
Abstract
Although the use of audiovisual telemedicine has grown in recent years especially during recent COVID-19-related lockdowns, evidence shows there is still a lack of tools that can be used for the assessment of telemedicine encounters. The few validated questionnaires that are available for assessing telemedicine encounters are not often used. Non-validated questionnaires dominate research, leading to results that cannot be compared or extrapolated to other research or medical sites. Development of standard measures for the assessment of telemedicine encounters has been advocated by stakeholders. The objective of this study is to provide a comprehensive set of measures by developing a conceptual approach and a preliminary Telemedicine Assessment Toolkit (TAT) for the assessment of audiovisual telemedicine encounters. A two-step conceptual approach was used to identify potential domains and sub-domains by qualitative analysis of a pool of questions from studies published from 2016 to 2021. Questions were adopted from validated questionnaires or generated to represent the underlying concept of each sub-domain, resulting in a core block of comprehensive questions. A toolkit is proposed with question-measures that cover the sub-domains relevant to the assessment of telemedicine encounters. This study recommended 11 domains to be used for the assessment of telemedicine encounters: “usability,” “patient satisfaction,” “patient–provider interaction,” “patient perspectives,” “telemedicine readiness,” “qualitative feedback,” “comparison to standard (in-person) care,” “privacy,” “technology,” “patient feeling,” and “patient costs.” Of the 11 domains, 26 underlying sub-domains were created. From the subdomains, a 30-question core block was proposed. The core-block together with a precursor block aimed to retrieve demographic/patient characteristics and, together with a customizable clinical outcomes block, complete the comprehensive toolkit. The toolkit, upon testing and validation, would enable researchers and system owners to assess patient-oriented aspects of audiovisual telemedicine encounters more accurately and accelerate the adoption of common audiovisual telemedicine assessment measures.
Introduction
Telemedicine provides continuity of care by enabling the exchange of medical information from one site to another via electronic communications with the main goal of improving the health of patients. Telemedicine as a routine mode of delivering healthcare has continued to further accelerate with improvements in communication infrastructure and coordinated global response to crises such as disease outbreaks. Telemedicine services are conducted using different systems like telephonic, store and forward (asynchronous), digital remote monitoring, and more recently wearable devices. Synchronous audiovisual encounters or video consultations have grown in use due to the enhanced capacity of real-time visual cues important for patient engagement, clinical observation, and visual assessment. 1
Despite the growing adoption of audiovisual telemedicine, insufficiency in the scientific evidence derived from telemedicine assessment persists, particularly in effectiveness, impact on patient management, and costs. 2 Systematic reviews continue to highlight the need to standardize populations, interventions, and outcome measures to reduce study heterogeneity, facilitate meta-analysis and develop controlled studies with larger samples.2,3
Non-validated measures are used in assessing telemedicine encounters,4,5 leading to inability to combine and compare study results. Validated questionnaires specific for telemedicine such as the Telemedicine Satisfaction Questionnaire (TSQ), the Telehealth Usability Questionnaire (TUQ), Telemedicine Satisfaction and Usability Questionnaire (TSUQ), the Patient Assessment of Communication in Telemedicine (PACT), and the Telemedicine Satisfaction Scale Questionnaire (TESS) are not often used despite being available in the literature.6–10 Limitations contributing to the low use of validated questionnaires identified in the literature include neglect of key assessment criteria such as patient views and access to care, while focusing on satisfaction and clinical effect.11,12 The lack of built-in mechanisms for continuous improvement despite the rapid change in technology over time is also an issue with current validated assessment tools. 7 Because of the lack of standard measures, the consistency of assessment strategies and the development of standardized measures are research priorities across health care. 13
Standard measures covering the essential elements of a discipline are needed because they enhance the ability of researchers to combine data from several studies, improve the strength of evidence and broaden its applicability to several groups of people and situations. 14 Several initiatives have been launched to develop tools to collect uniform datasets.14–16 The Global Tobacco Control Surveillance program by the Centers for Disease Control and Prevention-CDC, 17 and the Patient Reported Outcomes Management Information System-PROMIS 18 used approaches that integrate the collective wisdom of researchers within their field to design comprehensive assessment tools. Similarly, in developing the quality of life questionnaires,19–21 the methodologies utilized consensus domains to address the problem of heterogeneity.
Prior literature describe how research can conceptualize attributes into domains.22,23 When combined, theories and concepts help researchers to understand and explain what needs to be comprehensively measured. 24 To achieve general acceptance and adoption, uniform measures for the assessment of telemedicine encounters sourced from existing literature should be developed around a conceptual approach, similar to the work done in other health fields.
A previous study retrieved questions from validated and non-validated questionnaires used by researchers in the literature from January 2021 through November 2021, 25 creating a question pool that can be analyzed to identify conceptual domains.
The goals of this study were (1) to identify the most common domains for the assessment of audiovisual telemedicine encounters, (2) to propose a conceptual approach with key domains and sub-domains to be used for the assessment, (3) and to develop a preliminary toolkit with comprehensive measures to be used for the assessment of audiovisual telemedicine encounters.
Methods
We used a two-step conceptual approach that led to the development of a preliminary comprehensive toolkit for the assessment of audiovisual telemedicine encounters. We integrated qualitative and quantitative techniques in a mixed method design, as identified in prior literature. 26
Domain and sub-domain identification and questions categorization
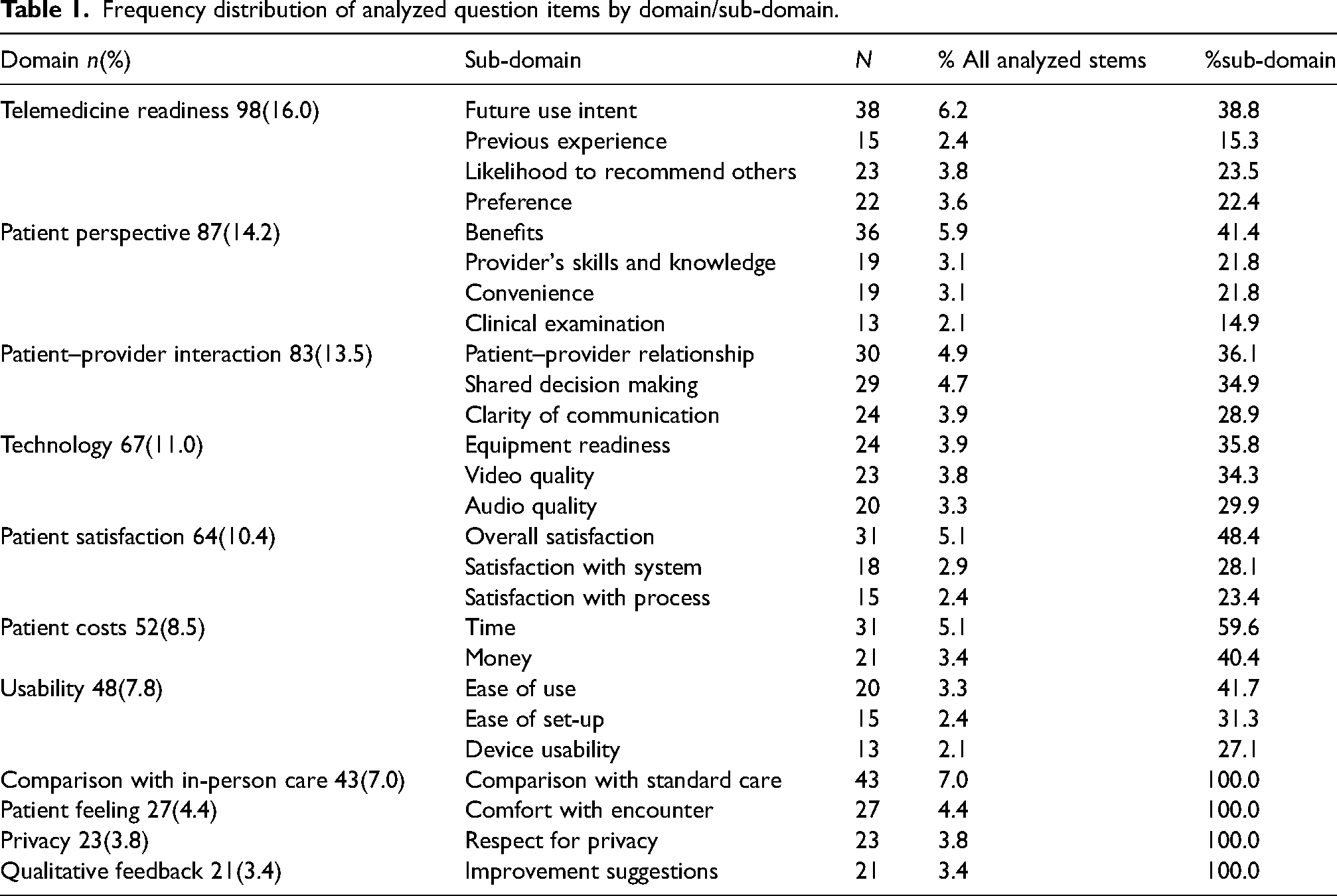
Previous research identified 702 unique question stems used to assess telemedicine encounters. 25 Two authors (RA and GD) reviewed 702 questions to identify domains using open coding. Open coding for unique domains continued until saturation occurred with no new domain being identified. Existing literature was reviewed to ensure no domains were overlooked. Then, two authors (RA and GD) proceeded to associate each question to a domain working independently. To categorize the question stems that the two authors assigned to different domains, author 1 (RA) reviewed the non-matched items coded by author 2 (GD), while GD reviewed the non-matched items coded by RA. Disagreements were resolved by consensus based on discussion of the keywords associated with each criterion to identify a set of consensus codes and domains (Table 1).
Frequency distribution of analyzed question items by domain/sub-domain.
For each domain, a similar approach was used to identify sub-domains. The question stems from each sub-domain were reviewed for their sentence structure and archetype questions that best represent the sub-domain (Table 2).
Question measures for Telemedicine Assessment Toolkit Core Questionnaire generated from underlying sub-domains for Telemedicine encounters, uniformly adopted response scale and item sources
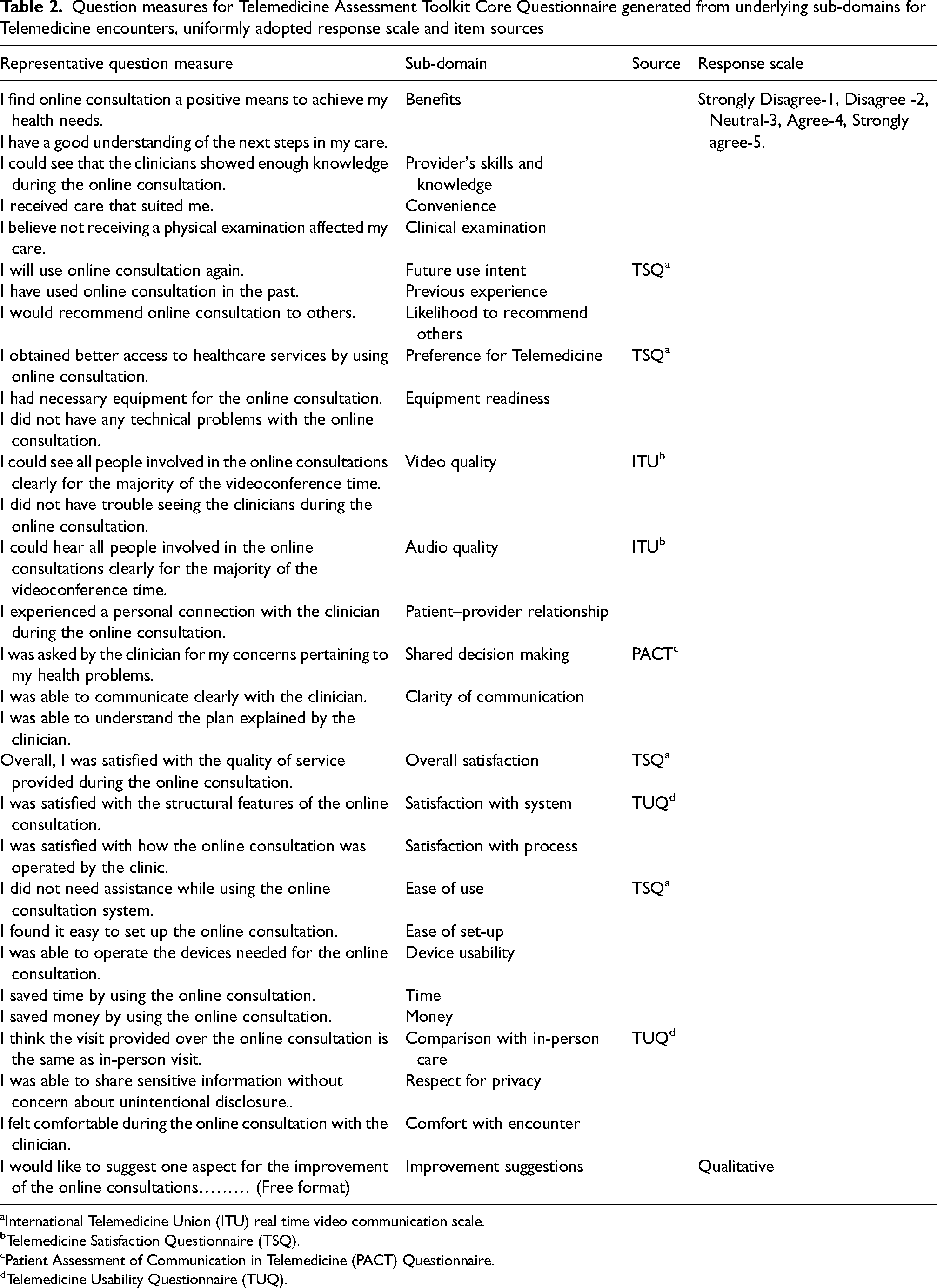
International Telemedicine Union (ITU) real time video communication scale.
Telemedicine Satisfaction Questionnaire (TSQ).
Patient Assessment of Communication in Telemedicine (PACT) Questionnaire.
Telemedicine Usability Questionnaire (TUQ).
Tool kit item generation
For each of the selected sub-domains, we listed the unique question stems coming from the previously published article. 25
If an existing validated assessment tool had been used to assess the sub-domain, one or more specific questions from that validated questionnaire were selected for inclusion in the tool kit. For the novel sub-domains, one or more questions were generated from the list of question-stem of the sub-domain, and if needed, the item was rewritten slightly to match the uniform answers scale we adopted. The uniform answer scale used was a 5-point Likert agreement scale from strongly disagree to strongly agree.
The final comprehensive question list for the toolkit core block is a matrix of all questions (item-measures) in domains that were considered important for widespread acceptance and implementation in line with prior recommendations for robust telemedicine assessment27,28 (Table 2).
Results
At the end of the domain identification step, 19 core domains emerged. The domains were: technology (n = 67, 9.5%), comparison to in-person care (n = 65, 9.3%), patient satisfaction (n = 64, 9.1%), future/previous use (n = 57, 8.1%), communication (n = 53, 7.6%), patient costs (n = 52, 7.4%), provider evaluation (n = 49, 7.0%), patient view of impact (n = 49, 7.0%), usability (n = 48, 6.8%), access to care (n = 42, 6.0%), qualitative feedback (n = 27, 3.9%), patient feeling (n = 27, 3.9%), privacy (n = 23, 3.3%), likelihood to recommend telemedicine (n = 23, 3.3%), non-relevant questions (n = 16, 2.3%), patient demographic and characteristics (n = 15, 2.1%), overall rating (n = 11, 1.6%), reason to use telemedicine (n = 8, 1.1%), and clinical outcome (n = 6, 0.9%).
The domain “access to care” represents the patient's opinions on how well the telemedicine encounter was able to deliver quality care to the patient at the time and place the patient needed it most, while the domain “patient view of impact” represents how well the telemedicine encounter was able to fulfill the psycho-social needs of the patient as assessed by the patient. The “clinical outcome” domain assesses how the telemedicine encounter affected the individual's daily functioning and well-being. 29
The authors removed five domains. The non-relevant questions domain (n = 16, 2.3%) included questions of a general nature, for example, “Do you use social media” or “did you travel last month to Hubei province,” etc. The domain “reason to use telemedicine (n = 8 1.1%)” was considered of little relevance given few questions in the category, the domain “overall rating” (n = 11, 1.6%) was excluded because, after testing, the toolkit aims to provide a single composite score for summative analysis. Clinical outcomes domain (n = 6, 0.9%) was found to be already standardized for a wide range of conditions in medicine within the Patient Reported Outcome Management Information System (PROMIS). 30 The domain “patient demographic and characteristics” (n = 15, 2.1%) includes questions that the electronic system could auto generate, for example, patient health condition, demographic and location or type of device connection.
Among the remaining 14 domains, some domains overlapped, and the authors decided to combine them. The domain “provider evaluation” and “communication” were merged into a domain called “patient–provider interaction.” Similarly, the “likelihood to recommend” and “future/previous use” were merged into “telemedicine readiness.” Finally, “access to care” and “patient view of impact” were merged under “patient perspectives.”
After an additional analysis of the questions, sub-domains were identified for each of the domains. Five sub-domains that had less than 13 questions or 2% of the total number of questions among the domains were removed from further analysis: scheduling, technical support availability, other costs, location of encounter, telemedicine advantages and disadvantages. The final 26 sub-domains under the 11 domains representing 613 questions of the initial 702 questions are reported in Table 1.
Question measures generated for toolkit
The demographic and clinical domains identified as already having established sources from which data could easily be obtained to complete a comprehensive assessment were designated as customizable blocks for the toolkit. Along with the core block of encounter assessment questions generated in this study, the three blocks created a three-block functional structure for the proposed tool kit.
The comprehensive core block of question measures listed in the toolkit is organized under 26 sub-domains, assembled under the 11 domains, which are relevant to assessing telemedicine encounters.
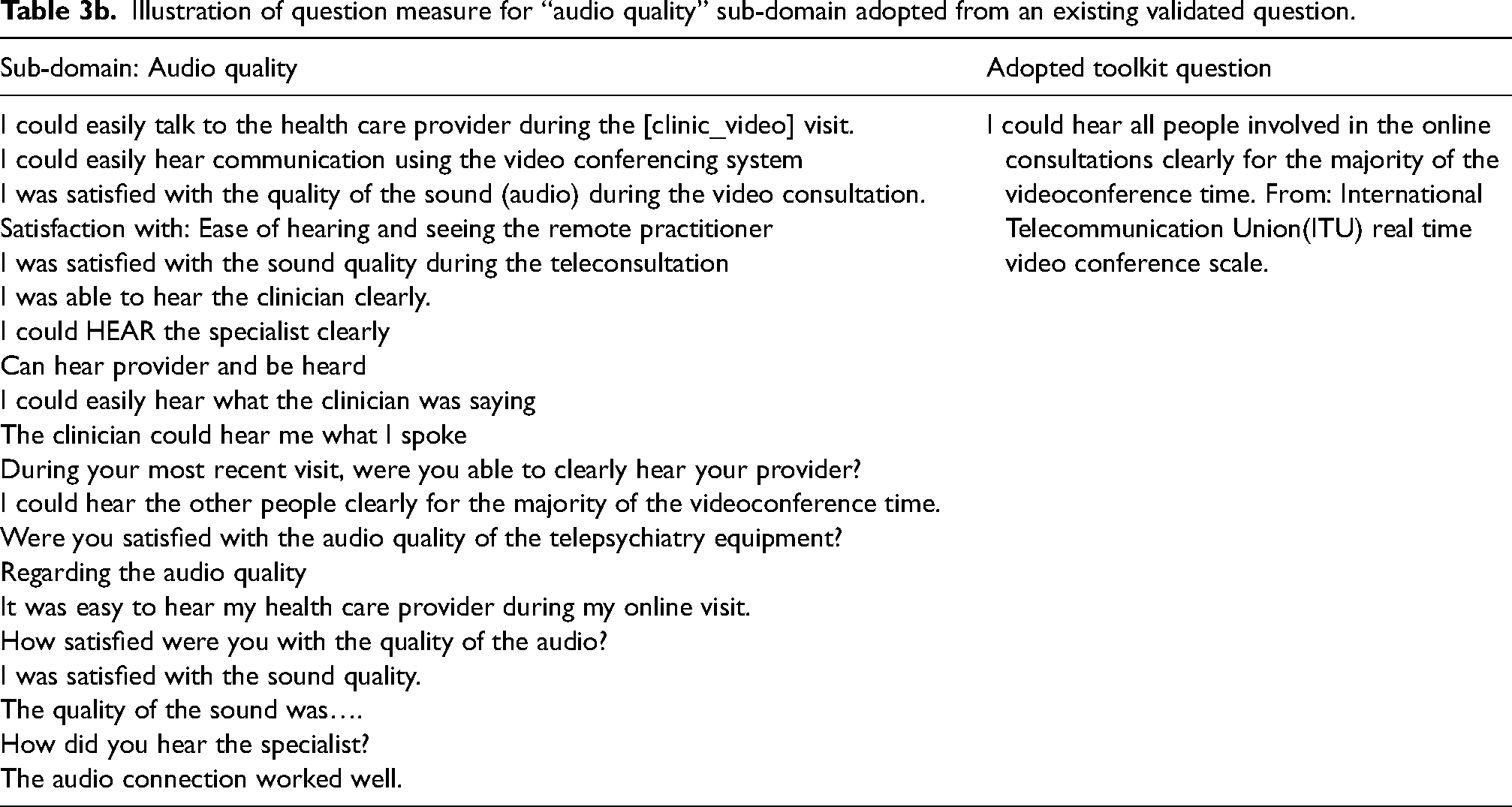
For each sub-domain, a search was done among validated questionnaires to find one or more question measures that summarize all questions identified for that specific core concept. For instance, for the sub-domains, “overall satisfaction,” “future use,” “ease of use,” and “ preference for telemedicine,” we used one question each from the TSQ. 6 For the sub-domains, “satisfaction with system” and “comparison to in-person care,” we used one question each from the TUQ. 7 For the sub-domain “shared decision making,” we used one question from the PACT questionnaire. 10 For the sub-domain “audio quality,” we used one question from the international telecommunications union (ITU) scale for real time video communication, and two questions from the same ITU scale was used for the sub-domain “video quality.” 31 Questions adopted from each validated questionnaire and their sources are indicated in Table 2 with an illustration for the sub-domain “video quality” in Table 3b.
For the 17 sub-domains where a question from a validated questionnaire could not be found, we generated a new question as illustrated using the sub-domain “clarity of communication” in Table 3a. The comprehensive matrix of 30 questions for the core block, with a 5-point Likert agreement scale from strongly disagree to strongly agree and associated sub-domains is reported in Table 2.
Illustration of a question measure for “clarity of information” sub-domain generated from existing non-validated items.
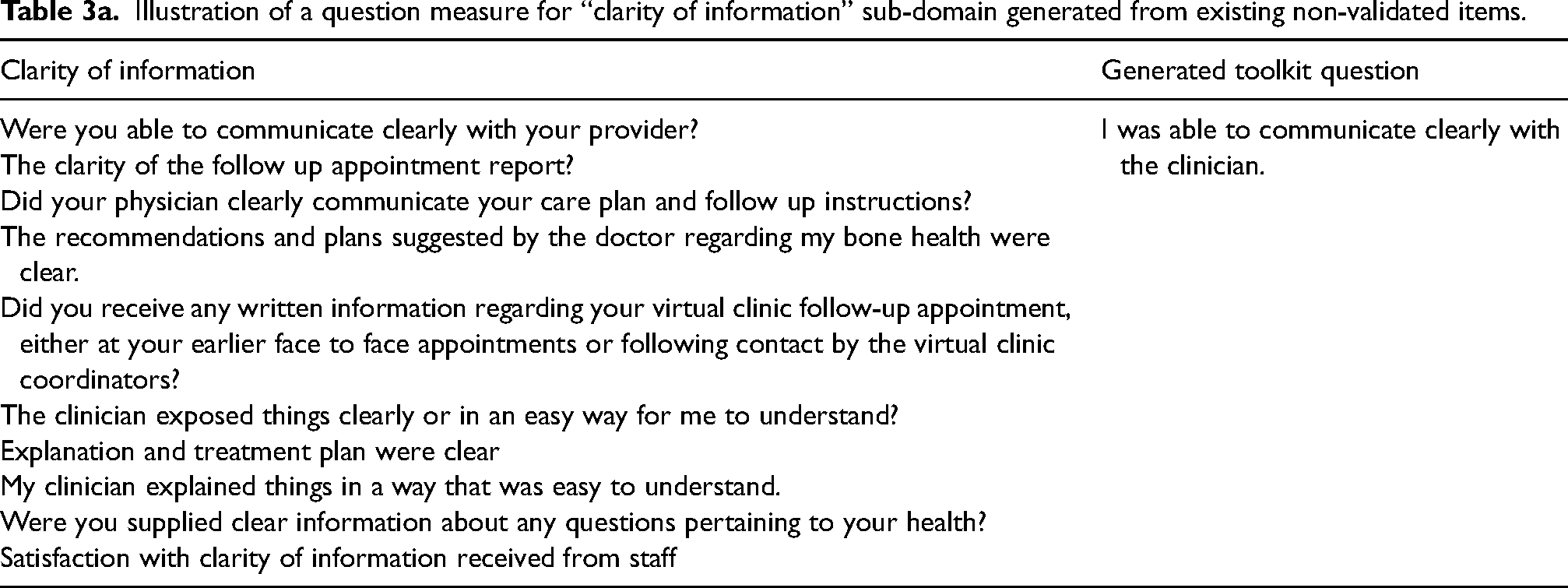
Illustration of question measure for “audio quality” sub-domain adopted from an existing validated question.
Discussion
We have presented a novel conceptual approach and proposed a toolkit with comprehensive measures for assessing audiovisual telemedicine encounters. The goal is to reduce heterogeneity with non-validated measures and improve the use of validated measures in assessing telemedicine encounters. This approach aims to create meaningful measures from the outset as advocated by psychometricians.32,33
Conceptual approach
This study recommended 11 domains: patient satisfaction, patient–provider interaction, patient perspectives, patient feeling, patient costs, technology, privacy, telemedicine readiness, usability, qualitative feedback, and comparison to standard (in-person) care. These domains have received substantial contributions from researchers in prior telemedicine encounter research and we applied consensus judgments and objective quantitative rules to conceptualize and organize them under coherent domains and sub-domains. This approach is consistent with prior methodology that use representative review of the work that has been done to provide the basis for formulating a more comprehensive model of information system success, 34 and evaluating usability of mobile applications. 35 Contents of each domain were then interpreted based on what is known in the literature.
The results of our analysis, while being consistent with other studies, provided more insight towards a comprehensive assessment strategy. For instance, we found that, patient satisfaction was a focus of many researchers with 10.4% of analyzed questions aiming to assess satisfaction, similar to other studies which identified satisfaction as a focus of researchers, to the neglect of other aspects. 11 In addition, we also found that four other domains, patient perspective (14.2%), telemedicine readiness (16.0%), patient–provider interaction (13.5%), and technology (11.0%) were of higher relevance to researchers based on the number of questions asked by researchers to assess these domains, suggesting that researchers in the studies viewed the other domains as more relevant for comprehensively assessing telemedicine encounters. The latent need for objective domains is believable because satisfaction has known limitations as a complex measure, varying based on different factors,28,36 such as user expectation which is affected by culture and values.
The conceptual approach adopted in this study currently includes the domain “comparison to standard (in-person) care,” since it was considered relevant by researchers in the literature, but we consider it a tentative domain, diminishing in relevance in the future. It is foreseeable that the comparisons between telemedicine and in person care will gradually become unnecessary as funding, a skilled workforce and new clinical models of care, propel patients and the healthcare systems to embed telemedicine as routine delivery modality, a scenario predicted by two recent studies.37,38
Toolkit construction
During the process of developing measures, we generated 30 questions representing the underlying conceptual sub-domains (Table 3). The questions cover 94.9% of the potential sub-domains identified from the initial item pool. Each question was designed to measure the essential characteristic of the individual 26 sub-domains and written to be specific and precise, without ambiguous or unfamiliar terms. We made use of word choices using lay language appropriate for different patient reading levels, while avoiding double-barreled phrases and social desirability bias which occurs when respondents conceal their true opinion to make themselves look good to the observer. This approach is consistent with prior instrument development research during the phase of generating measures within the information systems field. 39
Most questions were linked to the 5-point Likert agreement scale while one question was designed to enable qualitative feedback. Despite the rapid change in technology over time, the lack of built-in mechanics for continuous improvement remains an issue with the current validated assessment tools. 7 The qualitative response available in the toolkit will enable system owners and researchers to gather feedback for improvement.
The proposed Telemedicine Assessment Toolkit (TAT) comprises three functional blocks providing assessment of the telemedicine encounters: the demographic block, the core block, and the clinical outcomes block. This adopts a similar method as used in the CDC global tobacco surveys where a core questionnaire set in provided with optional customizable question sets. 17 The demographic block should retrieve from the electronic medical records of the provider demographic and patient characteristics information such as age, sex, socioeconomic status, educational status, patient location, and technology literacy. The core block has 30 questions covering 11 domains as described in this study, while the clinical outcomes block asks questions from the patient reported outcome health measures from the PROMIS system. PROMIS computer adaptive measures are standardized for documenting the impact of illness and health care interventions on an individual's daily functioning and well-being. 29 We propose that the toolkit will allow the researchers or providers to add the specific disease states from the PROMIS to the final questionnaire to be administered.
Since short-term patient assessments and long-term impacts of telemedicine encounters are needed for a successful assessment strategy, we recommend that the toolkit should be administered at regular intervals post-visit. This is essential to establishing disease impact patterns in different contexts over the timespan of multiple telemedicine encounters.
The TAT would enable different users stakeholders within telemedicine to achieve specific goals and tasks. Providers would find it a helpful tool when improving patient–provider interaction, process, and structure of care delivery as well as clinical performance. Third party payers and managed care organizations would find the TAT useful in justifying reimbursement algorithms with comparing in-person to audiovisual telemedicine visits. Researchers will find TAT a simplified tool to adopt in whole, or at the least select measures with uniform word choice which would enhance comparability between studies and simplify pooled analysis of data. From a societal perspective, policymakers and regulators would be able to use the TAT to conduct pilot tests and rely on pooled data from research in the field in designing health, privacy, or licensing policies. Additionally, industry and professional groups would find TAT a comprehensive material for developing generally acceptable standards for telemedicine encounters.
We acknowledge that this research may not have captured every questionnaire available in the literature since the article used to retrieve the questions had a time frame from 2016 to 2021. 25 Also, only patient-focused questionnaires with audiovisual encounters were included. Questions focused on provider assessments, questions not written in English, and questions to be used for pediatric patients were excluded from the study which provided the question stems that were analyzed. 25 The conceptual approach and toolkit may not extrapolate to other telehealth systems, for example, remote monitoring, wearables, or asynchronous modes of telemedicine and studies in other languages. There may also be potential limitation due to non-inclusion of the home health setting in the referenced article. 25 Also, we generated two questions for four of the sub-domains: clarity of communication, equipment readiness, benefits and video quality, a limitation which reflects a need for further refinement of these four multidimensional sub-domains in future studies.
Future studies should focus on “goodness of fit” testing, refinement, calibration by collecting feedback from experts, and validation by field testing while conducting empirical investigations of the relationships between the questions. Also, a systematic review of the articles published since 2021 similar to the one used in this paper should be performed to verify that the TAT questions would still be able to cover all the questions asked.
The toolkit will allow researchers and telemedicine systems to standardize encounter assessment and increase data pooling, statistical power, and interpretation from small settings and diverse telemedicine platforms. While telemedicine could be used to promote and facilitate continuity of care, barriers still exist. For example, according to a survey of hospital and physician practice managers, one-third of telemedicine platforms are not integrated with electronic health records at all and only 17% were fully integrated. 40 The TAT presented in this paper could also serve as first step towards a fully integrated care.
Conclusion
This study uses a systematic and conceptual approach to create comprehensive measures using mixed qualitative and quantitative methods. The toolkit proposed in this study, upon testing and validation, should enable researchers and system owners to assess patient-oriented aspects of audiovisual telemedicine encounters more accurately. The toolkit will also accelerate the attainment of standardized measures and adoption of common audiovisual telemedicine assessment measures.
Footnotes
Acknowledgments
We thank the College of Allied Health Sciences, Interdisciplinary Health Sciences Department and the staff of the Greenblatt Library at Augusta University for the use of library materials and assistance in obtaining full text articles. We acknowledge the support of the staff of the Center for Writing Excellence at Augusta University for editorial review of the toolkit items.
Author contributions
All authors contributed meaningfully to conceptualization, article selection, writing, reviewing, and editing this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.