
Abstract
Aim
To evaluate Sweden's first implementation of a 24/7 high-acuity virtual in-patient ward through a digi-physical in-patient care (DPIPC) program, a hospital-at-home care model combining a virtual hospital-based medical command centre and in-person ambulating medical services functioning as an extension of the Department of Medicine at a secondary-level hospital in Stockholm.
Methods
A single-centre descriptive study where adult patients with acute medical illness requiring inpatient-level care were assessed for voluntary treatment in the DPIPC program as a substitute for traditional in-patient care. The primary outcome was patient satisfaction with care. Secondary outcomes included health care use, safety, and quality during the care episode.
Results
From October 2022 to June 2023 a total of 200 patients were treated within the DPIPC program. The program covered 63 unique medical conditions, with infectious disease (44%) and pulmonary disease (17%) being the most common. The median length of stay (LOS) in the DPIPC program was 3 days (IQR 3) with a median LOS of 2 days (IQR 3) in the physical hospital prior to inclusion. There were no incidents of patient mortality or hospital-related complications during the DPIPC period. A total of 11 (5.5%) patients were escalated to the traditional hospital, 4 (36.4%) of which required ambulance. The median DPIPC patient satisfaction was 10 (IQR 0) and Net Promotor Score was 88.
Conclusions
Implementing a 24/7 high-acuity virtual in-patient ward is feasible and safe for selected patients with acute medical illnesses. Patient satisfaction and care quality within the program is high.
Keywords
Introduction
Healthcare systems are facing significant challenges, including aging populations, rising healthcare demands and costs, and shortages of hospital resources and personnel. These limitations have adverse effects on the efficiency and quality of care, resulting in decreased patient and staff satisfaction and increased healthcare expenses. 1
With the lowest number of hospital beds per 100,000 citizens in Europe, 2 Sweden experiences overcrowded wards which has been shown to compromise patient safety, 3 highlighting the urgent need for innovative solutions. The care model hospital-at-home (H-a-H) has been identified as a possible solution and provides acute hospital-level care in a patient's home as a substitute for traditional in-patient care in a brick-and-mortar hospital. International experience indicates that H-a-H care can improve patient experience, reduce length of stay (LOS), reduce costs while also maintaining the quality and safety of traditional in-patient care.4–10 To date, Sweden has no 24/7 high-acuity H-a-H program substituting hospital-level in-patient care.
The H-a-H model is wide-spread in several countries such as Australia, Spain and the United States, though ways-of-working and the use of digital tools within each program can vary significantly.4,11 We aim to evaluate Sweden's first implementation of a 24/7 high-acuity virtual in-patient ward through a digi-physical in-patient care (DPIPC) program – a modified H-a-H care model combining a virtual hospital-based medical command centre and in-person ambulating medical services functioning as an extension of the Department of Medicine at a secondary-level hospital in Stockholm.
Methods
This was a single-centre descriptive study where adult patients presenting with acute medical illness requiring hospital-level care were treated in a DPIPC program as a substitute to traditional brick-and-mortar in-patient care.
Setting and study population
The study was conducted at the Department of Medicine at Sankt Görans Hospital, a secondary-level 340-bed Hospital in Stockholm, Sweden, from October 4th, 2022, through to June 21st, 2023. Prior to admitting patients into the program, the hospital and DPIPC clinicians conducted a thorough risk assessment, ensured compliance with healthcare standards and regulations and engaged in extensive communication with physicians and care staff at the hospital.
The patient inclusion process was initiated by hospital clinicians who communicated with DPIPC clinicians when identifying potential candidates for the program. DPIPC clinicians reviewed the charts of candidates and approached them or their proxy, described the program, and completed a history and bedside physical examination to determine final eligibility status. Patients were included directly from the emergency department (Admission Avoidance) and from the brick-and-mortar hospital ward after having stayed at least one night at the hospital (Early Discharge). Patient inclusion did not require a referral.
Patients were eligible for DPIPC admission if they; were 18 years or older, lived within 30 minutes from the hospital via car, concentrated to the DPIPC program, patient or relative could ambulate to the front door, had a set diagnosis and care plan, were clinically stable, would require no more than four planned home visits per day.
An absolute exclusion criterion was if patients were in need of a higher care level than a regular inpatient ward. Relative exclusion criteria included new onset of oxygen dependency of >3 litres per minute and factors making the patient unsuitable for DPIPC such as high risk of falling, inability to operate the tablet or a home environment unsuitable for H-a-H care. Eligible admissions were not related to diagnosis or condition and patients were able to be admitted between 7 AM and 6 PM all days of the week. Living alone was not an exclusion criteria. Admission to the DPIPC program was completely voluntary and patients could opt out of the program at any point of their care episode.
An around-the-clock virtual medical command centre was set up at the hospital where a registered hospital nurse and hospital physician were available to patients and ambulating care staff through chat, video calls and telephone. The command centre monitored patients’ vital signs and managed all care coordination of both digital consultations and in-person care via ambulatory care staff (registered nurses and nurse practitioners) available to patients in their homes.
Upon admission, patients were introduced to an in-home technology kit consisting of a tablet from which they could contact the medical command centre at the hospital at any time and see their schedule of digital and physical appointments with medical personnel. Patients also received medical devices to measure their vital signs: a blood pressure cuff, a pulse oximeter, an ear thermometer, and a weight scale. Back-up supplies such as power supply battery and cellular communications modem was provided as needed as well as a lifeline device emergency response bracelet, for example if the patient was deemed at high risk of fall.
The episode of DPIPC was initiated after a clinical handoff from the hospital physician to the H-a-H physician. Patient information was kept in the hospital EMR. Care coordination of orders were planned and organised in the command centre and communicated to the patient and ambulating care staff. The patient was transferred home by taxi service or by DPIPC personnel. Once the patient was at home, an ambulating nurse or nurse practitioner made an introductory home visit within 2 hours making sure the home was suitable for DPIPC and that the technology set up was satisfactory.
Patients received daily digital video rounds by the DPIPC physician based in the medical command centre. A total of five DPIPC physicians were active within the program, all of whom were specialists in internal medicine. Patients received at least one physical visit per day by ambulating nurse. In-person acute care services included, but were not limited to, physical examination, illness and vital signs monitoring, intravenous infusions (e.g. antibiotics, diuretics, fluids for rehydration), wound care, medication administration, mobile diagnostics such as ultrasound and 12-lead ECG, nursing care and education regarding the patient's illness – all of which could be overseen by the medical command centre when necessary. Frequently, physician had video calls facilitated by an ambulating nurse at home.
A physiotherapist was available as needed. Equipment in the form of medical consumables and medical durables such as oxygen concentrator, inhalator, home infusion kit and crutches were provided to the patients’ home as needed. All medical equipment was CE-marked. Nurses prepared all ordered medication for the first 2 days of the program. Thereafter, depending on patient compliance, patients either took care of their own per oral medicine or nurses continued to prepare all medication.
In the event of patient deterioration, the medical command centre connected through video with the patient to perform a virtual evaluation of the patient's medical status. If deemed necessary, the patient could be transferred back to the hospital for evaluation or admission to a physical ward, either by ambulance or by DPIPC personnel depending on severity of their condition. This was termed escalation. When escalated, the DPIPC physician met up with the patient either in the home or at the hospital. Escalated patients were transported directly to a ward at the Department of Medicine bypassing the emergency department. The nurse in the command centre was available to the patients 24 hours a day and could at any time contact the on-call DPIPC physician for a consultation and/or visit the patient for an urgent evaluation. When the patient's acute illness had resolved, the patient was discharged from acute care and provided a discharge summary and relevant outpatient follow-up in the exact same manner as a regular in-patient at the brick-and-mortar hospital would have received.
Data collection and analysis
All data were collected prospectively. Data collection included standardised data from medical charts, administrative record abstractions and ratings of care. All measures were derived from the Electronic Health Record or patients and registered by a research nurse. Because these data were used for internal program evaluation and reporting patient consent for data collection was not required. Regional Human Research Ethics Committee approval was obtained.
The primary outcome was patient satisfaction with care. Secondary outcomes included health care use, safety, and quality during the acute care episode. Patient satisfaction was measured through a rating questionnaire relating global patient experience1–10 and how likely they were to recommend DPIPC to a patient in a similar position on a scale of 0 to 10. The latter was calculated through a Net Promoter Score (NPS) by subtracting the percentage of Detractors (0–6 scores) from the percentage of Promoters (9–10 scores), resulting in a score ranging from -100 to 100. 12
Health care use comprised of total LOS, digital consultations and activities, laboratory orders, radiological examinations, and escalations. Safety was measured through frequency of iatrogenic complications such hospital-related infections, delirium and fall injury. Care quality was measured through 30-day all-cause mortality and hospital readmissions. Patient characteristics was measured such as demographics, activities of daily life and perceived life quality through EQ-5d.
Continuous variables are expressed as mean ± standard deviation or as median and interquartile range, in cases of skewed distributions. Categorical variables are expressed as frequencies and percentages.
Results
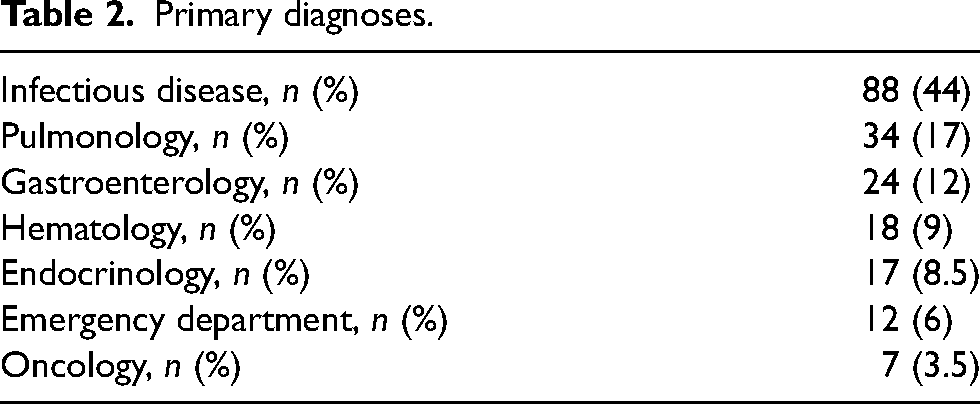
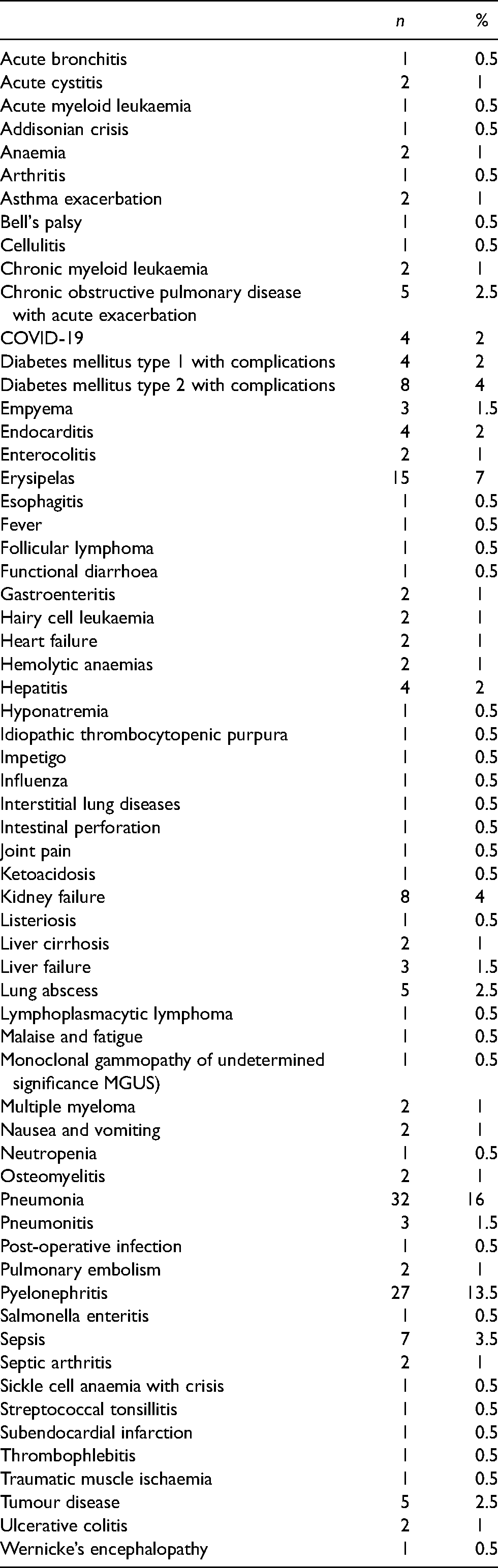
From October 2022 to June 2023 a total of 305 patients were marked as potential patients for DPIPC by hospitalist physicians at the Department of Medicine. Seventy-five patients (71.4%) were excluded due to geographical or medical reasons as presented in flow chart (Figure 1). Out of 230 eligible patients, 30 patients (13%) did not consent. Patients’ baseline characteristics are presented in Table 1. The median age of participants was 67.5 years with a balanced gender distribution (42% female). The DPIPC program included 63 unique medical conditions (Appendix 1) where infectious disease (44%) and pulmonology (17%) where most prevalent (Table 2). Patients had a median medical severity of 2 and a majority of patients had several previous chronic conditions and medications.
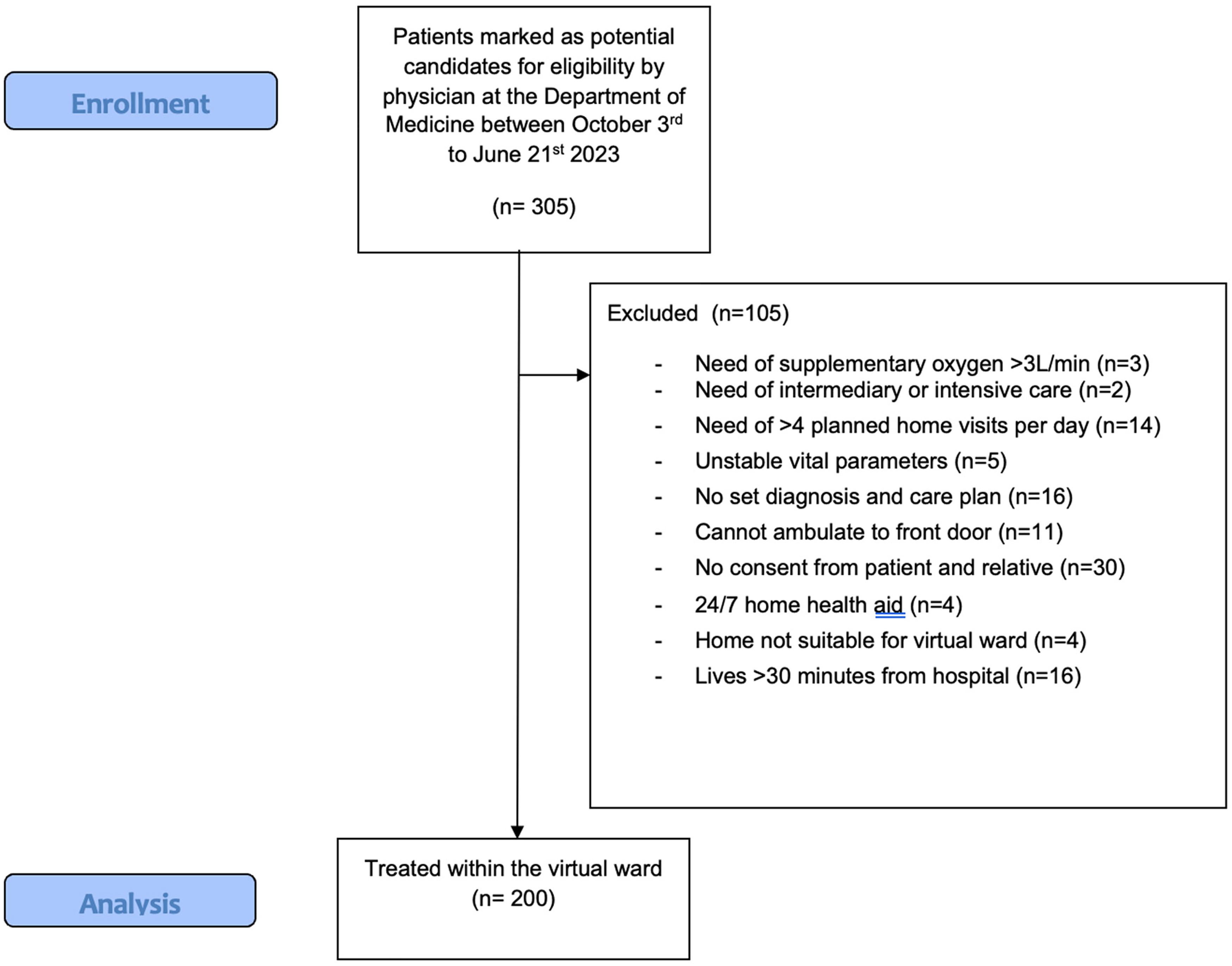
Study flow chart.
Baseline characteristics.
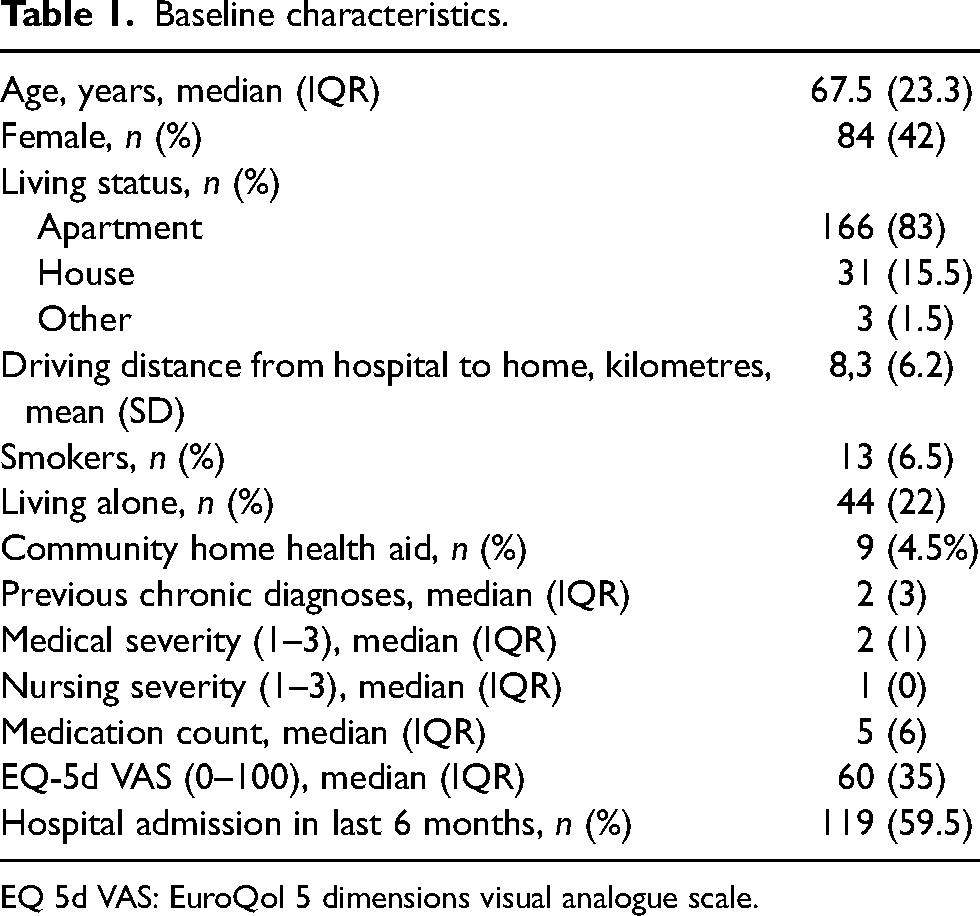
EQ 5d VAS: EuroQol 5 dimensions visual analogue scale.
Primary diagnoses.
The median LOS under DPIPC was 3 days (IQR 3, range 0.4–28.8 days) with patients having a median LOS of 2 days (IQR 3, range 0.0–42.1 days) in the physical hospital prior to entering DPIPC. There were no incidents of patient mortality or hospital-related complications such as fall, delirium or pressure ulcers during the care period (Table 3). A total of 11 patients (5.5%) were escalated to the physical hospital during admission of which 8 patients’ (72.7%) primary condition deteriorated, 2 patients (18.2%) had acute on-set of atrial fibrillation and 1 patient (9.1%) had unclear abdominal pain requiring diagnostic surgery. Of the 11 escalations, 4 (36.4%) were transported with ambulance to the hospital. Post-discharge data revealed that 5.5% were readmitted to the hospital within 30 days. One patient (0.5%) died within 30 days of discharge due to a known terminal peritoneal carcinoma. A majority of patients (78.5%) provided feedback with regards to patient satisfaction and reported a median patient satisfaction of 10 (IQR 0, range 5–10) and NPS of 88 (Table 3). A summary of the digital interactions between patients and health care personnel is presented in Table 4, showing high usage of chat messages and self-reported vital parameters.
Outcomes.
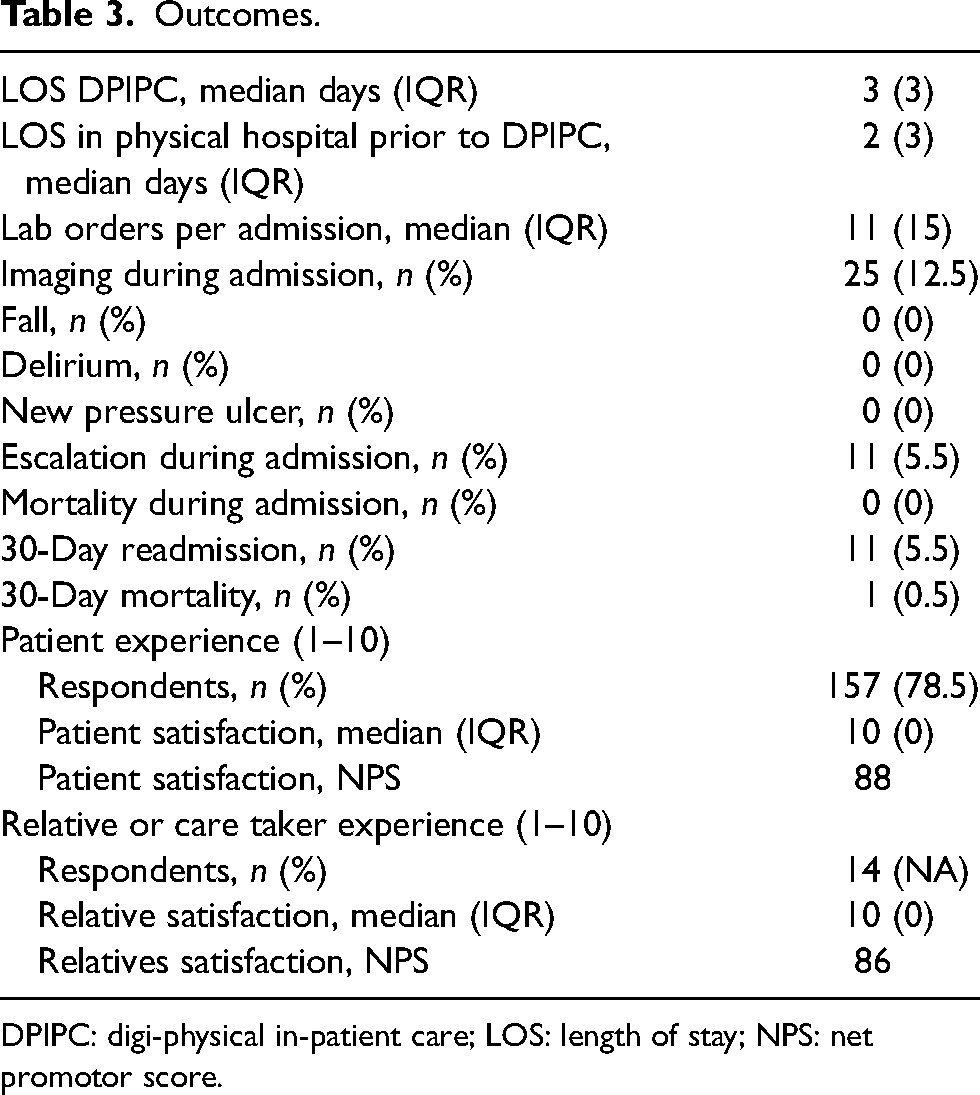
DPIPC: digi-physical in-patient care; LOS: length of stay; NPS: net promotor score.
Digital interactions between patient and health care personnel.
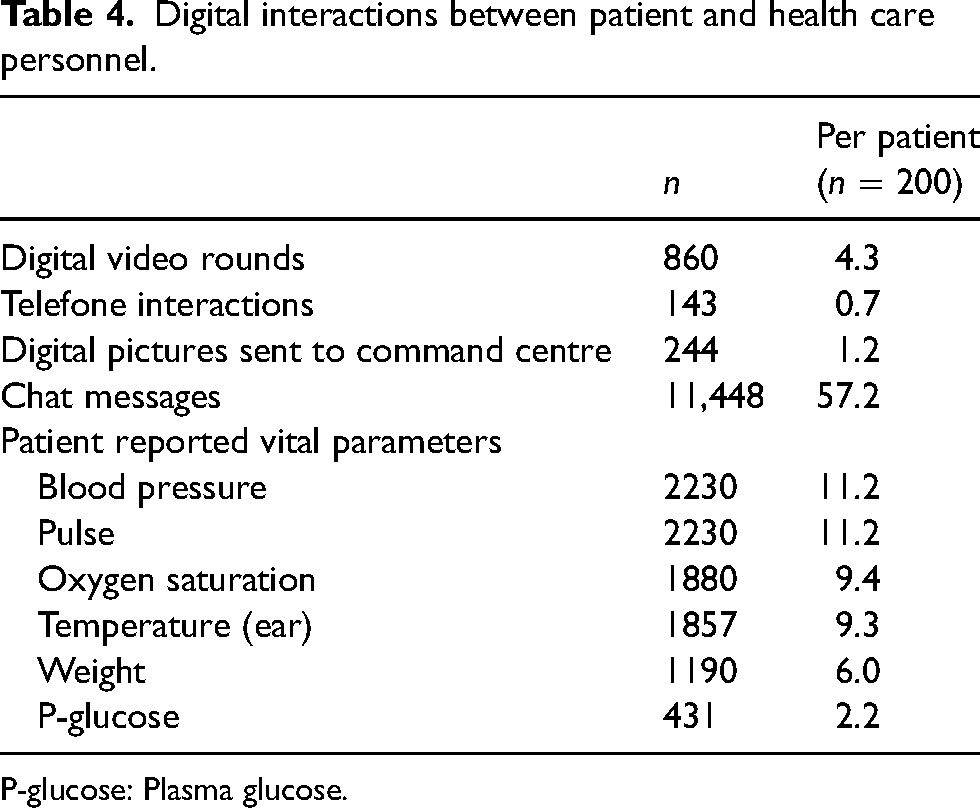
P-glucose: Plasma glucose.
Discussion
The objective of our study was to examine the feasibility of implementing Sweden's first digi-physical H-a-H program at a secondary-level hospital as an alternative to traditional in-patient care. The DPIPC program, a modified H-a-H care model integrating both digital and physical components of H-a-H care, was evaluated and our primary outcome revealed high patient satisfaction, alongside noteworthy secondary outcomes, such as the short average LOS and low readmission rates.
The ‘H-a-H’ care model is well established and is associated with faster patient recovery and higher patient satisfaction when compared to traditional hospital care. However, these programs rely on daily home visits by both physicians and nurses.4–10 In the wake of the COVID-19 pandemic, healthcare systems underwent significant digital transformations13–16 and though digital tools and technology have been associated with improved communication and better care quality, their use within H-a-H programs is still rare.17–19 In the present study, we used a digi-physical approach where physicians could remain in the hospital owing to remote communication capabilities for both patients and ambulating care givers. A significant proportion of eligible patients (87%) opted for the DPIPC program, suggesting that a digi-physical model feels safe to patients and relatives at inclusion. Patients rated the care experience at discharge with a median rating of 10 and a Net Promotor Score of 88, showing that patients were very satisfied and would to a very high extent recommend this care model to others. This could be reflective of an evolving healthcare landscape where patients are both more used to and appreciate digital tools and seek more personalised and convenient care models.
The care provided within the program leans heavily on a patient-centric approach: patients have the opportunity of being with their loved ones, eating preferred meals, navigating their personal space, and resting in their familiar bed, all under the safe guidance of health care professionals. Previous studies have found that the home environment stands out as the preferred setting of care for both patients and caregivers in terms of self-care during and after their care episode.20,21 To be able to educate patients in the home with first-hand knowledge of their actual routines increases patient engagement and compliance which, in our opinion, makes the transition from in-patient care to out-patient care smoother and could reduce readmission rates. The readmission rate 30 days after discharge was 5,5% in the present study, which can be compared to 8.6% for the Department of Medicine in general during the same period the year before the implementation.
A significant concern with H-a-H models is patient safety. However, our study revealed no occurrences of common hospital-related complications like falls, delirium, or pressure ulcers. Hospital-based imaging was performed on 12.5% of patients and 5.5% of patients needed escalation to the physical hospital, demonstrating the need for robust routines and an around-the-clock connection to the physical hospital to ensure that patients receive appropriate care levels when required. In-patient conditions are by definition unpredictable and the hospital's resources in the form of diagnostic and treatment capabilities as well as competence is vital for high care quality. Included patients had acute medical conditions with a median medical severity of 2 (out of 3). A majority had multiple pre-existing chronic conditions and medications, and a significant portion had been hospitalised within the 6 months leading up to the current admission, indicating that they were highly acute and complex cases. Despite this, only one mortality occurred within 30 days post-discharge attributable to a previously identified terminal condition. This suggests that the DPIPC program upholds patient safety standards in line with those of conventional inpatient care.
In the present study, the inclusion criteria were broad resulting in the inclusion of a wide variety of patients from the Department of Medicine. Despite not including patients from the Department of Cardiology, which contributes to a significant proportion of patient inclusions in other hospital at home programs, we saw a remarkably high patient inclusion rate compared to other nascent programs. 22 We believe that a critical aspect of our program’s successful implementation was the comprehensive informational sessions given to the brick-and-mortar hospital physicians. This equipped them to recognise suitable patients for DPIPC, streamlining referrals enhancing our initiative’s uptake. Included patients had a short average LOS of 3 days in DPIPC and had varying LOS at the physical hospital prior to inclusion (range 0.0–42.1 days) further demonstrating flexibility of DPIPC.
If properly introduced, digital tools such as chat, video and remote patient monitoring could provide efficiency to H-a-H programs and be a valuable mechanism for patient education and early signs of patient deterioration. 23 The heavy utilisation of chat messages and self-reported vital parameters indicates that patients actively engaged with the digital tools provided, irrespective of age and tech-savviness. Such active engagement not only promotes patient autonomy but also saves time for health care personnel and providers can make informed decisions based on real-time data. However, enhanced monitoring capabilities alone isn’t sufficient to manage high-acuity patients at home. Monitoring advancements must be met with an equal increase of on-site on-demand diagnostic and treatment capabilities, carried out by healthcare professionals who possess or can readily access the necessary specialised expertise. Otherwise, we believe there could be a notable surge of in-program escalations. The DPIPC model allows for the unique knowledge that specialised hospitalists possess to be easily accessed and benefit both patients and ambulating care providers.
Limitations
Our study has limitations. Data collection relied on retrospective information extracted from electronic medical records. Patient inclusion could be subjected to care giver selection bias as relative exclusion criteria were decided at the discretion of the attending DPIPC physician. Individuals more comfortable with technology or those with prior favourable to virtual healthcare experiences might have been more predisposed to opt for the DPIPC program potentially introducing additional selection bias.
This was a single-centre study, and the geographic makeup of admitted patients was limited to a domicile <30-minute drive time to a centrally located hospital potentially excluding rural patients potentially limiting the study's generalisability.
Conclusions
Sweden's first DPIPC program presents a promising alternative to traditional in-patient care, with its high patient satisfaction and encouraging safety metrics. As the healthcare sector continues to evolve, it is essential to further investigate and refine such innovative care models, ensuring they meet the dynamic needs of patients while maintaining, if not enhancing, the quality of care.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mikael Kastengren discloses that he is the co-founder and Chief Research and Development Officer of Medoma AB, the company that provides equipment and staff as a subcontractor to Capio Sankt Görans Hospital to operate the DPIPC program. No other authors have any personal or financial conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Appendix 1. Complete list of diagnoses
| n | % | |
|---|---|---|
| Acute bronchitis | 1 | 0.5 |
| Acute cystitis | 2 | 1 |
| Acute myeloid leukaemia | 1 | 0.5 |
| Addisonian crisis | 1 | 0.5 |
| Anaemia | 2 | 1 |
| Arthritis | 1 | 0.5 |
| Asthma exacerbation | 2 | 1 |
| Bell's palsy | 1 | 0.5 |
| Cellulitis | 1 | 0.5 |
| Chronic myeloid leukaemia | 2 | 1 |
| Chronic obstructive pulmonary disease with acute exacerbation | 5 | 2.5 |
| COVID-19 | 4 | 2 |
| Diabetes mellitus type 1 with complications | 4 | 2 |
| Diabetes mellitus type 2 with complications | 8 | 4 |
| Empyema | 3 | 1.5 |
| Endocarditis | 4 | 2 |
| Enterocolitis | 2 | 1 |
| Erysipelas | 15 | 7 |
| Esophagitis | 1 | 0.5 |
| Fever | 1 | 0.5 |
| Follicular lymphoma | 1 | 0.5 |
| Functional diarrhoea | 1 | 0.5 |
| Gastroenteritis | 2 | 1 |
| Hairy cell leukaemia | 2 | 1 |
| Heart failure | 2 | 1 |
| Hemolytic anaemias | 2 | 1 |
| Hepatitis | 4 | 2 |
| Hyponatremia | 1 | 0.5 |
| Idiopathic thrombocytopenic purpura | 1 | 0.5 |
| Impetigo | 1 | 0.5 |
| Influenza | 1 | 0.5 |
| Interstitial lung diseases | 1 | 0.5 |
| Intestinal perforation | 1 | 0.5 |
| Joint pain | 1 | 0.5 |
| Ketoacidosis | 1 | 0.5 |
| Kidney failure | 8 | 4 |
| Listeriosis | 1 | 0.5 |
| Liver cirrhosis | 2 | 1 |
| Liver failure | 3 | 1.5 |
| Lung abscess | 5 | 2.5 |
| Lymphoplasmacytic lymphoma | 1 | 0.5 |
| Malaise and fatigue | 1 | 0.5 |
| Monoclonal gammopathy of undetermined significance MGUS) | 1 | 0.5 |
| Multiple myeloma | 2 | 1 |
| Nausea and vomiting | 2 | 1 |
| Neutropenia | 1 | 0.5 |
| Osteomyelitis | 2 | 1 |
| Pneumonia | 32 | 16 |
| Pneumonitis | 3 | 1.5 |
| Post-operative infection | 1 | 0.5 |
| Pulmonary embolism | 2 | 1 |
| Pyelonephritis | 27 | 13.5 |
| Salmonella enteritis | 1 | 0.5 |
| Sepsis | 7 | 3.5 |
| Septic arthritis | 2 | 1 |
| Sickle cell anaemia with crisis | 1 | 0.5 |
| Streptococcal tonsillitis | 1 | 0.5 |
| Subendocardial infarction | 1 | 0.5 |
| Thrombophlebitis | 1 | 0.5 |
| Traumatic muscle ischaemia | 1 | 0.5 |
| Tumour disease | 5 | 2.5 |
| Ulcerative colitis | 2 | 1 |
| Wernicke’s encephalopathy | 1 | 0.5 |