
Abstract
Introduction
The goal of this systematic review was to examine the efficacy of behavioral health care treatments for post-traumatic stress disorder (PTSD), depression, and anxiety delivered via telehealth.
Methods
We searched a combination of keywords related to telehealth, relevant mental health disorders, and evidence-based psychotherapies in three databases (PubMed, PsycInfo, and Embase) from database inception to April 2022. We included randomized controlled trials published in English wherein at least one arm received an evidence-based psychotherapy via telehealth. To be included, studies also had to enroll an adult population with symptoms or diagnosis of PTSD, depressive disorder, or anxiety disorder.
Results
Moderate quality of evidence was consistent with only small differences, if any, in efficacy between video teleconferencing (VTC) and in-person delivery for patients with PTSD (d = 0.06, 95% CI −0.17, 0.28). However, for those with depression, in-person delivery was associated with better outcomes compared to VTC (d = 0.28, 95% CI 0.03, 0.54; low quality of evidence). We also found that evidence-based treatments delivered over telephone were more efficacious for depression compared to treatment as usual (d = -0.47, 95% CI −0.66, −0.28; very low quality of evidence). Very low quality of evidence supported the use of telehealth versus waitlist for anxiety (d = -0.48, 95% CI −0.89, −0.09).
Conclusions
A synthesis across 29 studies indicates that the efficacy of telehealth for delivery of evidence-based behavioral health interventions varies by target diagnosis and telehealth modality. More research is needed on the efficacy of telehealth treatments for depression and anxiety.
Introduction
Synchronous telehealth refers to the real-time provision of health care services via telephone or video teleconferencing (VTC) services. 1 Synchronous telehealth provides several advantages when compared to in-person care. Common barriers to behavioral health care include local provider availability, transportation, and scheduling conflicts. 2 Synchronous telehealth offers more flexibility in terms of scheduling, requires no transportation to a treatment location, and expands the geographical range of providers available to a patient. These advantages may be particularly useful for unique populations, such as military service members who experience frequent relocations and overseas deployments. Synchronous telehealth can improve the establishment and/or continuity of care and alleviate concerns about privacy and stigma in military service members.3,4
Historically, concerns about the security of technological platforms, ability to effectively manage patient risk, and licensure/jurisdictional boundaries limited the use of telehealth in behavioral health care, but much of that changed with the onset of the COVID-19 pandemic in early 2020. 5 In the United States, restrictions enacted to suppress the COVID-19 pandemic began to proliferate in March 2020. Non-essential medical procedures were suspended and access to medical facilities was limited to medical personnel and patients who could not be treated remotely. 6 To meet the behavioral health need within the confines of COVID-19 containment measures, many systems adopted platforms to deliver care remotely, and professional organizations passed emergency orders to mitigate barriers related to licensing jurisdictions. For example, in the Military Health System, the use of telehealth markedly increased during the pandemic. 7 Even as containment measures have abated, many systems maintain some level of telehealth services and multiple studies have shown that patients are satisfied with this service modality.8–10
Three recent meta-analyses have examined telehealth modalities for delivery of behavioral health treatment.11–13 A meta-analysis of telehealth studies with U.S. military veterans 12 of both randomized and non-randomized controlled studies found that in-person treatment was more effective at reducing post-traumatic stress disorder (PTSD) symptoms at posttreatment than VTC (d = -0.25, 95% CI −0.39, −0.11) or telephone (d = -0.34, 95% CI −0.56, −0.11). In this study, authors grouped together in-person alternatives of the same therapy protocol and comparison groups where treatment was not controlled by the study team. The authors also used the standard deviation of the change scores to generate standardized mean differences. This technique can produce biased effect size estimates. 14 Another meta-analysis 13 did not find a difference between VTC and in-person care at posttreatment for PTSD treatments delivered in primary care (d = -0.00, 95% CI −0.18, 0.17). The discrepant findings across these two reviews may be due to methodological differences (i.e. different populations and inclusion of non-randomized studies in one of the reviews). With respect to depression, McClellan and colleagues 12 found no differences between in-person delivery compared to VTC (d = 0.00, 95% CI −0.14, 0.13) and telephone (d = -0.09, 95% CI −0.33, 0.14), whereas the comparison of in-person delivery to VTC for anxiety was inconclusive (d = 0.24, 95% CI −0.17, 0.54). The small number of included studies and the inclusion of non-randomized studies limit these findings. A more recent meta-analysis included 11 randomized controlled trials (RCTs) that performed head-to-head comparisons of VTC and in-person therapy in the treatment of depression. 11 They also found no conclusive differences in treatment efficacy (g = 0.04, 95% CI −0.12 to 0.20) or attrition rates (OR = 1.07, 95% CI 0.78 to 1.49). However, these meta-analyses included studies where depression was not the main target and do not speak to the efficacy of treatments that were specifically designed to treat depression. Further, the findings from these meta-analyses are limited by their focus on specific populations (i.e. veterans only or primary care), inclusion of non-randomized studies which can introduce bias, and scope limitations (i.e. omission of relevant service delivery modalities, comparator groups, and mental health conditions). More comprehensive reviews of the telehealth literature include two rapid reviews15,16 and an evidence brief. 17 Overall, the findings from these reviews suggested that telehealth is comparable to in-person delivery. Since none of these reviews conducted meta-analyses, the conclusions are limited.
The Veterans Affairs (VA)/Department of Defense (DOD) clinical practice guidelines (CPGs) highlight the need for further research into this topic. The VA/DOD CPG for the Management of Major Depressive Disorder (MDD) indicates that there was insufficient evidence to recommend for or against telehealth for patients with MDD, 18 citing the lack of RCTs comparing telehealth to in-person treatment and noting limitations of the trials they did find (e.g. population limited to U.S. veterans, telehealth modality limited to VTC). While the VA/DOD CPG for Management of PTSD and Acute Stress Disorder recommends VTC for PTSD, it does not include a recommendation for the use of telephone. 19
The goal of this systematic review was to provide a comprehensive review of the telehealth literature, including different modalities and comparators, and to characterize the state-of-the-science on behavioral health care treatments delivered via telehealth. We performed a meta-analysis and assessed the quality of the evidence across RCTs evaluating the efficacy of evidence-based behavioral health treatment for symptoms or diagnosis of PTSD, depression, or anxiety disorder when delivered via telehealth. Specifically, we sought to answer the following research questions: (a) What is the efficacy of evidence-based interventions for symptoms or diagnosis of PTSD, depression, and anxiety delivered synchronously via telehealth (telephone or VTC) compared to in-person delivery, treatment as usual, or waitlist control? and (b) What is the efficacy of evidence-based interventions delivered via telephone compared to VTC? The synthesis of these findings will help inform future policies and practices related to the provision of evidence-based behavioral health care, as well as address some of the current gaps in the existing syntheses of the literature described above.
Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 20 We registered a protocol for this systematic review with PROSPERO International Prospective Register of Systematic Reviews (PROSPERO Protocol number: CRD42022357247).
Inclusion criteria
We included RCTs (including crossover trials that randomized the order of interventions) published in English of evidence-based telehealth psychotherapies for patients with symptoms or diagnoses of PTSD, depression, or anxiety disorder. For the specific anxiety and depression disorders eligible, see the full eligibility criteria in the Supplementary Material. The telehealth modality had to be delivered synchronously by a provider in real-time via telephone or video. Evidence-based interventions for each condition were determined a priori, based on CPGs that were available at the time we started this review. 21 –24 We excluded interventions where evidence-based treatment had been abbreviated or altered.
Search strategy
A library specialist searched a combination of keywords related to the concepts of telehealth, relevant mental health disorders (i.e. PTSD, anxiety, depression), and evidence-based psychotherapies in three databases (PubMed, PsycInfo, and Embase) from database inception through April 2022. We limited the search to clinical trials published in the English language and utilized controlled vocabulary mapping and concept expansion strategies when applicable. Variations of the complete PubMed search (Supplementary Material) were conducted across all other databases. The team consulted with subject matter experts and searched the National Institutes of Health ClinicalTrials.gov database, World Health Organization's International Clinical Trials Registry Platform, and reference lists of previously published systematic reviews on telehealth11–13 to identify additional published clinical trials.
Data screening and assessment of bias and quality of the evidence
The review team dually screened titles and abstracts for eligibility. The team resolved disagreements through discussion and consensus. We obtained full-text articles for records marked for inclusion at the title/abstract stage and dually screened them using the same criteria. The team then used a customized data extraction form to standardize the data collection process and ensure internal reviewer consistency. A single reviewer extracted study characteristics and results for each study, which were reviewed and verified by a second reviewer. The review team also judged the methodological quality of each study (i.e. selection, performance, detection, attrition, reporting, and other bias) using the Cochrane Risk of Bias Tool. 25 Each study was assessed by two raters, and discrepancies within each pair of raters were resolved through discussion. Lastly, we used Grading of Recommendations Assessment, Development and Evaluation (GRADE) system to assess the quality of the evidence for PTSD, depression, and anxiety outcomes using the following five domains: risk of bias, imprecision, inconsistency, indirectness, and publication bias. 26
Statistical analysis
We conducted univariate meta-analyses of standardized posttreatment differences in PTSD, anxiety, and depression outcome measures. We analyzed the primary outcomes separately by the target diagnosis of the included studies. We extracted or calculated standardized differences at posttreatment. To the extent possible, we followed the technique of Feingold 14 to generate standardized differences using the baseline standard deviation of the outcome measure. We combined assigned treatment groups that shared a delivery modality, such as in-office telehealth and in-home telehealth, when a study had more than two randomized treatment groups. For studies that reported more than one measure of the primary outcome, we used the clinician-administered measure or the measure that was most consistent with other included studies if they did not differ by administration method. In each meta-analysis, we estimated summary effect sizes using a random effects estimator. We evaluated statistical heterogeneity using the I2 estimate. When we encountered statistical heterogeneity, we examined potential covariates (evidence-based therapy protocol, study-qualifying diagnosis, and other study design characteristics) to identify potential effect measure modification. We also evaluated evidence of publication bias using funnel plots when possible. We conducted all analyses using Stata 15. 27
Results
The database searches yielded 2259 references. Hand-searching reference lists and clinical trial protocol databases produced 12 additional records. After removing duplicates, the team screened 1711 references. A total of 29 studies were subsequently included in the review (see reference list in the Supplementary Materials). The PRISMA flow diagram (Figure 1) provides a detailed accounting of exclusions. Characteristics of included studies are described in Table 1. Fourteen RCTs evaluated telephone interventions, 14 evaluated VTC interventions, and in one RCT, participants could choose either telephone or VTC delivery. There were 14 studies that exclusively enrolled civilians, 11 that exclusively enrolled veterans, and four that enrolled mixed samples (three of which included service members).
PRISMA flow chart.
Characteristics of included randomized controlled trials.
BA: behavioral activation; BAI: Beck Anxiety Inventory; BDI: Beck Depression Inventory; CAPS: Clinician-Administered PTSD Scale for DSM-5; CBT: cognitive behavioral therapy; CPOSS: Charleston Psychiatric Outpatient Satisfaction Scale; CPT: cognitive processing therapy; CPT-C: cognitive processing therapy - cognitive only; CSQ: Client Satisfaction Questionnaire; DASS-21: Depression, Anxiety and Stress Scale - 21 items; EAP: Employee Assistance Program; FtF: Face-to-Face; GAD-7: General Anxiety Disorder-7; GAS: Global Assessment Score; GTAS: Group Therapy Alliance Scale; HAMD: Hamilton Depression Rating Scale; HPQ: Health and Work Performance Questionnaire; K6: Kessler Psychological Distress Scale; Min: minutes; Mos: months; NR: not reported; PCL: PTSD Checklist; PE: prolonged exposure; PROMIS: Patient-Reported Outcomes Measurement Information System; PHQ9: Patient Health Questionnaire; PST: problem solving therapy; PTSD: post-traumatic stress disorder; SAS-SR: Social Adjustment Scale-Revised Version; SCID: Structured Clinical Interview for the DSM-5; SCL-90: Symptom Checklist-90; SDPQ: Service Delivery Perceptions Questionnaire; SF-12: Short Form-12; SF-36: 36-item Short Form Health Survey (SF-36); STAI: State-Trait Anxiety Inventory; TAU: treatment as usual; VTC: video teleconference; WAI: Working Alliance Inventory; WAI-S: Working Alliance Inventory - Short Form; wks: weeks; VA: Veterans Affairs.
Telehealth interventions for PTSD
Twelve studies enrolled participants with PTSD. We conducted a meta-analysis using PTSD symptom data from the 11 studies that compared synchronous VTC to in-person treatment directly. The summary effect size and confidence interval across all studies was consistent with no appreciable difference in efficacy; however, this estimate was associated with substantial statistical heterogeneity (Table 2). Stratification by high risk of bias associated with random sequence generation explained some of the observed heterogeneity. Most of the statistical heterogeneity occurred in the subset of studies with a high risk of bias determination. From the studies with low risk of bias in sequence generation, the summary effect size confidence interval was consistent with small differences in efficacy in either direction. There was no evidence of publication bias. We classified the quality of evidence as moderate (Table 3). We did not downgrade the quality of evidence assessment for imprecision despite the confidence interval covering zero 28 because the endpoints of the confidence interval were consistent with small effects in either direction. The lack of study group concealment was a common limitation across the included studies (Figure 2). Only one study provided data on treatment for PTSD delivered via telephone, and the comparison was to treatment as usual as opposed to an in-person version of the same treatment protocol.
Cochrane risk of bias assessment.
Meta-analysis results, by outcome and comparison.
SMD: standardized mean difference; CI: confidence interval; VTC: video teleconference; TAU: treatment as usual. Note: Negative mean differences favor telehealth.
GRADE quality of evidence.
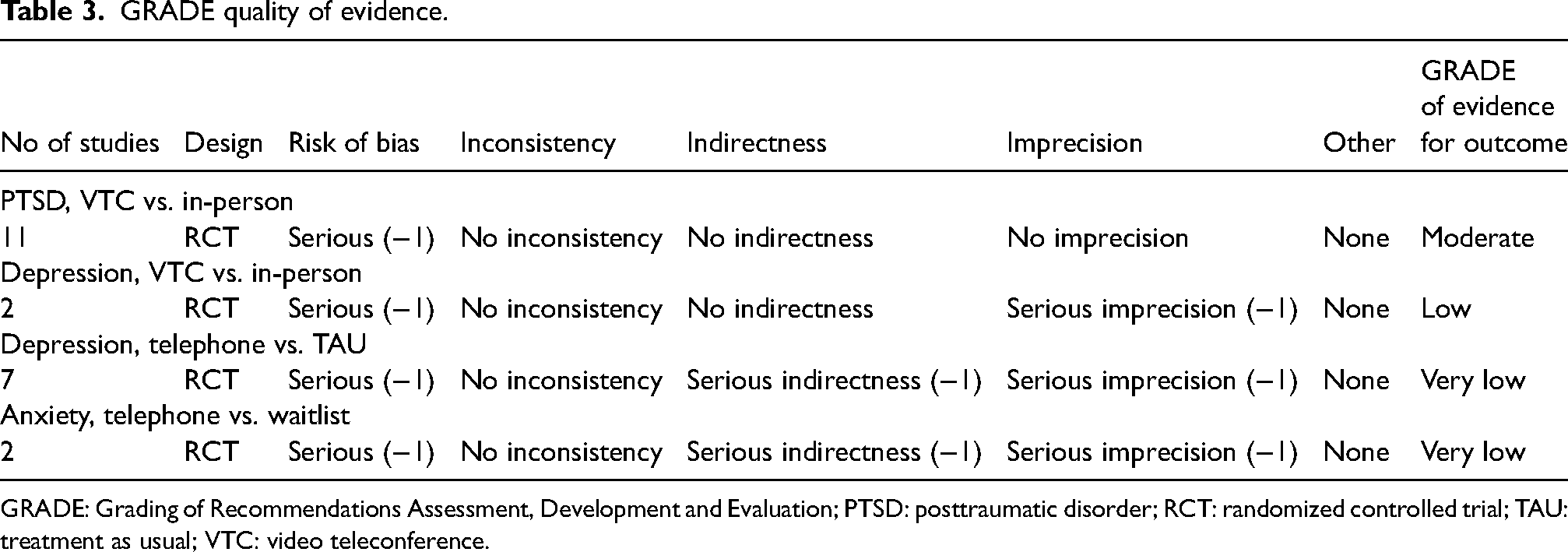
GRADE: Grading of Recommendations Assessment, Development and Evaluation; PTSD: posttraumatic disorder; RCT: randomized controlled trial; TAU: treatment as usual; VTC: video teleconference.
Telehealth interventions for depression
Twelve studies examined telehealth in the treatment of depression. Two studies compared VTC to the in-person alternative, one compared VTC to treatment as usual, one compared telephone to in-person delivery, one compared telephone to waitlist, and seven compared telephone delivery to treatment as usual. The confidence interval summary effect size for the two studies that compared VTC to the in-person was consistent with true differences ranging from effectively none to moderate superiority of the in-person protocol. We rated the quality of evidence for this comparison as low because of study-specific risk of bias and imprecision.
The evidence across the seven studies that compared telephone delivery to treatment as usual was consistent with small-to-moderate superiority of telephone delivery. Since this comparison did not involve the same treatment protocol for both study groups, we cannot isolate the effect attributable to telehealth. We rated the quality of the evidence as very low for individual study risk of bias, indirectness, and imprecision.
Telehealth interventions for anxiety
Five studies targeted anxiety as the primary diagnosis. Two studies compared telephone to waitlist. The other three studies each differed in the type of comparison under study. The summary effect size estimate and confidence interval for the two studies that compared telephone delivery to waitlist were consistent with superiority of telephone delivery. The confidence interval was consistent with both very small and very large true differences. We rated the quality of evidence as very low for study-specific risk of bias, indirectness, and imprecision.
Effects of telehealth interventions for PTSD, depression, and anxiety on secondary outcomes
The majority (k = 20) of studies examined additional outcomes such as quality of life, therapeutic alliance, satisfaction with treatment, and functioning within important life domains (e.g. mental, physical, social, and occupational). The estimates for these outcomes are reported in Table 1. The heterogeneity of the measures used, target diagnoses, and modalities compared across each of these constructs precluded computation of meta-analytic estimates. In general, patients assigned to telehealth interventions may have greater improvements in mental health functioning post-intervention relative to treatment as usual or information control and did not differ from those assigned to in-person delivery. However, the results were inconclusive for other types of functioning and quality of life. Further, patients randomized to telehealth treatment expressed a high degree of therapeutic alliance and satisfaction.
Discussion
A synthesis across 29 studies indicated that the efficacy of telehealth for delivery of evidence-based behavioral health interventions varies by target diagnosis and telehealth modality. Moderate quality of evidence showed that VTC may be comparable to in-person delivery for patients with PTSD. However, for those with symptoms or diagnosis of depression, in-person delivery was associated with better outcomes compared to VTC. We also found that evidence-based treatments delivered over telephone were more efficacious for depression compared to treatment as usual; however, the quality of the evidence was rated as very low. Very low quality of evidence supported the use of telehealth versus waitlist for symptoms or diagnosis of anxiety.
Our findings are consistent with other research showing that VTC and in-person delivery may be comparable for patients with PTSD.11–13,15,16 However, our findings with respect to VTC for depression diverge from other meta-analyses.11,12 Those meta-analyses included studies where depression was not the main target. Thus, unlike our findings, they do not speak to the efficacy of evidence-based treatments that were specifically designed to treat depression. The results support the conclusions of other research regarding the benefits of telehealth for psychology, psychiatry, and across other medical disciplines.29,30 Our findings are relevant to workgroup members engaged in the updates of CPGs. The VA/DOD MDD CPG currently states that there is insufficient evidence to recommend telehealth for the treatment of MDD. 18 Our finding that telephone may be more beneficial than treatment as usual indicates the need to reevaluate these recommendations in the future. Our findings also support the current recommendations for evidence-based treatment delivered via VTC for PTSD. 19
No studies directly compared telehealth modalities (i.e. VTC versus telephone) and indirect comparison between modalities was not possible due to use of different comparators across modalities (in-person for VTC studies and treatment as usual/waitlist for telephone studies). Though some evidence supports the delivery of evidence-based interventions via telephone, research comparing telephone to in-person delivery or VTC is needed.
Limitations and future directions
We included only English language studies. Our findings only apply to evidence-based treatments delivered via telehealth; non-evidence-based treatments were outside the scope of this review. This body of research included studies that used self-report measures for the measurement of mental health symptoms. Clinician-rated outcomes minimize concerns related to blinding of outcome assessment. Future telehealth studies should utilize clinician-rated tools to measure outcomes.
Greater use of telehealth interventions may be promising for increasing access to evidence-based behavioral health treatment among certain populations. Telehealth may be particularly useful for service members who deploy to remote areas and individuals who live in rural settings. However, more research is needed on the efficacy of telehealth treatments for depression and anxiety. The field would benefit from studies comparing telehealth to in-person delivery. Future studies should also compare different telehealth modalities to each other. Because some patients might prefer telephone to VTC or vice versa, greater choice with respect to modality might improve adherence to treatment. Currently, smartphones offer patients the choice of auditory and VTC options for connecting with providers.
Further, this body of literature is limited in the breadth of the evidence-based interventions that were evaluated for telehealth. For patients with PTSD, only prolonged exposure and cognitive processing therapy were evaluated. For depression, RCTs examined behavioral activation, cognitive behavioral therapy, and interpersonal therapy. Only cognitive behavioral therapy was evaluated in patients with anxiety. Future research should evaluate telehealth delivery for other types of evidence-based interventions.
Conclusions
A synthesis across 29 studies indicates that the efficacy of telehealth for delivery of evidence-based behavioral health interventions varies by target diagnosis and telehealth modality. More research is needed on the efficacy of telehealth treatments for depression and anxiety. Research is needed to compare telephone to in-person delivery and VTC. This body of literature is limited in the breadth of the evidence-based interventions that were evaluated for telehealth.
Declarations of conflicting interests
The views expressed are those of the authors and do not represent the official policy or position of the Psychological Health Center of Excellence, Defense Health Agency, Department of Defense, or the United States Government.
This systematic review has been conducted to inform Military Health System stakeholders on the state-of-the-science on telehealth. The results presented here are relevant to military and civilian populations alike. Our forthcoming dissemination efforts discuss relevance of this topic to military service members and other Military Health System beneficiaries.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X231224491 - Supplemental material for Evidence-based telehealth interventions for posttraumatic stress disorder, depression, and anxiety: A systematic review and meta-analysis
Supplemental material, sj-docx-1-jtt-10.1177_1357633X231224491 for Evidence-based telehealth interventions for posttraumatic stress disorder, depression, and anxiety: A systematic review and meta-analysis by Marija S Kelber, Derek J Smolenski, Courtney Boyd, Lisa M Shank, Dawn M Bellanti, Tiffany Milligan, Amanda Edwards-Stewart, Salvatore Libretto, Kelly Parisi, Maria A Morgan, and Daniel P Evatt in Journal of Telemedicine and Telecare
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.