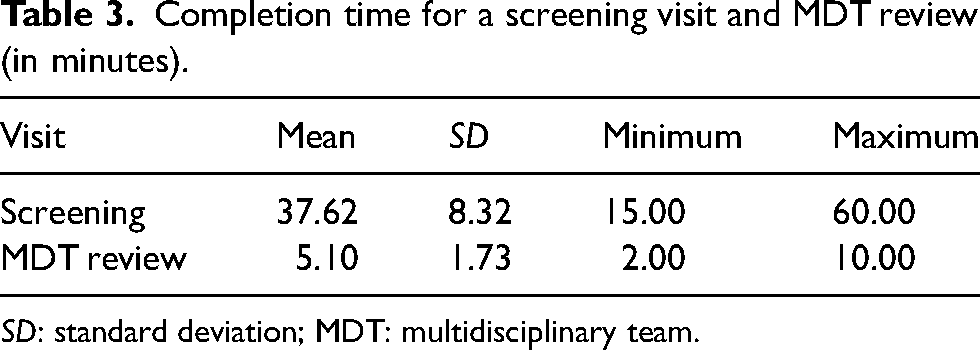
SD: standard deviation; MDT: multidisciplinary team.
Discussion
This study introduced a new telehealth service and investigated its impact on improving access to specialist ear-health services in a metropolitan tertiary children's hospital. The Ear Portal service reduced waiting times of children referred due to OM-related concerns to a median of 28 days to receive specialist ear health care from 450 days for the Standard Healthcare group to access face-to-face specialist services. Our finding is in line with that of Smith et al., 20 which showed that a telehealth school screening service in a remote Aboriginal community in Queensland reduced waiting time to a median of 29 days from the date of the referral by a local health worker to the date of ENT specialist asynchronous review. This service helped in identifying urgent cases who were prioritised and booked for the next outreach clinic.
The clinical recommendations for maximum waiting times for the triage categories included in this study are 90 and 365 days for category 2 and 3 referrals, respectively. These timeframes are usually difficult to adhere to in public hospitals in Australia, as the number of referrals often exceeds the specialists’ capacity.12,14,15,17,24 The median waiting time for receiving a diagnosis and care plan by the MDT in the Ear Portal service was 28 days, which is within the clinically recommended timeframes. Only one child (1.2%) in the Ear Portal group had to wait longer than these timeframes, compared to 80% of children in the Standard Healthcare group. Extended waiting times in the Ear Portal group were mainly caused by caregiver-related delays, while only one outlier was linked to staff-related delays.
One advantage of this service was the reduction in specialists’ time required to provide a diagnosis and treatment plan, which was only required during MDT asynchronous review. Our results showed that the mean and maximum times for reviewing and discussing the results of a participant, in addition to providing individualised care plans by the MDT was 5.1 and 10.0 min, respectively. In comparison, the time required for audiology and ENT initial appointments in standard care is fixed at 45 min and 15–20 min, respectively. The Ear Portal MDT was able to make clinical decisions for approximately 90% of children based on pre-recorded data by non-clinicians during the screening visits that required an average of 37 min. Therefore, this service resulted in noticeable time saving for clinicians. Although having non-clinicians test children can save clinicians’ time, it may have limited opportunities for caregivers to discuss their concerns during the appointment or receive an interpretation of their child's findings from the specialist directly, which is one limitation of the service.
A large proportion of children (43.9%) had normal findings at the time of assessment and could potentially be removed from the ENT outpatient waiting list. However, over half of those children were scheduled for ENT face-to-face follow-up due to other symptoms mainly related to an obstructive sleep disorder. Another 16.1% were scheduled for audiology plus ENT face-to-face follow-up, which was overall the most frequent recommendation in this study. The lack of age-appropriate hearing tests (e.g. Visual Reinforcement Audiometry) in this study, leading to unknown hearing status for 54.9% of children, is likely to have prompted the need for further face-to-face follow-ups. These findings encourage incorporating age-appropriate hearing tests and obstructive sleep disorder questionnaires in the Ear Portal service or other similar services. This may help reduce the caseload in hospitals and improve access to face-to-face care for children with more complicated ENT conditions.
On the other hand, approximately 84% of children with normal audiological findings did not require further audiology face-to-face follow-up. Therefore, the Ear Portal service could also help reduce the workload on the Audiology clinic in the hospital. Also, 6.1% of children were directly waitlisted for surgery, who might have otherwise waited for extended periods for ENT review in the standard healthcare pathway prior to being waitlisted for surgery. As such, the service could also facilitate early intervention, which could help reduce the burden of recurrent OM for children requiring surgical interventions.
The benefits of telehealth in improving access for patients in remote and rural areas have been previously demonstrated.19–23 This study extends upon this and has shown the potential benefit of a hospital-centred telehealth service in streamlining health practices in metropolitan areas where specialist services are in high demand.
This study was limited by the small number of children in the Standard Healthcare group (n = 5). The outpatient ENT clinic at PCH was closed for approximately 18 months during the COVID-19 pandemic for non-urgent cases, which delayed and reduced our ability to recruitment in the Standard Healthcare group. However, our findings showed that waiting times of the Standard Healthcare group were up to 631 days, which is in line with the previously published data that showed that waiting times can be up to two years for children's initial ENT appointment in a public hospital in the state where this study was conducted. 16 Future studies will need to evaluate the long-term efficacy of this methodology to determine if patients who are discharged then represent with the same medical condition. Greater efforts to train primary healthcare providers in the diagnosis and management of OM could also be done to help reduce the number of referrals to tertiary care and facilitate more timely diagnosis and management in the community without requiring specialist care.
Conclusion
This study demonstrated the benefits of a telehealth service within a tertiary children's hospital in Australia. The Ear Portal service reduced waiting times to a median of 28 days compared to 450 days in the Standard Healthcare pathway and could therefore improve access of children with OM-related concerns to specialist care. The median waiting time in the Ear Portal service was within the recommended timeframes. Specialists’ involvement in the service was only required in reviewing findings of children that could be collected by non-clinicians. Therefore, services like the Ear Portal can be adopted as a process going forward or expanded to other sites to help reduce waiting times to access care, reduce the amount of time required from specialists to provide a diagnosis and treatment plan, and therefore increase the capacity of hospitals to manage high caseloads.
Footnotes
Acknowledgements
This work is supported and funded by Telethon-Perth Children's Hospital Research Fund, the Medical Research Future Fund via the Western Australia Health Translation Network Rapid Applied Research Translation program. Chris Brennan-Jones was supported by a National Health and Medical Research Council Fellowship (GNT 1142897) and a Western Australian Department of Health Emerging Leader Fellowship. We thank all the children and caregivers who took part in the study. We also thank Kathryn Jajko and all Ear Portal team members at the Telethon Kids Institute, and medical, nursing and administrative staff from the PCH ENT Department, Erin Maywood and Nicole Irvine from the PCH Audiology Department, and Robert Proctor from the PCH Telehealth Department for their significant contribution to the development and implementation of this project. We acknowledge that this research was undertaken on Noongar Whadjuk Boodja, the traditional land of the Whadjuk Noongar people, and acknowledge their Elders past, present and emerging.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Medical Research Future Fund via the Western Australia Health Translation Network Rapid Applied Research Translation program, Telethon-Perth Children’s Hospital Research Fund, National Health and Medical Research Council, Western Australian Department of Health.