
Abstract
Introduction
Telehealth has the potential to improve access to mental health care, especially for people living in rural and remote regions. Yet, telehealth accessibility remains a challenge in Australia, and there is a scarcity of appropriate, psychometrically sound tools for evaluating telehealth use by mental health service users. The aim of this study was to adapt and validate a scale for measuring factors associated with mental healthcare telehealth use.
Methods
A 39-item scale was adapted from the Theoretical Domains Framework questionnaire (TDFQ); a 14-domain framework for measuring implementation of evidence-based practice in health research and service delivery. Since use of the TDFQ in the service user and telehealth space is novel, we adapted and piloted the TDFQ using a rigorous and iterative consultation process and analysis. The study sample included 208 people who use mental health services (52% male). Preliminary analysis identified 32-items for inclusion in the exploratory factor analysis. Internal reliability and construct validity were also analysed.
Results
The resulting 21-item telehealth adaption of the TDFQ includes four factors, each with good internal reliability: satisfaction and habit (6 items), knowledge and training (5 items), benefit and value (6 items), and emotionality (4 items). Both the total scale and individual factors were positively associated with telehealth use.
Discussion
The telehealth adaption of the TDFQ is a psychometrically sound tool for assessing factors associated with the use of telehealth by people who use mental health services.
Keywords
Introduction
Australia is facing a shortage of mental health providers to meet the treatment needs of the one in five Australians who experience a mental illness in any one year. 1 This situation worsened during the COVID-19 pandemic, with a 47% increase in workforce shortages in the healthcare sector, including mental health services. 2 Further to this, 30% of Australians live in rural and remote regions. 3 While the prevalence of mental illness in these areas is proportionate to metropolitan cities, access to mental healthcare, including psychology and psychiatry, is significantly more limited. 4
Telehealth, defined as the delivery of healthcare using information and communication technology (ICT) to facilitate audio, visual and/or data exchange between patients and healthcare providers, 5 stands to be a powerful tool for expanding access to care. For instance, telehealth has been shown to reduce financial burden, employment disruption and travel expenses, particularly for rural and remote residents and those with poor access to transport, 6 and allows for scheduling flexibility for the provider and service user. In mental health settings, telehealth can be the preferred modality for service provision in certain psychiatric conditions (e.g., OCD) and patient cohorts (e.g., forensic settings). It is also increasingly being used for early intervention in co-responder models in partnership with police and ambulance services. 7 Telehealth also decreases the risk of airborne infectious disease transmission, such as COVID-19, 6 an important consideration for both mental health patients and clinicians, particularly those with chronic health conditions.
The effectiveness of telehealth has been extensively researched. Eze et al.'s (2020) umbrella review found that telehealth-delivered mental healthcare was as effective as in-person delivery in 90% of reviews focusing on mental health. 8 Snoswell et al.'s (2021) systematic review of 38 high quality meta-analyses also revealed that telehealth delivered care was as clinically effective, or more clinically effective, than traditional care across telepsychology and telepsychiatry care. 9 In our own research, 89% of service users reported that tele-mental health allowed them to feel safe, maintain control, communicate their needs, and have their privacy protected. 10
Recognising the potential of telehealth to meet the needs of people who access mental health services and anticipating a rise in mental health challenges post-pandemic, Australia's ‘Group of Eight’ universities, 11 along with peak bodies in psychiatry 12 and psychology, 13 have called for the permanent integration of telehealth into routine mental health practice. Despite this advocacy, and substantial investment by the Australian Government to improve access to psychologists via the Better Access Initiative, 14 telehealth accessibility remains a prominent issue in Australia. 15 To address key identified barriers to telehealth use, understanding the perspectives and experiences of people who use mental health services is critical.16,17
Notably, there is a dearth of end-users’ voices in prior tele-mental health research, with studies focusing primarily on service provider perspectives. 18 In particular, there are no validated and reliable tools for measuring factors associated with the use of telehealth by people who use mental health services in the Australian context. Moreover, the use of international measures is constrained by methodological shortcomings, including a focus on outdated or specific hardware and systems, small, nonrepresentative samples,19–23 lack of piloting and psychometric evaluation,20,21,23 and adoption of items from outdated questionnaires. 23 These limitations render current international measures unsuitable for adaption in the Australian mental health context, highlighting the requirement for a tool to address this need.
The present study
To address the scarcity of psychometrically sound tools for measuring factors associated with telehealth use by mental health service users, we assessed the adaptability of the Theoretical Domains Framework Questionnaire (TDFQ) for this context. The TDFQ is a highly cited, flexible tool designed for application in healthcare settings. 24 The tool was developed to measure the 14 domains of the Theoretical Domains Framework 25 : (1) knowledge; (2) skills; (3) social/professional role and identity; (4) beliefs about capabilities; (5) optimism; (6) beliefs about consequences; (7) reinforcement; (8) intentions; (9) goals; (10) memory, attention and decision processes; (11) environmental context and resources; (12) social influences; (13) emotions; and (14) behavioural regulation. 26
The TDFQ is intended for use with the Behaviour Change Wheel (BCW); the most comprehensive and practically useful methodology available for developing behaviour change interventions. 27 After identifying the domain of intervention using the TDFQ, the BCW suggests a target intervention based on a synthesised list of 93 behaviour change tactics. The TDFQ was therefore considered well suited for informing practical guidance to address identified telehealth implementation challenges in the current study. 27
Methods
The present study formed part of a larger mixed methods research project, which sought to improve the uptake of telehealth in mental health services within the Hunter New England (HNE) region of New South Wales, Australia. Ethical approval for this research was obtained from the HNE Health Research Ethics Committee (ETH01176).
Questionnaire adaption
The TDFQ has been applied in a range of research and healthcare contexts, including for intervention design and identifying factors influencing service adoption by providers. 28 However, to our knowledge, this study represents the first attempt to adapt the TDFQ to assess telehealth service uptake by people who access mental health services. To do this, we refined existing items and added telehealth specific items. We then sought expert review of the adapted TDFQ from healthcare providers (psychologists, social workers, psychiatrists, and mental health service managers) to determine suitability for the mental health service context. After consultation, 34 items from the original TDFQ, and five purposely designed questions were included in the initial questionnaire. The five purpose designed questions can be found in Table 2 and cover privacy and confidentiality (item 35), digital accessibility (item 36), physical limitations (item 37), control and convenience (item 38), and quality of communication between patient and clinician (item 39). The 5-point response scale of the TDFQ was maintained (1 = strongly disagree to 5 = strongly agree), however, six items (7, 24, 31, 32, 35, and 37) were reverse scored (1 = strongly agree to 5 = strongly disagree) to ensure that higher values on all items reflected positive endorsement of the item. The resulting 39-item questionnaire was piloted among mental health peer workers to obtain feedback on item readability, clarity, and face validity. As a result, minor amendments were made to the wording of some questions. The final 39-item questionnaire, corresponding original TDFQ domains, and item inclusion or exclusion from the final scale can be found in Table 2.
Sample and recruitment
Service users were eligible to participate in the study if they were i) aged 18 years or older, ii) an Australian resident, and iii) a person who uses a HNE mental health service, which provides specialist drug and alcohol, psychiatry, psychotherapy, and acute mental health care across metropolitan, regional, and rural regions of the HNE district. An anonymous online self-report questionnaire was disseminated (i) via unpaid social media (i.e., Facebook, Twitter, Reddit) campaign, (ii) on iPads in a community mental health service with the support of a peer worker, and (iii) through text messages sent by HNE mental health and drug and alcohol services. Upon completion of the survey, participants were given the choice to be entered into a draw for an iPad Tablet as reimbursement for their time.
Data collection
All data were collected using REDCap data collection software 29 between June and December 2022. Participants were provided with the following definition of telehealth prior to completing the 39-item adapted questionnaire: ‘Telehealth is the secure transmission of a clinical consultation by videoconference over the internet. Telehealth allows patients to have flexible delivery consultations with health professionals without the need and inconvenience of travel. Telehealth allows patients to talk to, hear and see health professionals using high-speed internet, cameras, speakers, and monitors at both locations’, which reflects how telehealth operates within the HNE mental health services. They were then asked to provide demographic, mental health service use, and telehealth use information (see Table 1). This included open ended questions asking about barriers and facilitators to telehealth use, which are reported elsewhere. 10 The survey took approximately 20 min to complete.
Patient sample characteristics
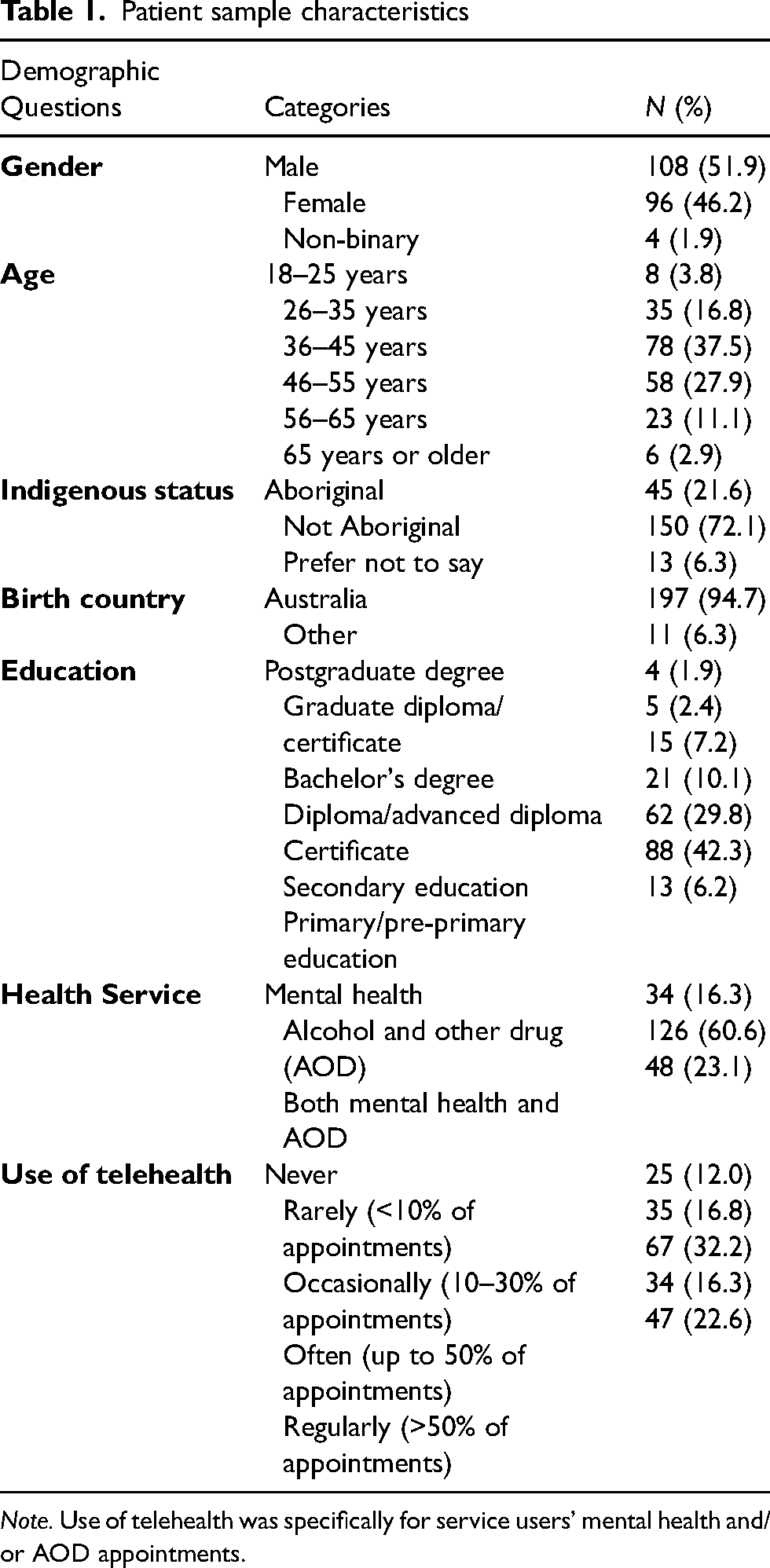
Note. Use of telehealth was specifically for service users’ mental health and/or AOD appointments.
Adaption of the TDFQ for telehealth use among people who use mental health services
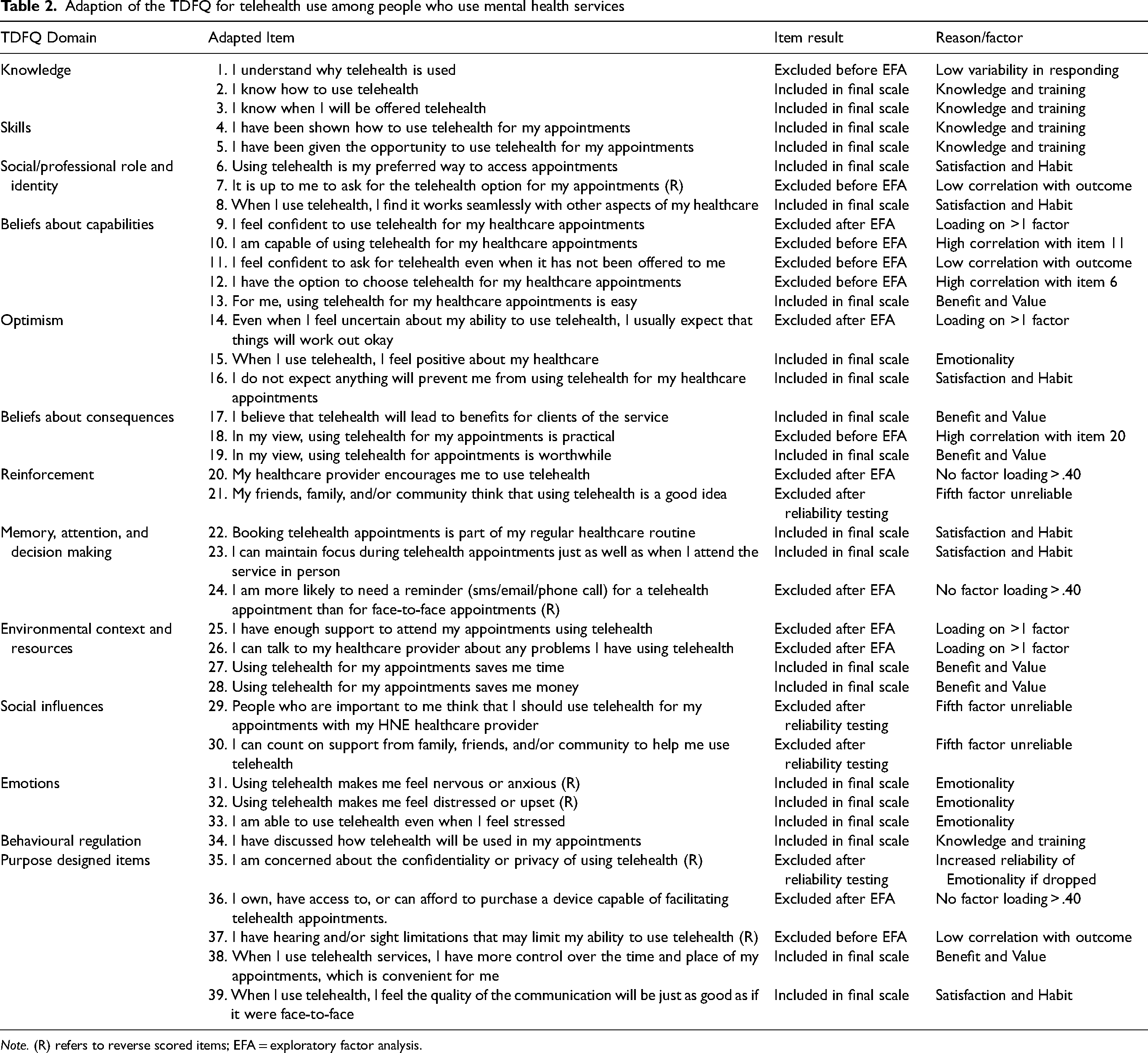
Note. (R) refers to reverse scored items; EFA = exploratory factor analysis.
Data analysis
Data were analysed using IBM Statistical Package for the Social Sciences (SPSS) version 29. 30 Descriptive statistics were used to explore the demographic characteristics of the sample. The mean and standard deviation for each item total score was calculated to ensure variability in responding.
Exploratory factor analysis
Since the TDFQ has not previously been adapted for service users, we conducted an exploratory factor analysis (EFA); a statistical method for identifying order and structure in multivariate data. 31 Specifically, EFA is used to test a pool of items or questions to identify those meaningfully measuring a construct (item reduction), and groups these items to show the possible underlying dimensions of a questionnaire. 32 For this analysis, we followed Watkin's EFA best practice guide. 32 To ensure that the data were appropriate for factor analysis, a Kaiser-Meyer-Olkin (KMO) test of sampling adequacy and Bartlett's test of sphericity were conducted. Mardia's estimates were checked for multivariate skew and kurtosis using WebPower online software (https://webpower.psychstat.org/). Prior to conducting the EFA, correlations among items and the outcome variable were explored for inclusion. The EFA was conducted using Principal Axis (PA) factoring extraction method with Promax rotation, which allows for more realistic representation and interpretation of the data. 32 A value of between .40 and .90 was set as the acceptable factor loading coefficient. Three items per factor are considered acceptable, however four items are considered robust 32 and was chosen as the minimum for this study.
Internal reliability
Cronbach's alpha coefficient (a) and corrected item-total correlations were used to measure internal reliability. A Cronbach's alpha range of .80 to .95 was used to identify reliability of the total scale and each factor, and a corrected item-total correlations of greater than .40 were used to identify internal reliability of each item. Cronbach's alpha was used to check whether removal of any items would increase factor reliability.
Construct validity
To ensure that the final scale measured telehealth use, Spearman's correlations (rs) were used to correlate each factor and the total scale against a question asking how often respondents used telehealth for their mental healthcare appointments (see Table 1). Significant and positive correlations were expected to show that higher scores were associated with increased telehealth use. Spearman's correlations between the final scale and each factor, telehealth use, and demographic variables explored whether demographic factors influenced responding. Figures with a p-value of less than .05 were considered statistically significant.
Results
Respondent characteristics
In total, 337 service users responded to the survey invitation, with 208 completing the survey and constituting the final sample. Participants in the final sample were majority male (n = 108, 51.9%), between 36 and 55 years of age (n = 136, 65.4%), and people who use alcohol or other drug (AOD) services (n = 126, 60.6%) (Table 1). Also included in the sample were 45 Indigenous Australians, representing 21% of the sample.
Exploratory factor analysis
KMO values for the full scale and each item (.938) and Bartlett's tests of sphericity (Chi-square = 4735.55, p < .001) show that the sample and data were appropriate for EFA. Bivariate correlations among items and the outcome variable resulted in the removal of five items prior to EFA. Three items (7, 11, 37) were removed for not correlating significantly with the outcome variable. Items 10 and 11, items 6 and 13, and items 19 and 20 were highly correlated (r = .806, .813, and .820, respectively) and assessing similar concepts, showing redundancy. Items 10, 6, and 20 were retained for higher correlation with the outcome variable. A further one item (item 1) was removed for low variability in responding (mean = 4.36, SD = .72). Therefore, 32 of the 39 items were included in the EFA. A significant value for Mardia's estimates (p < .001) shows that multivariate skew and kurtosis were present in the data. Therefore, PA factoring with Promax rotation was used as this method makes no distributional assumptions. 32
Prior to EFA, internal reliability testing indicated high redundancy among the 32 items (a = .952). The eigenvalues and scree plot resulting from PA factoring indicated extraction of a five-factor solution. At this stage, 7 items were omitted due to no factor loading above .40 (items 20, 24 and 36), or loading onto more than one factor (items 9, 14, 25 and 26). See Table 2 for item inclusion and exclusion.
Internal reliability
The internal reliabilities of factor one, ‘satisfaction and habit’ (six items; a = .893), factor two, ‘knowledge and training’ (five items; a = .825), factor three, ‘benefit and value’ (six items; a = .897), and factor four ‘emotionality’ (four items; a = .808) were good. Factor five, which appeared to be measuring support and encouragement, included only three items (21, 29, and 30) and had an internal reliability below the acceptable threshold of .800 (a = .715). Additionally, two items on factor five (21 and 30) showed an increase in internal reliability if removed. Therefore, factor 5 was removed from the questionnaire. The remaining 21-item scale showed excellent internal reliability (a = .944), and removing any other items led to a decrease in Cronbach's alpha, showing that they were essential for the questionnaire's reliability. See Table 3 for internal reliabilities, factor loadings, and item statistics for the final 21-item questionnaire. All resulting subscale scores indicate that higher values reflect agreement with that subscale.
Final questionnaire items, factors, and factor descriptives
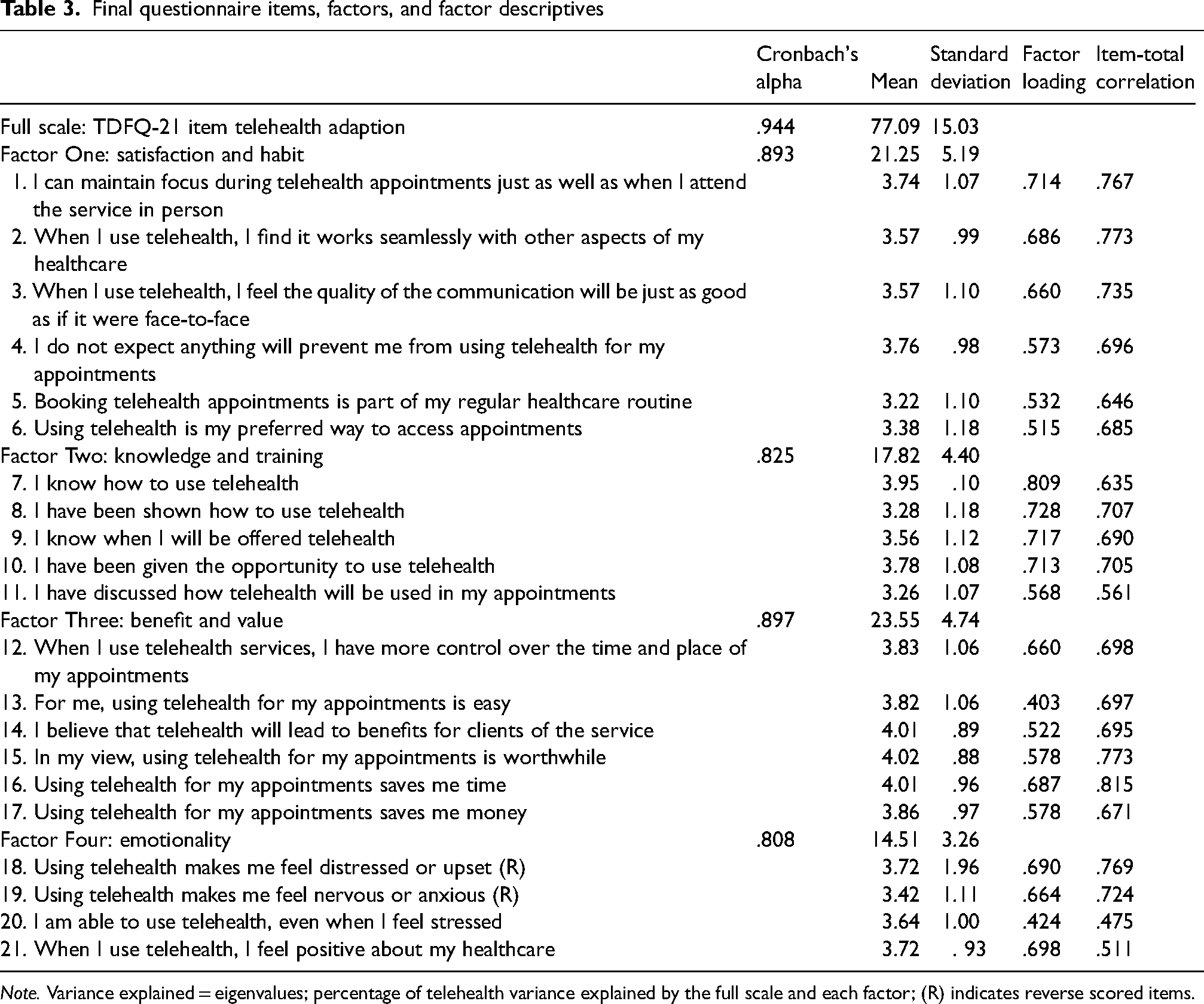
Note. Variance explained = eigenvalues; percentage of telehealth variance explained by the full scale and each factor; (R) indicates reverse scored items.
Construct validity
Spearman's correlation coefficients were calculated for the total questionnaire, each factor, telehealth use, and demographic factors. As expected, telehealth use was significantly and positively correlated with the total scale (rs = .490, p < .001), factor one (rs = .482, p < .001), factor two (rs = .348, p < .001) factor three (rs = .405, p < .001), and factor four (rs = .404, p < .001). Age was negatively and significantly correlated with factor three (rs = -.143, p = .041). There were no other significant correlations between demographic factors and the final scale or each factor.
Discussion
The aim of this study was to assess the adaptability of the TDFQ for measuring factors associated with telehealth use among people who use mental health services in Australia, and to provide a preliminary validation and reliability of the resulting scale. The final scale consisted of 21 items (Cronbach's a = .944) loading onto four factors including (i) satisfaction and habit, (ii) knowledge and training, (iii) benefit and value, and (iv) emotionality; each with good internal reliability (Cronbach's a = .808 - .897). The EFA supported the extraction of a five-factor scale, however psychometric evaluation identified problematic internal reliability of factor five which was thus removed. Further, the total scale and each of the four factors are significantly associated with self-reported telehealth use, showing that higher factor values were associated with increased telehealth use.
The resulting scale and its factors show a unique composition in relation to the original domains of the TDFQ.33,34 Of the 12 TDFQ domains included in the EFA, items from 10 domains were included in the final scale. The TDFQ domains ‘reinforcement’ and ‘social influences’ were not represented in the final scale, however items from these domains were represented in the fifth unreliable factor, which appeared to be capturing support and encouragement. Five items were purpose designed in consultation with expert stakeholders, covering privacy and confidentiality (item 35), digital accessibility (item 36), physical limitations (item 37), control and convenience (item 38), and quality of communication between patient and clinician (item 39). Of these items, two were included in the final scale (items 38–39), while three (items 35–37) did not meaningfully contribute to the factor structure. While this is a somewhat surprising outcome, it is possible that individuals who are concerned about privacy and security may not have responded to the questionnaire for these reasons. It is also possible that people had less concerns around privacy as some of the telehealth services were embedded in public hospital settings which also provides in-person care. While our sample only included a small proportion of older adults (3% were aged 65 year or older) which may be a limitation due to digital accessibility barriers among this population, 35 other research shows that older people are interested in engaging with telehealth for mental health, 36 showing that further research is required to examine the sentiment of this group more fully.
Prior research reinforces the importance of patient-centred approaches to telehealth implementation.16,18 Our adaption of the TDFQ allows people who use mental health services to be activity engaged in their tele-mental health care delivery by directly assessing factors that are associated with their telehealth use. An important consideration for factor three ‘benefit and value’ is the significant negative correlation with age, indicating that younger people may value the benefit and value associated with telehealth use more than those of older ages. Importantly, this telehealth adaption of the TDFQ was developed in the post-COVID-19 pandemic landscape, making it a timely and appropriate tool for inclusion in tele-mental health research and clinical implementation.
It is important to acknowledge that this study did not include measures of social inclusion or socioeconomic status. This represents a significant limitation, since people who experience social exclusion across multiple domains report more mental health problems and additional barriers to accessing telehealth services. 37 In fact, responses to the open-ended questions in our survey suggested that some participants, such individuals from CALD backgrounds and First Nations people, encountered barriers to the use of telehealth that led to a sense of disempowerment. 10 While our sample included 21% First Nations representation, a proportion greater than the percentage of First Nations people living in the HNE region where the study was conducted (7.1%), the adaption was not designed for use among this population, and is thus unlikely to align with First Nations ways of knowing. 38 Additionally, while the HNE region of NSW is represented by a regional and rural population, the proportion of the sample living rurally is unknown. It is also important to note that this study used a specific definition of telehealth that did not include digital apps, websites, or other programs that offer mental health treatments and support asynchronously. Given the proliferation of digital mental health programs in recent years, exploring the utility of the TDFQ in this context is an important future direction.
Conclusion
To our knowledge, this is the first tool adapted from the TDFQ to measure factors associated with telehealth use among people who use mental health services in Australia. The resulting brief, easy to administer, and reliable self-report scale has the potential to address identified gaps in telehealth research including non-rigorous methodologies and a lack of patient-centredness. The scale has a coherent factor structure specific to the Australian tele-mental healthcare context, and with consideration of the scale's limitations, its practical use in research and clinical practice has the potential to address mental healthcare inaccessibility for many Australians. Future research should consider combining the TDFQ-telehealth adaption with theories of social justice and including non-digital and/or culturally aligned research methods to establish the scale's reliability and validity among older adults and populations who experience social exclusion, including those from lower SES, those who are CALD, and First Nations peoples. To further establish the scales psychometric validity, future research should also explore convergent and divergent validity, and test-retest reliability.
Footnotes
Acknowledgements
The authors would like to thank the research participants and the peer workers who supported them for their time and valuable contribution to this research. We would also like to thank Kate Simpson, Pam Davis, Fionna Murphy, Brendan Flynn, Luke Wolfenden, and Laura Wall for their contributions as collaborators on this project. Artificial intelligence (AI) was not used in the writing of this manuscript.
Author contributions
JW was involved in the project design and data collection, conducted the analysis and interpretation of the data, and drafted all sections of the manuscript. MH (project lead), and PB provided feedback throughout the interpretation and writing of the manuscript CT was involved in project design, data collection, and adaption of the questionnaire. RG supported data collection within mental health services. RC, CB, RW, and JR were involved in the expert review of the adapted questionnaire. FKL was involved in project design. All authors provided feedback and reviewed and approved the final manuscript.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Hunter Medical Research Institute (HMRI) Advanced Out of Hospital Care (AOHC) Telehealth Research Initiative (Grant ID number: G2011010).
Hunter Medical Research Institute, (grant number G2011010).
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.