
Abstract
Aim
The purpose of this study is to explore the effectiveness of a hospital-based asynchronous ear, nose, and throat (ENT) telehealth service (the Ear Portal) in reducing cost and improving access for children with otitis media.
Methods
Participants were recruited to the Ear Portal from a tertiary hospital ENT waiting list. Ear and hearing assessments were conducted during appointments by the Ear Portal research assistant, and data was stored for an asynchronous review by the Ear Portal multidisciplinary team. A cost-minimisation analysis was conducted for the Ear Portal and the standard care pathways. Waiting times to provide care for both pathways were calculated for children with semi-urgent (i.e. Category 2) and non-urgent (i.e. Category 3) referrals.
Results
The running cost for the Ear Portal was $67.70 for initial appointments and $37.34 for follow-up appointments. Conversely, the running cost for the standard care pathway was $154.65 for initial appointments and $86.10 for follow-up appointments. A total of 223 appointments were required to offset the initial Ear Portal investment of $19,384.00. The median waiting time for the Ear Portal from initial contact to care plan delivery was <30 days, whereas the median waiting times for children in the standard care pathway were 291 days (interquartile range (IQR) = 117) for Category 2 and 371 days (IQR = 311) for Category 3 referrals.
Conclusion
Under the current circumstances, the Ear Portal service can reduce costs for the health care system by reducing marginal costs per patient in addition to providing ENT specialist care within the clinically recommended timeframes.
Keywords
Introduction
Otitis media (OM) is a middle ear inflammation and is a common condition in early childhood, leading to frequent primary care visits and antibiotic prescriptions.1,2 Acute OM symptoms typically include fever and pain lasting for a few days and can be followed by middle ear effusion that may last up to three months.3,4 Symptoms can become recurrent or persistent for a subset of children, and the presence of effusion in the middle ear cavity can lead to varying degrees of conductive hearing loss. 5 It has been suggested that persistent conductive hearing loss in early childhood may increase the risk of various developmental problems, including language,6–8 behaviour,9–11 and auditory processing.12,13 Therefore, timely access to specialist care is recommended for children with recurrent and persistent OM to avoid risks of medical and developmental complications.9,12,14
In Australia, geographical barriers often pose a challenge to accessing specialist outpatient care for individuals living in remote and rural regions. Individuals residing in urban areas may also experience delayed access to specialist outpatient clinics and elective surgery due to a multitude of reasons, including unnecessary referrals and the increasing demand on Australia's public hospital outpatient clinics, which is further worsened by the recent outbreak of COVID-19.15–18 Patients in urban regions often exceed the clinically recommended timeframes to receive their initial outpatient consultation, which may lead to deterioration in patient health and quality of life and add a significant economic burden to patients and the healthcare system.16,19
Several initiatives have been undertaken to improve access to ear, nose, and throat (ENT) outpatient speciality care. These include auditing referrals 18 and utilising advanced-scope allied health professionals as the first point of contact, thereby reducing the waiting times for ENT outpatient care.20,21 Furthermore, the provision of healthcare via telehealth has also been widely explored. Studies examining the feasibility of these services in rural and remote areas demonstrated encouraging results for audiological screening purposes,22,23 improved access to care, 24 and reduced waiting times for ENT specialist care. 25
When evaluating costs associated with telehealth services, a review by Snoswell et al. 26 demonstrated a potential for cost reduction in multiple medical disciplines, especially when patient and clinician travel was funded by the healthcare system. Reduced costs for patients and healthcare providers, particularly due to reduced travel expenses, were also reported in various otolaryngology disciplines. 27 Yet, little research has been conducted on the cost implications of an ENT telehealth service for individuals living in urban regions. Therefore, the purpose of this study is to evaluate the feasibility of an urban ENT telehealth service in a paediatric tertiary hospital to reduce costs for the healthcare system and wait times for outpatient specialist care. This may yield valuable information for stakeholders and policymakers to make more informed decisions and offer future research ways to improve access to specialised care for children with OM.
Methods
The Ear Portal pathway
The Ear Portal is a hospital-based asynchronous telehealth service that was designed to provide fast-tracked access to ENT specialist care for children. Children were eligible for the service if they (i) were between the ages of six months and 18 years, (ii) resided within the greater metropolitan area of Perth, Western Australia (<60 km), (iii) were referred to the ENT outpatient clinic in a tertiary hospital (Perth Children's Hospital (PCH)) due to having recurrent and persistent OM or concerns related to OM, such as hearing and/or speech-language development, (iv) did not have an appointment scheduled at the hospital at the time of recruitment, (v) and were triaged by ENT specialists at the hospital as Category 2 (i.e. semi-urgent referrals) and Category 3 (i.e. not-urgent referrals). Children requiring regular face-to-face follow-ups in the hospital (e.g. children with craniofacial abnormalities) and children triaged as Category 1 (i.e. requiring urgent care) were not eligible to participate in the Ear Portal service.
Children who were eligible to access the service were identified from the referral list at PCH. Research assistants (RAs) contacted the caregivers of eligible children to ascertain their interest in participation. Those who expressed interest in participation were emailed a detailed information sheet regarding the Ear Portal study, and initial (i.e. screening) appointments were booked based on caregivers’ preferences. The initial assessments were conducted by an RA or audiologist at the PCH research clinic after consent forms were signed by caregivers. During the assessments, a comprehensive case history was obtained from caregivers, including detailed information regarding the child's medical background in addition to familial medical and demographic information. Ear and hearing assessments, including video otoscopy, tympanometry, otoacoustic emissions, and screening audiometry (i.e. ≥25 dB HL), were also conducted. Parent-reported screening questionnaires were administered to all children.
All data was recorded and stored for an asynchronous review by the Ear Portal multidisciplinary team (MDT), which met fortnightly to review the findings, make a diagnosis, and provide individualised care plans for each child. The MDT consisted of an ENT registrar, an ENT clinical nurse specialist (CNS), and an audiologist. Care plans were then delivered to caregivers by the Ear Portal RA via phone calls. A simplified description of the Ear Portal and the standard care pathways is illustrated in Figure 1.
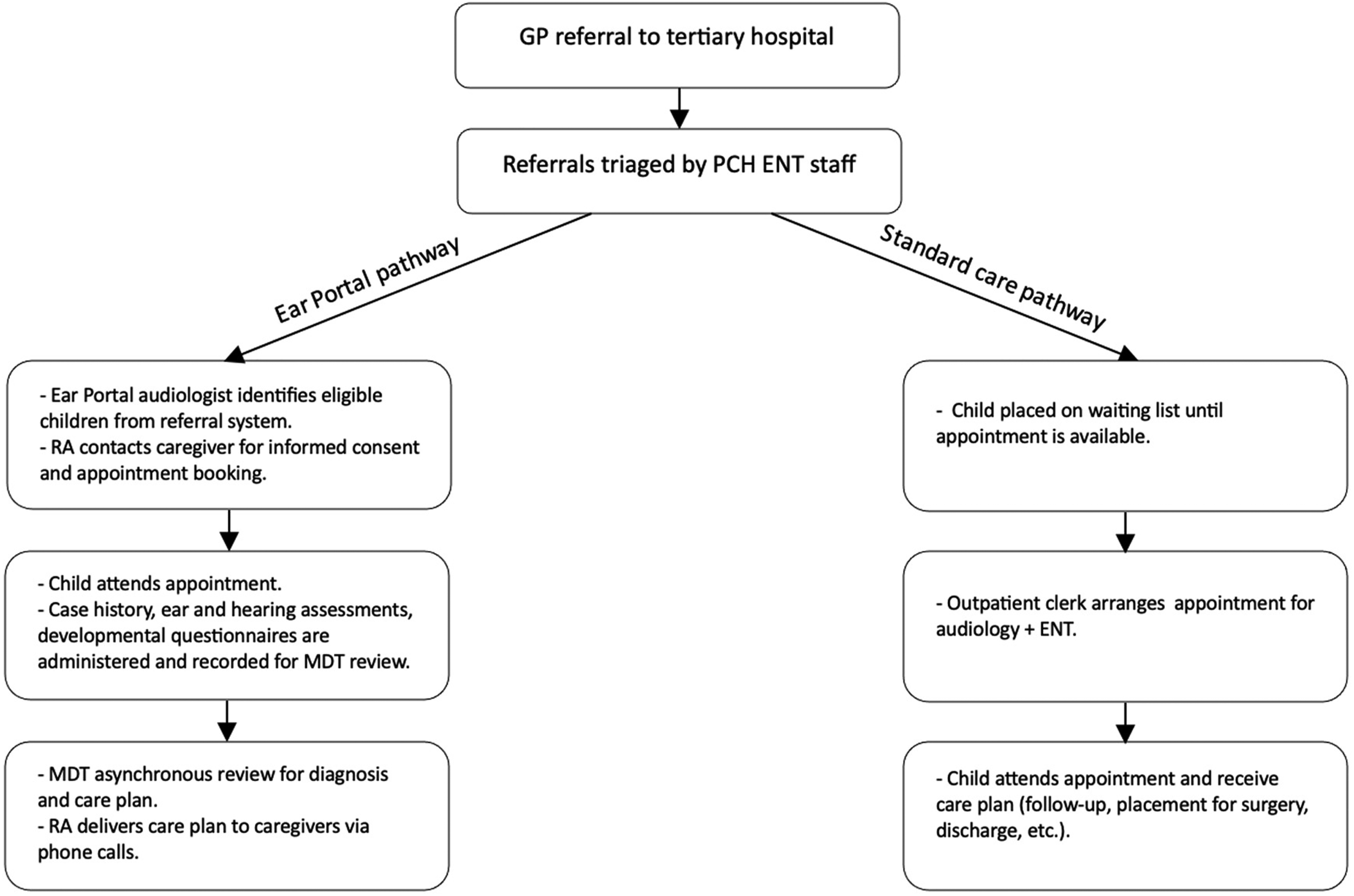
Flowchart illustrating the Ear Portal and the standard care pathways.
Ethical considerations
Ethical approvals for the Ear Portal project were obtained from the Child and Adolescent Ethical Committee, The Western Australian Aboriginal Health Ethics Committee, and The University of Western Australia. The study was prospectively registered on the Australian New Zealand Clinical Trials Registry (ACTRN1269000039189p).
Cost-minimisation analysis
The reporting of economic information in the current study was based on the Consolidated Health Economic Evaluation Reporting Standards. 28 Cost-minimisation analysis was calculated for both care delivery models by categorising the costs into fixed and variable costs. Variable costs reflect the total costs involved in each appointment type (i.e. initial or follow-up). Fixed costs were exclusive to the Ear Portal service and involved the cost of the initial investment to set up the service. The cost of infrastructure was not included as the Ear Portal utilised existing hospital infrastructure. Similarly, the cost to the family was not evaluated, as families were required to be present at the hospital for both care delivery pathways. The study adopted a hospital perspective, particularly in the evaluation of costs.
The variable costs for the Ear Portal service included in the analysis involved the cost per appointment, which includes the salaries of staff from the identification of an eligible participant through care plan delivery. This included a research audiologist, an RA, and the Ear Portal MDT (i.e. ENT and CNS), which were based on the average time required for each member involved. Similarly, the variable costs of the standard care pathway included the salaries of staff members required for each appointment, which were based on the allocated time for each staff member from appointment scheduling to care plan delivery. A single-factor sensitivity analysis was conducted by varying factors that exhibited uncertainty or variability. The time per session was influential in shaping the costs of both care pathways when altered within a reasonable range (±25%).
The outcomes of both care delivery pathways are presumed to be similar, whether the appointments were conducted face-to-face or via telehealth. All costs were reported for the Australian 2022-2023 financial year at a conversion rate of AUD$1 = US$0.67 at the time of the analysis.
Analysis of waiting times
All children enrolled in the Ear Portal experienced a period of waiting time on the hospital's waiting list prior to being identified for enrolment. Therefore, this prior waiting period was calculated as the waiting time for the standard care pathway. We referred to this period as the ‘minimum waiting time’ as it reflects the known period experienced by children before telehealth intervention rather than the ‘true’ waiting period that would have occurred if caregivers were not offered access to the Ear Portal service (Figure 2).
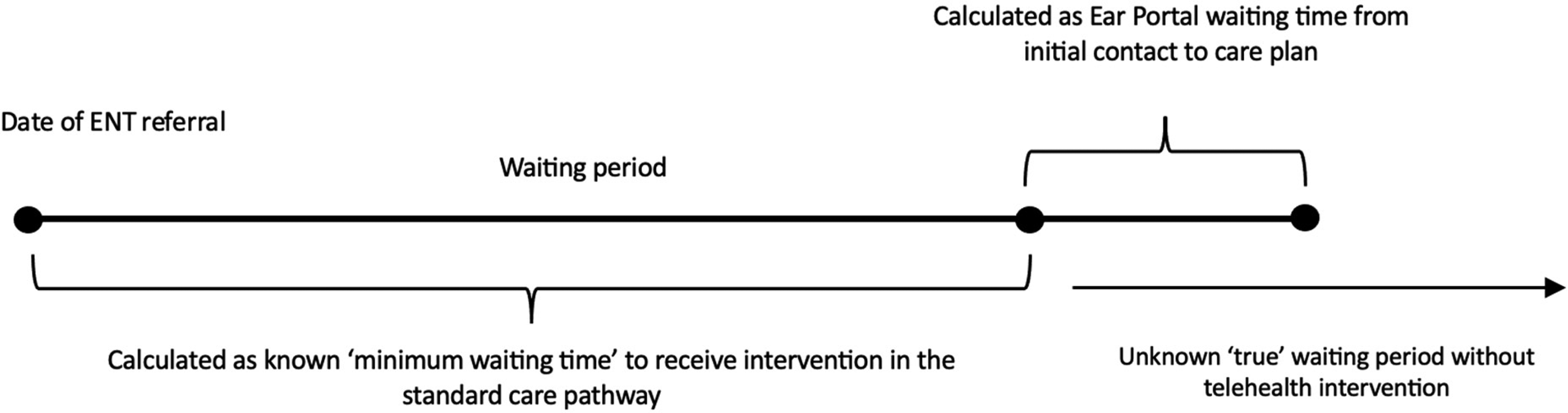
Estimated timeline displaying the process of care delivery from the date of ear, nose, and throat (ENT) referral. The estimated timeline in the standard care was only calculated until telehealth intervention. The ‘true’ waiting time in the standard care is unknown.
In contrast, the waiting times to access the Ear Portal service were calculated from the date caregivers were initially contacted by the Ear Portal team via phone calls to the date of care plan delivery (Figure 2). Exploratory statistics were used to identify significant outliers – children who received significantly delayed assessments in the Ear Portal service. Outliers were removed from the analysis only if they were determined to be caregiver-related delays (n = 7).
Binary variables of waiting times were created to identify the proportion of children who received access to an ENT specialist after the clinically recommended timeframes allocated to Categories 2 (i.e. within 90 days) and 3 (i.e. within 365 days).
Results
Costs of care delivery pathways
A total of 291 appointments were conducted since the commencement of the Ear Portal service in June 2020 until July 2023. These appointments included initial and follow-up appointments. The equipment required to conduct assessments in the Ear Portal service is described in Table 1. The total fixed costs amounted to $19,384.00 that were invested in the service in 2020 (average conversion rate in 2020: AUD$1 = US$0.69). The total running cost per session was $67.70 for initial appointments and $37.34 for follow-up appointments (Table 2). In contrast, the total running cost per session at the standard care pathway was $154.65 for initial appointments and $86.10 for follow-up appointments (Table 2). The total variable cost of the Ear Portal appointments since inception (i.e. during a three-year period) was $18,736.06. Assuming all 291 appointments were conducted at the standard care pathway, the total variable cost is estimated to be $39,107.85. The Ear Portal service was cost-efficient for both appointment types compared with the standard care pathway. The Ear Portal service also resulted in increased productivity for ENT specialists by increasing the average volume of patients reviewed by the MDT to approximately 11 patients, compared with three patients in the standard care pathway (Table 3).
One-time fixed cost to set up the Ear Portal service in 2020.
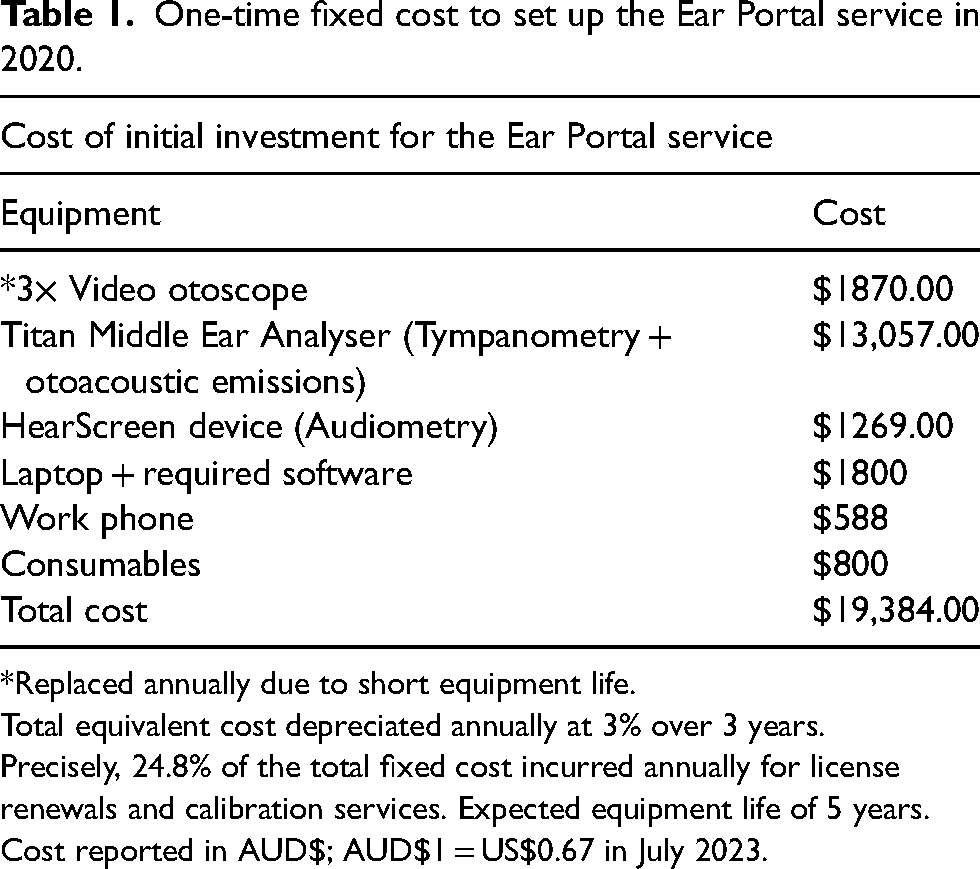
Replaced annually due to short equipment life.
Total equivalent cost depreciated annually at 3% over 3 years.
Precisely, 24.8% of the total fixed cost incurred annually for license renewals and calibration services. Expected equipment life of 5 years.
Cost reported in AUD$; AUD$1 = US$0.67 in July 2023.
Estimates of cost per patient for both care delivery pathways based on the unit cost of salaries and time for each staff member and activity.
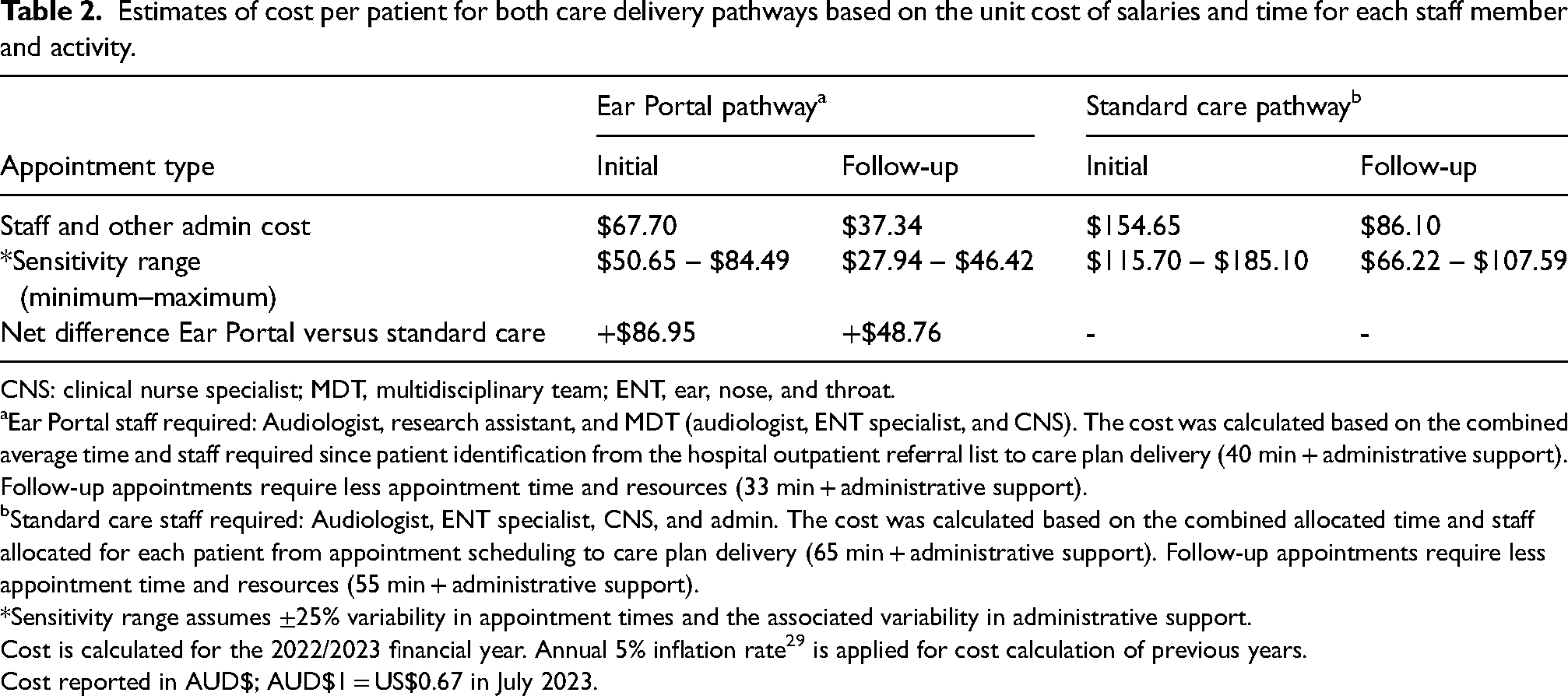
CNS: clinical nurse specialist; MDT, multidisciplinary team; ENT, ear, nose, and throat.
Ear Portal staff required: Audiologist, research assistant, and MDT (audiologist, ENT specialist, and CNS). The cost was calculated based on the combined average time and staff required since patient identification from the hospital outpatient referral list to care plan delivery (40 min + administrative support). Follow-up appointments require less appointment time and resources (33 min + administrative support).
Standard care staff required: Audiologist, ENT specialist, CNS, and admin. The cost was calculated based on the combined allocated time and staff allocated for each patient from appointment scheduling to care plan delivery (65 min + administrative support). Follow-up appointments require less appointment time and resources (55 min + administrative support).
Sensitivity range assumes ±25% variability in appointment times and the associated variability in administrative support.
Cost is calculated for the 2022/2023 financial year. Annual 5% inflation rate 29 is applied for cost calculation of previous years.
Cost reported in AUD$; AUD$1 = US$0.67 in July 2023.
Cost and patient volume comparisons between the Ear Portal and the standard care pathways.
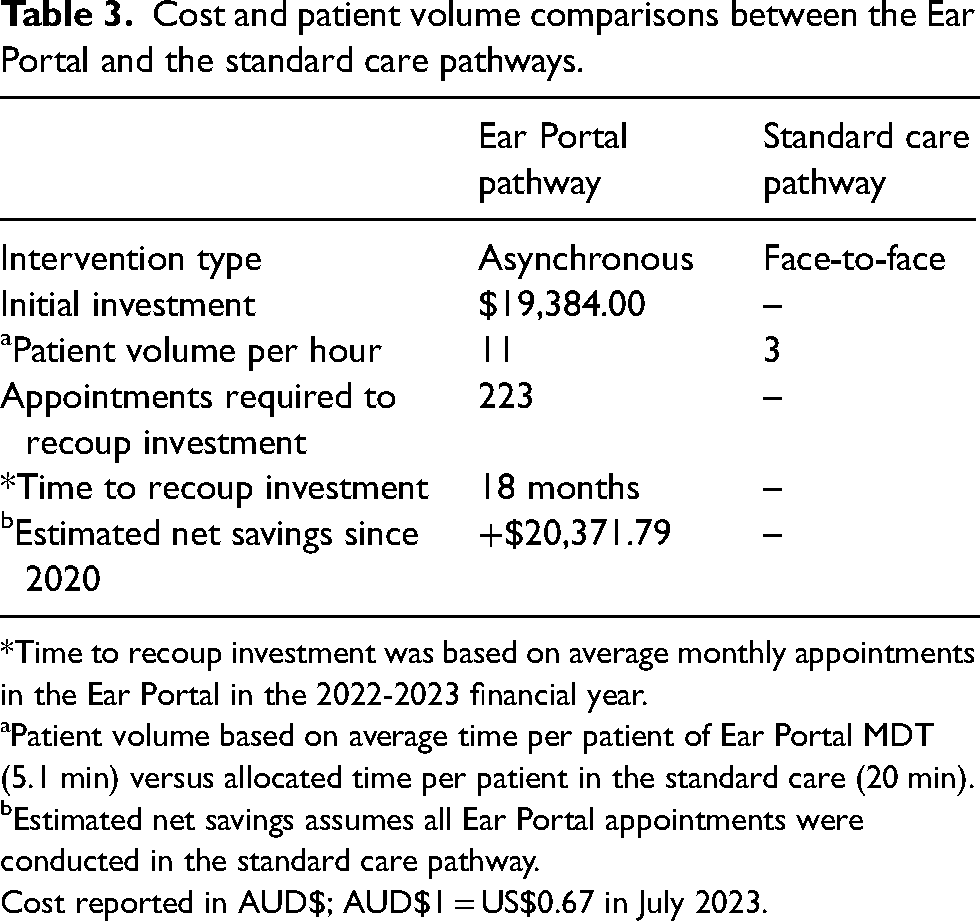
Time to recoup investment was based on average monthly appointments in the Ear Portal in the 2022-2023 financial year.
Patient volume based on average time per patient of Ear Portal MDT (5.1 min) versus allocated time per patient in the standard care (20 min).
Estimated net savings assumes all Ear Portal appointments were conducted in the standard care pathway.
Cost reported in AUD$; AUD$1 = US$0.67 in July 2023.
Waiting times
The median waiting times for Categories 2 and 3 referrals to access the ENT specialist care and the proportion of children receiving care outside the clinically recommended timeframes for their triage category in both care delivery pathways are summarised in Table 4.
Description of the median waiting times (in days) for both care delivery pathways.
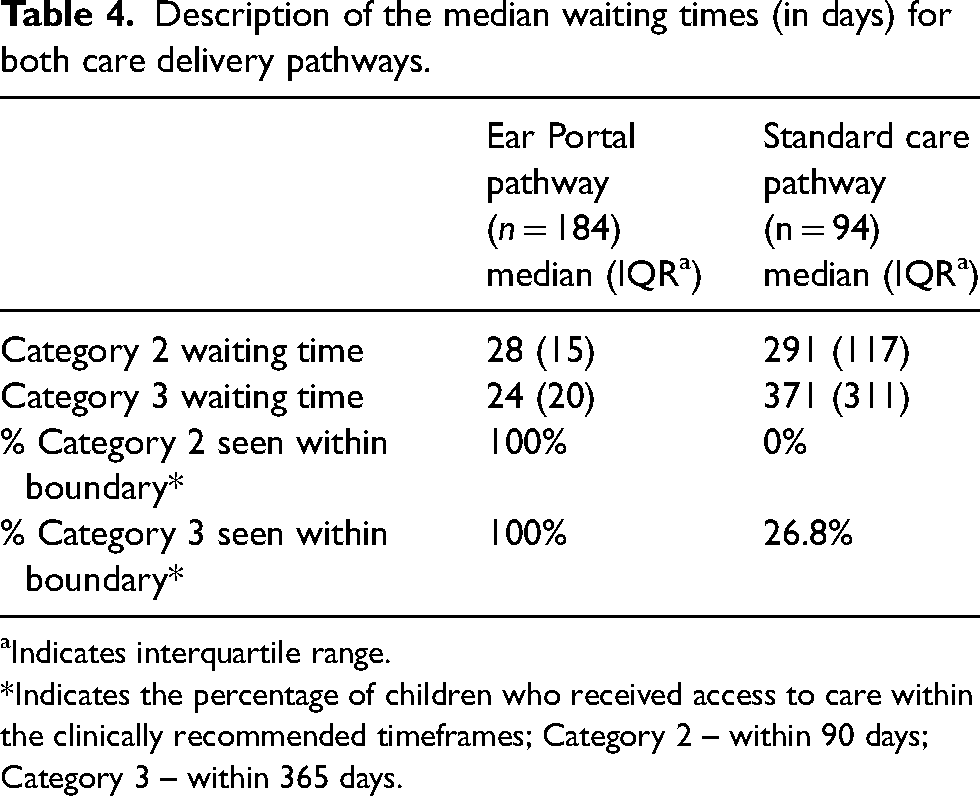
Indicates interquartile range.
Indicates the percentage of children who received access to care within the clinically recommended timeframes; Category 2 – within 90 days; Category 3 – within 365 days.
Discussion
The present study aimed to investigate the cost implications of running the Ear Portal, a telehealth service for children referred to ENT outpatient specialist care due to OM-related concerns, and explore the waiting times associated with this service to receive specialist care. A cost-minimisation and comparative analysis revealed that the provision of care via the Ear Portal was associated with reduced costs for the healthcare system and improved access to care when compared with the ENT outpatient standard care pathway.
The Ear Portal service was associated with lower overall costs compared with the standard care pathway. The total running cost per session for an initial appointment was $67.70, compared with $154.65 for the standard care pathway. Similarly, the cost to conduct follow-up appointments was 43.4% lower when using the Ear Portal service. However, due to the associated setup cost of the Ear Portal, cost savings can only be realised after 18 months or when a threshold of 223 appointments is reached. The short equipment life of the video otoscope slightly increased the annual overhead fixed costs. However, all other pieces of equipment are assumed to have a life expectancy of five years. The total number of appointments conducted in the Ear Portal since inception is 291 with an average of 1.4 appointments per patient. Had all of these appointments been conducted in the standard care pathway, the total cost savings would have been approximately $20,371.79. The Ear Portal resulted in cost savings in a number of ways. For example, the face-to-face initial appointment with the ENT specialist in the standard pathway is fixed at 20 min per consult, with an additional 45 min to conduct ear and hearing assessments with an audiologist. In contrast, the average total time allocated to each patient in the Ear Portal was 47.6 min. Therefore, the Ear Portal service could result in cost reduction by reducing the marginal cost per patient and the resources typically allocated to each patient in the standard care pathway. The sensitivity analysis demonstrated that the most influential determinant of cost was the reduction of initial appointment time by 25% in both care delivery pathways.
In a mobile screening and surveillance service, Nguyen et al. 30 reported the cost-effectiveness of their telehealth initiative primarily by preventing hearing loss and the associated educational and rehabilitation costs in a sample of Australian Indigenous children at risk of ear disease. Cost minimisation for the healthcare system in Australia was also reported in studies that utilised ENT telehealth services.31,32 Given that their studies focused on providing ENT telehealth services for patients living in rural areas, reduced costs were mainly achieved by eliminating patient travel expenses subsidised under the Patient Travel Subsidy Scheme. For example, Xu et al. 32 reported cost minimisation for the healthcare system by providing a videoconferencing telehealth service for individuals with ENT conditions, resulting in a cost savings of approximately AUD$47 per consultation. Similarly, post-operative ENT telehealth reviews for patients with OM resulted in a cost savings of approximately AUD$1354–2158 due to eliminated travel expenses. 31 While the Patient Travel Subsidy Scheme was not explored in this study as all patients resided in urban regions, it is still anticipated that cost minimisation for patients (e.g. travel costs, loss of work days, and parking fees) can be achieved given that receiving audiology and ENT appointments on the same day in the standard care pathway is not always feasible. Furthermore, by replacing face-to-face appointments with asynchronous telehealth appointments, there is a potential to increase ENT specialists’ productivity, as demonstrated in this study. This was achieved by providing ENT specialist care plans for approximately 11 patients per hour, whereas the standard care pathway could only accommodate three patients per hour. This can also avoid factors such as patient no-shows during face-to-face appointments, which can significantly impact the capacity of the ENT department. Therefore, increased productivity via telehealth services can reduce the burden on the healthcare system, allowing ENT specialists to reallocate saved time to patients with more severe conditions and those awaiting surgical interventions, ultimately enhancing the efficiency of the healthcare system.
In terms of waiting times for both pathways, the Ear Portal telehealth service showcased improvements in access to ENT specialist care by reducing the waiting times for children awaiting intervention for OM-related concerns compared with the standard care pathway. For children triaged as Categories 2 and 3, the median waiting time for the Ear Portal telehealth service to provide appointments and an ENT specialist care plan was <30 days. Conversely, the median waiting time in the standard care pathway for Categories 2 and 3 was 291 and 371 days, respectively. While comparison with other studies was not possible due to differences in methodological designs, the efficacy of telehealth services to improve access to ENT specialists and reduce waiting times is well established for individuals residing in rural areas. 25 Therefore, the current findings add to the existing body of literature, demonstrating the efficacy of telehealth services in reducing waiting times for children awaiting ENT outpatient specialist care in urban areas. Furthermore, this study highlighted the efficacy of the Ear Portal telehealth service for the provision of intervention within the clinically recommended timeframes for children with OM-related concerns, whereas only 26.8% of children in Category 3 were able to access the standard care pathway within the clinically recommended timeframes. A plausible explanation for the shorter waiting times in the Ear Portal pathway lies in patient volume. That is, although the reported waiting times in the standard care pathway were for children with medical conditions similar to those who accessed the Ear Portal, the ENT department at a tertiary hospital manages a broad range of ENT conditions. This can lead to longer waiting times due to the prioritisation of care for children with more severe medical issues. In contrast, the Ear Portal service was specifically designed for children with OM-related issues, with a higher motivation to provide prompt access for these children. Although children with OM may not fit the criteria for urgent care, there is a high variability in OM recurrence and persistence across children. This makes the impact on developmental outcomes relatively unknown, especially when children experience lengthy waiting times. Moreover, early treatment of OM not only reduces the risk of OM complications (e.g. tympanic membrane perforations, mastoiditis, and meningitis) but may also reduce the cost associated with OM complications.30,33 Implementing telehealth at a tertiary hospital can act as a ‘first point of contact’ to capture those at risk of medical and developmental outcomes.4,9,14,34 This can help in providing timely care for those requiring prompt access to care, potentially reducing the burden on patients, their families, and the public healthcare system.
Strengths and limitations
The ability of the Ear Portal to provide timely care for children referred to outpatient specialist care was possible because of the support and endorsement from the PCH ENT Department, which ensured that it fully incorporated the new Ear Portal service paradigm into department practices. This allowed the service to work collaboratively with hospital staff to provide regularly scheduled and timely intervention plans for children awaiting specialist intervention. It is difficult to replicate comparable real-world conditions between local health services. However, having the support of clinical and administrative leaders within health services is critical to the successful implementation of novel treatment pathways such as the Ear Portal. One limitation of this study was the lack of information regarding the average time required per appointment at the standard care pathway. This would have allowed for more comparable calculations of the costs associated with both services. Additionally, while cost-minimisation analysis provided important information regarding the cost reduction between two care delivery pathways, information regarding patient health outcomes and quality of life remains to be explored. The use of cost–utility analysis in future studies can be beneficial in providing important information on patients’ outcomes that reflect the efficacy of these services.
Conclusion
Under the presented circumstances, the Ear Portal telehealth service was shown to reduce marginal cost per patient and increase the productivity of ENT specialists compared with the standard care pathway. However, the service was only cost-efficient when a threshold of 223 appointments was reached to offset setup costs. Additionally, the service was able to reduce waiting times for children with OM compared with the standard care pathway. Providing assessments and care plans can be achieved in <30 days. Alternatively, waiting times at standard care can be up to 371 days, exceeding the clinically recommended timeframes.
Footnotes
Acknowledgements
We thank all the children and caregivers who took part in the study. We also thank Kathryn Jajko and all Ear Portal team members at the Telethon Kids Institute, and medical, nursing and administrative staff from the PCH ENT Department, Erin Maywood and Nicole Irvine from the PCH Audiology Department, and Robert Proctor from the PCH Telehealth Department for their significant contribution to the development and implementation of this project. We acknowledge that this research was undertaken on Noongar Whadjuk Boodja, the traditional land of the Whadjuk Noongar people, and acknowledge their Elders past, present and emerging.
Author's note
Robyn SM Choi is also affiliated at School of Allied Health, Curtin University, Perth, Western Australia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Telethon-Perth Children's Hospital Research Fund, the Medical Research Future Fund via the Western Australia Health Translation Network Rapid Applied Research Translation program. Chris Brennan-Jones was supported by a National Health and Medical Research Council Fellowship (GNT 1142897) and a Western Australian Department of Health Emerging Leader Fellowship.
Data availability
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.