
Abstract
Introduction
Telehealth may offer a valuable resource for family caregivers’ physical and psychological well-being; however, understanding its effectiveness is crucial to determining its true potential. Thus, this systematic review and meta-analysis aims to examine the effectiveness of telehealth interventions focused on family caregivers’ physical and psychological well-being, along with other factors during the care of older adults with various diseases (such as neurocognitive disorders, chronic conditions, and musculoskeletal diseases).
Methods
PubMed, Web of Science, Scopus, and Cochrane Library databases were searched. Studies that investigated the effects of telehealth on family caregivers of older adults with any disease and a comparison group receiving any type of intervention were selected. Two independent reviewers carried out the study selection and data extraction. We conducted a meta-analysis using standardized mean differences (SMDs) to pool the continuous outcomes included. Heterogeneity (I² and Tau²), publication bias (Egger's test and funnel plots), risk of bias (Joanna Briggs Institute tool), potential mediators (meta-regressions), and robustness (leave-one-out method) were also assessed.
Results
Twenty-six studies were selected (23 randomized controlled trial and 3 quasi-experimental studies), including a total of 2932 family caregivers. Telehealth was more effective than usual care in improving psychological well-being (SMD = 0.21; p = 0.006), caregiving competence (SMD, 0.73; p = 0.007), and reducing caregiver burden (SMD = −0.26; p = 0.01) in a follow-up shorter than 4 months. It was not effective in reducing anxiety or depression (SMD = −0.18 and −0.40; p = 0.08 and 0.20, respectively), nor in improving physical fitness (SMD = −0.16; p = 0.460). Considering a follow-up period of 4–12 months, the only outcome in favor of telehealth was the improvement in managing patients’ problematic behaviors (SMD = −1.27; p < 0.0001). It was not effective for psychological well-being, anxiety, depression, or caregiver burden (SMD = 0.15, 0.22, 0.08, and −0.33; p = 0.290, 0.260, 0.550, and 0.550, respectively).
Conclusion
Telehealth may be a valuable option for supporting family caregivers of older adults in improving psychological well-being, caregiving competence, and reducing burden, but the benefits may not last long term.
Keywords
Introduction
The global population of people aged 65 and older is expected to more than double, increasing from 761 million in 2021 to 1.6 billion by 2050. 1 This represents a significant challenge, especially regarding healthcare.1,2 Older adults experience various conditions related to aging 3 and more chronic diseases, 4 which increases the demand for continuous and prolonged care. 2 In Europe, 19% of the population over 65 years old requires a family caregiver to assist with Activities of Daily Living. 5 Family caregivers have become an essential part of healthcare for older adults during hospital admissions and in-home care. 6 Typically, family members of older adults, known as “informal caregivers” or “family caregivers” provide this care. They face a very challenging situation as most of them care for the older adults without adequate knowledge and skills or sufficient resources. 5
Caring for a relative can be a positive experience due to the motivation and satisfaction of staying close to the loved one. 7 However, it is important to highlight the adverse effects of caregiving on the physical and psychological health of family caregivers. 8 On the one hand, physical demands are particularly high when assisting individuals with reduced mobility or those requiring intensive care, as these situations often involve physically strenuous tasks such as transfers and mobilization. 9 On the other hand, the spent time to care their relative 10 and balancing caregiving responsibilities with professional, social, and familial roles11,12 may affect the mental health of caregivers increasing the risk of anxiety and depression. 13 These challenges can also contribute to a decline in psychological well-being by impacting key components of Carol Ryff's six-factor model, including self-acceptance, positive relationships with others, autonomy, environmental mastery, a sense of purpose and meaning in life, and personal growth and development. 14 These negative effects on psychological well-being, considered by the International Classification of Functioning, Disability and Health as quality of life, particularly when considering the subjective perspective of an individual's condition, 15 can increase the perceived burden of caregiving, ultimately impacting caregivers’ quality of life. 16 This is particularly concerning given that the caregiver's well-being can directly influence the physical and mental health of the care recipient.17,18
In response to this need, maintaining the health of family caregivers has received increasing attention from governments and healthcare providers. 1 Some studies have developed intervention programs specifically targeted at family caregivers, including psychological interventions, 19 education and support, 20 patient management workshops, 21 or training in coping skills and communication between the family member and the caregiver 22 with beneficial outcomes for caregivers’ health and well-being. However, the difficulty of leaving their family member alone in some cases, 23 and the family caregivers’ time restrictions 24 make it difficult for them to participate in in-person intervention programs.
In this context, telehealth understood as a service aimed at providing care through technologies such as videoconferencing, remote patient monitoring, or mobile applications has emerged as a viable option for delivering interventions remotely. 25 Researchers have explored various ways to use new technologies through different methods such as mobile applications, 26 websites, 27 telephone calls, and videoconferences. 28 To our knowledge, a review by Zhai et al. 29 is the most recent and comprehensive systematic review, examining 40 articles on telehealth for family caregivers of children, adults, and older adults. However, they provided a synthesis of narrative evidence rather than a quantitative analysis (e.g., meta-analysis), making it difficult to draw conclusions and report clinical recommendations on the effects of telehealth interventions for family caregivers. Additionally, their review included studies up to 2021, and telehealth has undergone significant growth in recent years. Thus, a 3-year update including meta-analysis, specifically focusing on older adults, is well justified.23,26
This systematic review and meta-analysis provides a significant contribution to the current scientific literature by systematically presenting and analyzing the existing evidence on telehealth interventions targeting family caregivers of older adults. The aim of this systematic review and meta-analysis is to determine the effects of telehealth interventions targeting family caregivers of older adults (aged 65 and above) with various diseases (such as neurocognitive disorders, chronic conditions, and musculoskeletal diseases) on their psychological well-being, depression, anxiety, self-reported physical fitness, caregiving competency, and caregiver burden, compared to any type of interventions, evaluated at both short-term follow-up (up to 12 weeks) and long-term follow-up (over 4 months).
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guided this review (Supplemental Material Tables S.7 and S.7a), 30 and the protocol was registered in advance in the PROSPERO database (ID: CRD42024513465).
Data sources and search strategy
PubMed, Web of Sciences, Scopus, and Cochrane library databases were searched up to January 5, 2024. The search strategy is available in Supplemental Material Table S.1 to be replicated. Additionally, a hand-search using the same search strategy was performed in Google Scholar, and reference lists of included studies were reviewed to find other potentially eligible studies.
Study selection
The following criteria determined the inclusion of the studies: 1) older adults (over 65 years old) with any disease with a family caregiver; 2) telerehabilitation, telehealth, or similar interventions conducted via smartphones, phones calls, tablets, or computer; 3) the inclusion of control groups receiving any type of intervention; 4) the inclusion of any clinical outcome related to the family caregivers; and 5) clinical trials including randomized control trials and quasi-experimental studies. The exclusion criteria were: 1) not original articles (e.g., letter to editor or reviews) and 2) grey literature (e.g., conference papers or meeting abstracts). Two researchers (M.O-.P. and E.M-.F.) independently performed the study selection process, and any discrepancy was resolved through discussions and consensus, with the mediation of a senior third investigator when necessary (P.M-.G.). The systematic review software Covidence (www.covidence.org; Veritas Health Innovation) was used in the study selection process.
Data extraction
For each study, we extracted the following information: 1) author's name, publication year, and country, 2) study design, 3) population the intervention was aimed at (i.e., family caregivers, older adults), 4) family caregivers information (i.e., sample size, women/men percentage, average age, most frequent relationship percentage), 5) older adults information (i.e., sample size, women/men percentage and average age), 6) type of disease of the person they were caring for, 7) studied outcomes (i.e., psychological well-being, depression, anxiety, self-reported physical fitness, caregiving competency, and caregiver burden), 8) assessment instruments used, 9) telehealth intervention type, 10) Intervention duration and follow-up, and 11) control intervention information. Two investigators (M.O-.P. and E.M-.F.) performed data extraction, and any discrepancy at the screening and data extraction stages was resolved by mutual discussion or arbitration by the senior investigator (P.M-.G.).
Risk of bias
The risk of bias was evaluated using the Joanna Briggs Institute Critical Appraisal Tool for Systematic Reviews checklists. They included 13 items for RCTs, but three were removed as not applicable to this review, and nine items for non-RCTs. Each item was rated on three possible responses: “yes” (criterion met), “no” (criterion not met), or “unclear.” Two investigators (M.O-.P. and M.M-.T.) individually analysed the risk of bias for each study, and any discrepancy was resolved by discussion with a third investigator (P.M-.G.).
Meta-Analysis
The means difference (telehealth intervention vs. control intervention) of continuous outcome variables after intervention was used to calculate the total effect size. The reported standard deviations were used, if not reported, were calculated using reported standard error (SE) or confidence intervals (CIs) as is described in the Cochrane Handbook for Systematic Reviews of Interventions (Chapter 10; Section 10.5.2). 31 Since the included studies had assessed the outcome measures using different scales (e.g., Zarit scale or Caregiver Strain Index to determine burden), we standardized the results to a uniform scale using standardized mean difference (SMD) to enable the pooling of data in the meta-analysis. The Higgins I2 statistic and p value were used to test the heterogeneity of included studies, which were classified as not important (0–40%), moderate (30–50%), substantial (50–75%), or considerable (75–100%). 32 A meta-analysis of the included studies was performed using either the random-effects or fixed-effects model, depending on whether substantial heterogeneity was found in the included studies, which was determined by the Tau-squared heterogeneity test. Each meta-analysis included an overall effect size and subgroup effect sizes according to the studied diseases (e.g., neurocognitive disorders, heart failure, or lung cancer).
Three sensitivity analyses were performed: (1) to test the robustness of the results, (2) to evaluate the presence of publication bias, and (3) to examine whether several potential mediators might influence the results of the meta-analyses. For the robustness analysis, studies were removed one at a time and we tested whether the overall effect size (i.e., z score and p value) was significantly modified in magnitude or direction. 33 The publication bias was assessed by a funnel plot and the Egger regression asymmetry test, using the small sample bias-corrected SMD (Hedges’ g) as the effect size metric. 34 It is noted that applying Egger's test to SMDs can lead to inflated false positive results because the SMD and SE are not independent. To address this issue, we used a modified version of the SE proposed by Pustejovsky and Rodgers. 35 The influence of potential mediators was analyzed via meta-regressions 36 including the following factors: publication year, type of intervention, intervention focus (patients only vs. patients and caregivers), delivery method, control intervention, sample size, average age, and percentage of women/men.
The meta-analysis was performed using the Review Manager Version 5.3 (The Nordic Cochrane Center, The Cochrane Collaboration, 2014, Copenhagen, Denmark), and the meta-regression with the RStudio statistical programme (version 1.4.1106, R Core Team 2020; R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org/) using the {meta} and {metafor} packages.37,38
Results
Study selection
The database search resulted in a total of 1627 articles of which 604 were duplicates. From 1039 nonduplicated articles, 972 were excluded after the first screening of title and abstract, and another 39 were further excluded after the full-text screening. Thus, 26 articles meeting the inclusion criteria were included in the systematic review, 17 of them with valid data to be included in the meta-analysis. Figure 1 summarizes the inclusion flowchart.
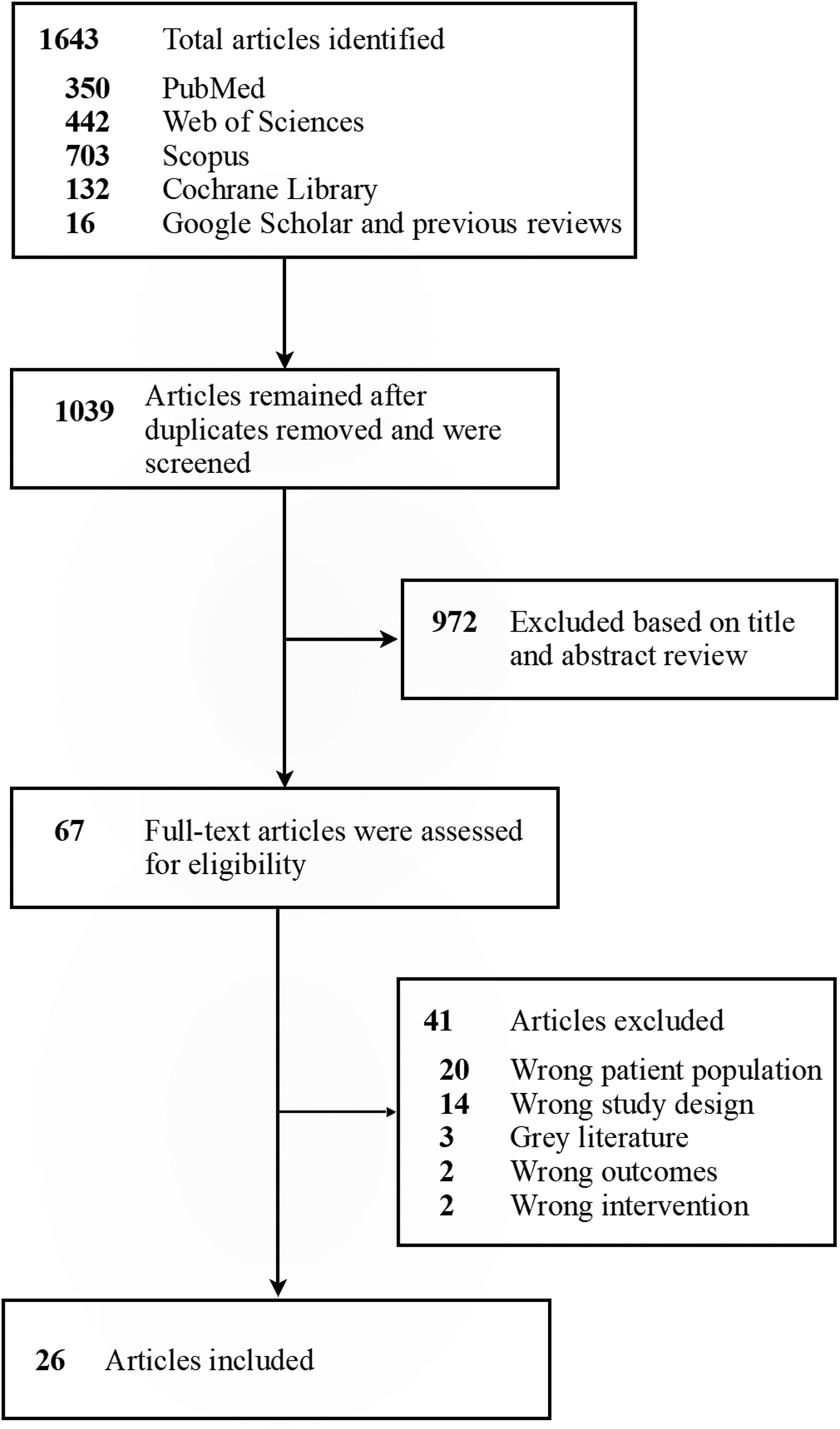
Flowchart of the systematic review process.
Characteristics of the included studies
Table 1 shows the main characteristics of the included studies. Of the 26 studies, 19 were RCTs,39–57 2 randomized pilot trial,58,59 1 randomized controlled feasibility trial, 60 1 cluster randomized trial, 61 and 3 non-RCTs.62–64 The whole sample size was 2932 family caregivers, with average ages ranging from 41 to 73 years. Approximately 72% of the participants were women (2 studies did not specify the sex of the participants).52,57 A total of 17 studies reported the caregiver–patient relationship; of these, 13 studies found that most of the caregivers were spouses39,40,42–44,46–50,56,59,63 and in 4 studies most of them were children of the patient.55,58,61,64 The diseases of the older adults receiving care were neurocognitive disorders in 17 studies39,40,43,45–50,53,54,56–58,61–63 (e.g., dementia or mild cognitive impairment), heart conditions in four studies,41,42,51,55 spinal cord injury in two studies,44,60 lung cancer in one study, 59 hip fracture in one study, 64 and fragility in one study. 52 Seven studies delivered their intervention through a website,39,40,43,46,48,60,64 five used telephone calls,42,54,55,57,59 nine utilized videoconferences,41,44,47,49,53,56,58,62,63 four employed mobile health (mHealth) applications,45,50,51,61 and one combined videoconferences and mHealth. 52 In 14 studies, the interventions were exclusively directed at family caregivers,39,40,42–44,46,48,49,54,56,60–63 while in 12 studies, they were directed at both older adults receiving care and family caregivers.41,45,47,50–53,55,57–59,64
Characteristics of 26 included studies.
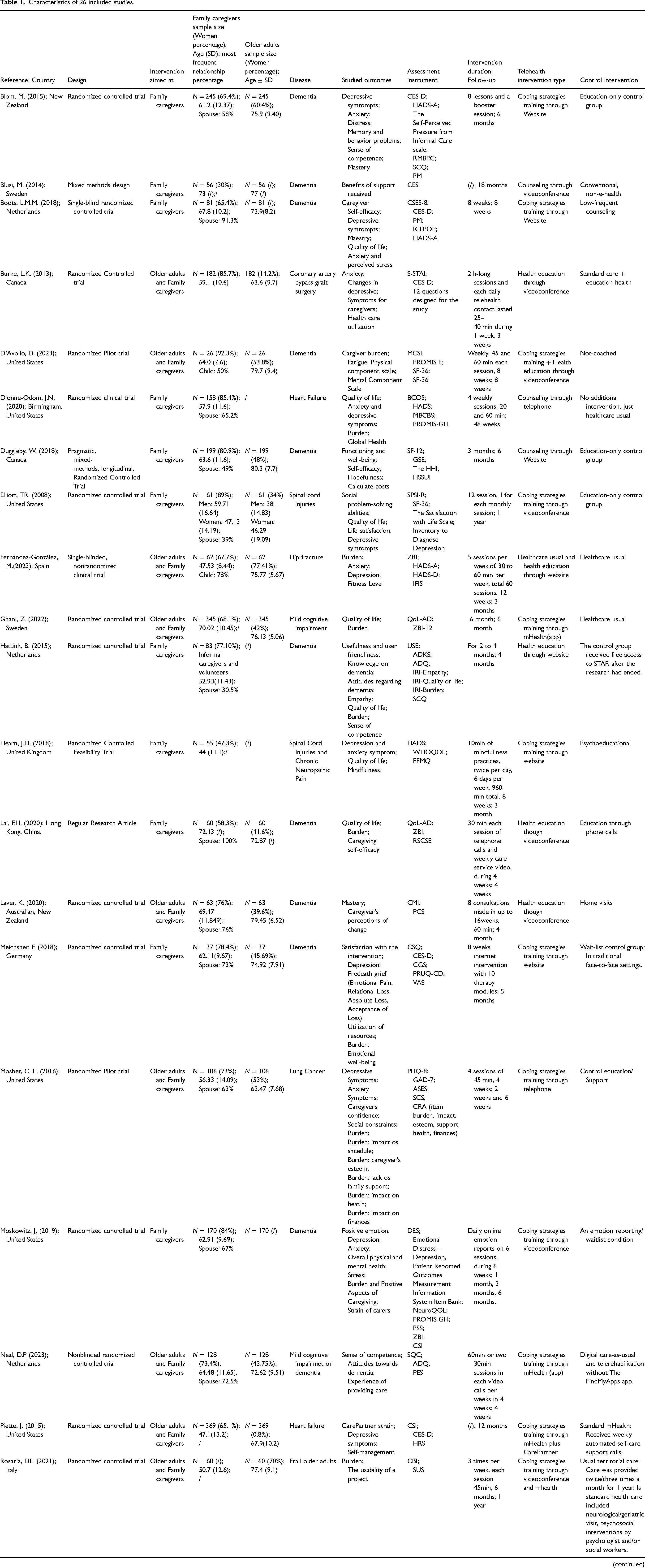
ADQ: The Approaches to Dementia Questionnaire; ADKS: Alzheimer's Disease Knowledge Scale; ASES: The Arthritis Self-Efficacy Scale; BDI-II: The BDI-II, Beck Depression Inventory II; BCOS: Bakas Caregiver Outcomes Scale; CAS-R: The Control Attitudes Scale-Revised; CBI: Caregiver Burden Inventory; CES: Care Effectiveness Scale; CES-D:Center for Epidemiologic Studies Depression Scale; CGS: The Caregiver Grief Scale; CSI: The Caregiver Strain Index; CMI: Caregiving Mastery Index; CRA: The Caregiver Reaction Assessment; CSQ: The Client Satisfaction Questionnaire; CSES (−8): Caregiver Self-Efficacy Scale; CES-D: The Depression Scale by the Spanish Center of Epidemiological Studies; CPD: Dysfunctional thoughts on caring; DASS: Depression, Anxiety and Stress Scales; DES: Differential Emotions Scale; DHFKS: The Dutch Heart Failure Knowledge Scale; EQ5D: EuroQol-5D; FFMQ: Five Facet Mindfulness Questionnaire; GAD-7: Generalized Anxiety Disorder seven-item Scale; GSE: The General Self-Efficacy Scale; HADS: Hospital Anxiety and Depression Scale; HADS-D: Item depression subscale of the Hospital Anxiety and Depression Scale; HADS-A:Item anxiety subscale of the Hospital Anxiety and Depression Scale; HSSUI: The Health and Social Services Utilization Inventory; HRS: The Health and Retirement Survey; ICEPOP: Investigation Choice Experiments for the Preferences of Older People; IFIS: The International Fitness Scale; IRI: The Interpersonal Reactivity Index; QoL-AD: Quality of Life-Alzheimer’s Disease; MAACL: The Multiple Affect Adjective Check List-Revised; MBCBS: Montgomery-Borgatta Caregiver Burden Scales; MBCL(-A,-B): Mindfulness-Based Compassionate Living; MCSI: The Modified Caregiver Strain Index; MDS: Minimun dataset (MDS-Caregiver); NPI-Q: Neuropsychiatric Inventory Questionnaire; NeuroQOL: Quality of Life in Neurological Disorders PES: Positive Experience Scale; PCS: The Perceived Change Scale; PHQ-8: The Patient Health Questionnaire-8; PHQ-9: Patient Health Questionnaire-9; PM: Pearlin Mastery Scale; PANAS: The Positive and Negative Affect Scale; PROMIS-GH: The PROMIS Global Health instrument; PROMIS F: The PROMIS fatigue. Promis adoption of the FACIT-fatigue; PRUQ-D: The Psychosocial Resource Utilization Questionnaire for Family Caregivers of People with Dementia; PSS: The Perceived Stress Scale; RMBPC: The Revised Memory and Behavioral Problem Checklist; RSCSE: The Revised Caregiving Self-Efficacy Scale; SCQ: Sense of Competence Questionnaire; SCS: Social constraints scale; SF-36: Short Form Health Survey; SF-12: 12 item Short Form Health Survey; SPSI-R: Social Problem-Solving Inventory-Revised; STAI: State-Trait Anxiety Inventory; SUS: Usability System Scale; The HHI: Herth Hope Index scores; USE: Usefulness, Satisfaction and Ease of use questionnaire; VAS: Visual analog scale ranging from 0 to 100; WHOQOL: World Health Organization Quality of Life Brief Scale; ZBI: The Zarit Burden interview; ZBI-12: The short form Zarit Burden Interview.
Lastly, Tables S.2, S.3, and S.4 of Supplemental Material show the risk of bias assessment. We noted some critical points within the included articles. In 12 studies (52%), the evaluators were blinded to the treatment assignment. In 16 studies (70%), the allocation to treatment groups was concealed. Furthermore, 18 studies (78%), provided information on per-protocol or intention-to-treat analysis and 20 studies (87%) used appropriate statistical analysis. All studies (100%), used true randomization for participant assignment, had similar treatment groups at baseline, measured outcomes in the same way in both treatment groups and measured the outcomes reliably and in the same manner for both treatment groups. The quasi-experimental studies generally demonstrated adequate quality. Two studies (67%) conducted pre- and postintervention outcome measurements and performed appropriate statistical analysis for this. In all studies (100%), the cause and effect were clear, the study participants were similar across comparison groups, completed participant follow-up, measured outcomes consistently across comparison groups, and did so reliably.
Effects of telehealth interventions on psychological well-being
A total of eleven trials evaluated the effects of telehealth interventions on family caregivers’ psychological well-being: seven in patients with neurocognitive disorders,40,45,46,48,49,58,63 two in patients with heart failure,42,55 and two in patients with spinal cord injuries.44,60 Considering all diseases together, we found more favorable results of telehealth interventions for improving psychological well-being (SMD, 0.21; 95% CI, 0.06–0.36; p = 0.006) of family caregivers. Regarding the subgroup results (neurocognitive disorders, spinal cord injuries, and heart failure), a trend favoring telehealth was observed in the three subgroups analyzed but these results were not significant in any disease subgroup. Funnel plot and Egger's test show potential evidence of publication bias. Results were robust, as statistical significance did not change after removing each study one by one. Meta-regression analysis did not demonstrate that any of the potential mediators influenced the results (all p > 0.05).
A total of five studies evaluated the changes in long-term follow-ups (from 4 months to 1 year), showing no better results for telehealth interventions in improving psychological well-being in informal family caregivers, neither in the overall analysis nor in the subgroup analyses of the different diseases. All these results are presented in Figure 2 and Supplemental Material, Figures S.1 and S.2, and Tables S.5 and S.6.
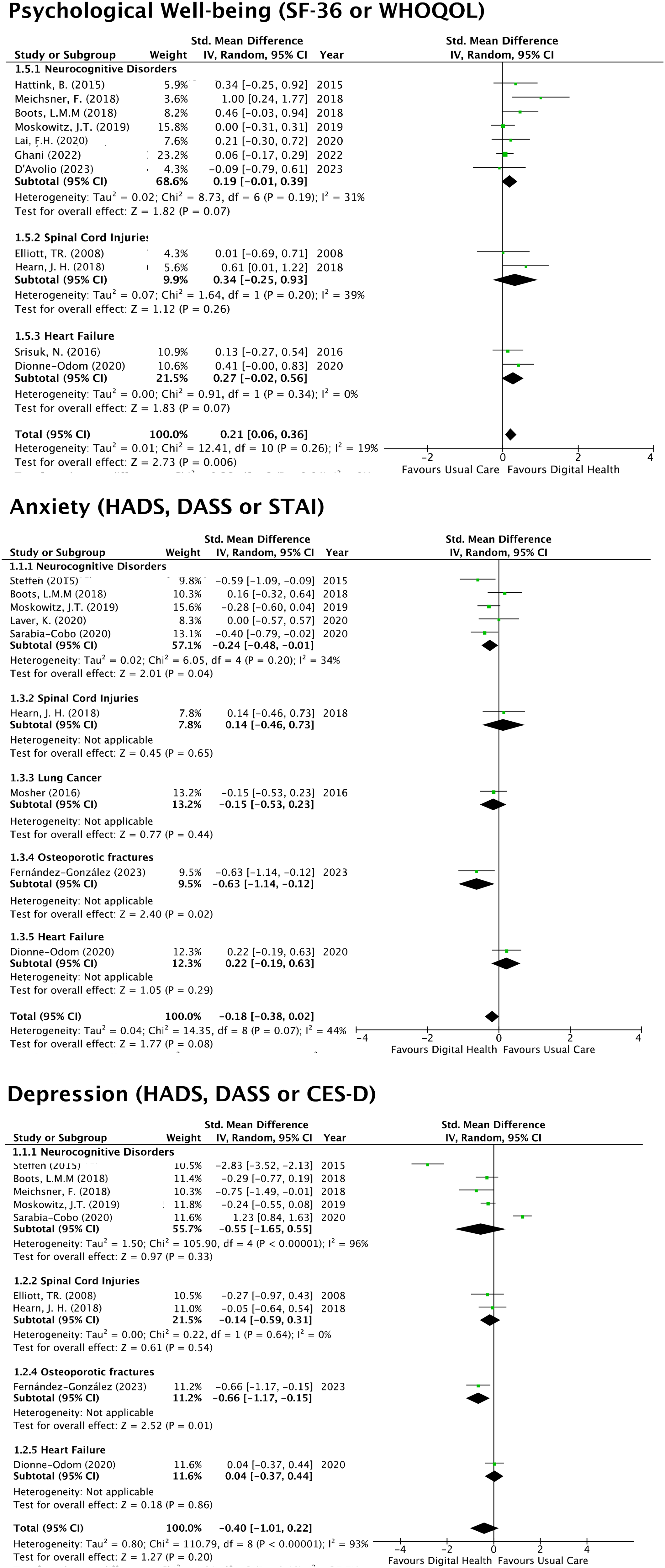
Pooled standardized mean difference for change in family caregivers’ psychological well-being, depression and anxiety outcomes at short-term follow-ups (up to 12 weeks). All analyses are divided by categories of diseases. CES-D: Center for Epidemiologic Studies Depression Scale; DASS: Depression, Anxiety and Stress Scales; HADS: Hospital Anxiety and Depression Scale; SF-36: Short Form Health Survey; STAI: State-Trait Anxiety Inventory; WHOQOL: World Health Organization Quality of Life Brief Scale.
Effects of telehealth interventions on anxiety and depression
Eleven trials evaluated the effects of telehealth interventions on family caregivers’ depression and anxiety: six on patients with neurocognitive disorders,40,47–49,54,56 one on patients with heart failure, 42 one on patients with lung cancer, 59 two on patients with spinal cord injuries,44,60 and one on patients with osteoporotic hip fractures. 64 Considering all diseases together, no significant results were found in favor of telehealth intervention for decreasing either anxiety or depression (SMD, −0.18 and −0.40; p = 0.08 and 0.20, respectively). In the neurocognitive disorders subgroup, significant results in favor of telehealth were observed for reducing anxiety (SMD, −0.24; p = 0.04). The results between groups were similar in long-term follow-ups (from 4 months to 1 year), showing no better results for telehealth interventions in reducing anxiety or depression in informal family caregivers in the overall analysis. Conversely, in the subgroup analyses of the different diseases, the neurocognitive disorders subgroup showed a favorable result toward control intervention in the depression outcomes at long-term follow-up (SMD, −0.56; p = 0.01). Funnel plot and Egger's test did not show any evidence of publication bias in depression but did in anxiety results. Results for anxiety were robust, as statistical significance did not change after removing each study one by one. However, the results for depression were not robust, as removing the Sarabia-Cobo 54 study made the results favorable to telehealth interventions. Meta-regression analysis showed that the type of telehealth intervention influenced depression results, with the greatest effect from counseling interventions, followed by coping strategies and health education (β = 0.98; p = 0.014). All these results are presented in Figure 2 and Supplemental Material, Figures S.1, S.2, and S.3, and Tables S.5 and S.6.
Effects of telehealth interventions on self-reported fitness
A total of six trials evaluated the effects of telehealth interventions on family caregivers’ physical fitness measures: three in patients with neurocognitive disorders,49,58,63 one in patients with heart failure, 55 and one in patients with osteoporotic hip fractures. 64 Considering all diseases together, we did not find more favorable results of telehealth intervention for increasing physical fitness measures of family caregivers (SMD, −0.16; p = 0.46). Funnel plot and Egger's test did not show any evidence of publication bias. Results were robust, as statistical significance did not change after removing each study one by one. Meta-regression analysis did not demonstrate that any of the potential mediators influenced the results (all p > 0.05). All these results are presented in Figure 3 and Supplemental Material, Figures S.2 and S.3, and Tables S.5 and S.6.
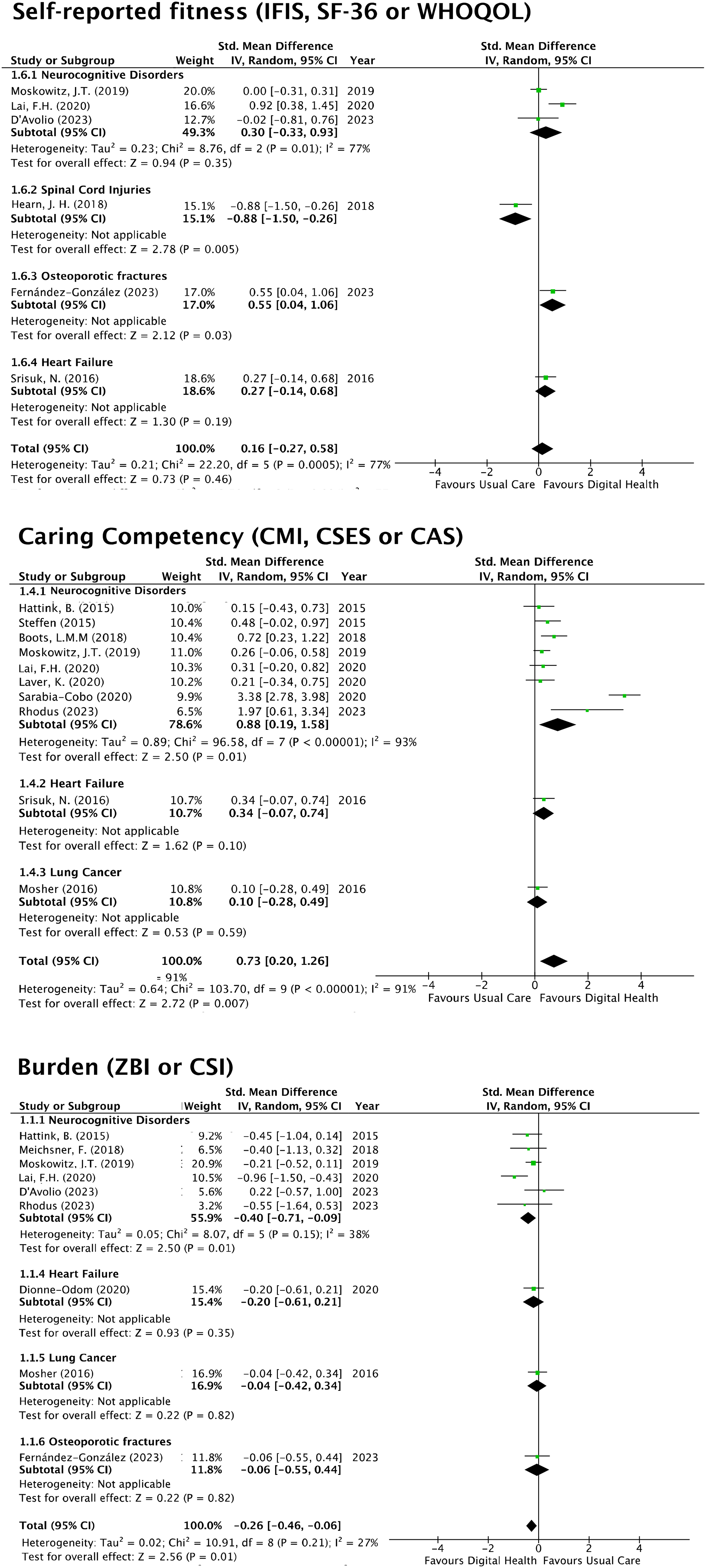
Pooled standardized mean difference for change in family caregivers’ self-reported fitness, caring competency, and burden outcomes at short-term follow-ups (up to 12 weeks). All analyses are divided by categories of diseases. CAS-R: The Control Attitudes Scale-Revised; CMI: Caregiving Mastery Index; CSES: Caregiver Self-Efficacy Scale; CSI: The Caregiver Strain Index; ISFIS: The International Fitness Scale; ZBI: The Zarit Burden interview.
Effects of telehealth interventions on caring competency and problematic behavior of the care patient
A total of 10 trials evaluated the effects of telehealth interventions on family caregivers’ caring competency: eight on patients with neurological disorders,40,46,47,49,53,54,56,63 one on patients with heart failure, 55 and one on patients with lung cancer. 59 Considering all diseases together, we found more favorable results of telehealth intervention for improving caring competency (SMD, 0.73; 95% CI, 0.20–1.26; p = 0.007). We only found sufficient studies for subgroup analyses in patients with neurocognitive disorders, and we also found more favorable results of telehealth intervention for improving caring competency (SMD, 0.88; 95% CI, 0.19–1.58; p = 0.01). Funnel plot and Egger's test did not show any evidence of publication bias. Results were robust, as statistical significance did not change after removing each study one by one. Meta-regression analysis did not demonstrate that any of the potential mediators influenced the results (all p > 0.05).
A total of three trials evaluated the long-term effects (from 4 months to 1 year) of telehealth interventions on problematic behavior of the care patient, all in patients with neurocognitive disorders.47,54,56 We found more favorable results of telehealth intervention for reducing behavioral issues of patients with neurological disorders (SMD, −1.27; 95% CI, −1.87 to −0.68; p < 0.0001). All these results are presented in Figure 3 and Supplemental Material, Figures S.1 and S.2, and Tables S.5 and S.6.
Effects of telehealth interventions on family caregiver’s burden
Ten trials evaluated the effects of telehealth interventions on caregiver burden: seven on patients with neurological disorders,45,46,48,49,53,58,63 one on patients with heart failure, 42 one on patients with lung cancer, 59 and one on patients after osteoporotic hip fractures. 64 We found no overall heterogeneity in subgroup analyses (I2 = 27%; p = 0.21). When considering all diseases together, telehealth interventions showed more favorable results in reducing caregiver burden (SMD, −0.26; 95% CI, −0.46 to −0.06; p = 0.01). The only subgroup with enough studies, patients with neurocognitive disorders, showed significant effects favoring telehealth interventions (SMD, −0.40; 95% CI, −0.71 to 0.09; p = 0.01). For long-term effects (4 months to 1 year), telehealth interventions did not show significant results in reducing caregiver burden (SMD, −0.33; 95% CI, −1.38 to −0.73; p = 0.055). Funnel plot and Egger's test did not show any evidence of publication bias. Results were robust, as statistical significance did not change after removing each study one by one. Meta-regression analysis did not demonstrate that any of the potential mediators influenced the results (all p > 0.05). All these results are presented in Figure 3 and Supplemental Material, Figures S.1 and S.2, and Tables S.5 and S.6.
Discussion
The results of this systematic review and meta-analysis could contribute to enhancing the knowledge of the effects of telehealth on family caregivers of older adults with various conditions, including neurocognitive disorders (e.g., dementia or mild cognitive impairment), osteoporotic hip fractures, heart failure, lung cancer, and spinal cord injuries. In turn, this could assist in decision-making regarding the implementation of telehealth interventions in clinical practice. Considering all the conditions included in the analysis, we found telehealth was more effective than usual care in improving psychological well-being, caregiving competence, and reducing caregiver burden in follow-up shorter than 4 months. Regarding the results on condition subgroups (neurocognitive disorder, spinal cord injuries, lung cancer, osteoporotic fractures, and heart failure), we found sufficient studies only in neurocognitive disorders. For these family caregivers, there was a greater reduction in anxiety and caregiver burden, as well as improvements in caregiving competence for those receiving a telehealth intervention. Furthermore, we found promising results in the subgroups of osteoporotic hip fractures and spinal cord injuries; however, there was not yet enough evidence to draw solid conclusions. The effects of telehealth interventions were less favorable in follow-up periods of 4–12 months. In longer-term follow-up, telehealth showed better results only for reducing behavioral issues in patients with neurological disorders but did not significantly improve caregiver well-being, anxiety/depression, or burden.
In most of the included studies, the caregivers were women, primarily spouses of the older adults. These results are not contradictory, as Zarzycki et al. suggest, since social and cultural norms in many countries assign women the responsibility of taking on the caregiver role. 65 In this context, it is essential to acknowledge that women are at a higher risk of experiencing caregiver burden, particularly when they are required to balance both employment and caregiving responsibilities. 66 These demands can have a detrimental impact on their physical and emotional health. 67 Therefore, it is crucial to design and tailor interventions based on the specific needs of caregivers.
The most commonly used format in the interventions was, first, videoconferences, followed by websites. These results align with those of other authors68,69 and could be explained by the relative simplicity of these systems. The use of intuitive and easy-to-use tools is a key factor, as some participants may have a low level of digital health literacy due to barriers such as lack of knowledge, unfamiliarity, or limited use of technological resources, especially among older persons. 70 Considering that the age range of caregivers in the studies included in this systematic review and meta-analysis was between 41 and 73 years, and that the family members they cared for were over 65 years old, it is likely that both older caregivers and patients had a low level of digital health literacy. Yuen et al. 71 concluded that higher levels of digital health literacy may be associated with better health outcomes. This may explain why the favorable results were not maintained in the long-term follow-up.
Digital health interventions for family caregivers have increased significantly in recent years, especially for family caregivers of patients with cancer or dementia.27,29,72–75 However, there is limited evidence regarding telehealth interventions for family caregivers of older adults, particularly in conditions other than neurocognitive disorders. Moreover, most of the above systematic reviews do not clarify whether the interventions are exclusively aimed at the family caregiver or at both the family caregiver and the older adult, 29 nor do they provide information about the age of the care recipients. 75 Similarly, meta-analyses in this field have predominantly focused on family caregivers of individuals with dementia, such as the studies by Zhao et al. and Leng. Our meta-analysis includes 17 studies and provides findings that contribute to expanding the scientific evidence by incorporating family caregivers of older adults with various health conditions, rather than focusing on a single condition. Additionally, this systematic review identified 14 studies targeting family caregivers, most involving patients with neurocognitive disorders such as dementia. Twelve studies included both older adults and their caregivers; half focused on neurocognitive conditions, while the others addressed diseases such as heart failure, lung cancer, osteoporotic fractures, and frailty. The emphasis on neurocognitive disorders may reflect the intensive, long-term care required, increasing caregiver burden, and the need for individualized support. 76 In contrast, conditions such as heart failure often allow patients to participate in their care and support their caregivers, enabling a mutually reinforcing dyadic relationship. 77 Accordingly, interventions may be designed to benefit both caregiver and patient. This finding may have important implications for clinical practice, particularly in guiding the objectives of interventions. On one hand, telehealth interventions tailored specifically for caregivers, according to Leng et al., 27 show better results in caregivers’ health. On the other hand, interventions targeting both patients and caregivers could improve their relationship and enhance the positive effects of the intervention 78 by considering the patient–caregiver relationship as an interconnected unit, where the well-being of one directly impacts the well-being of the other. 79
The results of our meta-analysis showed an improvement in the psychological well-being of family caregivers who received telehealth interventions. However, these results should be interpreted with caution, as none of the condition-specific subgroup analyses showed significant results in favor of telehealth. The study that demonstrated the best results in family caregivers’ psychological well-being was conducted by Meichsner et al. 48 who carried out coping strategy training interventions with a specific psychoeducation module. This finding coincides with Morgan et al. 80 who concluded that the most effective internet-based interventions for improving family caregivers’ psychological well-being are those that include psychosocial, psychoeducational, or psychotherapeutic aspects. However, the improvement on well-being was not maintained in long term, which reveals the need to analyze the above interventions in depth, particularly in terms of duration and content. Scientific evidence shows that the duration of interventions varies widely, ranging from a few weeks to several months. 81 Nevertheless, the effect of an intervention does not depend only on its duration but also significantly on its content and its incorporation into the caregiver's daily routine to achieve prolonged effects. 82 The interventions included in our meta-analysis focused on counseling, coping strategies, and health education, showing positive effects on the psychological well-being of family caregivers, but did not lead to improvements in anxiety or depression levels. The controversy of the effects of digital interventions on anxiety and depression of family caregivers has been reported in previous systematic reviews,27,74 showing medium to small beneficial effects, 83 or no significant differences between telehealth and conventional interventions. 28 The lack of evidence for telehealth in reducing anxiety and depression suggests it may be no more effective than alternative approaches.
We did not find significant results for the improvement of family caregivers’ self-reported fitness. This may be because the analyzed studies did not include interventions focused on their physical health, or because telehealth is no better than alternatives for improving this outcome. Most of the interventions designed for family caregivers were focused on psychological factors. Future research should include interventions that promote physical activity of family caregivers for several reasons. First, because physical activity has a positive effect on the overall and mental health of caregivers, as it can be a preventive approach for health problems and promote their well-being.84,85 Second, because telehealth can facilitate caregivers’ access to intervention programs designed to improve their physical condition. Third, telehealth interventions can be performed at home, which helps them to adopt physical activity routines and healthy lifestyles 86 during the limited free time they have. 24
Significant results were observed in favor of telehealth for improving caregiving competency, as the most common interventions were coping strategy training and health education. The only subgroup that showed significant results in favor of telehealth was neurocognitive disorders. These results are consistent with those demonstrated in the study by Leng et al. 27 which found that family caregivers of relatives with dementia improved their self-efficacy and knowledge in caring for their family member after receiving internet-based interventions. Similarly, in the overall analysis, we found significant results in favor of telehealth to reduce caregiver burden; however, significant results in favor of telehealth were only found in the neurocognitive disorders subgroup. These findings contradict the studies by Zhao et al. 74 and Li et al. 87 where no significant results were found for alleviating caregiver burden through telehealth. However, these investigations included a lower number of studies in their analysis. Favorable results on burden in our study could be explained by the relationship between psychological well-being, caregiving competency, and burden. Several authors have demonstrated that the acquisition of caregiving skills and perceived self-efficacy influence family caregivers’ burden and psychological well-being.88,89 Likewise, burden is a factor that influences family caregivers’ perception of well-being. 90
We found that the positive effects of telehealth in comparison to the control group on family caregivers’ outcomes (psychological well-being and caregiver burden) were not maintained after 4 months. However, the improvement in managing patients’ problematic behaviors in the telehealth group was achieved in long term. Our results support that telehealth interventions for family caregivers managing patients are more effective than usual care in the short term, but these favorable effects diminish in follow-ups of 4–12 months. Future interventions are needed to sustain the improvements in family caregivers’ outcomes over the long term. Some strategies would be: i) the inclusion of the contents of the intervention on the family caregivers’ routines, and ii) the provision of counseling in the long term to remember the healthy habits.
The clinical implications of our findings are significant, which support the benefits of telehealth for family caregivers of patients with various conditions—particularly within the first twelve weeks of intervention—should be interpreted with caution, as the majority of interventions have been conducted with caregivers of patients with neurocognitive disorders. Therefore, incorporating such interventions into healthcare services could improve access for family caregivers to care and resources, particularly those with transportation and mobility limitations. Most current evidence on telehealth effects for family caregivers of older adults comes from studies on neurocognitive disorders. 28 The evidence on the impact of telehealth on caregivers of older adults with cancer, spinal cord injuries, heart failure, frailty, and musculoskeletal diseases remains limited. Future research should focus on this population to expand knowledge in this field. Moreover, future studies should evaluate the effects of outcomes over a longer period due to the limited evidence in interventions beyond 16 weeks. Future interventions should also design strategies to maintain long-term results, including more comprehensive follow-up with family caregivers, progressively modifying interventions according to the evolution of the care recipient, or emphasizing the incorporation of the knowledge and skills learned into the caregivers’ habits and routines. In this context, future research should focus on two important aspects, first, intervention based on behavior change theories such as the stages of change model or the integrated theory of health behavior change, and use behavior change techniques (e.g., feedback on behavior, action planning, or habit formation). 91 Second, designing interventions focused on physical and psychological health, such as counseling, coping strategies, or health education. Additionally, these interventions should be adapted to the caregivers’ needs based on the care recipient's disease. For example, interventions focused on training in patient management to caregivers of older adults with mobility limitations 21 or those focused on managing behavioral changes for caregivers of older adults with neurocognitive disorders. 56
This study is not without limitations that need to be mentioned. First, the pooled effects reported in the meta-analysis come mainly from studies including family caregivers of patients with neurocognitive disorders, whereas there are fewer studies on other conditions such as osteoporotic hip fractures, lung cancer, heart failure, and spinal cord injury. Second, we found high heterogeneity in most analyses, likely due to the inclusion of family caregivers of older adults with various diseases and the use of different assessment scales. Third, while we generally found adequate quality in the included studies, we identified weaknesses mainly in the blinding of evaluators to treatment allocation and in the assignment to treatment groups, as well as in the reporting of per-protocol or intention-to-treat analysis. In contrast, this article has several strengths, including (i) the registration of the protocol in the Prospero database to add transparency and to reduce the likelihood of reporting bias; and (ii) the interpretation of results through the synthesis of quantitative evidence via meta-analysis to pool effect estimates, as well as sensitivity analysis (meta-regression, publication bias, and robustness). Future studies should improve blinding, the method of random assignment to treatment groups, and the reporting of statistical analyses performed.
Conclusion
The findings of this study highlight the short-term (up to 3 months) effectiveness of telehealth in improving the psychological well-being, caregiving competence, and burden of family caregivers of older adults with spinal cord injuries, heart failure, long cancer, and especially neurocognitive disorders. However, in follow-ups from 4 to 12 months, telehealth was only more effective in helping caregivers manage the problematic behaviors of care recipients, only in patients with neurocognitive disorders. These results should be interpreted with caution because most of the evidence comes from studies involving patients with neurocognitive disorders, so further research is needed to generalize these findings to other conditions such as cancer, spinal cord injuries, heart failure, or musculoskeletal disorders. Despite this limitation, our findings suggest that telehealth is a valuable option for supporting family caregivers. It is essential that telehealth interventions are tailored to the specific needs of caregivers based on the disease of the person they are caring for, and that strategies are developed to achieve and sustain positive long-term outcomes.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X251357054 - Supplemental material for Effectiveness of telehealth interventions for family caregivers of older adults with multiple diseases: A systematic review and meta-analysis
Supplemental material, sj-docx-1-jtt-10.1177_1357633X251357054 for Effectiveness of telehealth interventions for family caregivers of older adults with multiple diseases: A systematic review and meta-analysis by Mariana Ortiz-Piña, M Encarnación Martín-Franco, Pablo Molina-García, Rafael Prieto-Moreno, Marta Mora-Traverso, Trevor Russell and Patrocinio Ariza-Vega in Journal of Telemedicine and Telecare
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.