
Abstract
Introduction
During the COVID-19 pandemic, telehealth services represented a critical tool in maintaining continuity and access to care for adults in the USA. However, despite improvements in access and utilization during the pandemic, disparities in telehealth utilization have persisted. It is unclear what role access and willingness to use telehealth play in telehealth disparities.
Methods
We used data from the nationally representative COVID-19's Unequal Racial Burden (CURB) survey, an online survey conducted between December 2020 and February 2021, n = 5500. Multivariable Poisson regression was used to estimate the prevalence of perceived telehealth access and willingness to use telehealth services among adults with and without chronic conditions.
Results
Overall, 60.1% of adults with and 38.7% of adults without chronic conditions reported having access to telehealth. After adjustment, adults with chronic conditions were more likely to report telehealth access (adjusted prevalence ratio [aPR] = 1.35, 95% confidence interval [CI] = 1.21–1.50). Most adults with and without chronic conditions reported being willing to use telehealth services (85.1% and 79.8%, respectively), and no significant differences in willingness were observed across chronic condition status (aPR = 1.03, 95% CI = 0.95–1.13). Perceived telehealth access appeared to be a predictor of telehealth willingness in both groups (chronic conditions: aPR = 1.22, 95% CI = 0.97–1.54; no chronic conditions: aPR = 1.37, 95% CI = 1.22–1.54). The prevalence of perceived barriers to telehealth was low, with the majority reporting no barriers (chronic conditions = 51.4%; no chronic conditions = 61.4%).
Discussion
Perceived access to telehealth was associated with telehealth willingness. Investing in approaches that increase telehealth accessibility and awareness is needed to improve access to telehealth for adults with and without chronic conditions.
Introduction
With federal regulators expanding telehealth policies and increasing insurance reimbursement for telehealth services during the COVID-19 pandemic, telehealth became an integral part of ensuring continued access to healthcare,1–3 especially for patients in areas with fewer healthcare providers and who travel longer distances to in-person healthcare facilities.1,4–6 However, both before7,8 and during the first year of the pandemic,9,10 studies have shown that disparities in telehealth access and utilization exist (and persist) across race-ethnicity, rurality, and socioeconomic status.7–10 For example, using data from our COVID-19's Unequal Racial Burden (CURB) survey, we previously found that while rural adults were just as willing to use telehealth as non-rural adults, they were less likely to report having access to telehealth services in early 2021. 11 While marginalized communities, especially those with chronic conditions, 12 would benefit from access and utilization of telehealth services, questions remain about how perceived access and willingness to use telehealth services were impacted during the pandemic.
Chronic conditions are the leading cause of disability and account for 7 in 10 U.S. deaths, 13 and racial-ethnic disparities in the prevalence of chronic conditions have been well documented.14–17 Telehealth can maintain continuity of healthcare, 18 which is important for effective chronic care management to improve quality of life. 19 Studies during the pandemic have found that adults with chronic conditions are willing to learn and use telehealth for their medical care,20,21 and at least one study has found those with chronic conditions were more likely to use telehealth. 22
Yet to date, most of the telehealth research during the pandemic has focused on utilization,23–26 as opposed to access or willingness to use telehealth services. Telehealth utilization studies during the pandemic have also largely been restricted to Medicare beneficiaries24,26 or to Black/African American, Latino, and White adults,24–26 limiting generalizability to other populations. A comprehensive assessment of telehealth access and willingness using nationally representative cohorts that include American Indian/Alaska Native, Asian, Native Hawaiian/Pacific Islander, and multiracial communities are still needed. Thus, the purpose of this study was to (1) assess differences in perceived access and willingness to use telehealth services, (2) assess racial-ethnic differences in perceived access and willingness to use telehealth, and (3) identify barriers to telehealth, among a nationally representative diverse cohort of adults with and without chronic conditions living in the USA.
Methods
Study design and participants
This study used data collected from the CURB online survey administered by YouGov, a consumer research firm that uses a proprietary, opt-in survey panel comprised of over 1.8 million U.S. residents to conduct nationally representative online surveys. Panel members are recruited through a variety of methods to ensure diversity, and then matched to a theoretical target sample for each survey.
For this study, the target sample was drawn from the 2018 American Community Survey 1-year sample data and included 500 American Indian/Alaska Native, 1000 Asian, 1000 Black/African American, 1000 Latino (including 500 Spanish-speaking), 500 Native Hawaiian/Pacific Islander, 1000 White, and 500 multiracial adults aged ≥18 years (n = 5500 total). English- and Spanish-speaking status among Latino participants was assigned based on survey language preference; 87.6% of Latino participants who took the survey in Spanish also self-reported poor English-speaking skills. Members who completed the online survey were then proximity-matched and weighed to obtain a nationally representative sample within each racial-ethnic group (e.g. Asian participants were weighted to represent all Asian adults living in the USA).
Surveys were completed between December 8, 2020, and February 17, 2021 and were offered in both English and Spanish (Latino participants only). More information about the CURB survey development and sampling design have been published elsewhere.27,28 The National Institutes of Health Office of Institutional Review Board Operations determined that this study does not qualify as human subjects research because data were de-identified (IRB# 000166).
Perceived access, willingness, and barriers for telehealth
To measure perceived access to telehealth, participants were asked: “Does the place where you usually go for care offer telehealth (virtual) visits?” Response choices included: no, yes, and don’t know. To measure willingness, participants were asked: “Would you be willing to meet with a doctor or nurse by smartphone, telephone, tablet, or computer?” with response options being yes with video, yes without video, and no. Responses were dichotomized into yes (with or without video) versus no for analyses.
We measured perceived telehealth barriers by asking the question: “Do you have any of the following concerns about telehealth or virtual visits? (Check all that apply).” Response options included: (1) I do not have an internet connection; (2) My smartphone has a limited data plan; (3) I may have problems with the quality of the audio or video; (4) I may have problems using the application for the virtual visit; (5) I worry that I may not feel comfortable using the new technology; (6) I do not have a telephone, smartphone, tablet, or computer that will work with the application; (7) I may not have a private place to do a telehealth visit; (8) I have vision or hearing problems that may make it hard to have a telehealth visit; (9) They may not speak my language or have an interpreter available; (10) Other (write-in response); and (11) I have no concerns about using telehealth.
Chronic conditions
Participants were also asked: “Has a medical doctor ever told you that you have any of the following conditions? (check all that apply).” Response choices included: (1) chronic obstructive pulmonary disease (COPD); (2) heart conditions (such as heart failure, coronary artery disease, or cardiomyopathies); (3) type 2 diabetes; (4) chronic kidney disease or dialysis; (5) sickle cell disease; (6) cancer in the past year; (7) immunocompromised state (weakened immune system) from solid organ transplant; (8) obesity; (9) COVID-19; and (10) none of the above. Individuals who selected any of the above conditions besides COVID-19 and obesity were classified as having a chronic condition.
Statistical analyses
Descriptive statistics and chi-square tests were used to compare perceived access to telehealth, willingness to use telehealth, and perceived telehealth barriers across race-ethnicity and chronic condition status. Multivariable Poisson regression was used to estimate differences in the perceived access to telehealth (yes vs. no/don’t know) and willingness to use telehealth between adults with and without chronic conditions. Multivariable Poisson regression was also used to assess racial-ethnic differences in perceived access and willingness to use telehealth, among individuals with and without chronic conditions. Separate models were run for individuals with and without chronic conditions. All models were adjusted for age, gender, urbanicity, census division, health insurance, self-reported physical health, education, family annual income, and perceived access to telehealth (telehealth willingness models only).
We also performed several sensitivity analyses. First, among those with at least one chronic condition, we used multivariable Poisson regression, adjusting for the covariates mentioned above, to assess whether specific chronic conditions were associated with perceived access or willingness. A single model was used to estimate the independent associations. Second, among those with at least one chronic condition, we modeled the association between the number of chronic conditions (multimorbidity vs. single comorbidity) on perceived access and willingness to use telehealth.
All analyses were conducted in SAS version 9.4 (SAS Institute, Inc., Cary, NC) and weighted to obtain nationally representative estimates within each racial-ethnic group. Robust variance estimates were used to account for survey weighting in all models.
Results
Overall, 1152 participants (21.0%) reported having at least one chronic condition. The prevalence of chronic conditions, stratified by sociodemographics, is reported in Supplemental Table 1. American Indian/Alaska Native adults (32.0%) had a higher prevalence of chronic conditions, compared to all other racial-ethnic groups (15.2%–23.5%), P < 0.0001. Increasing age, lower education, and poorer self-reported physical health were also associated with higher prevalence of chronic conditions, P < 0.0001 for all (Supplemental Table 1). No other meaningful differences in the prevalence of chronic conditions across sociodemographics were observed.
Perceived access to telehealth
Adults with chronic conditions were significantly more likely to report having access to telehealth, compared to those without chronic conditions (60.1% vs. 38.7%, P < 0.0001; Figure 1). Almost half of all adults without chronic conditions were unsure about their telehealth access (44.3%). This trend was also consistent across race ethnicity.
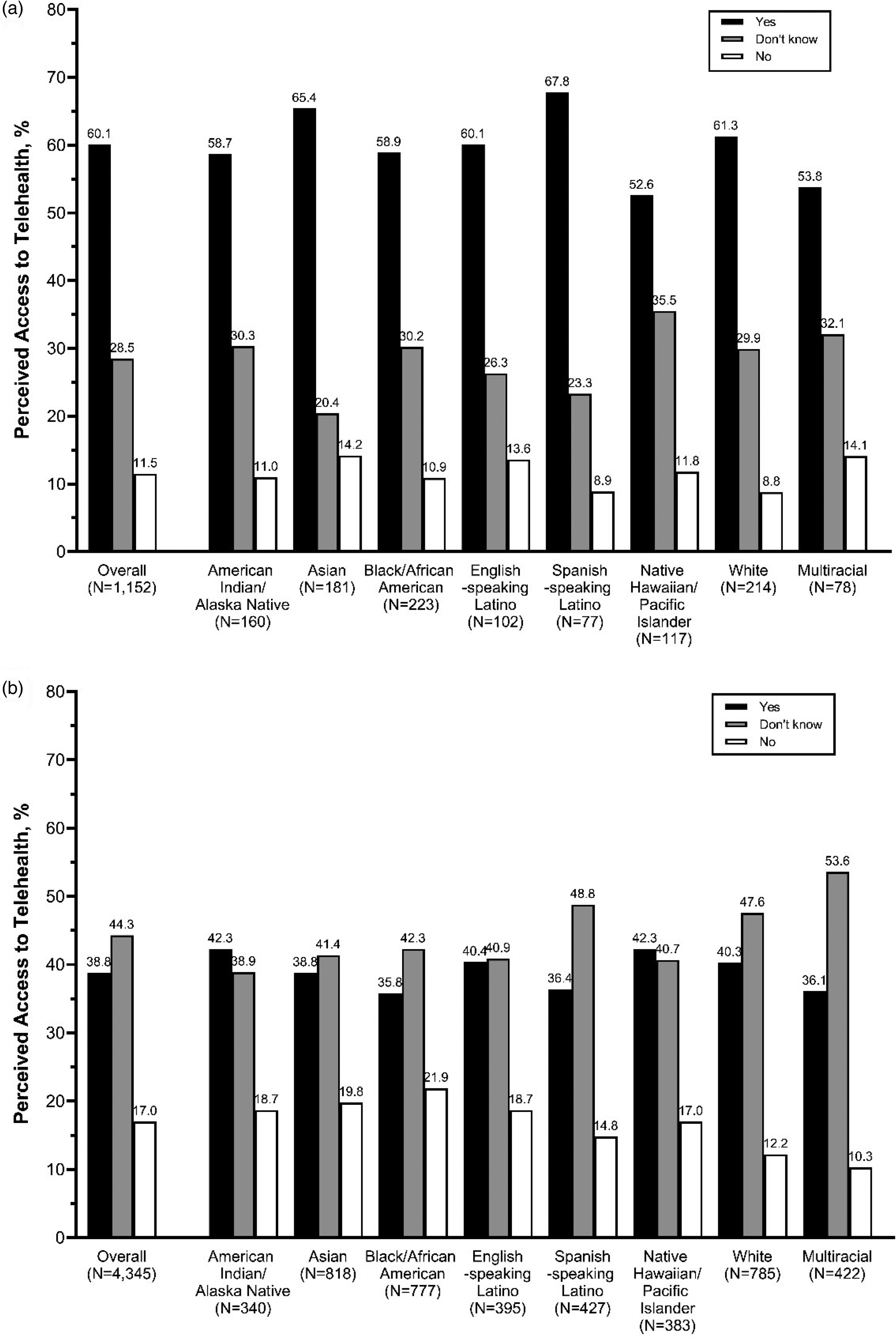
Prevalence of perceived access to telehealth among adults (a) with chronic conditions and (b) without chronic conditions, overall and stratified by race ethnicity, weighted to be nationally representative within racial-ethnic groups.
After adjusting for sociodemographics, adults with chronic conditions were still more likely to report having access to telehealth services, compared to adults without any chronic conditions (adjusted prevalence ratio [aPR] = 1.35, 95% confidence interval [CI] = 1.21–1.50, Supplemental Table 2). When stratified by chronic condition status, no racial-ethnic differences in perceived telehealth access were observed among adults with chronic conditions; however, among adults without chronic conditions, Spanish-speaking Latino adults (aPR = 1.40, 95% CI = 1.11–1.75) were more likely to report access to telehealth services, compared to White adults (Table 1).
Adjusted associations between sociodemographics and the prevalence of perceived access and willingness to use telehealth among adults with and without chronic condition status, weighted to be nationally representative within each racial-ethnic group.
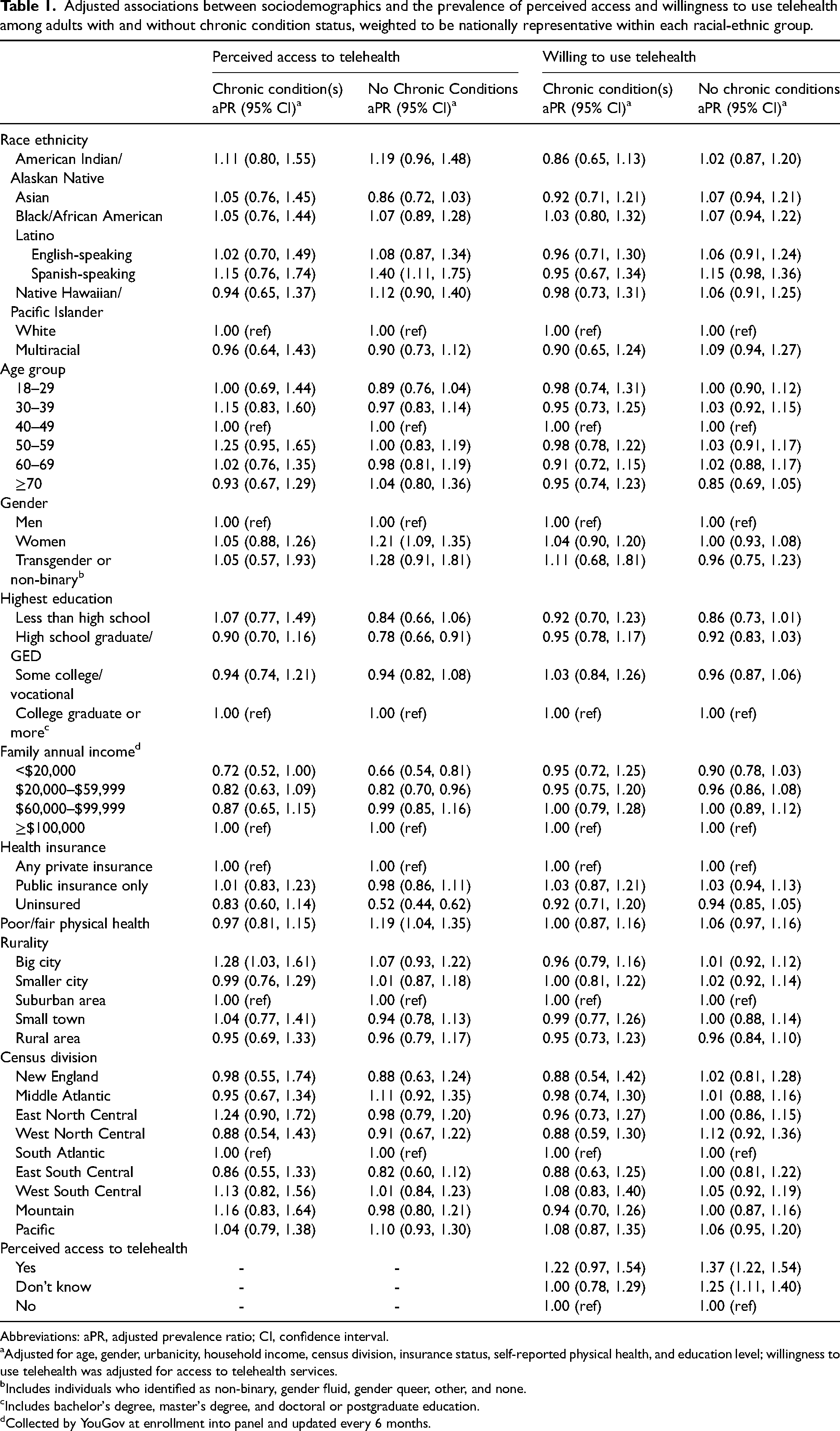
Abbreviations: aPR, adjusted prevalence ratio; CI, confidence interval.
Adjusted for age, gender, urbanicity, household income, census division, insurance status, self-reported physical health, and education level; willingness to use telehealth was adjusted for access to telehealth services.
Includes individuals who identified as non-binary, gender fluid, gender queer, other, and none.
Includes bachelor's degree, master's degree, and doctoral or postgraduate education.
Collected by YouGov at enrollment into panel and updated every 6 months.
When examining specific chronic conditions, only adults with chronic kidney disease (aPR = 1.34, 95% CI = 1.03–1.76), compared to those without chronic kidney disease, were more likely to report having access to telehealth (Table 2). Having more than one chronic condition, compared to only one, was also associated with having increased perceived access to telehealth (aPR = 1.32, 95% CI = 1.08–1.61).
Adjusted associations between specific chronic conditions and having multiple chronic conditions, perceived access to telehealth, and willingness to use telehealth services.
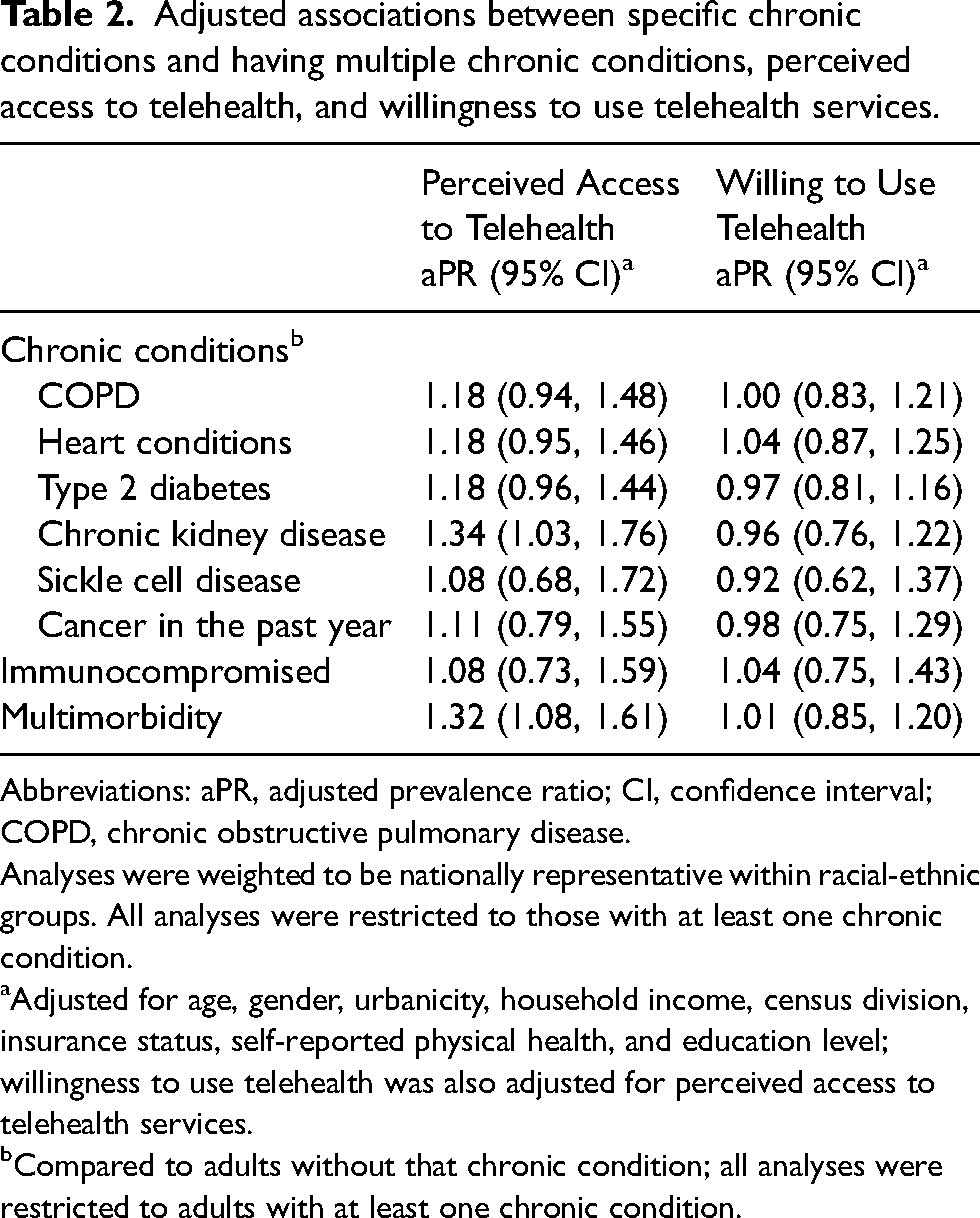
Abbreviations: aPR, adjusted prevalence ratio; CI, confidence interval; COPD, chronic obstructive pulmonary disease.
Analyses were weighted to be nationally representative within racial-ethnic groups. All analyses were restricted to those with at least one chronic condition.
Adjusted for age, gender, urbanicity, household income, census division, insurance status, self-reported physical health, and education level; willingness to use telehealth was also adjusted for perceived access to telehealth services.
Compared to adults without that chronic condition; all analyses were restricted to adults with at least one chronic condition.
Willingness to use telehealth
Smaller differences were observed for telehealth willingness, with most adults with and without chronic conditions being willing to use telehealth services (85.1% and 79.8%, respectively, Figure 2). Similar trends were observed across race ethnicity. After adjustment, no significant differences in telehealth willingness were observed between those with and without chronic conditions (aPR = 1.03, 95% CI = 0.95–1.13, Supplemental Table 2). Additionally, no differences in willingness to use telehealth were observed across type of chronic condition or multimorbidity status (Table 2).
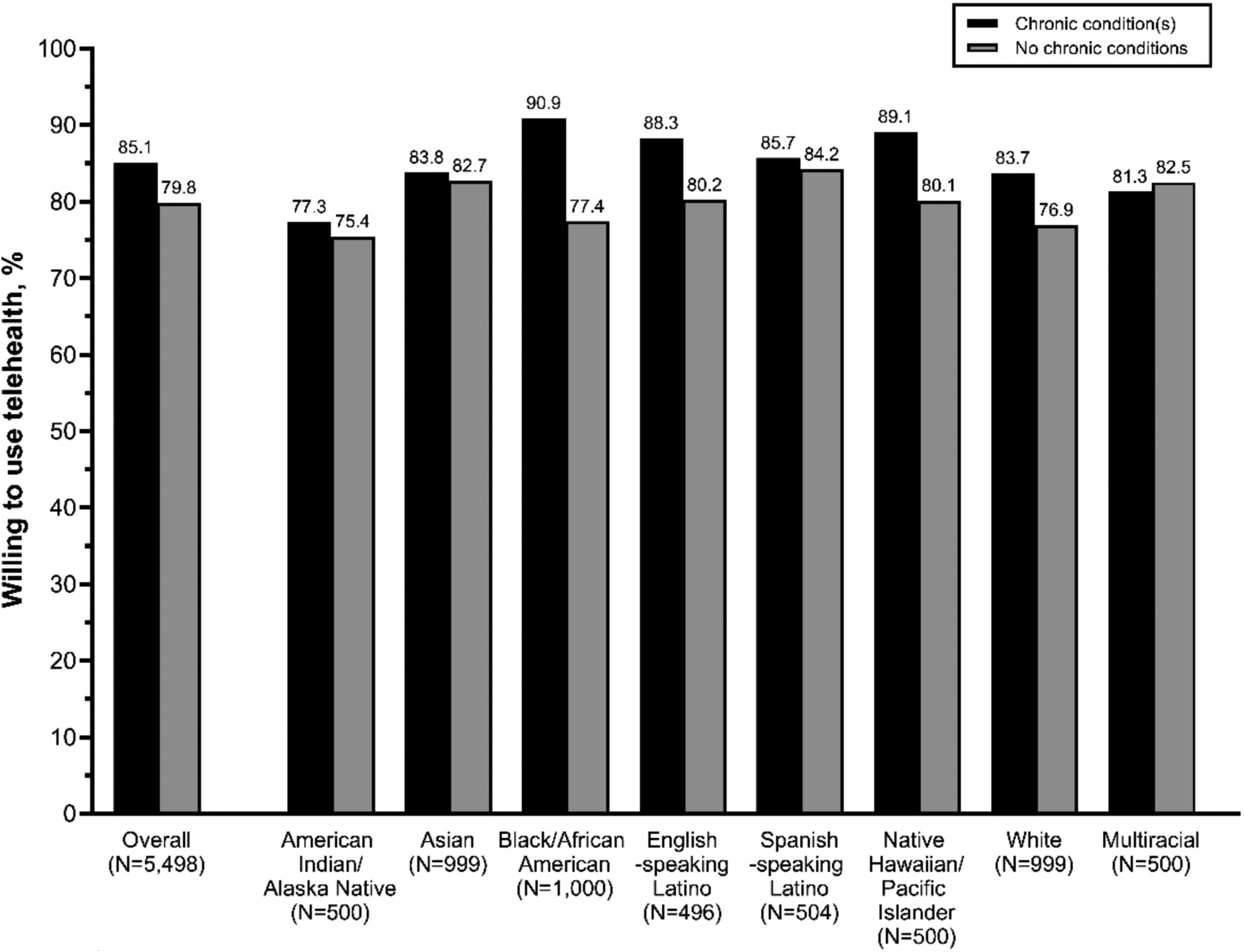
Prevalence of willingness to use telehealth among adults with chronic conditions and without chronic conditions, stratified by race ethnicity, weighted to be nationally representative within racial-ethnic groups.
Among both adults with and without chronic conditions, adults who reported having access to telehealth, compared to no access, appeared more willing to use telehealth (with chronic conditions: aPR = 1.22, 95% CI = 0.97–1.54; without chronic conditions: aPR = 1.37, 95% CI = 1.22–1.54), although estimates were imprecise (Table 1). Among adults without chronic conditions, those who were unsure about their access, compared to those having no access, were also more willing to use telehealth (aPR = 1.25, 95% CI = 1.11–1.40).
Perceived barriers to telehealth
The prevalence to each perceived telehealth barrier was relatively low among both adults with and without chronic conditions (Figure 3). Among adults with chronic conditions, the three most common were: (1) problems with using the telehealth application (15.6%); (2) feeling uncomfortable with technology (13.6%); and (3) problems with audio/video quality (12.8%). Overall, 51.4% of adults with chronic conditions and 61.4% of adults without chronic conditions reported no barriers to telehealth use.
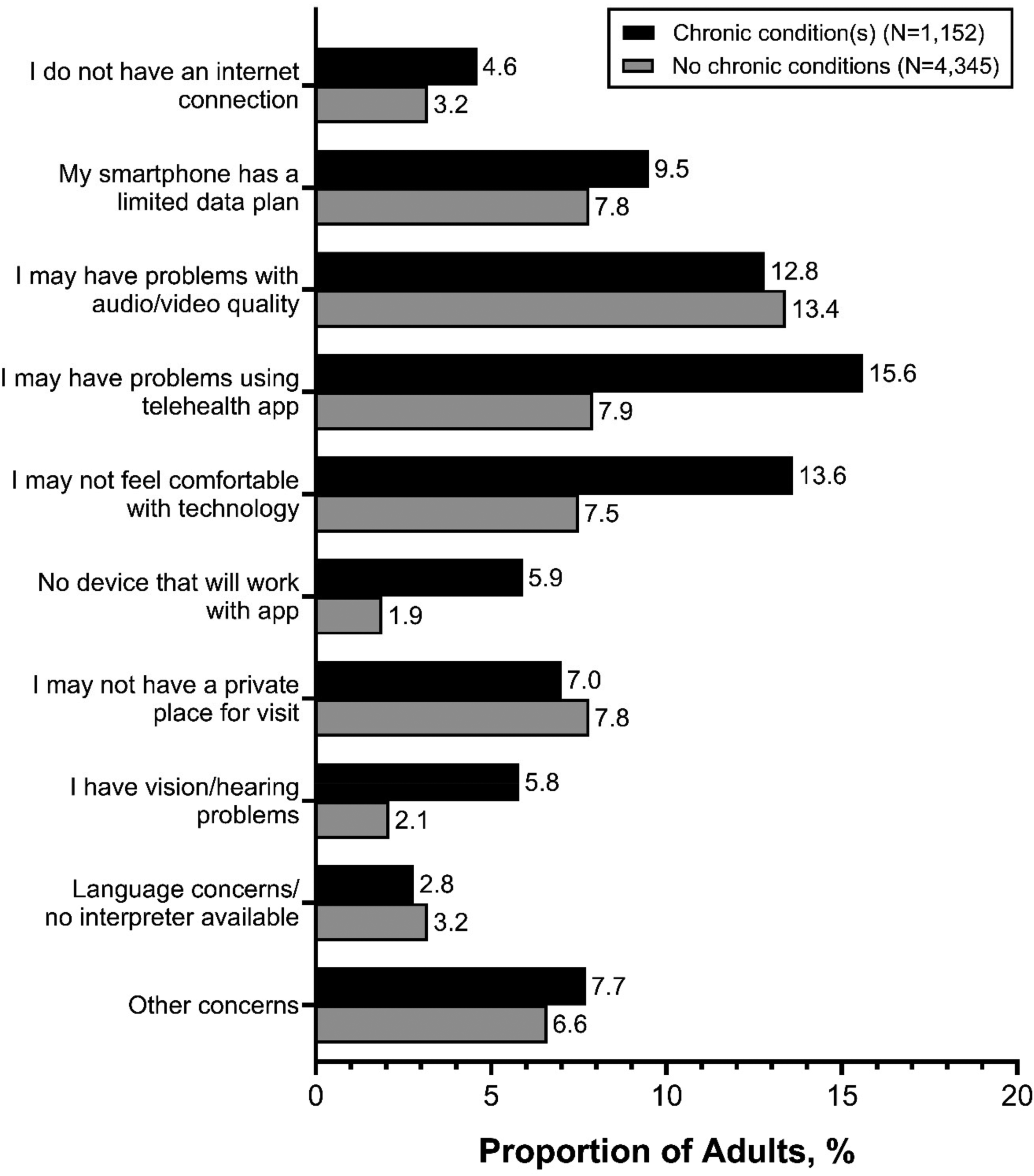
Prevalence of perceived telehealth barriers, stratified by chronic condition status. Results were weighted to be nationally representative within racial-ethnic groups. Overall, 51.4% of adults with chronic conditions and 61.4% of adults without chronic conditions reported no perceived barriers (data not shown).
Similar trends in perceived barriers to telehealth were observed across racial-ethnic groups, with a few notable exceptions (Supplemental Tables 3 and 4). First, Spanish-speaking Latino adults (with and without chronic conditions) were more likely to report having language concerns and/or having no available interpreter (chronic conditions: 10.4% vs. 0%–4.0%; no chronic conditions: 18.3% vs. 0.7–2.8%) compared to other racial-ethnic groups, P < 0.0001 for both. While the overall prevalence of perceived barriers was relatively low, only 33.1% of Spanish-speaking Latino adults and 37.3% of American Indian/Alaska Native adults with chronic conditions reported having no concerns (other racial-ethnic groups: 45.7%–60.2%, P = 0.0009 and P = 0.0001, respectively, Supplemental Table 3). Among those without chronic conditions, multiracial adults were more likely to report problems with audio/video quality (21.1% vs. 10.2–15.9% P < 0.0001) and not having a private place for the telehealth visit (14.2% vs. 3.5–10.2%, P < 0.0001, Supplemental Table 4).
Discussion
Using data from a nationally representative, diverse sample of adults living in the USA, we found that adults with chronic conditions were more likely to report having access to telehealth services compared to adults without chronic conditions; however, minimal differences were seen in the willingness to use telehealth services between these two groups. Perceived access to telehealth services was also one of the strongest predictors of willingness to use telehealth. No racial-ethnic disparities in perceived access or willingness to use telehealth were observed, although perceived access was associated with higher household income, private insurance, and higher levels of education. While perceived barriers to telehealth were relatively low among most racial-ethnic groups, only two in three American Indian/Alaska Native and Spanish-speaking Latino adults reported at least one barrier to using telehealth. Taken together, these results suggest that efforts should be directed toward increasing access and raising awareness of telehealth access to addressing racial-ethnic disparities in telehealth utilization.
Compared to other studies that have found racial-ethnic minorities and other marginalized communities to be less likely to utilize telehealth services during the pandemic,29–31 our study did not find disparities in reported telehealth access. Historically, racial-ethnic minorities and other marginalized communities have experienced disparities in healthcare access and utilization, including telemedicine and telehealth services.32,33 For instance, when primary care transitioned to entirely remote during the first year of the COVID-19 pandemic, there was evidence that non-Hispanic White patients, English-speaking patients, and patients with private insurance were overrepresented in telehealth patient visits for chronic disease management.12,34 Other studies have also found that racial-ethnic minorities and other marginalized communities were less likely to utilize telehealth services during the pandemic.29–31 Moving forward, evaluating telehealth utilization and addressing disparities remains important for the continuity of care for patients with chronic conditions. 35
Although willingness to use telehealth seemed to increase from the pandemic,36,37 privacy concerns, out-of-pocket costs, and the degree of trust in the healthcare system have still been reported as barriers to access and use.38,39 While we found that roughly half of adults reported no barriers to telehealth, adopting strategies to improve telehealth platforms are still needed. For instance, educational campaigns that address digital literacy and incorporate technological solutions (e.g. ensuring health professionals receive appropriate training to deliver telehealth services and providing tablets that will facilitate the use of telehealth)1,3,40,41 that improve access may be fundamental to ensuring equitably patient-centered telehealth care for populations vulnerable to communication barriers.
Disparities in perceived telehealth barriers, even after the expansion of telehealth services during the pandemic, have also been described.42–44 In our study, we found that Spanish-speaking Latino and American Indian/Alaska Native adults were more likely to report perceived barriers to telehealth services, especially those with chronic conditions. Studies among Latino adults have consistently found that they face unique challenges to accessing technology-enabled resources due to language barriers and gaps in digital literacy.32,45,46 At least one study prior to the pandemic also found that Latino adults experience more barriers to accessing or using technologies for health purposes. 47 Interestingly, we found that Spanish-speaking Latinos were more likely to report having access to telehealth, which may be linked to a high satisfaction of telehealth service as well as cultural perceptions of healthcare and physicians within the Latino community. 48 It is also possible the telehealth systems being used have built-in language interpretation which can better assist those with limited English proficiency, 49 allowing Spanish-speaking Latino adults to overcome potential language barriers with visual cues and reduced concerns with audio quality, consistent with literature showing better communication outcomes with video interpreters over phone interpreters.49,50 This may also explain why relatively few Spanish-speaking Latino adults reported language concerns as a barrier to telehealth (10.4% and 18.3% among those with and without chronic conditions).
There is a lack of research in telehealth access, willingness, and barriers within American Indian/Alaska Native populations, with most prior studies finding that they have lower access to broadband internet services.51,52 Similarly, we found that American Indian/Alaska Native adults were more likely to report having barriers to telehealth. They also appeared to be less willing to use telehealth compared to other racial-ethnic groups. This differs from a study that found 93% of American Indian adults reported being willing to use telehealth 51 and a report that found telehealth use among American Indian/Alaskan beneficiaries to be higher than White and Black adults. 53 Given the limited literature on telehealth and potential barriers among the American Indian/Alaska Native population, more research is needed to assess the health challenges that may exist within this community and if telehealth could potentially reduce adverse health outcomes.
This study is not without limitations. First, the CURB survey was conducted online and individuals with low broadband access, no access to technology, and/or have lower digital literacy would be less inclined to participate. This potential selection bias may mean that we are underestimating the prevalence of telehealth barriers. Second, because the survey was administered in English and Spanish (Latino participants only), non-English-speaking adults and non-Spanish-speaking Latinos were more likely to be excluded. This may have also created a language barrier, particularly for non-English-speaking individuals in other racial-ethnic categories, limiting the generalizability of these results. This may have particularly impacted our Asian adult cohort, as 12.3% reported limited English proficiency, compared to the national estimates of 31.9% of Asian adults having a limited English proficiency. 54 Access to telehealth was self-reported, and we did not have information to whether their usual healthcare location offered telehealth services, and if so, what services were available. Lastly, this study was conducted in late 2020, and changes in telehealth access, willingness, and barriers may have occurred since the survey was conducted. Despite these limitations, this study is one of the first to conduct a nationally representative and comprehensive assessment of perceived access, willingness, and barriers to telehealth after its expansion during the COVID-19 pandemic among a diverse population of adults with and without chronic conditions.
In conclusion, this study suggests that willingness to use telehealth services is dependent on its accessibility. Given that willingness to use telehealth services is strong across all sociodemographic groups, targeting barriers, increasing awareness, and increasing access to telehealth are critical to promote telehealth use and reduce racial-ethnic disparities. Given that telehealth continues to be an important tool to provide timely and accessible healthcare services to adults in the USA, investing into strategies to improve telehealth services will maintain high-quality care and could mitigate health disparities that arise due to the COVID-19 pandemic, especially among adults with chronic health conditions.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X231199522 - Supplemental material for Telehealth access, willingness, and barriers during the COVID-19 pandemic among a nationally representative diverse sample of U.S. adults with and without chronic health conditions
Supplemental material, sj-docx-1-jtt-10.1177_1357633X231199522 for Telehealth access, willingness, and barriers during the COVID-19 pandemic among a nationally representative diverse sample of U.S. adults with and without chronic health conditions by Randy Le , Izabelle Mendez, Stephanie A Ponce, Alexis Green, Sherine El-Toukhy, Anna M Nápoles and Paula D Strassle in Journal of Telemedicine and Telecare
Footnotes
Acknowledgements
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Division of Intramural Research, National Institute on Minority Health and Health Disparities, National Institutes of Health.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.