
Abstract
Background
The patient navigation programme (PNP) is an effective health intervention to address barriers in accessing timely and equitable cancer care. However, its expansion in Malaysia for breast cancer care faces challenges due to limited capacity building among nurses and navigators, particularly nurses who are actively involved in the operation of the PNP centres. The Extension for Community Healthcare Outcomes (ECHO®) model, a tele-mentoring approach, offers a scalable and sustainable solution for capacity building among the nurses and navigators. This study aims to evaluate the feasibility and impact of using the ECHO model to train nurses and navigators on patient navigation competencies focused on improving breast cancer care delivery.
Methods
The study involved nurses in breast cancer care from Ministry of Health (MOH) state referral hospitals in Malaysia and newly recruited nurses and social workers by Cancer Research Malaysia to subsequently be placed as nurse and community navigator for the upcoming new centres. Participants received an ECHO-based training programme comprising bi-weekly virtual sessions of a six-domain curriculum covering 12 topics on patient navigation competencies. Pre- and post-session assessments were conducted to measure satisfaction, knowledge and confidence in conducting patient navigation.
Results
Most participants were within the age range of 31–35 (n = 38; 40.4% [95% CI, 30.5%–50.3%]) with majority being female (n = 87; 92.6% [95% CI, 87.2%–97.9%]) and MOH nurses (n = 71; 75.5% [95% CI, 66.8%–84.2%]). An average of 28 participants attended each session. Participants expressed high level satisfaction while showing improvements in knowledge and confidence with an average increase in mean score of (1.45 [95% CI, 0.84–2.13]; p < .05) and (0.61 [95% CI, 0.51–0.65]; p < .05) respectively following the intervention.
Conclusion
The study demonstrates the feasibility and effectiveness of the ECHO model for patient navigation capacity building among nurses and navigators. Findings support broader implementation of the ECHO model to strengthen breast cancer care delivery.
Introduction
Breast cancer remains as the most prevalent malignancy in Malaysia, with an annual incidence rate of 46.1 per 100,000 women and a 5-year survival rate of 66.8%, which falls short of the regional average of 70.8%.1–3 Alarmingly, late-stage diagnoses constitute 48% of total cases, highlighting a significant disparity in goals outlined in the National Strategic Plan for Cancer Control is to enhance 5-year survival rates by reducing late-stage diagnoses to 25% by the year 2030. 4 Access to timely, cost-effective, and efficacious diagnostic and therapeutic interventions is crucial for the realization of this target. 5
Patient navigation (PN) is a patient-centred strategy designed to facilitate timely patient progression through complex healthcare systems by enhancing care coordination and providing support to overcome barriers to care. 6 Since 2015, Cancer Research Malaysia (CRMY) in collaboration with the Ministry of Health (MOH) has implemented a breast cancer patient navigation programme (PNP) in four of 13 states in Malaysia namely Selangor, Negeri Sembilan, Sabah and Sarawak. 7 Over the years, PNP has improved timeliness in cancer care, with increases of 18% in diagnosis, 10% for surgery and 17% for neoadjuvant treatment. Furthermore, the programme has reduced treatment default rates from 13% to 2%. 8 These achievements highlight the need for nationwide expansion of the PNP to all hospitals with cancer surgical services.
Globally, structured patient navigation and workforce development programmes are receiving increasing recognition. A recent publication in JAMA Network Open underscored the value of training and tele-mentoring models like Extension for Community Healthcare Outcomes (ECHO) in enhancing access to specialty care and improving clinical outcomes, particularly in resource-constrained settings. 9 This strengthens the rationale for the implementation of the ECHO model for PN capacity building in Malaysia and potentially across other low- and middle-income countries (LMICs).
The PNP model centres on collaboration within a multidisciplinary team including healthcare providers (e.g. MOH staff such as surgeons, medical officers and nurses) and CRMY navigators. 8 Capacity building for this team – particularly for nurses and navigators who are heavily involved in the PNP operation – is currently limited. Navigators at the four established PNP centres received training via the George Washington University Cancer Centre's Online Academy Patient Navigation module, followed by on-the-job peer training. 8 However, MOH healthcare providers, who are equally involved in PNP centre operations, lack specific training in patient navigation. This gap highlights the need for a scalable and sustainable training programme to develop patient navigation competencies and support PNP expansion. Effective and ethical patient navigation requires adequate training and certification, yet standardized training programmes addressing fundamental care coordination skills remain scarce.10,11
Project ECHO is the new-age collaborative educational model developed at the University of New Mexico School of Medicine in 2003 to improve access to complex specialty care for patients in underserved regions. 12 This hub-and-spoke tele-mentoring model of all-teach, all-learn approach is a cost-effective and accessible model that leverages videoconferencing technology to create knowledge-sharing networks. It connects subject matter experts or specialists (hub) and healthcare providers (spokes) across diverse locations through bi-weekly videoconferencing sessions which eliminates professional isolation. 13 The ECHO model has demonstrated substantial success in building capacity among healthcare professionals, leading to improved health outcomes across various diseases.14–17 Adopting this model, we developed a flexible competency-based training programme to build capacity for patient navigation in Malaysia. This nationwide study is the first of its kind, aims to evaluate the impact of the ECHO model on satisfaction, knowledge and confidence among nurses and navigators in conducting patient navigation. The results will determine the feasibility of the model for capacity building in patient navigation for breast cancer.
Methods
The study was approved by the Malaysian Research Ethics Committee (NMRR ID-23-03279-UPM) and conforms to the principles of Declaration of Helsinki.
Training module development
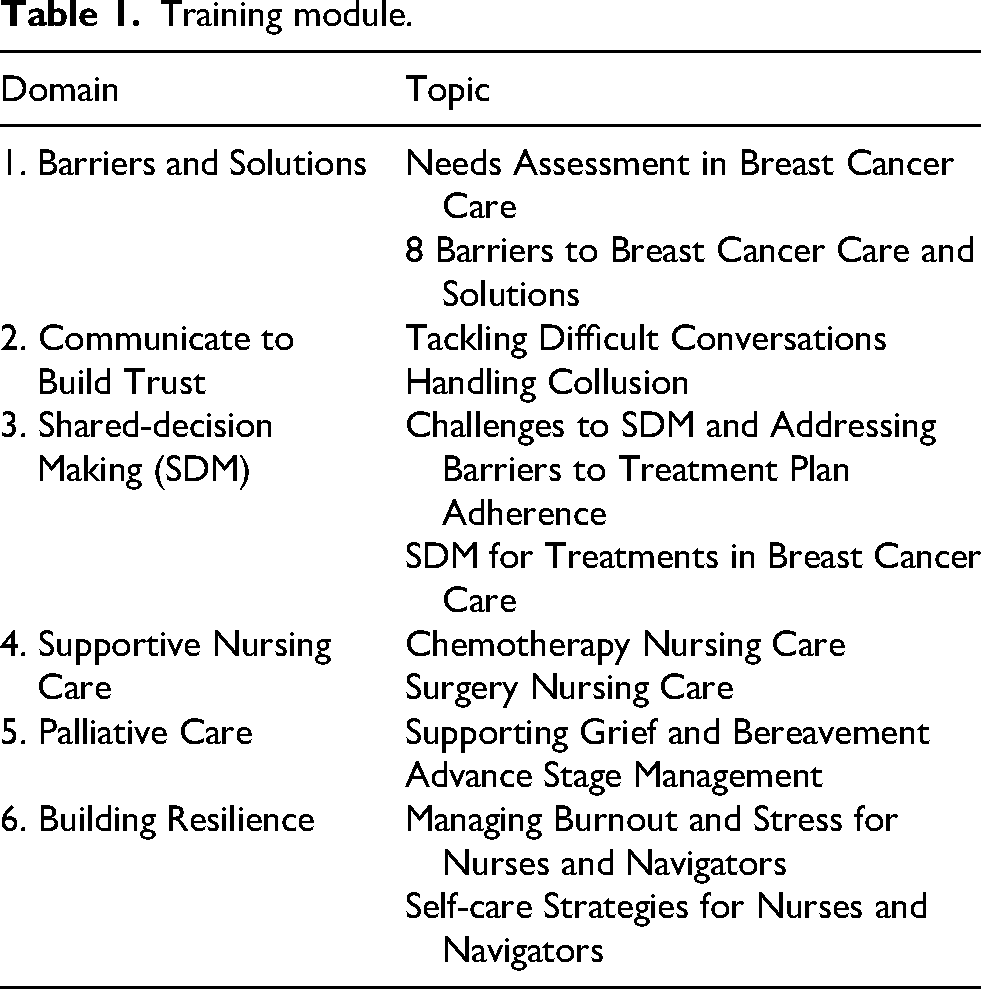
The core competencies for PN training in this study were determined based on George Washington PN module 18 and The Boston Medical Center PN Toolkit 19 to develop a culturally relevant curriculum that covers six domains; barriers and solutions; communication; shared-decision making; supportive nursing care; palliative care; and building resilience. Each domain consists of two learning topics tailored to the Malaysian context – informed by local guidelines, community practices and beliefs as in Table 1.
Training module.
Recruitment of spokes
Programme promotional materials were shared with the senior navigators of the four established PN centres to be distributed among their colleagues who are nurses. These nurses then shared the promotional materials within their respective nursing groups on Whatsapp and Telegram effectively reaching staff nurses serving in other MOH state referral hospitals nationwide. Link for registration via Microsoft Forms were attached to the promotional materials to capture the number of estimated participations to maintain participants within the range for every session. Distributed promotional materials include details that invitation is extended to nurses involved in breast cancer care and servicing in MOH hospitals only. Registration was kept open and flexible throughout the programme, allowing participants to sign up for individual sessions instead of committing to the entire series, making it more accessible and removing barriers to participation. Prior to the training, CRMY recruited two nurses and four social workers to serve as nurse navigators and community navigators respectively for the upcoming new PNP centres. These newly recruited nurses and social workers, along with the MOH nurses (designated as ‘spokes’) volunteered to present cases during the training.
Conduct of training
The iECHO platform was used to deliver 12 ECHO sessions conducted bi-weekly over 6 months. Each session included a brief didactic talk, a case presentation, a group discussion and a summary. To ensure participants’ engagement and interactivity, a facilitator from the hub team was appointed to moderate the sessions. During the didactic talk, a subject matter expert shared foundational concepts, best practices and the latest insights pertaining to the topic. A ‘Spoke’ presents a case which was then discussed by all attendees, including the subject matter expert. Before closing each session, the facilitator summarized the discussions. Sessions were conducted in both English and Bahasa Melayu to enhance understanding and participation. The number of participants was maintained between 20 and 30 to ensure a high-quality and interactive learning environment. Pre- and post-session assessments were administered to participants, and all presentation materials (didactic talks, case studies, and additional references) were shared via the iECHO platform. Training certificates, endorsed for Continuous Professional Development points, were awarded to participants who attended the session and successfully completed both assessments.
Data collection and analysis
The ECHO model utilizes Moore's seven-level framework to assess participation, satisfaction, self-reported improvements in areas of learning and confidence in competency, patient and community outcomes. 20 An evaluation matrix was developed to analyse operations, spoke site engagement, satisfaction and spokes outcomes. Attendance was captured and extracted from the iECHO platform. Data on knowledge, satisfaction and confidence were collected through the pre- and post-session assessment via Microsoft Forms administered to participants at every session. The assessment form is divided into two sections for the pre-session assessment with one additional section for the post-session assessment. Section 1 measures confidence levels in their knowledge and self-efficacy in patient navigation. Section 2 assesses their knowledge of the topic and Section 3, included only in the post-session assessment, gathers feedback about the session to measure participants’ satisfaction. All assessment forms were designed in the national language, Bahasa Melayu, to ease understanding and responding. Data were analysed in Microsoft Excel 2019 using descriptive statistics and expressed as frequency, mean, standard deviation and paired t-test.
Results
Participants’ demographics are summarized in Table 2. Most participants were within the age range of 31–35 (n = 38; 40.4% [95% CI, 30.5%–50.3%]) and 26–30 (n = 29; 30.9% [95% CI, 21.5%–40.2%]) years old. Majority of the participants were female (n = 87; 92.6% [95% CI, 87.2%–97.9%]) MOH nurses (n = 71; 75.5% [95% CI, 66.8%–84.2%]) with newly recruited nurses (n = 2; 2.1% [95% CI, 0.0%–5.0%]) and social workers (n = 4; 4.3% [95% CI, 0.2%–8.3%]). 12 sessions were completed over the course of 6 months where a didactic and a case presentation were delivered at each session. The series has garnered participation from 13 different MOH hospitals across the nation. 94 participants (88 nurses, 2 newly recruited nurses and 4 social workers) attended more than one ECHO training session, 65 completed both pre- and post-assessments and were included in the analysis. On average, 28 participants attended each session. 69.1% [95% CI, 59.8%–78.5%] of the participants gained a certificate (n = 65).
Demographic details of participants attending ≥ 1 session (n = 94).
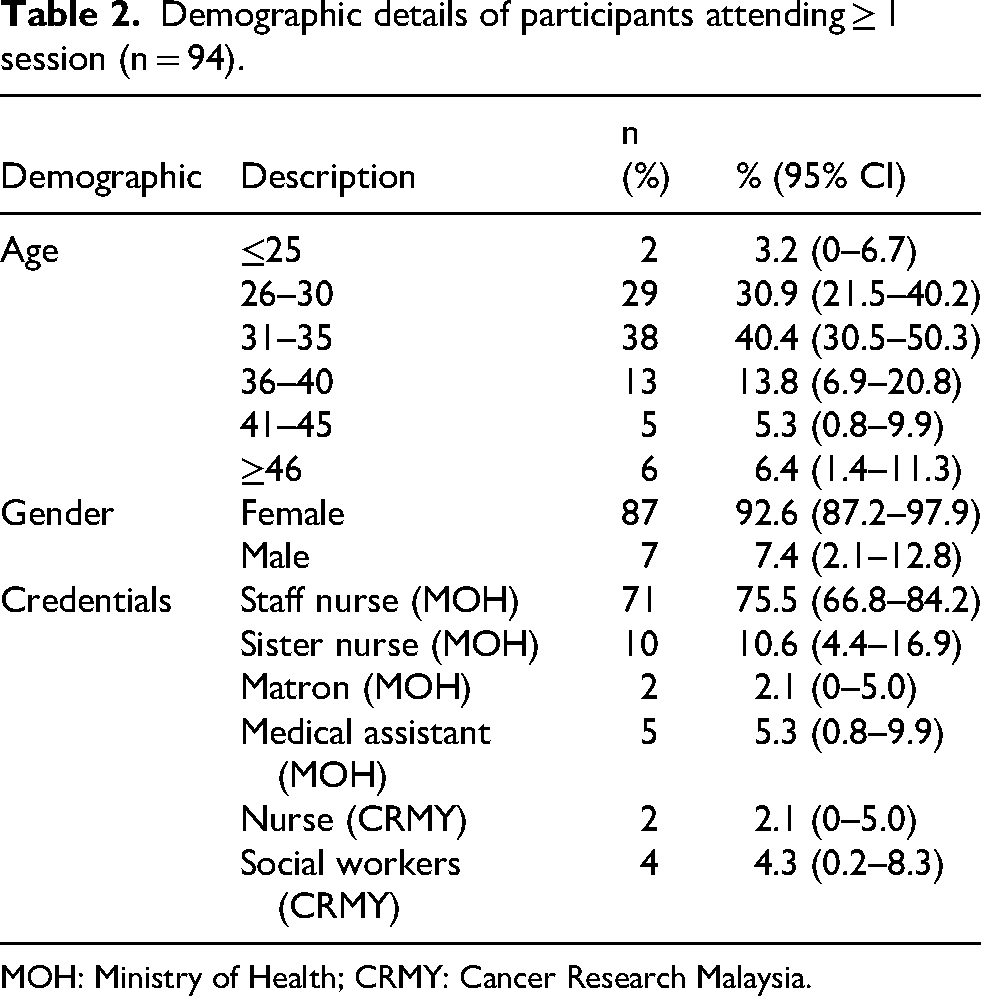
MOH: Ministry of Health; CRMY: Cancer Research Malaysia.
Participant satisfaction remained consistently high across all sessions, with ratings over 4.0 on a 5-point Likert scale (1 = very unsatisfactory, 2 = unsatisfactory, 3 = neutral, 4 = satisfactory, 5 = very satisfactory). The concluding session achieved a peak rating of 4.92 [95% CI, 3.89–4.45], and the overall satisfaction per session was 4.42 [95% CI, 4.08–4.76]. Table 3 summarizes the satisfaction ratings for each session.
Participant satisfaction for each PNP ECHO session (n=65).
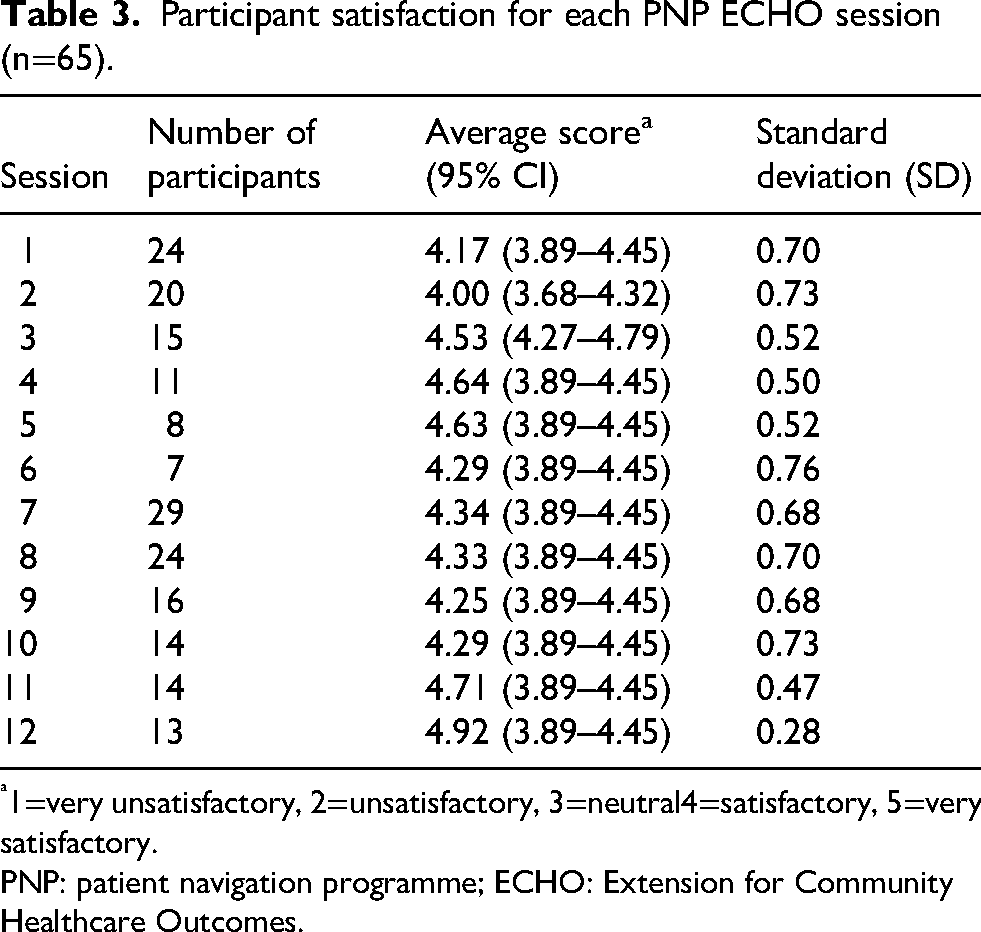
1=very unsatisfactory, 2=unsatisfactory, 3=neutral4=satisfactory, 5=very satisfactory.
PNP: patient navigation programme; ECHO: Extension for Community Healthcare Outcomes.
An improvement in knowledge was observed, with an average increase in mean score for knowledge of 1.45 [95% CI, 0.84–2.13]; p < .05. Table 4 illustrates the increase in knowledge mean score after every session. Significant improvements were noted for sessions 1 (mean score difference: 1.54 [95% CI, 0.24–2.84]; p = .022), 2 (mean score difference: 1.80 [95% CI, 0.55–3.05]; p = .007), 3 (mean score difference: 2.40 [95% CI, 1.03–3.77]; p = .002), 4 (mean score difference: 2.00 [95% CI, 0.63–3.38]; p = .009), 7 (mean score difference: 2.24 [95% CI, 1.12–3.36]; p < .001), 11 (mean score difference: 1.21 [95% CI, 0.02–2.42]; p = .048) and 12 (mean score difference: 3.46 [95% CI, 1.77–5.15]; p < .001).
Mean knowledge score pre-and post-PNP ECHO session (n = 65).
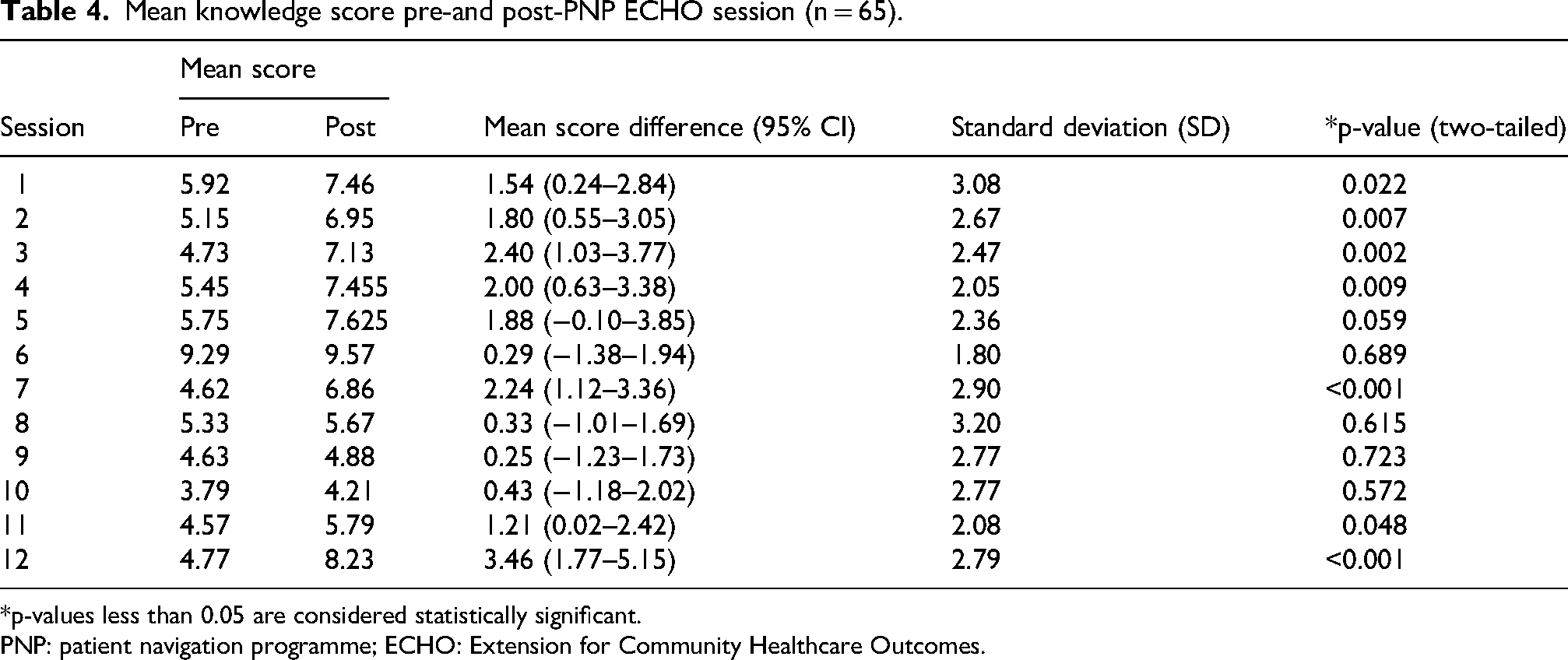
*p-values less than 0.05 are considered statistically significant.
PNP: patient navigation programme; ECHO: Extension for Community Healthcare Outcomes.
In terms of confidence and self-efficacy, participants reported an average increase of 0.61 [95% CI: 0.51–0.65]; p < .05 in mean scores on a 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree). The average rating was 3.50/5 at baseline and increased to 4.10/5 by the end of session 12. Table 5 shows the changes in participants’ self-rated confidence across training sessions. 21 of 65 participants reported intent to apply teachings.
Change in confidence or self-efficacy in PN competencies (n = 65).
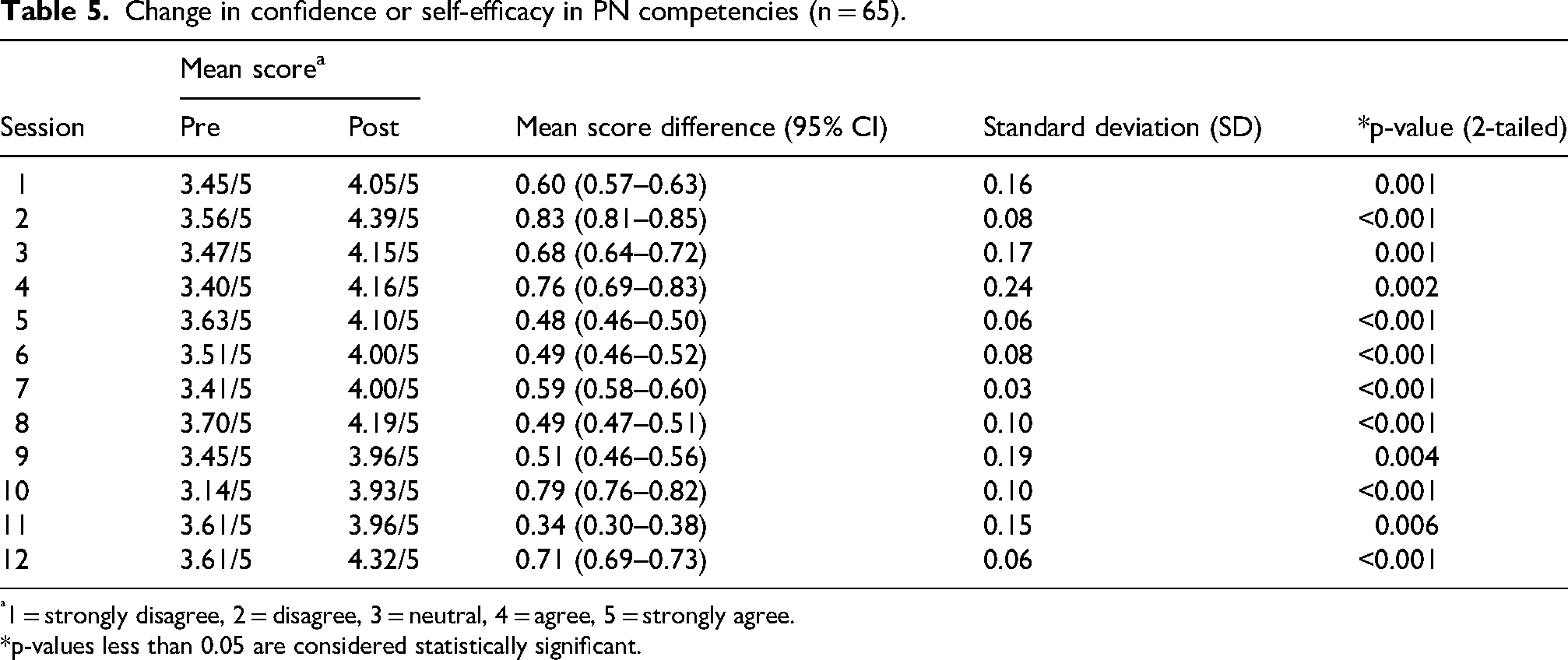
1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree.
*p-values less than 0.05 are considered statistically significant.
Discussion
The study indicated encouraging participation in the ECHO training for breast cancer patient navigation among the nurses involved in breast cancer care servicing in MOH state referral hospitals. Participants were satisfied with the training and demonstrated significant improvements in knowledge and confidence in conducting patient navigation, showing the feasibility of the training model for capacity building. This study provides compelling evidence for the potential of the ECHO model to be a scalable and sustainable solution to address the critical shortage of trained healthcare workers in cancer care delivery, particularly in LMICs. The findings emphasize the public health importance of implementing virtual capacity building programmes that are both cost-effective and accessible. Given the adaptability of the ECHO model, this approach can be extended to other disease areas and used to inform implementation science frameworks globally.
Competency-based training increases participant engagement, retention and satisfaction
The ECHO model shifts from a traditional, theoretical knowledge-focused approach to a competency-based training for healthcare professionals. This dynamic framework encourages continuous skill enhancement and knowledge acquisition for proficiency in specific role.13,14 In the United States, recent review highlighted the inconsistency in training for PN with significant variations in durations, locations, formats, learning strategies, trainers’ expertise and programme content. 11 To ensure effective PN, training should be standardized based on agreed-upon core competencies and quality standards, with established metrics to measure knowledge and skills required beyond traditional degree or clinical training. 10 Establishment of PNP for breast cancer since 2015 8 has now expanded to include eight state referral hospitals with recruitment and training of 17 navigators. Between 2015 and 2020, a total of 2633 women were navigated leading to improved timeliness in cancer care. 8 This achievement was recognized by the World Health Organization (WHO) and featured as a case study in the Patient Navigation for Early Detection, Diagnosis, and Treatment of Breast Cancer technical brief in 2024. 15 The experiences and achievements in PNP put the team in a credible position to devise a culturally relevant training module and conduct capacity building training.
Learning satisfaction, whether in e-learning or blended environments, has been linked to technology familiarity, perceived convenience and ease of use. 8 The iECHO platform leveraged this by integrating Zoom, a widely familiar tool from COVID-19, with access to essential resources for PN. This familiar and convenient design allowed participants to focus on the learning material, contributing to high technology acceptance and satisfaction. 16 Furthermore, the bilingual delivery of sessions in both English and Bahasa Melayu was an important facilitator for inclusive participation given the linguistic diversity of healthcare professionals in Malaysia that has additionally contributed to increase in engagement and satisfaction of training. While verbal discussion alternated between both languages depending on participants’ preference, the written information and evaluation materials were standardized to Bahasa Melayu to align with MOH training conventions and ensure consistency across sites. As majority of the participants are nurses servicing in MOH who primarily communicate in Bahasa Melayu in clinical setting, this approach did not appear to exclude English speaking participants who equally engaged actively during discussions. Nonetheless, future training iterations may consider providing all written materials bilingually to further enhance accessibility.
Tailored training programmes for PN in breast cancer could address specific competencies and operational challenges in patient care coordination aligning with global initiative to improve access to healthcare services for breast cancer.
Successful knowledge transfer through collaborative ECHO model
The significant improvement in knowledge observed in more than half of the sessions suggests that the ECHO model is a robust platform for building PN knowledge. Although participants’ knowledge did not improve for sessions 6, 8, 9 and 10 this may be due to several factors such as personal, contextual, relevance of topic for practice and participants’ baseline familiarity to topic. 17 Personal factors pertain to individual-level influences, whereas contextual factors encompass a spectrum of impacts, from close interpersonal interactions to broader influences such as institutional, organizational, community, and sociopolitical dynamics.21,22 Individual and contextual factors impact knowledge gain by affecting the learners’ adaptability and motivation in choosing to participate in the learning activities, put in effort and persist in self-regulation.23,24 In order to address this, future sessions should be tailored to participants’ prior knowledge and incorporate interactive components to foster deeper engagement.
Its core principles – tele-mentoring combined with evidence-based education – drive excellence through deliberate practice, role modelling and collaborative feedback. 20 The model's flexible teleconferencing format enabled nurses and navigators involved in breast cancer care from across the country to participate in the training, despite their heavy workloads in public hospitals. 23 This created a rich pool of knowledge and experience, enabling participants to learn best practices, updated knowledge and share experiences on PN in breast cancer care.
Educational reinforcement improves confidence and self-efficacy
Confidence and self-efficacy of participants in PN for breast cancer knowledge and competencies improved across the training. This is supported by the rise in average rating from 3.50/5 ‘Neutral’ pre-session to 4.10/5 ‘Agree’ post-session with notable gains in session 2 and 12. This pilot study supports existing research by demonstrating that educational reinforcement enhances confidence, which drives commitment to practice changes, knowledge and competence improvements further boosting confidence levels. 25
Although most sessions showed marked improvements in confidence, sessions 9, 10 and 11 recorded relatively modest changes. These may indicate either a plateau effect in confidence gains or less engaging formats. Studies suggest a positive association between engaging learning environment and academic performance and confidence development.26,27 The sessions recording modest changes in confidence correspond to the sessions with non-significant difference in knowledge. In a study, it was found that haematologists and oncologists who were involved in an online oncology continuing medical education programme with improved (b = .79, P < .001) or reinforced (b = .83, P < .001) knowledge exhibited significantly higher post-education confidence levels averaging 32% and 34% greater than the unaffected group. 28 Upcoming sessions should focus on periodic adjustments to content delivery to be able to sustain participant motivation and ensure a continued increase in knowledge and confidence.
Future direction of evaluating ECHO-based training implementation
Beyond evaluating self-reported individual level of knowledge, confidence and satisfaction gains, the sustainability and system-wide adoption of the ECHO model in Malaysia requires scoping consideration. Recent literatures highlight frameworks that evaluate the organizational and implementation success of ECHO programmes across diverse health systems. A comprehensive 54 indicator framework encompassing four domains; spoke engagement, hub and network design and operation, hub team engagement and local impact were developed and could be adopted for future iterations of Malaysian ECHO programmes for benchmarking progress and evaluate scalability. 29 In parallel, Proctor et al.'s taxonomy of implementation outcomes which comprises of acceptability, adoption, appropriateness, feasibility, fidelity, penetration and sustainability were adopted to the ECHO Ontario Mental Health programme delineating a structured approach to evaluating implementation impact in capacity building. 30 Organizational readiness and contextual adaptation for long-term sustainability were emphasized by the effective diffusion of ECHO initiatives that relies on strong leadership involvement, recognition of their value and alignment with institutional goals. 31 Incorporating such frameworks and indicators, many of which that could be measured through data available in the iECHO platform, would strengthen evaluation rigour, facilitate continuous quality improvement and support broader institutionalization of ECHO-based training programmes across Malaysia. Furthermore, the outcomes observed in this study appear to be consistent with global experiences reported by other ECHO hub organizations as highlighted in a global cross-sectional analysis of 13 ECHO hubs with 51 networks that demonstrated successful programmes characterized by effective pre-launch planning, consistent hub team engagement and alignment with institutional and governmental strategic priorities 32 – factors that similarly underscores the success of ECHO programmes in Malaysia. Demonstrable improvements in knowledge and confidence with high satisfaction observed in this study reflect key indicators of implementation success particularly within the domains of spoke engagement and local impact. 29 Regardless, future benchmarking with global ECHO networks would enable a more systematic comparison of performance metrics, fidelity and impact helping to identify opportunities for strengthening evaluation capacity and ensure the Malaysian ECHO experience continues to mirror international standards of excellence.
Strengths and limitations
The wide participation of nurses who had not previously conducted patient navigation demonstrates the effectiveness of the programme's engagement strategies. Additionally, session satisfaction assessed at every session provided better insights, as each session was conducted with structured evaluations. Limiting session sizes to fewer than 30 participants ensured effective knowledge transfer and promoted engagement. However, despite these promising results, the reliance on self-reported confidence ratings may introduce bias, as participants could overestimate their knowledge and self-efficacy.
Measuring overall confidence rather than session-specific confidence may also provide a more accurate indication of participants’ likelihood to implement patient navigation in their respective work settings. To address these limitations, future studies should incorporate additional evaluations, such as assessing changes in clinical practice and the impact of training on patient outcomes. The small sample size of newly recruited nurses and social workers (n = 6) who are subsequently to serve as nurse and community navigator thereafter limits the generalizability of findings for this subgroup, and variability in session outcomes highlights the need for ongoing curriculum refinement to ensure a consistent impact. Additionally, the absence of a control group limits causal inference. To address these limitations, future studies should incorporate randomized or quasi-experimental designs to rigorously evaluate the effectiveness of the ECHO model. Longitudinal studies should also assess whether training leads to sustained improvements in clinical practice and patient outcomes, particularly for newly recruited navigators. Furthermore, broader implementation studies can explore the contextual factors that affect scalability across diverse healthcare settings and disease areas.
Conclusion
This study highlights the effectiveness of the ECHO model for patient navigation capacity building in Malaysia. By demonstrating the model's feasibility and positive impacts, this research supports its use and expansion. Future implementation should focus on scaling up the reach of this training to include more healthcare workers and refine the programme to maintain its effectiveness. Benchmarking the programme against international standards would provide valuable insights into the continuous effectiveness and scalability with the use of established frameworks and success indicators in enhancing evaluation and align with global best practices.
Footnotes
Acknowledgements
We would like to thank the Director General of Health Malaysia for his permission to publish this article. We would also like to thank the nurses, newly recruited registered nurses and social workers who have taken an active role as case presenters in the training. We are grateful to the senior nurse and community navigators who were involved as the hub team and played a crucial role in conducting the training.
Ethical consideration
The study was approved by the Malaysian Research Ethics Committee (NMRR ID-23-03279-UPM) and conforms to the principles of Declaration of Helsinki.
Consent to participate
The study was approved by the Malaysian Research Ethics Committee (NMRR ID-23-03279-UPM). All participants provided written informed consent prior to participating.
Author contributions
KHC had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design done by KHC, JK, and AA. Acquisition, analysis, or interpretation of data done by KHC, AA, JK. Drafting of the manuscript done by KHC. Critical revision of the manuscript for important intellectual content done by all authors. Statistical analysis done by KHC, AA, and JK. Administrative, technical, or material support done by all authors. Supervision done by JK.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by charitable funds received by Cancer Research Malaysia through Yayasan PETRONAS. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are not available for sharing because they contain sensitive participants information and cannot be shared under the terms of the ethics approval.