
Abstract
Introduction
Mental health issues disproportionately affect rural and low-income populations, where access to prevention and treatment is limited. Implementing telemental health services (TMHS) in Federally Qualified Health Centers (FQHCs) could improve accessibility to mental healthcare. This study assessed the effect of TMHS on mental health services utilization in FQHCs, comparing centers with and without TMHS and examined differences in TMHS effect between FQHCs that adopted TMHS before and during the pandemic.
Methods
The study utilized FQHC-level data from Uniform Data Systems annual performance reports (N = 9540 FQHC-year) and county-level demographic, health status, and provider characteristic data from 2016 to 2022. A two-way fixed effects model was applied to examine the effect of TMHS on mental health visit rates, supplemented by the Sun and Abraham difference-in-differences estimator. The analysis included both pre-COVID and during-COVID TMHS adopters.
Results
FQHCs offering TMHS showed 1.04 times increase in overall mental health visit rates compared to those without TMHS. Centers serving higher proportions of Medicaid-insured (1.07 times) and low-income (below 200% FPL; 1.05 times) populations showed even higher visit rates. During-COVID TMHS adopters showed a significant increase (1.05 times), particularly in urban areas, whereas rural adopters did not see significant changes.
Conclusion
FQHCs offering TMHS showed increased mental health visit rates, especially among low-income and Medicaid-insured populations. FQHCs that adopted TMHS during the pandemic experienced a marked rise in mental health visits, but rural-urban disparities persist, highlighting the ongoing challenges in expanding access to mental healthcare in rural settings.
Introduction
In 2020, 21% of US adults reported having experienced mental illnesses. 1 The Centers for Disease Control and Prevention (CDC) shows that from August 2020 to February 2021, the percentage of adults suffering from anxiety or depression increased from 36.4% to 41.5%, and those reporting an unmet mental healthcare need increased from 9.2% to 11.7%. 2 Moreover, studies show significant mental health disparities based on income levels 3 and rurality. 4 Low-income populations are 1.5 to 3 times more likely to experience depression or anxiety compared to high-income populations. Rural residents experience higher rates of depression and are less likely to access mental health services than urban residents. 4 Despite effective prevention and treatment options to manage mental illnesses, the lack of accessible and affordable treatment resources remains a challenge. 5 Moreover, mental health resources are not uniformly distributed; consequently, rural and geographically isolated areas are underserved. 6 Relying on traditional modes of service delivery for mental healthcare may not meet the demand of people living in remote and underserved areas.
Telemental health services (TMHS) improve access and deliver cost-effective treatment while maintaining the quality of mental healthcare. Federally Qualified Health Centers (FQHCs) serve nearly 2.7 million patients seeking mental health services 7 and a disproportionate share of low-income families 8 who experience higher mental health problems and treatment disparities. 3 FQHCs are primary care clinics in the USA that receive federal funding to provide healthcare services in underserved communities, in areas designated as health professional shortage areas and must meet requirements, including providing care on a sliding fee scale for low-income patients. 9 Given the role of FQHCs as safety net primary care providers for low-income populations in urban and rural areas, 10 provision of TMHS in FQHCs could improve access for remote and underserved populations.6,11,12 However, lack of reimbursements, licensure requirements, privacy policies, and broadband gaps have historically made it challenging for FQHCs to offer TMHS.13,14 With the declaration of COVID-19 public health emergency on January 31, 2020 (ended on May 11, 2023), regulatory relaxations and changes like Medicaid and Medicare reimbursements for telemental health services, allowing audio-only telehealth and providing telehealth services without geographic/distant site restriction specific to FQHCs supported adoption of TMHS.13,15,16 However, most of these changes were temporary, and many of them are expected to expire by the end of 2024. Lawmakers are advocating for the continuation of these policies to maintain stable and ongoing telehealth services in FQHCs.
Our primary objective was to evaluate the effect of adopting TMHS on mental health service utilization in FQHCs to provide policy-relevant information on prolonging regulatory easing and boosting telehealth resources. Alongside, it is important to consider that the COVID-19 pandemic and subsequent PHE declaration led to state and federal telehealth policy relaxations that facilitated FQHCs to adopt and utilize telehealth to their full capabilities. 17 Besides, the heightened burden of mental health disorders during the pandemic could have contributed to increased utilization of mental health services. 18 To consider these pandemic-driven changes, our secondary objective was to examine if there are any differences in the effect of TMHS on mental health service utilization between FQHCs that adopted TMHS before the pandemic and those that adopted during the pandemic.
Methods
Measures and data sources
We used FQHC-level Uniform Data Systems (UDS) annual performance data from 2016 to 2022. 19 Our sample was an unbalanced panel including 9540 FQHC-year observations. Among other quality and clinical data, the UDS enquires about the types of telehealth services the clinic offers, including mental health services. We constructed our key predictor (treatment) variable, a binary variable indicating the availability of TMHS in a given FQHC. We focused on five utilization-related visit rate outcomes: (1) depression, (2) anxiety, (3) attention deficit and disruptive (ADD), (4) other mental disorders, and (5) all mental health (MH)—a composite of the above categories of mental health conditions (Supplementary Appendix 1). The visit rates (visits per patient) for each of these mental health conditions were calculated by dividing the total number of visits for a specific mental health diagnosis by the number of patients with that diagnosis. FQHC-level patient composition characteristics (e.g., age, sex, race, ethnicity, insurance, and poverty levels), and facility characteristics like rural-urban location, percentage of funding from community health center grants, and the number of delivery sites were included in the analysis as controls.
County socioeconomic covariates, including median income, unemployment, uninsured rates, rurality, and long commutes, were derived from Small Area Income and Poverty Estimates 20 and the American Community Survey. 21 County population health indicators like the percentage of people with frequent mental distress and the average number of poor physical health days were derived from the Behavioral Risk Factor Surveillance System. 22 Lastly, county provider characteristics like primary care provider ratio and mental health provider ratio) derived from Area Health Resource Files. 23 FQHC-level data was merged with county-level data by cross-walking the FQHC's ZIP code with the county using the Department of Housing and Urban Development ZIP Code Crosswalk Files. 24 As ZIP codes can cross county lines, we linked ZIP codes to the county in which the highest percent of the ZIP code was located.
Analytical methods
To assess our primary objective, we constructed a treatment variable “TMHS adopters” by classifying FQHCs offering TMHS as our treatment group (N = 5262) and those that did not offer it as the control group (N = 4278). To examine the effect of offering TMHS on mental health visit rate, we used a two-way fixed effects (TWFE) model with FQHC and year fixed effects (equation 1). We conducted a series of specification tests and evaluated empirical decisions before selecting TWFE as a suitable regression model (Supplementary Appendix 2).

VisitRates refers to the rate of MH visits (outcomes 1–5) in each FQHC. Subscripts i, c, and t refer to individual FQHC, county, and time in years from 2016 to 2022, respectively. The treatment variable, TMHS, equals 1 if an FQHC offered TMHS in a given year and 0 if it did not. The analysis includes control variables for patient demographics (DemoVars), FQHC organizational characteristics (OrgVars), and county-level factors (CountVars). Lastly, δ and Y are FQHC and year-fixed effects, and Є is a time-varying error representing unobserved factors that change over time that effect Y. The results of regression estimates are reported as Incidence Rate Ratios (IRR).
Additionally, considering that there are significant mental health utilization disparities based on income and rurality, we conducted subgroup analysis for urban and rural FQHCs and those with federal poverty level (FPL) below 200 with the same model specifications specified in equation (1).4,25 We also conducted subgroup analyses by insurance status, specifically for Medicaid and Uninsured categories which represent core FQHC populations. 26 For patient composition subgroups (FPL and insurance status), we selected the median as our standard cut-off point measurement as most groups showed skewed distribution, and the median is more resistant to outliers than the mean.
To assess our secondary objective, we constructed two treatment groups: (a) “pre-COVID TMHS adopters” defined as 1 if FQHC adopted TMHS before 2020 and “0” for those FQHCs that adopted on or after 2020 and those that did not adopt at all (treatment N = 3495; control N = 6064) and (b) “during-COVID TMHS adopters” defined as 1 if FQHCs adopted on or after 2020; and “0” for those that adopted before 2020 and those that did not adopt at all (treatment N = 2176; control N = 7383). We applied the same model described in equation (1) to estimate the effect of offering TMHS on mental health visit rates for both groups. Additionally, we looked at urban and rural FQHCs separately to examine if there are any differences in the treatment effects considering that there are substantial differences in telehealth adoption and its utilization based on rurality. 27
For all three treatments—TMHS adopters (not accounting for COVID effect), pre-COVID TMHS adopters, and during-COVID adopters—we applied the difference-in-differences (DiD) model using the Sun and Abraham estimator to evaluate the effect of providing TMHS on mental health visit rates over time. 28 This estimator is particularly useful when there is staggered treatment adoption which refers to a situation where the implementation of a treatment occurs at different times across different entities. FQHCs adopted TMHS in different years, and some did not adopt it at all.
In this approach, FQHCs that offered TMHS are grouped into cohorts based on the year they started providing the service. For each cohort, the average treatment effect on the treated (ATT) is estimated by comparing the visit rates of FQHCs that adopted TMHS at a specific time to those that never adopted TMHS (the counterfactual scenario). This is done in terms of the timing of treatment, focusing on relative differences between when the service was introduced and the observed outcomes (equation (2)). By analyzing outcomes relative to the time of adoption, this method avoids contamination from spillover effects from earlier periods, providing unbiased and consistent estimates of how offering TMHS affects visit rates for each cohort.
Results
Descriptive characteristics for the treatment “TMHS adopters” are summarized in Table 1. FQHCs that offered TMHS experienced 1.04 times increase in all MH visit rates compared to those without TMHS (Table 2). This increase was consistent across specific conditions such as depression, anxiety, and ADD. Urban FQHCs with TMHS showed higher visit rates for all MH (1.06 times), depression (1.07 times), and anxiety (1.07 times) when compared to urban centers without such services. In contrast, rural FQHCs offering TMHS did not show significant changes in visit rates, except for ADD, where visit rates were 1.06 times higher than rural centers without TMHS. In comparison to other FQHCs, FQHCs that offered TMHS serving a larger Medicaid population showed 1.07 times increase in all MH visit rates, consistent across different MH categories. Centers serving fewer uninsured individuals also noted a positive effect of TMHS, with increases in all MH (1.05 times) and depression-specific (1.06 times) visit rates. Additionally, FQHCs serving populations with incomes below 200% FPL exhibited higher visit rates (1.06 times) for depression, anxiety, and ADD.
Mean and standard deviation with significant tests for mental health visits, FQHC, and county-level characteristics among FQHCs that offered telemental health service (treatment group: n = 5262) and FQHC that do not offer telemental health service (control group: n = 4278) for all years (2016–2022 combined).
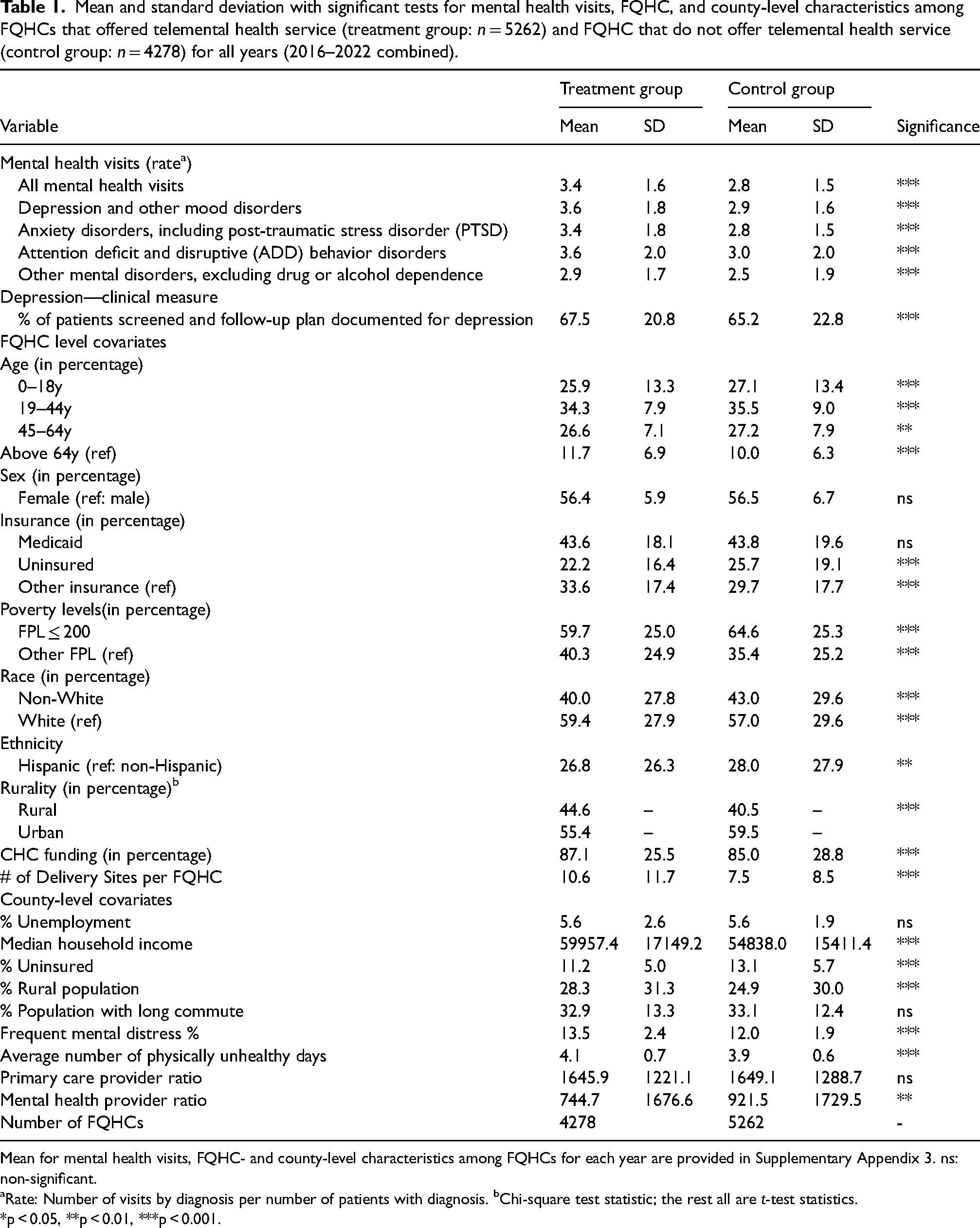
Mean for mental health visits, FQHC- and county-level characteristics among FQHCs for each year are provided in Supplementary Appendix 3. ns: non-significant.
aRate: Number of visits by diagnosis per number of patients with diagnosis. bChi-square test statistic; the rest all are t-test statistics.
*p < 0.05, **p < 0.01, ***p < 0.001.
Two-way fixed effects Poisson regression estimates of the association between telemental health service and mental health visit rate in all FQHCs and other subgroups of population served by FQHCs.
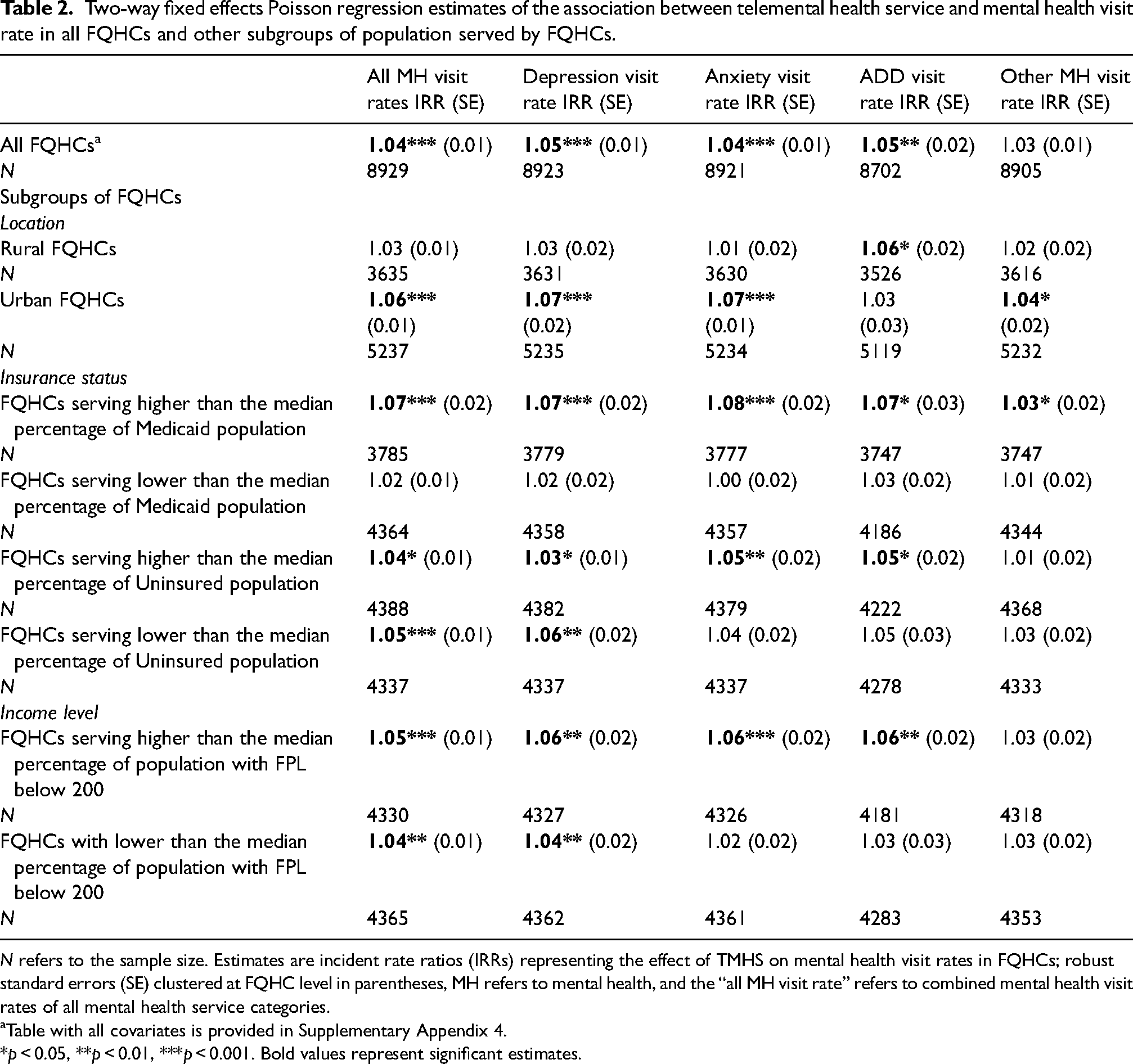
N refers to the sample size. Estimates are incident rate ratios (IRRs) representing the effect of TMHS on mental health visit rates in FQHCs; robust standard errors (SE) clustered at FQHC level in parentheses, MH refers to mental health, and the “all MH visit rate” refers to combined mental health visit rates of all mental health service categories.
Table with all covariates is provided in Supplementary Appendix 4.
*p < 0.05, **p < 0.01, ***p < 0.001. Bold values represent significant estimates.
Descriptive characteristics of pre-COVID TMHS adopters and during-COVID TMHS adopters are summarized in Table 3. For pre-COVID TMHS adopters, no significant effects on mental health visit rates were observed, these results were consistent across both rural and urban subgroups (Table 4). In contrast, during-COVID TMHS adopters showed significantly higher MH visit rates, with increases noted at 1.05 times for all MH visits combined and depression, and 1.06 times for anxiety and ADD visit rates. Urban FQHCs that adopted TMHS during the pandemic showed even greater increases, with visit rates being 1.09 times higher for all MH combined, depression, and anxiety, 1.07 for ADD, and 1.06 for other MH conditions. However, no significant effects were observed in rural counterparts during the same period. Further analysis using the same estimator but incorporating both pre- and during-COVID TMHS adopters as treatment covariates in a unified model, yielded similar results, validating the significant effect of TMHS on visit rates observed primarily among urban during-COVID adopters.
Mean and standard deviation with significant tests for mental health visits, FQHC, and county-level characteristics among FQHCs that offered TMHS pre-COVID (treatment = 3495; control = 6064) and FQHCs that offered TMHS during COVID (treatment = 2176; control = 7383).
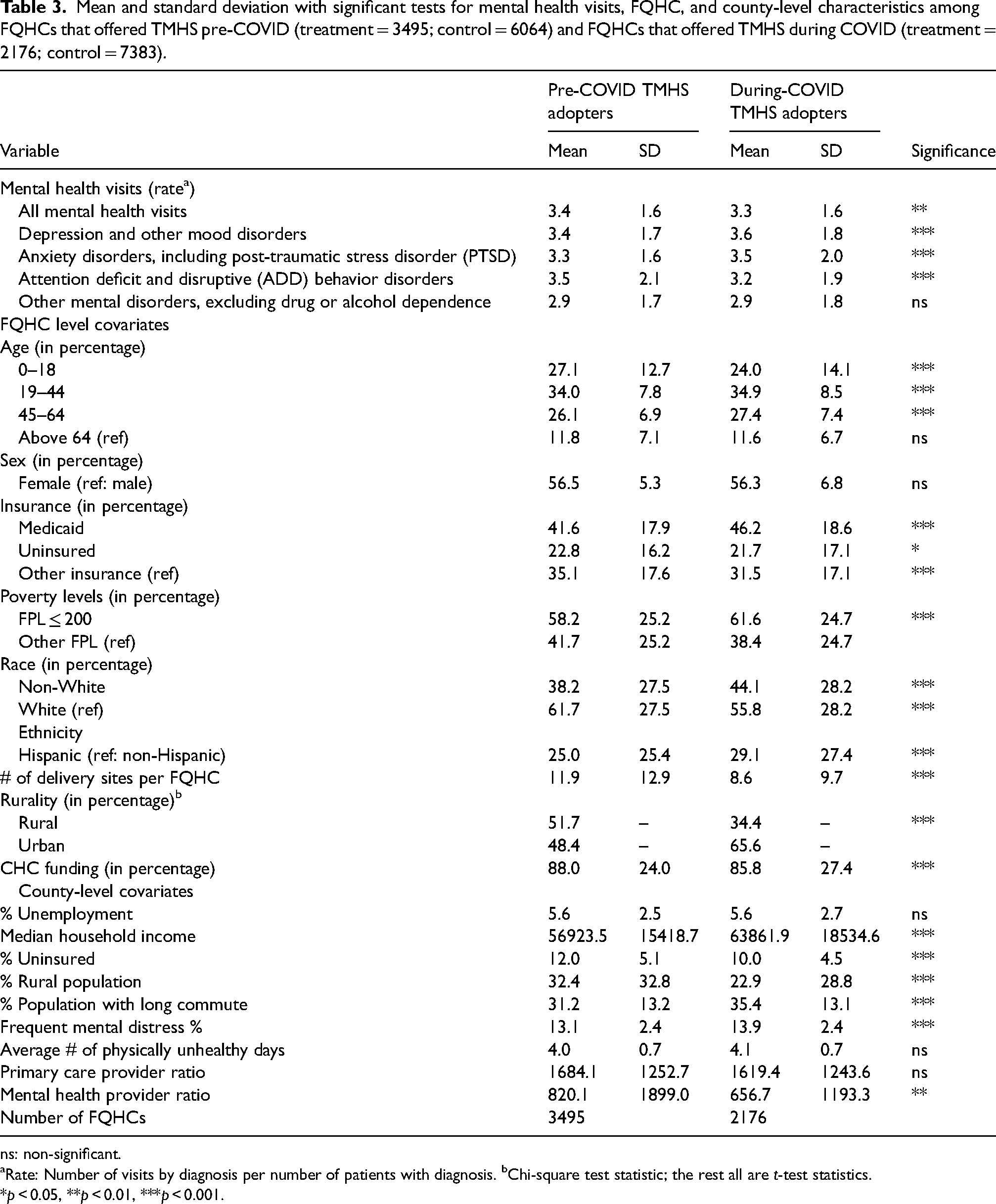
ns: non-significant.
aRate: Number of visits by diagnosis per number of patients with diagnosis. bChi-square test statistic; the rest all are t-test statistics.
*p < 0.05, **p < 0.01, ***p < 0.001.
Two-way fixed effects Poisson regression estimates of the association between telemental health service and mental health visit rate in FQHCs with treatment subgroups pre-COVID and during-COVID telemental health service (TMHS) adapters.
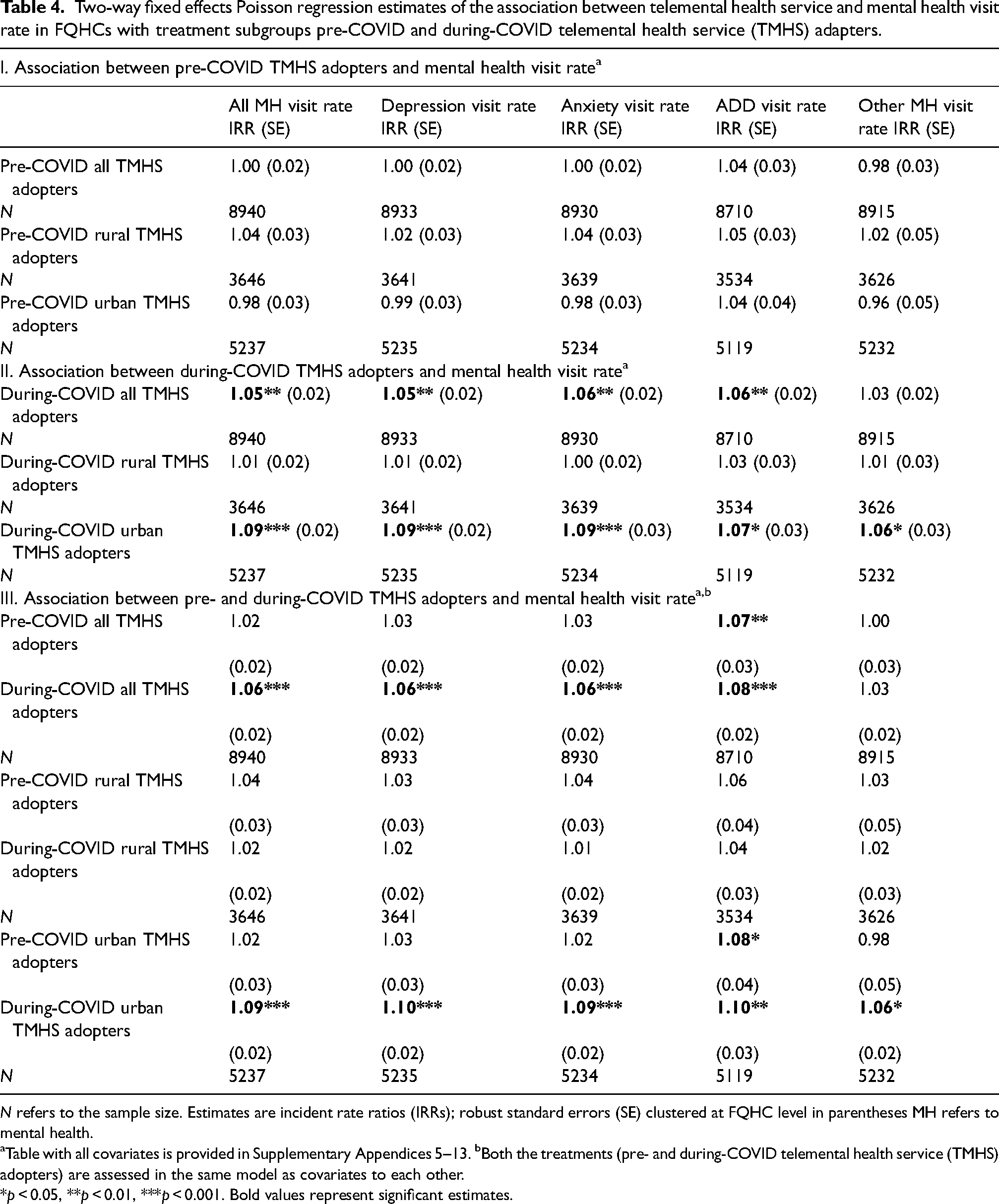
N refers to the sample size. Estimates are incident rate ratios (IRRs); robust standard errors (SE) clustered at FQHC level in parentheses MH refers to mental health.
aTable with all covariates is provided in Supplementary Appendices 5–13. bBoth the treatments (pre- and during-COVID telemental health service (TMHS) adopters) are assessed in the same model as covariates to each other.
*p < 0.05, **p < 0.01, ***p < 0.001. Bold values represent significant estimates.
The Sun and Abraham DiD estimator (equation (2)) findings, illustrated in Figure 1, showed a significant increase in all MH visit rates for the first four years following TMHS adoption in FQHCs, with a slight but still positively significant decrease in the fifth year compared to FQHCs that did not adopt TMHS (plot I). Both rural and urban TMHS adopters (depicted in plots II and III, respectively) demonstrated similar trends, with urban adopters experiencing a slightly larger effect. Notably, urban adopters showed non-significant effects of TMHS in the years prior to adoption, followed by a significant increase in the years after adopting TMHS. Consistent with the results from the TWFE Poisson estimator (equation (1)), pre-COVID adopters, including their urban and rural subgroups (shown in plots IV–VI), did not exhibit a significant effect of TMHS on all MH visit rates overtime. During-COVID adopters experienced a significant increase in overall mental health visit rates in the first year following adoption, with a slight reduction in the magnitude of this effect during the second year (plot VII). This effect was more pronounced in urban during-COVID adopters (plot IX), unlike rural during-COVID that showed no effect. Similar patterns were observed for depression, anxiety, ADD, and other mental health visit rates, provided in Figures 1–4 in Supplementary Appendix 14.
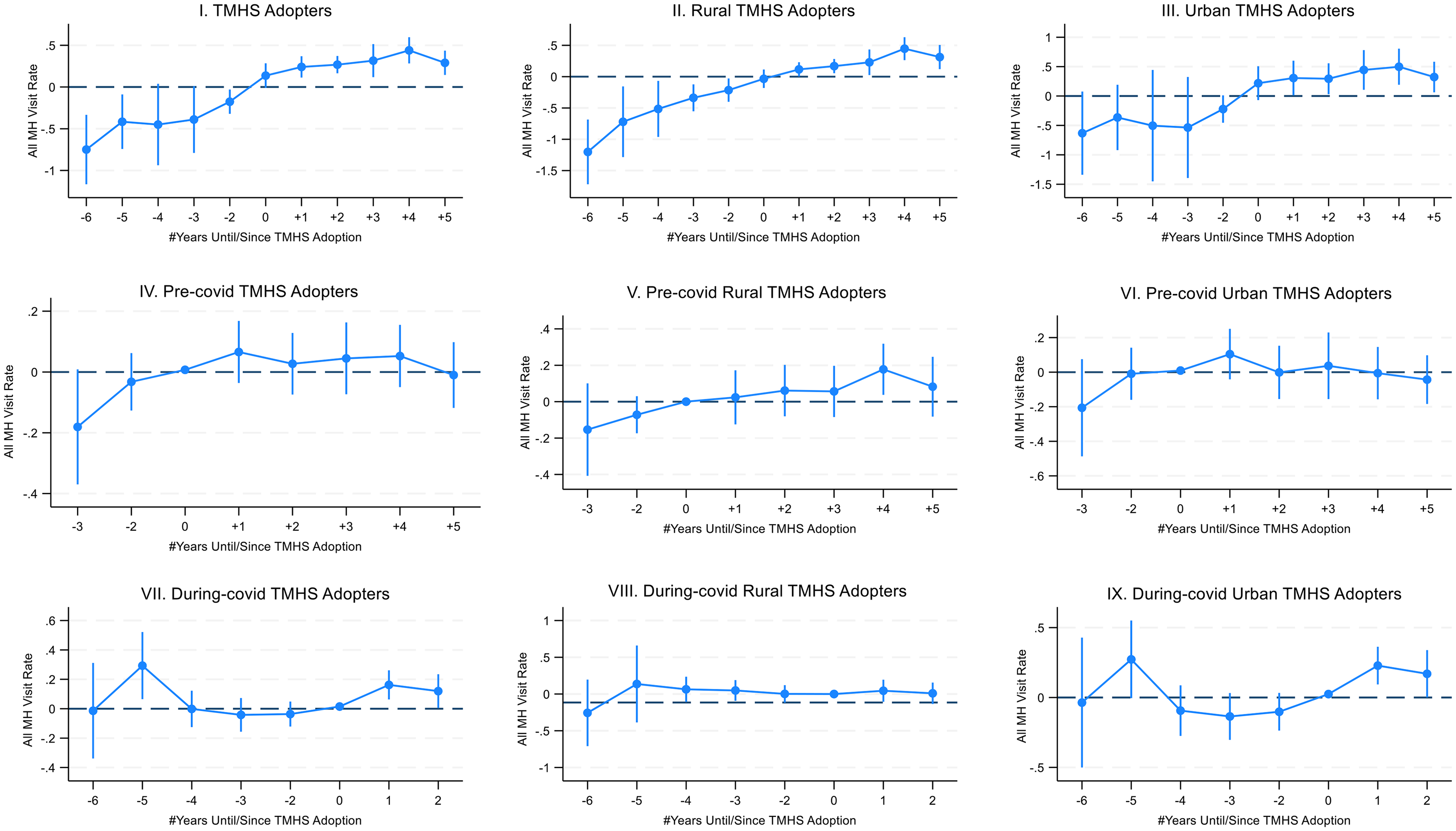
Sun and Abraham difference-in-differences estimator event study plots of the effects of telemental health service (TMHS) on all mental health (MH) visit rate. All MH visit rates refer to combined mental health visit rates of all mental health service categories. Plots contain estimates and 95% confidence intervals of the effects of TMHS from the estimation of equation (2). The reference time (0) was the year when TMHS was adopted by a given FQHC. Years before or after relative to TMHS adoption are expressed as leads (negative values) and lags (positive values) on the x-axis of the graph. All the plots (I–IX) use the same specifications as equation 2. Sun and Abraham estimators for other mental health visit outcomes (depression, anxiety, ADD, and other mental health visit rates) are provided in Figures 1–4 in Supplementary Appendix 14, respectively.
Discussion
In this study, we examined the effect of offering TMHS on mental health visit rates in FQHCs and differences in the effect of TMHS on visit rates between FQHCs that adopted it before the pandemic and those that adopted it during the pandemic. We found that FQHCs providing TMHS showed significantly higher rates of mental health visits overall, particularly for depression and anxiety, compared to FQHCs without such services. These findings highlight the critical role of TMHS in supporting underserved and vulnerable populations with mental health conditions. Our results are consistent with previous studies that noted a positive effect of telehealth availability on mental health visit rates at select FQHCs.29,30
The Sun and Abraham event study estimator that evaluated the effect of TMHS overtime showed a significant effect of THMS only among during-COVID adopters, no effect was observed in the pre-COVID adopters. The pandemic-related relaxations of telehealth policies specific to FQHCs like provision of reimbursements for TMHS, allowing audio-only telehealth and providing telehealth services without geographic/distant site restriction that supported them to offer TMHS, and increased funding to FQHCs to support them in providing telehealth services. 31 Prior research highlights how these changes reduced barriers, fostering broader adoption and utilization of telehealth. 32 Since all FQHCs were subjected to the same policy relaxations, one would expect an increase in mental health visit rates across both pre-COVID and during-COVID adopters after 2020. However, we saw a positive effect only in during-COVID adopters.
A possible explanation is that FQHCs adopting TMHS during the pandemic could set up a robust telehealth infrastructure, benefitting from increased funding to support their efforts to establish telehealth services compared to those that were already offering it. 33 Additionally, during-COVID adopters served a significantly higher population of low-income and Medicaid-insured populations compared to pre-COVID adopters. This demographic difference might explain the greater effect of TMHS in these centers, as reflected in our subgroup analysis which suggests that FQHCs serving higher populations of Medicaid and low-income individuals experience more significant benefits from TMHS. Enhanced Medicaid reimbursement policies, such as coverage for behavioral health services and parity for audio-only telehealth, likely facilitated this increased uptake and effectiveness of TMHS during the pandemic.13,34
The positive effect of TMHS in during-COVID adopters was more pronounced in urban FQHCs, and contrastingly no significant effect in their rural counterparts, highlighting urban-rural disparities in TMHS provision. Previous studies identified telehealth as a key strategy to overcome issues like the mental health professional shortages and distance barriers to a mental health center in rural areas.35,36 While telehealth has been identified as a crucial strategy, these populations still face challenges such as limited broadband access, low digital literacy, and reduced acceptance of telehealth, which can deter TMHS utilization.35,36 Telehealth interventions should address barriers in rural FQHCs, such as improving broadband connectivity, enhancing digital literacy, and increasing the cultural and practical acceptability of telehealth among rural communities. Such tailored strategies are vital for boosting the adoption of mental health services through telehealth in rural areas and reducing access disparities.
Limitations
First, the study analyzes data only from FQHCs and may not represent other healthcare settings. Second, the study included a period (2020–2022) when the pandemic heightened the burden of mental health disorders. Therefore, while interpreting the results, it is important to consider that the greater need for mental health services itself might have led to increased visits and not the presence of TMHS itself. Third, FQHCs that offer TMHS might have many in-house mental health services compared to those that do not offer. This could cause an important issue of confounding that is driving both the presence of TMHS and higher mental health visits. Lastly, to address endogeneity concerns, we lagged a few explanatory variables by one year, which led to the loss of the explanatory power of their effects on mental health utilization.
Conclusion
The study suggests that TMHS availability significantly increased mental health visit rates for conditions like depression and anxiety in FQHCs. Our findings reveal that FQHCs integrating TMHS during the pandemic saw a notable increase in visit rates. FQHCs serving higher populations of low-income and Medicaid individuals showed a greater effect of TMHS on visit rates, particularly those adopting TMHS during COVID, specifically indicating that they may have benefited from telehealth policy relaxations and associated expansion of telehealth services. The study also revealed significant rural-urban disparities: rural FQHCs adopting TMHS did not experience increased visit rates, unlike urban counterparts, despite a critical need for telehealth in rural areas to address mental healthcare gaps.
Supplemental Material
sj-docx-1-acr-10.1177_1357633X241307417 - Supplemental material for Effect of telemental health adoption on mental health services utilization in federally qualified health centers
Supplemental material, sj-docx-1-acr-10.1177_1357633X241307417 for Effect of telemental health adoption on mental health services utilization in federally qualified health centers by Khyathi Gadag, Kanika Arora and Whitney E Zahnd in Journal of Telemedicine and Telecare
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and informed consent statements
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available in the archived resources of the Uniform Data System (UDS) Training and Technical Assistance, Health Resources and Services Administration (HRSA)
19
[![]() ].
].
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.