
Abstract
Introduction
Telepsychiatry has been widely adopted following changes to the Medicare Benefits Schedule (MBS) telehealth policy. This study aimed to examine the effect of telehealth policy changes on the out-of-pocket costs of MBS-subsidised psychiatric consultations.
Methods
We extracted records of relevant face-to-face, video, and telephone consultations from linked MBS claims data, Pharmaceutical Benefits Schedule data (2017–2023) and the 2021 Census data. For each consultation mode, we calculated the average monthly bulk-billing rate and average fee gap for non-bulk-billed consultations. Multivariate regression analyses were conducted to examine the determinants of bulk-billing and the fee gap.
Results
In total, 13,507,907 consultations involving 1,234,328 unique individuals were analysed. The average bulk-billing rate was 50.9%, decreasing over time. Fee gaps increased across all consultation modes. Face-to-face consultations were generally less likely to be bulk-billed and incurred higher fee gaps than other modes. Over successive policy periods, video consultations had an increasingly lower likelihood of bulk-billing and were associated with higher fee gaps. Patients in rural and remote areas were likely to bear greater out-of-pocket costs, including for video consultations. Attention Deficit Hyperactivity Disorder (ADHD) prescription-related consultations were associated with lower bulk-billing rates and higher fee gaps, especially in the video mode.
Discussion
While the expansion of telepsychiatry increased service availability, it did not consistently reduce the financial burden of psychiatric care, especially for rural and remote Australians. The higher out-of-pocket costs associated with ADHD prescription-related consultations warrant closer policy attention.
Keywords
Introduction
The health economic implications of telepsychiatry are increasingly important. Health equity, such as equality of utilisation and access, is a central aspect. 1 Medicare, the universal health insurance in Australia, subsidises the fee-for-service private healthcare sector. Providers may charge fees equal to the stipulated rebate amounts (‘bulk-bill’) or more than the Schedule fee, resulting in out-of-pocket payments or fee gaps for patients. 2 Higher out-of-pocket costs may hinder access to psychiatric care. 3 These costs may also vary by consultation mode despite identical reimbursements across modes. 4 A detailed longitudinal analysis would provide a clearer understanding of the out-of-pocket cost burden of Medicare-reimbursed telepsychiatry.
Telepsychiatry has a decades-long history in Australia, beginning with regional initiatives for rural and remote areas, followed by the introduction of video psychiatric consultations in the Medicare Benefits Schedule (MBS) in the early 2000s, the availability of which was mostly restricted to patients in rural and remote areas. 5 Among the telepsychiatry items was the incentivised Item 288, which provided additional reimbursements for bulk-billed consultations with rural and remote patients. In response to the COVID-19 pandemic, MBS telehealth (including telepsychiatry) items were expanded considerably in March 2020 (‘Telehealth expansion’) to ensure ongoing access to care while reducing risk of COVID infection. This policy expansion meant that telepsychiatry consultations were now eligible for MBS reimbursement nationwide and could be delivered by telephone as well as video.6,7 To consolidate MBS telehealth items, most new video items were made permanent in January 2022, with some telephone items phased out by June 2022 (‘Telehealth consolidation’). At the same time, older items designed for the pre-pandemic system, including Item 288, were removed. Subsequently, Item 294 was introduced in November 2022 to replace the role of Item 288 under the consolidated post-pandemic framework.7,8
MBS telepsychiatry consultations surged early in the pandemic. 9 Despite relaxed lockdown measures, high usage persisted and was more pronounced than telehealth in other medical disciplines. 10 The expanded availability of telepsychiatry may have improved access to care, enabling more consultations despite a decline in face-to-face consultations. 11 Telepsychiatry can be especially helpful in overcoming the rural psychiatrist shortage as a barrier to service delivery within the context of telehealth expansion and consolidation. 12
Using person-level linked data, our study aimed to analyse the trends of the out-of-pocket costs of MBS telepsychiatry (video and telephone) and face-to-face psychiatric consultations, and the effects of telehealth policies on them. We estimated the bulk-billing rates and fee gaps by consultation mode across telehealth policy periods, adjusting for relevant factors. These included consultation types, provider and patient locations, and patient sociodemographic characteristics. Additionally, there has been a surge in public interest in Attention Deficit Hyperactivity Disorder (ADHD), with rising psychostimulant prescription rates, particularly following the COVID-19 pandemic13–15 and one-off psychiatric assessments, particularly for video consultations. 16 The changing pattern in service provision and escalating demands for ADHD treatment may be interrelated and contribute to higher out-of-pocket costs in telepsychiatry.
Methods
Data sources and data linkage
We utilised the Person-Level Integrated Data Asset from the Australian Bureau of Statistics (ABS), incorporating three datasets: (1)
These person-level datasets underwent a deterministic linkage process using the ABS Person Linkage Spine, which uniquely matches records based on personally identifiable information (e.g. name, address, date of birth) to generate individual-level Spine identifiers. This process enabled the accurate merging of records across data sources. The selected MBS dataset initially contained 13,613,402 psychiatric consultations; after duplicate removal and data cleaning, 13,507,907 consultations remained. Linkage with the 2021 Census identified 1,234,328 unique individuals, resulting in 12,227,341 matched MBS consultations –a linkage rate of 90.5%. Additionally, 3,940,018 consultations (29.2%) were successfully linked to PBS records.
Variables and data preparation
Medicare Benefits Schedule data-derived variables
Psychiatric consultations were identified using the relevant MBS item numbers (Supplementary Table 1). We extracted the consultation date, consultation mode and category, bulk-billing status, fee charged, benefit paid, and provider postal areas (POAs). We identified and removed pairs of claimed and refunded records in the dataset. The two primary outcome measures were (a) the monthly bulk-billing rate by mode and (b) the average fee gap per consultation by mode.
POAs are geographic areas approximated from postcodes using one or more Statistical Areas Level 1 (SA1 s). 19 We matched provider POAs with five remoteness area (RA) categories of relative geographic remoteness: major cities, inner regional, outer regional, remote, and very remote areas. 20 For POAs with more than one remoteness category, we assigned the category with the largest POA-to-RA ratio. 21 Remoteness information was unavailable for 67,256 MBS records because the recorded POAs were for PO boxes, which were not included in the RA classification.
Census data-derived variables
Information from the 2021 Census for matched individuals included: age, sex, marital status, education level, with ‘University qualification’ for the Australian Qualification Framework (AQF) level 6 (bachelor's degree) and above, ‘Professional qualification’ for AQF level 3–6 (diploma, certificate III–IV, etc.), and ‘12 years or below’ for AQF level below 3, 22 and employment status classified into employed (full-time/part-time), unemployed, not in the labour force, and not applicable. Equivalised weekly household income was adjusted for household sizes and compositions. 23 Among the Socio-Economic Indexes for Areas (SEIFA), we used the area-based quintiles of the Index of Relative Socio-economic Advantage and Disadvantage, 24 which summarises the socio-economic conditions of people and households within an area.25,26
Pharmaceutical Benefits Schedule data-derived variables
All PBS records by psychiatrists were extracted using the specialty code. 27 Prescriptions in the ATC nervous system group were retained. They were divided into antipsychotics, antidepressants, anxiolytics/sedatives/hypnotics, ADHD drugs, and other psychotropics based on ATC codes (Supplementary Table 2). Prescriptions were matched with MBS records using unique identifiers, prescription dates, and consultation dates. We created a categorical variable for ADHD prescription status: ‘ADHD prescription’ if at least one ADHD drug was prescribed, ‘Other prescriptions’ for matched prescription records not including ADHD drugs, and ‘No prescription’ when no match was found in PBS data.
Additional variable
To account for the possible effects of provider competition, annual psychiatrist counts for local government areas (LGAs) from the Health Workforce Data Tool and LGA population estimates from the ABS were used to calculate per capita (per 10,000 population) psychiatrist counts, and then matched with patient POA (based on the 2021 POA-to-LGA correspondence) 21 and year.
Data analysis
Data management and analyses were conducted using STATA 18© (StataCorp LP, College Station, TX). We produced descriptive statistics for the linked Census records. We calculated and plotted the average monthly bulk-billing rates and average fee gaps of non-bulk-billed consultations by mode from pre-expansion (before March 2020), expansion (March 2020 to December 2021), to consolidation (January 2022 onward). Student's t-tests were used to compare fee gap differences across consultation modes and categories. For categorical data analyses, Pearson's chi-square tests were applied.
Our multivariate analyses comprised: (i) logistic regression models to examine the likelihood of bulk-billing; and (ii) fixed-effects panel regression models to analyse the determinants of fee gaps. Both models were adjusted for patient demographics, consultation modes, provider and patient remoteness, telehealth policy periods, per capita psychiatrists, and ADHD prescriptions. Interaction terms were included to assess how policy periods, patients’ geographic locations, and ADHD prescriptions moderated the effects of consultation mode on bulk-billing decisions and fee gaps.
Ethical considerations
This study received ethics approval from the Human Research Ethics Committee of the Australian National University (H/2024/0986).
Results
Descriptive statistics
Sociodemographic characteristics
Among individuals who utilised MBS psychiatric consultations, 85.3% were between 15 and 64 years old (Supplementary Table 3). There was a female preponderance (56.1%), and just over half were never married. Those with the highest educational attainment of Year 12 formed the largest group (37.6%). More than half were employed (full-time/part-time). One in three lived in the highest SEIFA quantile areas. Three-quarters resided in major cities, while just over one per cent lived in remote or very remote areas. There were noticeable differences in patient and provider characteristics across consultation modes.
Bulk-billing rates
The overall average monthly bulk-billing rate was 50.9% (Table 1). Video consultations had the highest bulk-billing rate (65.5%), followed by telephone consultations (59.5%). The bulk-billing rate for face-to-face consultations was slightly below one-third. Bulk-billing rates followed a bimodal distribution (highest in short and very long consultations). Pre-expansion, video consultations had considerably higher bulk-billing rates than face-to-face consultations (Figure 1). Most telehealth items were bulk-billed in the initial weeks of expansion, but bulk-billing rates declined progressively, especially for video consultations, until they became relatively stabilised during consolidation. Meanwhile, the face-to-face bulk-billing rates decreased steadily throughout the policy periods.
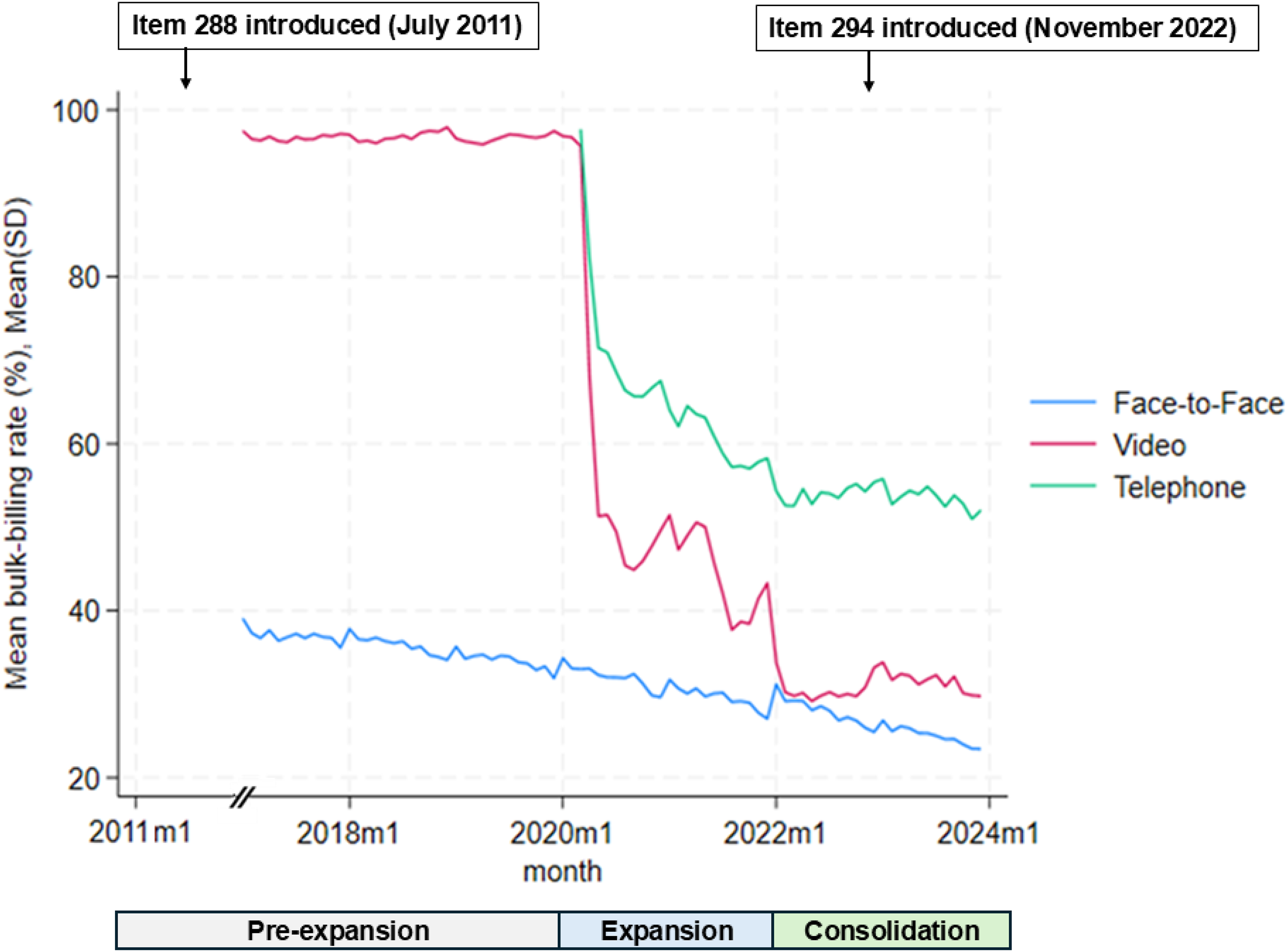
Monthly average bulk-billing rates of MBS psychiatric consultations by consultation modes (January 2017–December 2023). MBS: Medicare Benefits Schedule.
Mean monthly bulk-billing rate and SD of MBS psychiatric consultations by consultation modes, periods, and consultation types.
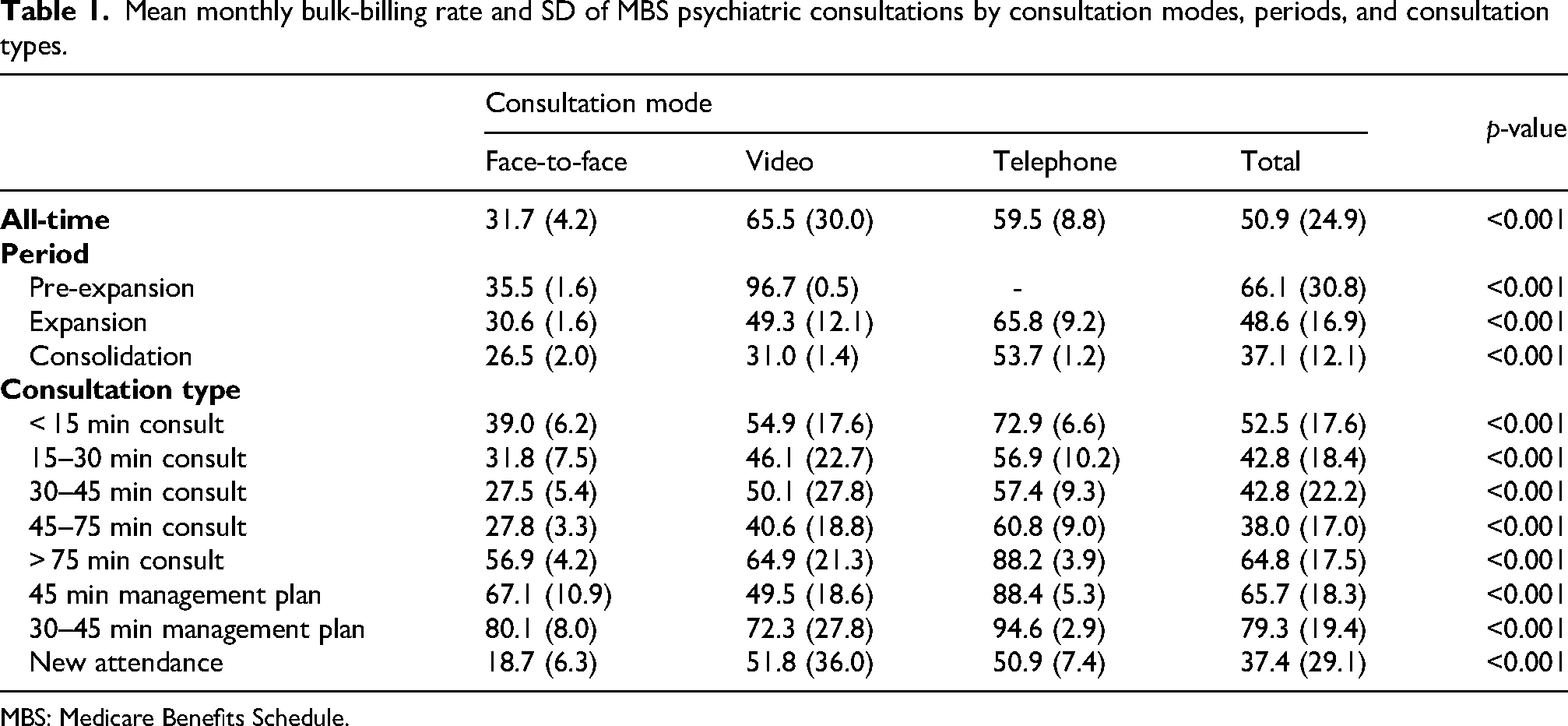
MBS: Medicare Benefits Schedule.
Fee gaps
Fee gaps increased across all consultation modes (Table 2). Telephone consultations have had the lowest fee gaps since their introduction. While video consultations were cheaper than face-to-face consultations before the telehealth expansion, they became more expensive afterwards (Figure 2). The differences in fee gaps across consultation modes became more pronounced during the consolidation period. A distinct annual pattern was observed: gaps decreased towards the end of each calendar year, likely due to the Medicare Safety Net reducing patient out-of-pocket costs (through additional reimbursements) after patients met their annual spending thresholds. 28
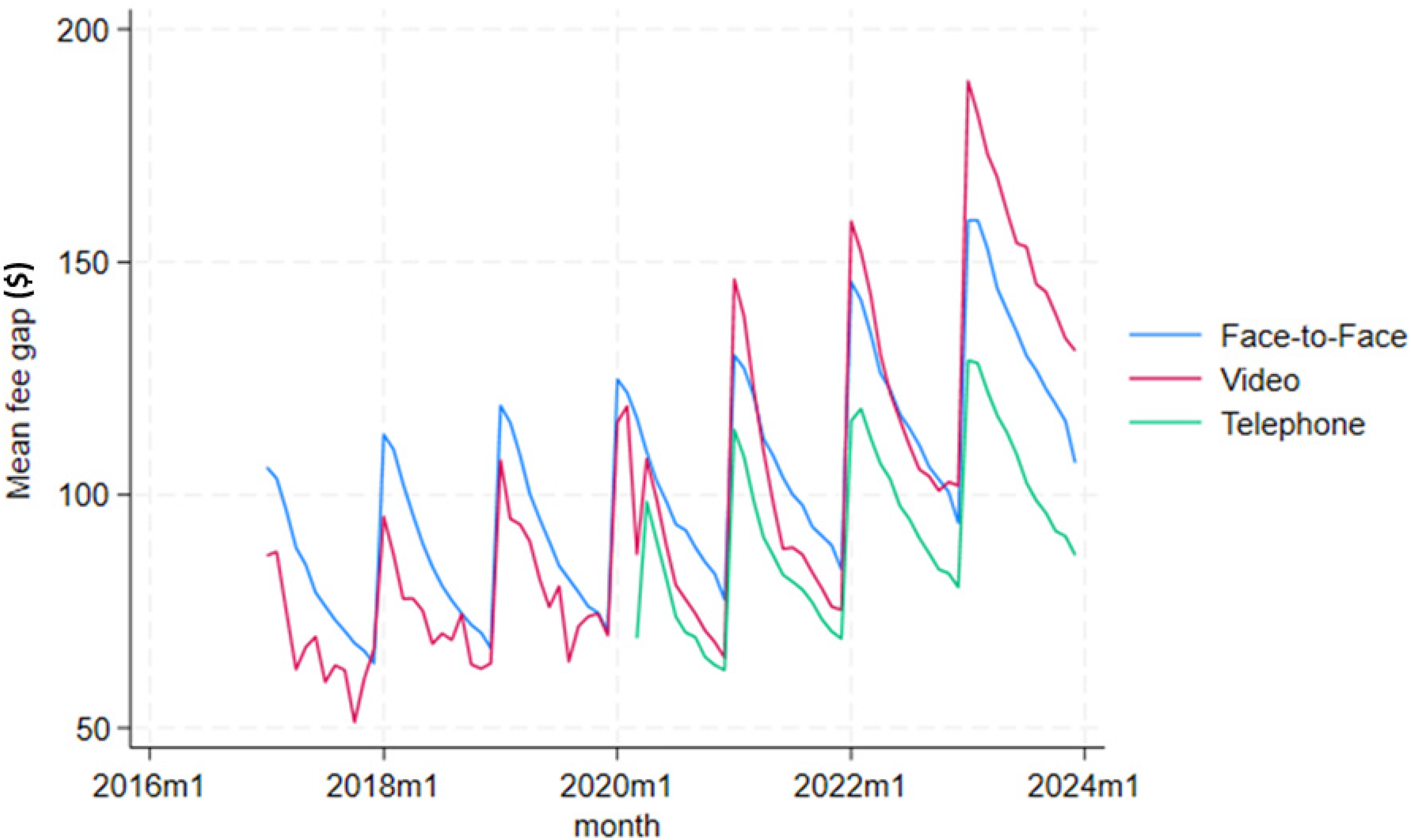
Monthly average fee gap per consultation of MBS psychiatric consultations by consultation modes (January 2017–December 2023). MBS: Medicare Benefits Schedule.
Fee gap differences ($$) of MBS psychiatric consultations by consultation modes, periods, and types.
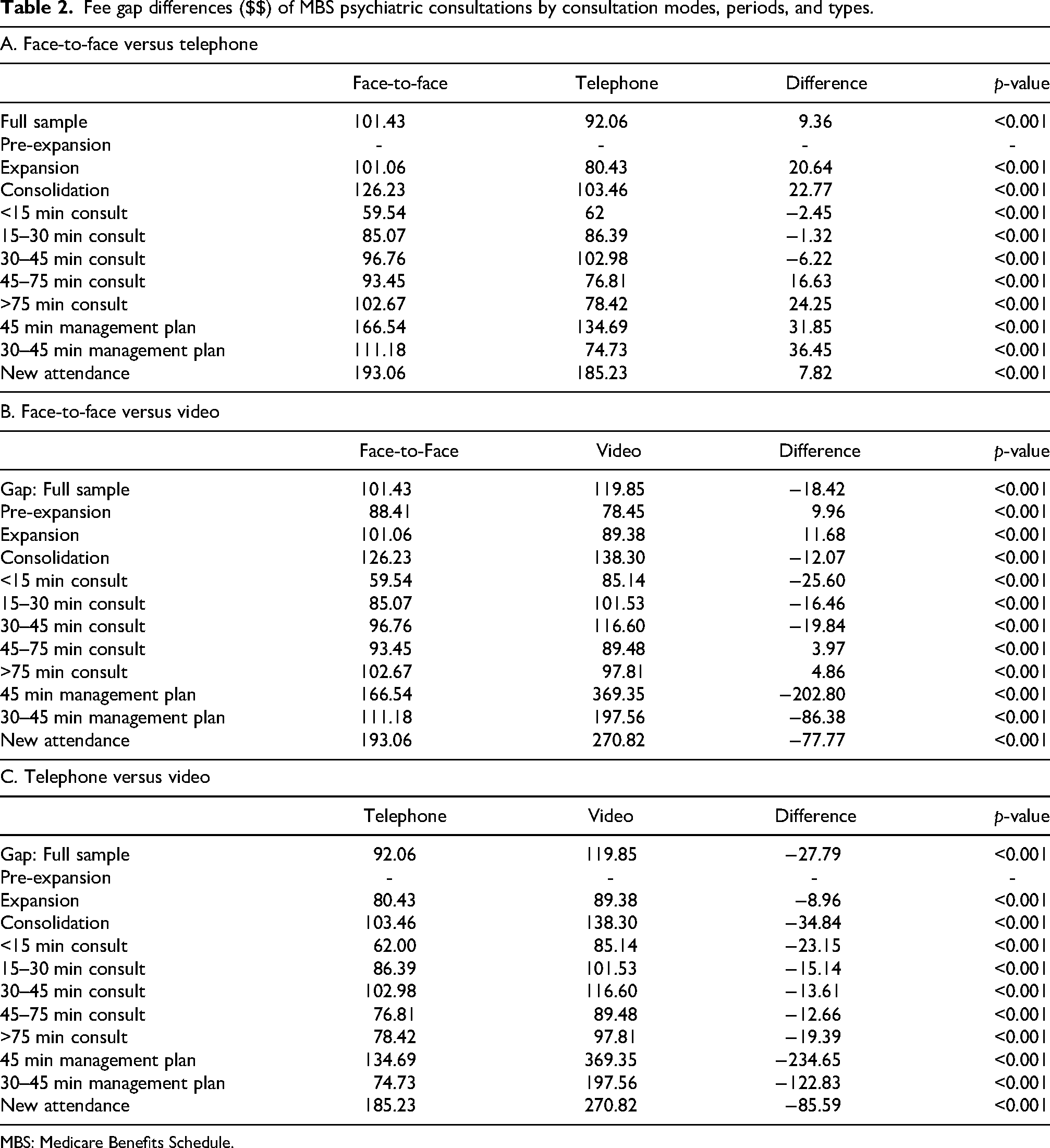
MBS: Medicare Benefits Schedule.
For very short and short consultations, face-to-face fee gaps differed little from telephone but were considerably higher in very long consultations and management plans (Panel A). Gaps for videoconferencing were significantly higher than face-to-face (+$$16 to +$$25) for consultations <45 min and doubled for management plans (Panel B). Telephone consultations were consistently cheaper than videoconferencing (Panel C).
Bulk-billing and gaps by other characteristics
Fee gaps were lower among patients ≥65 years, while males paid $$10 more than females despite similar bulk-billing rates. Gaps were lower among the widowed and higher among singles (Supplementary Table 4). The most socio-economically disadvantaged had the lowest gap and the highest bulk-billing rate (59.7%). Gaps were smallest in major cities and inner regional areas. The bulk-billing rate was highest for patients in outer regions but lower in very remote areas, where gaps were also higher. However, providers based in remote and very remote regions exhibited extremely high bulk-billing rates (>99%). ADHD-related prescription rates were associated with higher fee gaps and lower bulk-billing rates.
Regression analyses
Determinants of bulk-billing rates
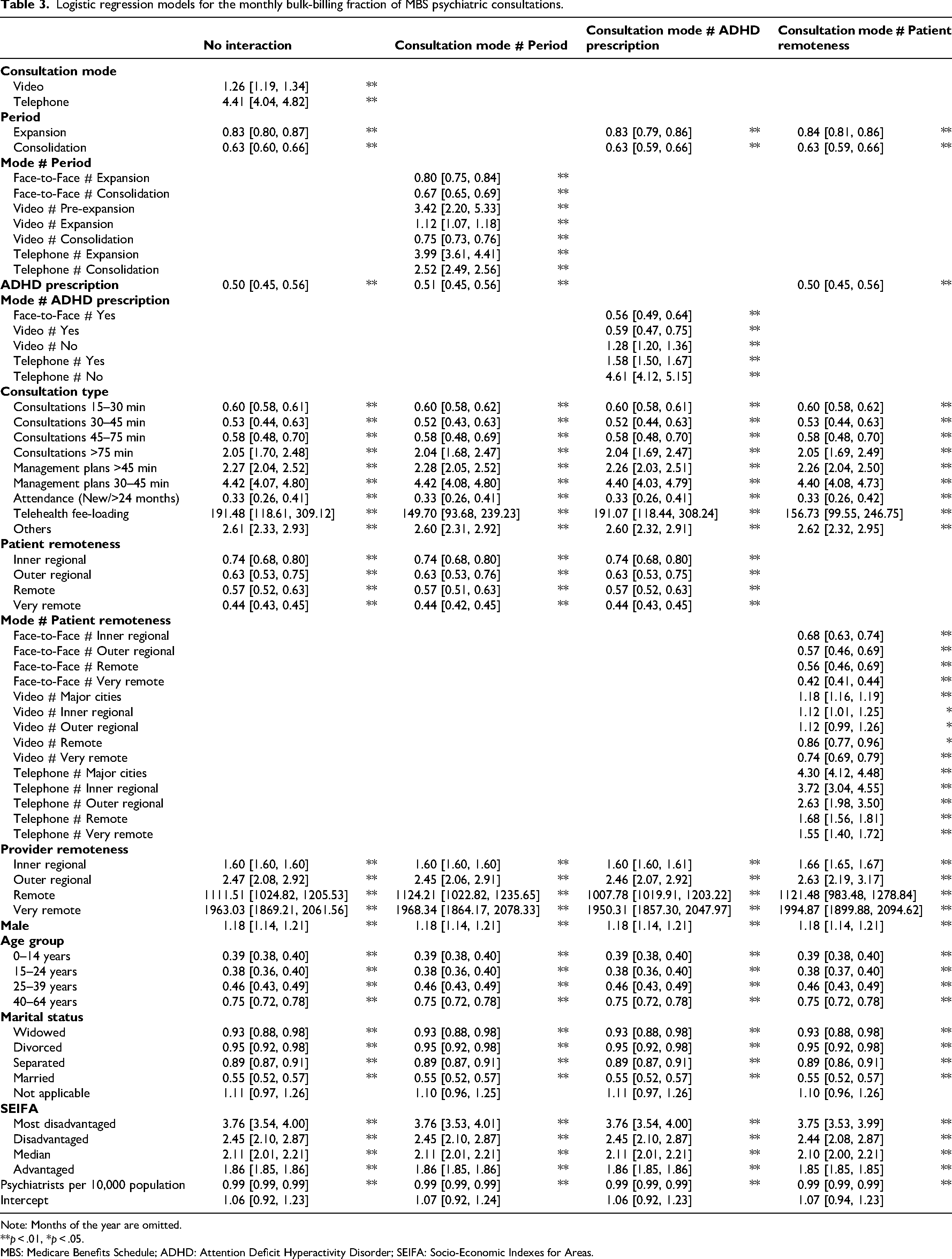
Overall, bulk-billing became significantly less likely during the telehealth expansion (Odds ratio [OR]: 0.83; 95% CI: 0.80, 0.86) and consolidation (OR: 0.63; 95% CI: 0.80, 0.66) (Table 3). Compared with pre-expansion face-to-face consultations, telephone consultations had higher odds of bulk-billing consistently in the expansion and consolidation periods (ORs: 2.52–3.99; p-values <0.01), while videoconferencing was more likely for bulk-billing during both pre-expansion (OR: 3.42; 95% CI: 2.20, 5.33) and expansion (OR: 1.12; 95% CI: 1.07, 1.18) but less likely during consolidation (OR: 0.75; 95% CI: 0.73, 0.76). Consequently, the likelihood of bulk-billing decreased more substantially for video consultations than for face-to-face consultations across subsequent telehealth policy periods.
Logistic regression models for the monthly bulk-billing fraction of MBS psychiatric consultations.
Note: Months of the year are omitted.
**p < .01, *p < .05.
MBS: Medicare Benefits Schedule; ADHD: Attention Deficit Hyperactivity Disorder; SEIFA: Socio-Economic Indexes for Areas.
Regular consultations (15–75 min) were less likely to be bulk-billed than those <15 min (ORs: 0.53–0.60, p-values <0.01). New attendances had the lowest odds of bulk-billing (OR: 0.33; 95% CI: 0.26, 0.41). Due to their inherent design, incentivised video items 288 and 294 were strongly associated with bulk-billing. Thus, the proportionately reduced usage of Item 288 since the introduction of new telehealth items likely contributed to falling video bulk-billing rates during the expansion phase (Figure 1), and the introduction of Item 294 might have helped to stablise video bulk-billing rates later on.
Non-metropolitan patients were less likely to be bulk-billed than metropolitan patients (ORs: 0.44–0.74; p-values <0.01). For video consultations, the likelihood of bulk-billing were higher in major cities and inner regions (ORs: 1.12–1.18; p-values vary from <0.01 to <0.05), but lower for remote and very remote areas (ORs: 0.75–0.87, p-values from <0.01 to <0.05), compared with face-to-face consultations for metropolitan patients. Providers in remote and very remote areas were extremely likely to bulk-bill (ORs: 111.51–1963.03; p-values <0.01). Males, the elderly, singles, and the less advantaged SEIFA quintiles were more likely to be bulk-billed. Per capita psychiatrist count was associated with minimally reduced bulk-billing rates (0.99; 95% CI: 0.99, 0.99).
ADHD prescription-related consultations were less likely to be bulk-billed. The OR for bulk-billing with ADHD prescriptions was 0.50 (95% CI: 0.45, 0.56) – indicating a 50% reduction in the likelihood compared to consultations without ADHD prescriptions. The likelihood of bulk-billing was lower for face-to-face (0.56; 95% CI: 0.49, 0.64) and video consultations (0.59; 95% CI: 0.47, 0.75) involving ADHD prescriptions compared with face-to-face consultations without such prescriptions.
Determinants of fee gaps
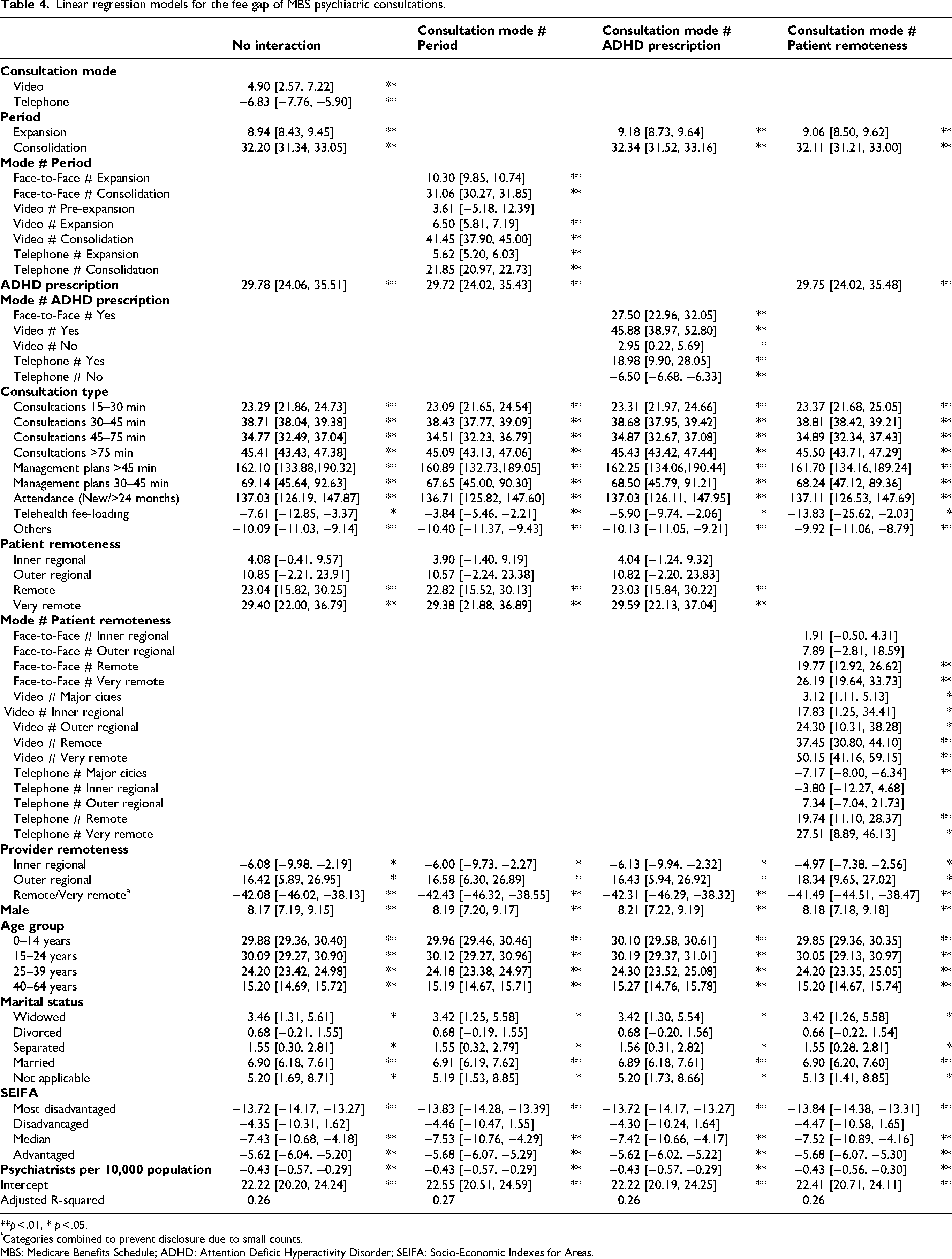
Fee gaps of non-bulk-billed video and face-to-face consultations were generally comparable (Table 4), with a difference of $$4.90 (95% CI: 2.57, 7.22). During the consolidation phase, video consultations had a marginal fee gap of $$41 (95% CI: 37.90, 45.00) relative to pre-expansion face-to-face consultations. This was $$10 higher than the corresponding face-to-face consultations. The telephone consultation fee gap was $$10 and $$20 lower than face-to-face and video consultations, respectively, during consolidation.
Linear regression models for the fee gap of MBS psychiatric consultations.
**p < .01, * p < .05.
Categories combined to prevent disclosure due to small counts.
MBS: Medicare Benefits Schedule; ADHD: Attention Deficit Hyperactivity Disorder; SEIFA: Socio-Economic Indexes for Areas.
Gaps were substantially higher for patients in remote ($$23.04, 95% CI: 15.82, 30.35) and very remote ($$29.40, 95% CI: 22.00, 36.79) areas compared to cities. The difference was more pronounced for video consultations. For patients in remote and very remote areas, video consultations cost nearly twice as much as face-to-face consultations (Remote: $$37 vs. $$ 20; very remote: $$50 vs. $$26). However, providers in these regions charged a substantially lower fee gap than those in metropolises (difference: -$$42.08; 95% CI: −46.02, −38.13).
The most disadvantaged patients paid $$14 less than the most advantaged (95% CI: −14.17, −13.27). Fee gaps increased with socio-economic advantage, and the paediatric and adolescent age groups incurred the highest gaps. The per capita psychiatrist count was associated with a slightly lower fee gap (-$$0.43; 95% CI: −0.57, −0.29).
The fee gap for ADHD-related consultations was $$30 higher (95% CI: 24.06, 35.51) than non-ADHD-related consultations. The difference was most pronounced in video consultations, approximately $$46 higher than non-ADHD face-to-face consultations. ADHD consultations via telephone and face-to-face were $$27 and $$18 cheaper, respectively, than those by videoconferencing.
Discussion
We found general patterns of declining bulk-billing and rising fee gaps for MBS psychiatric consultations between 2017 and 2023, with clear differences across consultation types and modes. Clinicians appeared more willing to bulk-bill for short and very long consultations. The higher bulk-billing rates for very long consultations may be associated with patients who had complex conditions and were often socio-economically disadvantaged. 29 Lower fee gaps for telephone consultations may be due to clinicians’ perception that telephone consultations are of lower quality 30 or less time-consuming. Experience with non-reimbursed telephone consultations before their inclusion may have anchored psychiatrists to lower charges. 31
Such out-of-pocket cost trends mirror those of general practitioners (GPs) and other specialists.32,33 A key factor in rising out-of-pocket payments is that Medicare funding has not kept pace with real-world costs. For instance, the Consumer Price Index increased by 13.9%, and the Average Weekly Earnings by 14.7%, from 2017–2018 to 2022–2023, but the rebate increase for the commonly used GP Level B item was only 7.3%. 34 After the initial plunge during the telehealth expansion phase, bulk-billing rates for video consultations stabilised and remained higher than those for face-to-face consultations. The costs of operating face-to-face clinics are substantial 35 and have increased considerably since the COVID-19 pandemic. 36 In contrast, telehealth services involve comparatively lower fixed costs – such as staff salaries, IT maintenance, and broadband costs – potentially yielding operational savings and making bulk-billing more financially viable. The reinstatement of the incentivised Item 294 improved bulk-billing rates among rural patients, but the overall effect was likely modest because only a small proportion of telepsychiatry consultations were reimbursed under this item. Further investigation is warranted into rural-metropolitan differences in bulk-billing rates and the role of incentivisation.
Two factors interacted strongly with consultation modes: telehealth policy and ADHD prescription. ADHD-related prescriptions were associated with greater out-of-pocket costs, particularly in face-to-face and video modes. Surging ADHD prescriptions in recent years15,37 reflect strong demand, suggesting an emerging business model where providers charge higher gaps for high-demand services. 38 Notably, during the consolidation, video consultations incurred higher fee gaps than face-to-face consultations. While telepsychiatry may increase access, it may also encourage discretionary care that attracts higher fees, paradoxically raising out-of-pocket costs. 39 Further research is needed on the effects of the rising demand for ADHD tele-assessments on health equity.
On one hand, we observed notable differences in out-of-pocket costs by patient and provider remoteness. The reasons for the contrast between patients and providers in very remote areas, i.e. the former being less likely to be bulk-billed while the latter being very likely to bulk-bill, are uncertain. One possible explanation is that patients in very remote areas received more services from metropolitan providers who were less inclined to bulk-billing. Given its relevance to rural access equity, further research into this issue is warranted. On the other hand, the per capita psychiatrist count had little practical impact on bulk-billing and the fee gap, despite the uneven distribution of the psychiatrist workforce. 40 Our findings concur with the Medicine in Australia Balancing Employment and Life survey, which suggests that local competition may not significantly affect billing practices. 41 Out-of-pocket costs for rural and remote patients increased, even for telepsychiatry. Some patients may consider telepsychiatry comparable in value to face-to-face services and be willing to pay similar prices. Moreover, the costs avoided by using telepsychiatry – travel, accommodation, time lost from work – may justify paying more.42–44 Nonetheless, the rising cost burden of telepsychiatry for rural patients may be at odds with Medicare's stated objective to ensure equal healthcare access for all Australians. 45
This study leveraged linked population databases, allowing a granular and comprehensive analysis with high statistical confidence. However, several limitations must be acknowledged. Administrative data may contain entry errors. Although the deterministic linkage process using the Spine IDs was highly specific and accurate, linkage errors cannot be entirely ruled out. The MBS data lacked clinical information such as diagnosis and symptom severity. Our out-of-pocket cost analysis was confined to Medicare-covered services. We did not consider other healthcare funding sources, such as private insurance. Without other patient costs, including direct costs (medications, diagnostic tests, transportation, accommodation) and indirect costs (productivity loss, caregiver burden), the scope of economic assessment was limited. Consultations not linked to PBS data may reflect prescribing delegated to GPs. Therefore, prescription rates may be underestimated. However, the initiation of ADHD prescriptions is mostly restricted to psychiatrists or paediatricians, 15 enabling us to chart prescription trends with some confidence. A few ADHD prescriptions by psychiatrists might have been for narcolepsy and, uncommonly, treatment-resistant depression. State governments around Australia are increasingly enabling GPs to diagnose and treat ADHD. 46 This significant policy change may have a medium-term impact on ADHD-related out-of-pocket costs.
In summary, the expanded availability of telepsychiatry has not uniformly alleviated financial burdens, with patients’ out-of-pocket costs having increased over time. The especially high costs associated with ADHD prescription-related video consultations may limit service availability for other psychiatric conditions, thereby hindering access to care. This is a crucial area for future research, both in terms of healthcare and economics. There may be a need for clinical guidelines on telepsychiatry and reforms to Medicare item design to ensure that government-subsidised services are not diverted into provider-centric business models that undermine quality of care and health equity.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X251393387 - Supplemental material for The out-of-pocket costs of Medicare-reimbursed telepsychiatry consultations since telehealth expansion in Australia: An administrative data linkage analysis
Supplemental material, sj-docx-1-jtt-10.1177_1357633X251393387 for The out-of-pocket costs of Medicare-reimbursed telepsychiatry consultations since telehealth expansion in Australia: An administrative data linkage analysis by Luke Sy-Cherng Woon, Paul Maguire, Rebecca E Reay, Tarun Bastiampillai, Jeffrey CL Looi and Wai-Man Liu in Journal of Telemedicine and Telecare
Footnotes
Acknowledgements
We thank the data custodians for permitting access to the dataset used in this study.
Ethical considerations
This study received ethics approval from the Human Research Ethics Committee of the Australian National University (H/2024/0986).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data availability statement
The data that support the findings of this study are available from the ABS and the Australian Department of Health, Disability and Ageing. Restrictions apply to the availability of these data, which were used under license for this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.