
Abstract
Introduction
Antibiotic resistance is a growing public health threat, resulting in challenges in effectively treating bacterial infections. Primary care providers account for the majority of antibiotic prescriptions, highlighting their critical role in antimicrobial stewardship. As telemedicine becomes more prevalent in primary care, there is limited data on how this shift has influenced antibiotic prescribing behavior. Our objective was to examine differences in antibiotic prescription rates for upper respiratory infections (URIs) between in-person and telemedicine appointments in a large primary care health system.
Methods
In this retrospective cohort study, we included patients 18 years and older treated in primary care clinics in the Greater Atlanta area from May 2020 to September 2023. Eligible encounters were billed with a diagnostic code related to URI. The main measures included patient demographics, insurance status, and visit modality. A multivariable logistic regression model evaluated differences in antibiotic prescriptions by visit type.
Results
There were 33,008 (66%) in-person visits and 16,965 (33.9%) telemedicine visits, totaling 49,973 encounters. The average age of patients was 56.8 (SD 17.5) years, 67.1% patients were female, and 37.6% were Black. There were no significant differences in antibiotic prescribing between telemedicine and in-person appointments (adjusted odds ratio 1.00, 95% CI 0.14–4.86, P > 0.5).
Discussion
Rates of antibiotic prescribing did not differ significantly between in-person and telemedicine primary care visits for URI. As a healthcare quality indicator, this result provides evidence that in-person and telemedicine appointments are comparable modalities of patient care.
Introduction
The World Health Organization states that antimicrobial resistance (AMR) is one of the top 10 global health crises. 1 AMR poses significant health risks as antimicrobial-resistant infections are more difficult to treat. Morbidity and mortality increase with widespread AMR, directly resulting in increased healthcare costs (estimated up to $1 trillion USD by 2025). 2
The Centers for Disease Control and Prevention (CDC) reports that the vast majority (80–90%) of antibiotic use occurs in outpatient settings. 3 Furthermore, most antibiotic prescriptions in ambulatory settings are prescribed to treat upper respiratory infections, for which evidence has shown antibiotics have little effect on symptom management or duration.4–6 For these reasons, antibiotic prescribing has been used as a quality metric in outpatient visits, particularly for URI, and significant efforts have been taken to increase antibiotic stewardship in this setting.7–10
In recent years, telemedicine has been a widely used alternative method for patients to attend outpatient appointments, as opposed to attending clinics in-person. Telemedicine has been a method of care delivery to patients with mobility or access issues since before the COVID-19 pandemic, with utilization rising over 700% during the first few months of the pandemic. 11 Now, in a post-pandemic era, telemedicine is still used for convenience and ease of access for patients. 12 Even so, after quickly adjusting their policies during the pandemic to expand coverage for telemedicine appointments, the Centers for Medicare and Medicaid Services (CMS) are discussing plans to sunset reimbursement, leading physician organizations such as the American Medical Association to lobby in support of continued coverage. 13 It is therefore critical to continue investigating how telemedicine compares to in-person office visits on important healthcare quality outcomes. A key question is whether there are possible differences in the quality of care and treatment between telemedicine and in-person appointments, with one metric being antibiotic prescriptions.14,15
Previous investigations into outpatient antibiotic prescribing practices have shown differences based on geographic location, neighborhood socioeconomic status, and patient demographics. 16 For example, studies have shown that areas with a higher physician density and poverty rate increase antibiotic prescription rates.17–19 Furthermore, White and non-Hispanic patients receive the highest overall antibiotic prescriptions, although there is evidence that Black patients receive more inappropriate antibiotic prescriptions.4,20 There is also evidence that patients with private insurance receive more antibiotic prescriptions than those with Medicare or Medicaid.4,20
In general, antibiotic prescribing during telemedicine appointments has been shown to be similar to, or lower than, in-person appointments; however, there are mixed results. One systematic review concluded that there was insufficient evidence to support a difference in antibiotic prescribing between the two modalities. 21 Other studies have shown lower rates of antibiotic prescribing, both in general and specifically for URI visits.22,23
Our study aimed to investigate the differences in antibiotic prescription rates between in-person and telemedicine visits for URIs in a large health system. The goal of this investigation was to determine comparability in modes of care delivery between in-person and telemedicine appointments using antibiotic prescribing as a metric, as it is widely used as a healthcare quality indicator. Given that telemedicine appointments lack an essential component of an in-person physical assessment, we hypothesize that telemedicine appointments will have higher antibiotic prescribing rates than in-person appointments. These rates will not be affected by age, race, gender, or insurance status.
Methods
Population
We conducted a retrospective study to compare antibiotic prescription rates in telemedicine vs in-person visits completed by primary care providers. As a response to the COVID-19 pandemic, beginning in March 2020, our healthcare institution offered telemedicine appointments for ambulatory visits via Zoom (Zoom Video Communication, Inc., San Jose, CA), which included both an audio and video component in a synchronous format, compliant with the Health Insurance Portability and Accountability Act and approved for clinical use in the United States. These visits are also covered under the notice of privacy practices required to be approved and signed by all new patients when they establish care with our healthcare system.
Our study included adult patients (>18 years old) whose Principal Visit Diagnosis in the electronic health record (EHR) was consistent with an Upper Respiratory Infection (URI) using the International Classification of Diseases, Tenth Revision (ICD-10) codes. The included ICD-10 codes were chosen based on common symptoms of URIs. Diagnoses for which antibiotics are the standard treatment (i.e., Otitis media, sinusitis) were excluded as to not have a confounding effect on rates of antibiotic prescribing. A list of principal visit diagnoses of included encounters and the frequency and percentage of each diagnosis that received an antibiotic prescription are shown in Supplementary Table 1.
Patients were included if they had either an in-person or telemedicine visit completed with a primary care provider between May 2020 and September 2023. We excluded patient visits that were repeated within a 2-week timeframe to avoid confounding due to the severity of URI. Patients diagnosed with COVID-19 verified by a positive polymerase chain reaction test were excluded from the study, as they were encouraged to schedule telemedicine visits or directed to urgent care if symptoms were severe. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines for cohort studies. 24
Variables
In this study, exposure depended on telemedicine or in-person visit modality, which were identified through the EHR for each encounter and coded as such in the model. A telemedicine visit was defined as a visit conducted with real-time, concurrent audio and video representation of the patient, and an in-person visit was defined as a visit where the patient was physically present in the clinic. The measured outcome was whether the visit resulted in an antibiotic prescription, as captured through EHR data.
Additionally, the EHR was used to collect data on other variables, including age, gender, patient-reported race, clinic location, insurance status, and hypertension diagnosis. Supplementary Table 2 shows a list of clinic identifiers used to assure data was pulled from primary care clinic encounters. We also extracted diagnoses via ICD-10 codes from patients’ problem lists to calculate the Charlson Comorbidity Index (CCI) for each patient. 25
To investigate the validity of extracted data relating to visit diagnoses and antibiotic prescription appropriateness, we also conducted a small manual chart review on 20 encounters, including 10 telemedicine encounters and 10 in-person encounters. The encounters were selected via a random number generator matched to the patient medical records number. The majority of encounters (75%) had antibiotics prescribed for an appropriate indication.
Statistical analysis
We created a multivariable logistic regression model to examine differences in antibiotic prescribing prevalence between visit modalities (in-person vs. Telemedicine) and the likelihood of antibiotic prescribing for upper respiratory infections (URIs) among primary care patients. The primary predictor variable, appointment type, was set as a factor with “in-person” as the reference level to allow comparison against telemedicine visits.
The model included patient demographic and clinical characteristics, such as age (included as a continuous variable), gender, and race. The CCI was included as a continuous variable to account for comorbidities, and hypertension status was included as a binary variable (as patient records indicated either “yes” or “no” if the diagnosis was present or not). Insurance type was also factored into the model, with private insurance as the reference category. An interaction term between race and appointment type was added to assess any differential effects of telemedicine on antibiotic prescribing across racial groups. Interaction terms were also assessed for age and gender. This approach, using a logit link function, enabled the calculation of odds ratios for each variable. All analyses were conducted using R (version 4.2.1; Rstudio, Inc., Boston, MA).
Due to the time course of our study taking place during the COVID-19 pandemic, we were interested to see if the time period had any effect on appointment types and antibiotic prescriptions. We performed a time sensitivity analysis, which showed that antibiotic prescribing generally increased after the pandemic; however, no significant differences were observed between telemedicine and in-person visits during any period.
Results
Demographics of the study population are shown in Table 1. Overall, there were 49,973 encounters in the study duration, with 33,008 (66%) being in-person visits and 16,965 (33.9%) being telemedicine visits. The average age at visit date was 56.8 (SD 17.5) years. A total of 22,152 (67.1%) of these visits were with female patients, and 10,854 (32.9%) were with male patients. Just under half of the visits were with White patients (48.1%), and 37.6% were with Black patients. The frequency of antibiotic prescriptions was higher during in-person appointments (2.7%) than during telemedicine appointments (1.2%).
Demographic characteristics of the cohort.
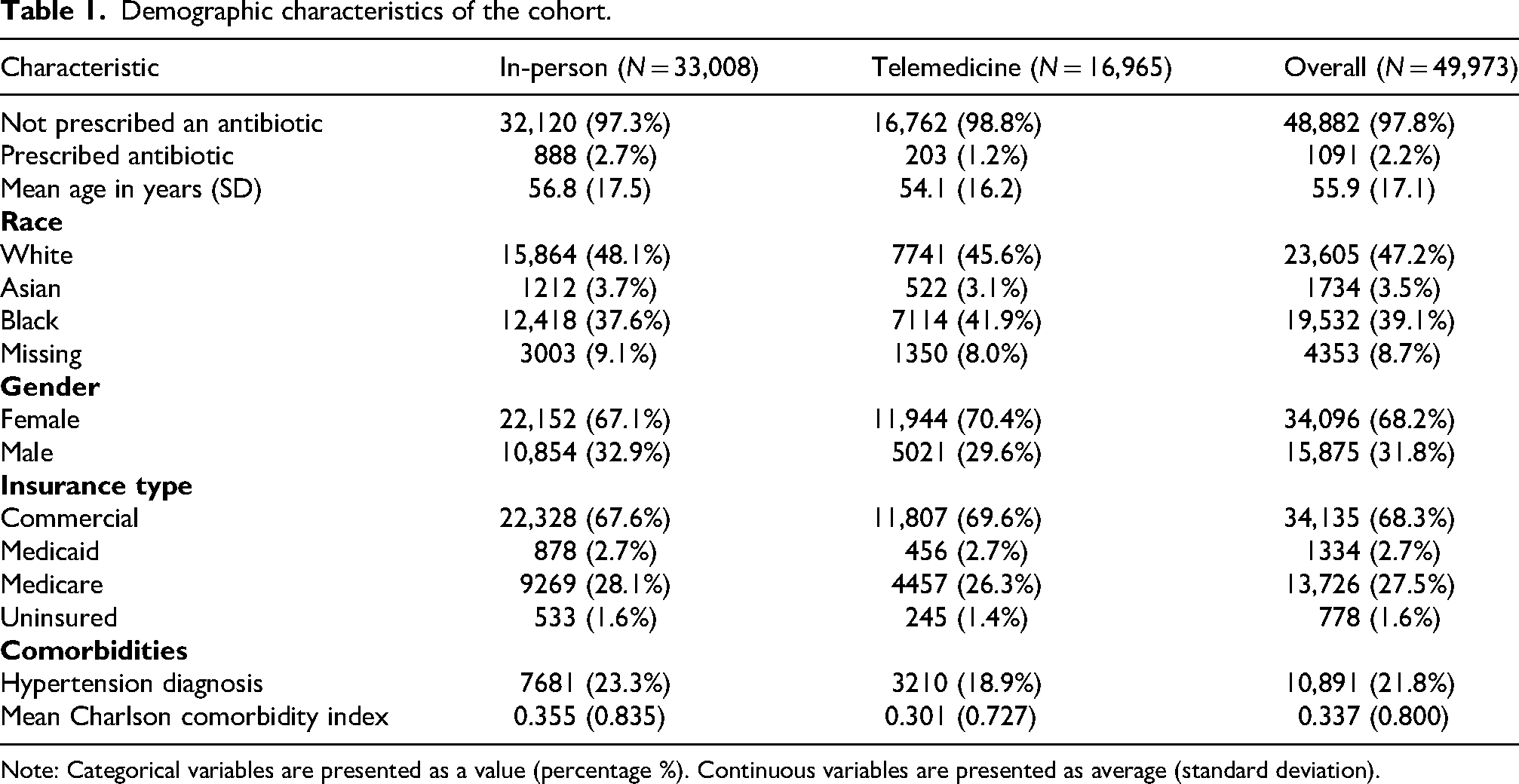
Note: Categorical variables are presented as a value (percentage %). Continuous variables are presented as average (standard deviation).
Table 2 shows the results of the unadjusted and adjusted multivariate logistic regression model. In the unadjusted model, there were significantly lower odds of antibiotics being prescribed in a telemedicine appointment (OR 0.44, 95% CI 0.37–0.51, P < 0.001). Patients with a higher Charlson Comorbidity Index were more likely to be prescribed an antibiotic (OR 1.17, 95% CI 1.10–1.23, P < 0.001). Compared to patients with private insurance, patients with Medicaid (OR 0.15, 95% CI 0.06–0.30, P < 0.001) and Medicare (OR 0.14, 95% CI 0.11–0.18, P < 0.001) were less likely to receive an antibiotic prescription.
Comparison of unadjusted and adjusted odds ratios for antibiotic prescription by visit modality, patient demographics, and clinical factors.
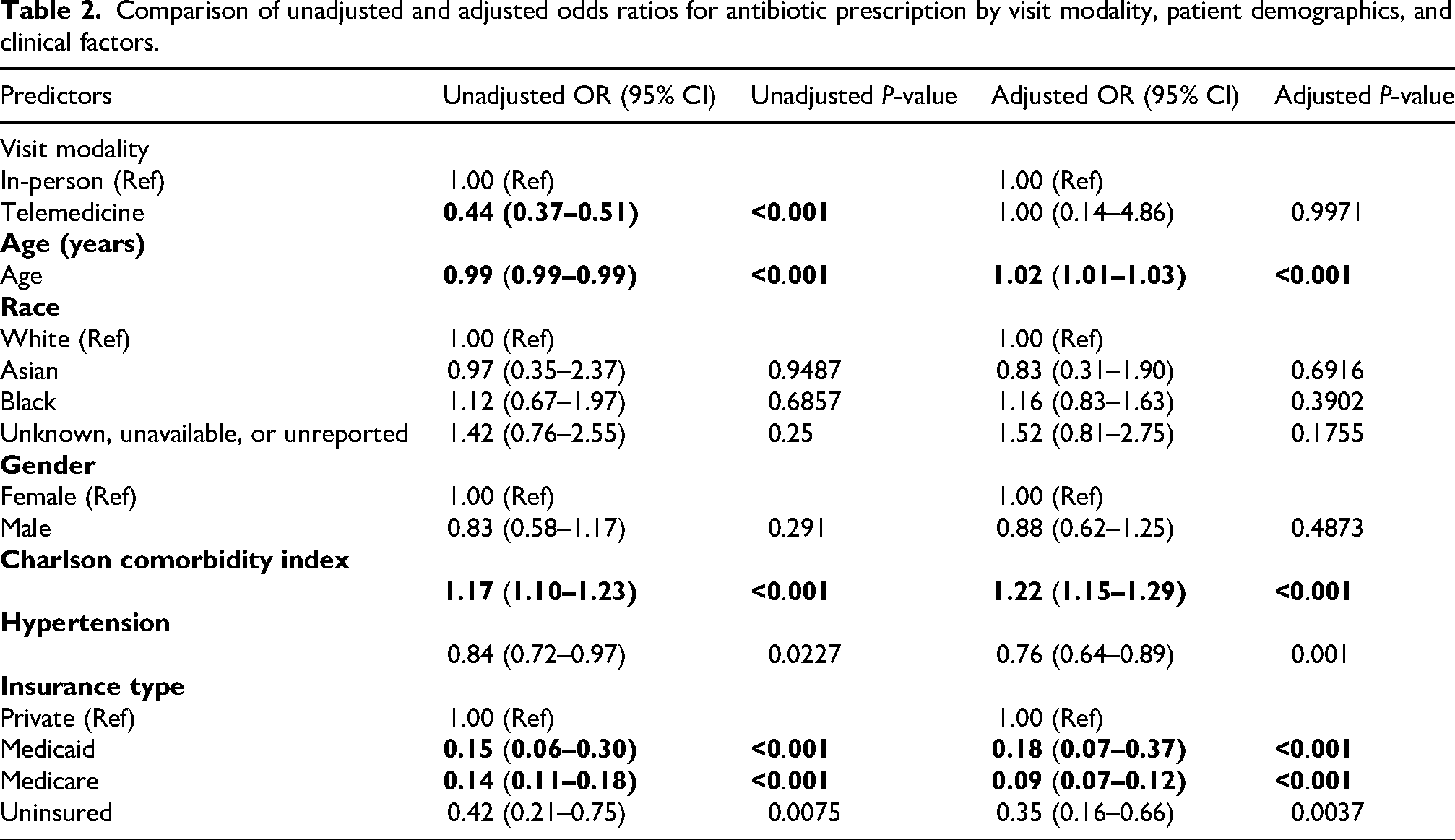
After adjustment, there was no significant difference in antibiotic prescribing between in-person appointments and telemedicine appointments. Older patients (AOR 1.02, 95% CI 1.01–1.03, P < 0.001) and patients with more comorbidities (AOR 1.22, 95% CI 1.15–1.29, P < 0.001) were more likely to receive an antibiotic prescription in the adjusted model. Patients with Medicaid (AOR 0.18, 95% CI 0.07–0.37, P < 0.001) and Medicare (AOR 0.09, 95% CI 0.07–0.12, P < 0.001) remained less likely than those with private insurance to receive antibiotics in the adjusted model.
Discussion
In this retrospective study of adult patients diagnosed with URIs and related symptoms at a large academic healthcare system, telemedicine visits did not significantly differ from in-person visits with respect to antibiotic prescribing.
Our finding that telemedicine visits do not differ from in-person appointments in antibiotic prescriptions contradicts our original hypothesis. This finding is similar to previous research. Two pre-covid studies found that antibiotic prescription rates were similar between in-person and telemedicine visits.26,27 However, one of these studies 26 reported that “Teladocs” were more likely to prescribe broad-spectrum antibiotics compared to in-office physicians. One contradicting study reported that antibiotic prescription rates were lower for telemedicine visits compared to in-office visits for respiratory infections. 14 Conversely, a paper conducted at Kaiser Permanente Northern California found that, overall, antibiotic prescribing is nearly equal between in-person and telemedicine primary care visits but varied by clinical concern. 27 Notably, the Kaiser study excluded URI as a diagnosis and examined other common clinical concerns for telemedicine.
It is notable that the antibiotic prescribing rates found in this study are much lower than national averages for primary care (∼75% in 2023). 28 However, a similar study examining antibiotic prescribing conducted at the same institution as our study also had a lower antibiotic prescribing rate than the national average (53.4%). 29 This previous study was conducted from 2015 to 2017, not encompassing the COVID-19 time-period like our study. A more recent paper also conducted in the Atlanta area focused on antibiotic prescriptions specifically for patients tested for COVID-19 30 (including patients with both negative and positive results), with an overall prescription rate of 6.7%, similar to the rate found in our study. Although our study excluded encounters for COVID-19-positive patients, we believe a combination of multiple factors has led to our low antibiotic prescription rate. These factors include utilizing data from a large academic healthcare system and the study period encompassing the COVID-19 pandemic, where antibiotic prescribing behaviors were increasingly cautious.
Limitations
Our study has significant strengths include a large sample size representative of a diverse patient population in a variety of practice settings. However, a few limitations must be acknowledged. Because our study is not a randomized trial, a causal relationship cannot be established. Patient characteristics between study groups are similar, decreasing the risk of selection bias. However, patients may choose whether to attend an in-person or telemedicine visit, creating more opportunities for selection bias. Furthermore, we had no way of knowing of any barriers patients may have faced in accessing telemedicine appointments (e.g., no home internet connection, no access to a device with audio and video capabilities, technology literacy issues, etc.).
Our data is solely from one large academic healthcare system in Georgia, Emory Healthcare, limiting generalizability on a national scale. We also lack detailed information on the duration and severity of symptoms, which is necessary to determine the appropriateness of antibiotic prescriptions. Relatedly, our inclusion criteria only captured encounters with a principal diagnosis related to URI, potentially missing visits where URI was addressed but another diagnosis was chosen as the principal. Finally, our extracted data from the EHR did not include information on providers (e.g., age, length of practice, degree type). These differences in providers could have an effect on prescribing behaviors and should be investigated in future studies.
Conclusions
Our study shows that there is no association between receiving an antibiotic prescription for an upper respiratory infection during a telemedicine appointment when compared with an in-person appointment in primary care. This finding supports that telemedicine and in-person appointments are comparable modalities of patient care regarding a key measure of healthcare quality in the outpatient setting. Additionally, we provided antibiotic prescription rates for common diagnostic codes associated with upper respiratory infections and demonstrated that antibiotic prescriptions greatly increased in the post-pandemic time period. Future studies should examine antibiotic stewardship during telemedicine appointments and how the appropriateness of prescriptions compares between the two visit modalities.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X261420387 - Supplemental material for Telemedicine versus in-person primary care visits for upper respiratory infections: Comparison of antibiotic prescribing
Supplemental material, sj-docx-1-jtt-10.1177_1357633X261420387 for Telemedicine versus in-person primary care visits for upper respiratory infections: Comparison of antibiotic prescribing by Lindsey Garrett, Zhuoyang Zhang, Julia Felrice, Julianne Gent, Ilana Graetz and Ambar Kulshreshtha in Journal of Telemedicine and Telecare
Supplemental Material
sj-docx-2-jtt-10.1177_1357633X261420387 - Supplemental material for Telemedicine versus in-person primary care visits for upper respiratory infections: Comparison of antibiotic prescribing
Supplemental material, sj-docx-2-jtt-10.1177_1357633X261420387 for Telemedicine versus in-person primary care visits for upper respiratory infections: Comparison of antibiotic prescribing by Lindsey Garrett, Zhuoyang Zhang, Julia Felrice, Julianne Gent, Ilana Graetz and Ambar Kulshreshtha in Journal of Telemedicine and Telecare
Footnotes
Abbreviations
Acknowledgments
Not applicable.
Authors’ information
The data in this article was presented at the 10th annual Health Services Research Day on May 7, 2024, by JF at Emory University Rollins School of Public Health and won the first-place award for the oral presentation category.
Ethics and consent to participate
This study was granted a waiver by the Emory Institutional Review Board, as patient data was deidentified before data analysis.
Consent for publication
Not applicable.
Authors’ contributions
LG was the major contributor to drafting and revising this manuscript. JF conducted data analysis and interpretation as well as contributed to drafting the Methods and Results section of the manuscript. JG assisted in data acquisition and conceptualizing the aims of the paper. ZZ contributed to data analyses and created all tables. IG contributed to data interpretation and revision of the Discussion section. AK supervised all work as the primary investigator. All authors read and approved the final manuscript.
Funding
Dr Kulshreshtha is supported by his NIH K23(AG066931) Grant. This work is also supported by two NIH grants (1R01CA262312 and R01CA218155) awarded to Dr Graetz, as well as funding from Prime Education, LLC. Dr. Graetz also received research grants from Donaghue Foundation and Pfizer.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.