
Abstract
Background
Navigating the healthcare system is complex. Care fragmentation is a major issue. Patient navigators have emerged to improve care continuity, especially for vulnerable individuals. With digital health expansion, digital navigator (DN) roles have been created to foster digital literacy, access and equity.
Objectives
To identify DN's roles in reducing health inequities and examine its terminology, professional background, training, techniques, skills, communication methods and outcomes.
Methodology
Systematic review across five databases. Data extraction included DN characteristics and outcomes. Thematic analysis compared expectations and findings.
Results
Sixteen studies were reviewed. Findings suggest that the DN may help reducing inequities in healthcare access, though it is not guaranteed. Gaps were found in DN roles, competencies, training and terminology. Most studies emphasised technical support, communication and clinical integration, with limited focus on social issues. Disparities were noted between expected and reported roles.
Conclusion
The DN role shows promise, especially in fragmented systems, but remains underexplored. Current approaches emphasise technology over social support. Broader understanding and implementation are needed.
Keywords
Introduction
Navigating a health system to seek care can be complex and overwhelming. To support patients in their journey, patient navigation (PN) emerges in the 1990s in the USA and Canada, to improve cancer screening in vulnerable populations. 1 PN has been defined as an individual or team who perform specific activities to facilitate patients, families and caregivers access to healthcare and social services, promoting continuity of care by removing barriers and ensuring efficient use of the healthcare system. 2 PN aims to bridge gaps in healthcare and reduce access barriers for clinically, socially and/or medically complex patients, acknowledging the relationship between health and social care, and the negative impact of fragmentation.1,2
Patients requiring navigation services often have complex needs and seek multiple specialists’ care, besides having repeated interactions with services, requiring referrals, adopting different modalities of care, and are often homebound, facing communication issues, or needing mental health or pain management support.3,4
In high-income countries, PN has been associated with optimised cancer diagnosis, treatment adherence and positive outcomes, especially in vulnerable populations. 5 Despite that, it remains palliative as causes of unsuccessful coordination and integration of care still need to be addressed. 2 Lack of clarity around the need for a PN, or its workflow, roles or responsibilities, results in diverse designs and targeted populations, reflecting diversity in current models of care. 2
The COVID-19 pandemic highlighted social and health inequities, access issues, fragmentation and lack of coordinated care. While digital health is a promising solution, its implementation can reinforce, exacerbate or even create new inequities, 6 disproportionately affecting underserved groups, such as those from low socioeconomic background, low digital literacy, culturally and ethnically marginalised. This reflects existing social inequities in digital health access, use and literacy.7,8
Digital navigators (DN) emerge in 2019 as a strategy to enhance and facilitate use and access of digital health technologies and services for continuous care. 9 Those include video consultations, remote patient monitoring, mobile health apps, wearables, electronic health records and medical artificial intelligence. 10 As digital healthcare emerged, the concept of ‘end-users’ will be adopted in this paper instead of ‘patients’ to name informed and active participants in managing their own health through digital means. 11
DN has been described as individuals or groups that offer technical and/or psychosocial support in implementing digital technologies in healthcare.12–15 They might be a clinician, medical assistant, nurse, case manager, peer specialist, admin staff or someone from the community with specific expertise in digital health.12,14
Aiming to expand care reach, provide technical support and integration of clinical, administrative, technical workflows, DN has had positive outcomes.9,14 For instance, a DN program in Boston reported increased enrolment rates in health web portals among Black and Hispanic populations. 16 While DN does not address structural issues, it aims to evolve with technology and potentially reduce healthcare barriers. 13
DN is a potential education strategy on the use of mobile health apps. 8 Other related responsibilities of this emerging role include evaluation, installation and troubleshooting apps and data collection, allowing healthcare professionals to focus on clinical issues. 15 Broad DN responsibilities include identifying user's eligibility for the technology, training on platform use, technical support and monitoring outcomes. 17
Additionally, DN may increase equitable healthcare access by offering targeted and personalised services that boost engagement, digital literacy and care integration.9,12–15 Addressing digital inequities is challenging, particularly considering complex overlaps of multiple layers of discrimination, shaped by social, power, demographic, spatiality and cultural intersectionality. 18 It is necessary to examine how individual characteristics, including race, gender, income, age, education, place of residence and migrant status, are related to access and use of digital health modalities, considering such association exists in health services in general. These findings can guide the development of urgent digital equity policies in healthcare. 8
Defining DN's role involves outlining its scope of practice, competencies and target problems to which it aims to address. Although DN is increasingly adopted worldwide, its competencies and responsibilities vary widely across healthcare settings and systems. This review aims to identify the role of DN in reducing healthcare inequities. Secondary objectives included summarising terminology used to describe DN, former occupation of the professional who became a digital navigator, required training, used techniques, skills, methods of communication and related outcomes.
Methods
A systematic review of literature was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and checklist (Supplemental Material 1). 19 The protocol for this review was registered at the Open Science Framework (https://osf.io/u3gzx/).
Search strategy
We adopted the PICo strategy 20 to frame our research question and define search strategies for the following databases: PubMed, Embase, CINAHL, Web of Science and EBSCO PsycInfo (Supplemental Material 2). Our targeted population (P) were adults, our phenomenon of interest (I) was DN and the context (Co) was digital health inequities. Searches were conducted in September 2024 with no restriction on publication period.
Eligibility criteria
Included articles were original studies in English, Portuguese and Spanish, exploring the role of DN to support the use of any modality of digital healthcare, including telehealth (telephone and video consultations), mobile health apps and web health portals.
Articles not referring to DN as individuals (e.g. AI system) were excluded. Studies describing DN services targeting healthcare professionals, exclusively theoretical or not mentioning health inequities were also excluded. Posters, abstracts, editorials, commentaries, literature reviews and opinion pieces were all excluded.
Screening and data extraction
References were screened using Covidence online platform. After removing duplicates, three reviewers (X, Y and Z) screened the references by title/abstract followed by full-text, each with two votes. Conflicts were solved during virtual meetings between reviewers. Manual inclusions were made based on the reference list of screened articles.
A data extraction spreadsheet was developed according to the research question, including study characteristics (author, year, country, study design, objectives, participants, sample size, health specialty, targeted condition, context of the problem and limitations) and DN characteristics (terminology, definition, roles, qualifications, training, description of the DN intervention, means of communication, goal-setting techniques, outcomes and challenges). In terms of the DN roles, techniques and skills applied; and expected outcomes to promote equity, a categorisation was developed summarising the main findings of five theoretical articles (Table 1).12–15,17
Digital navigator (DN) roles, applied techniques and equity-expected outcomes categories.
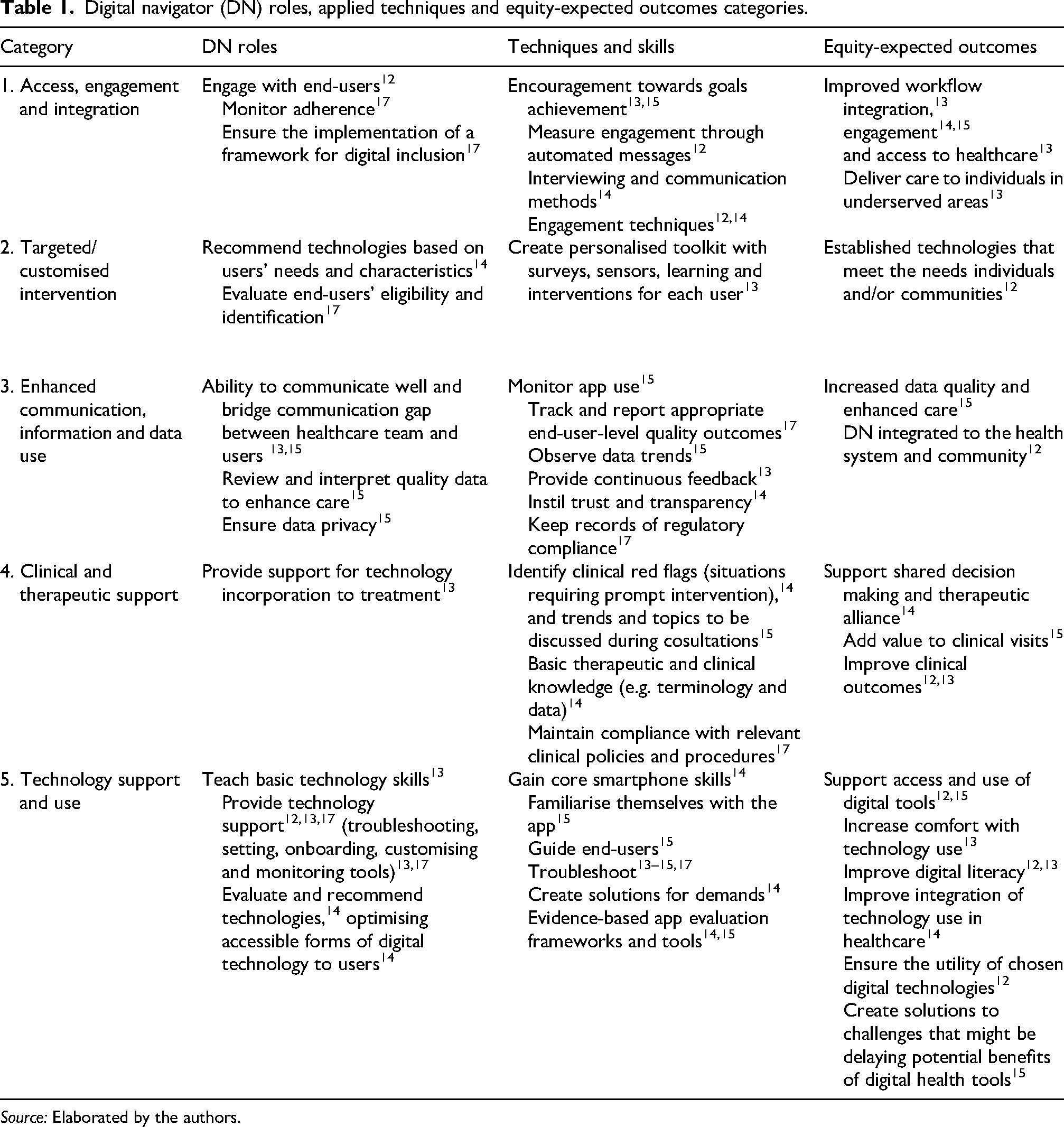
Source: Elaborated by the authors.
Data analysis
After finishing data extraction, each column of the spreadsheet was checked for consistency. Quantifiable aspects of DN (terminology, role, outcomes, training, means of communication and professional background or job title) were summarised and reported using frequencies and percentages. Qualitative findings were thematic synthesised. 21 A comparison between expected categories described in Table 1 and the findings from included studies was performed and a summary was cross-tabulated into five categories: (1) access, engagement and integration; (2) targeted/personalised intervention; (3) enhanced communication, information and data use; (4) clinical and therapeutic support; and, (5) technology support and use; under each of the three DN characteristics: (1) DNs roles; (2) techniques and skills; and, (3) equity-related outcomes. It is important to note that these categories encompass a wide range of activities attributed to DN in the reviewed literature, including functions that may extend beyond its core scope. These variety of activities were retained to comprehensively capture how digital navigation has been operationalised across current studies. Discrepancies in category allocation or description were discussed and adjusted during online meetings.
Quality assessment
Quality assessment of included studies was conducted using SQUIRE 2.0 (Standards for Quality Improvement Reporting Excellence), a guideline that provides a structured framework to improve transparency, completeness and accuracy of reporting for studies that describe interventions to improve the quality, safety and value of healthcare. 22 We attributed one point to each of the 18 SQUIRE categories, and zero if they were absent. The assessment was completed by the lead author (X) and uncertainties were discussed virtually between the authors (X, Y and Z). The higher the final SQUIRE 2.0 score, the better the reporting quality of included studies (maximum of 18).
Results
The search retrieved a total of 3521 references and 1641 duplicates were removed. The screening process is illustrated in Figure 1. Sixteen studies were reviewed.
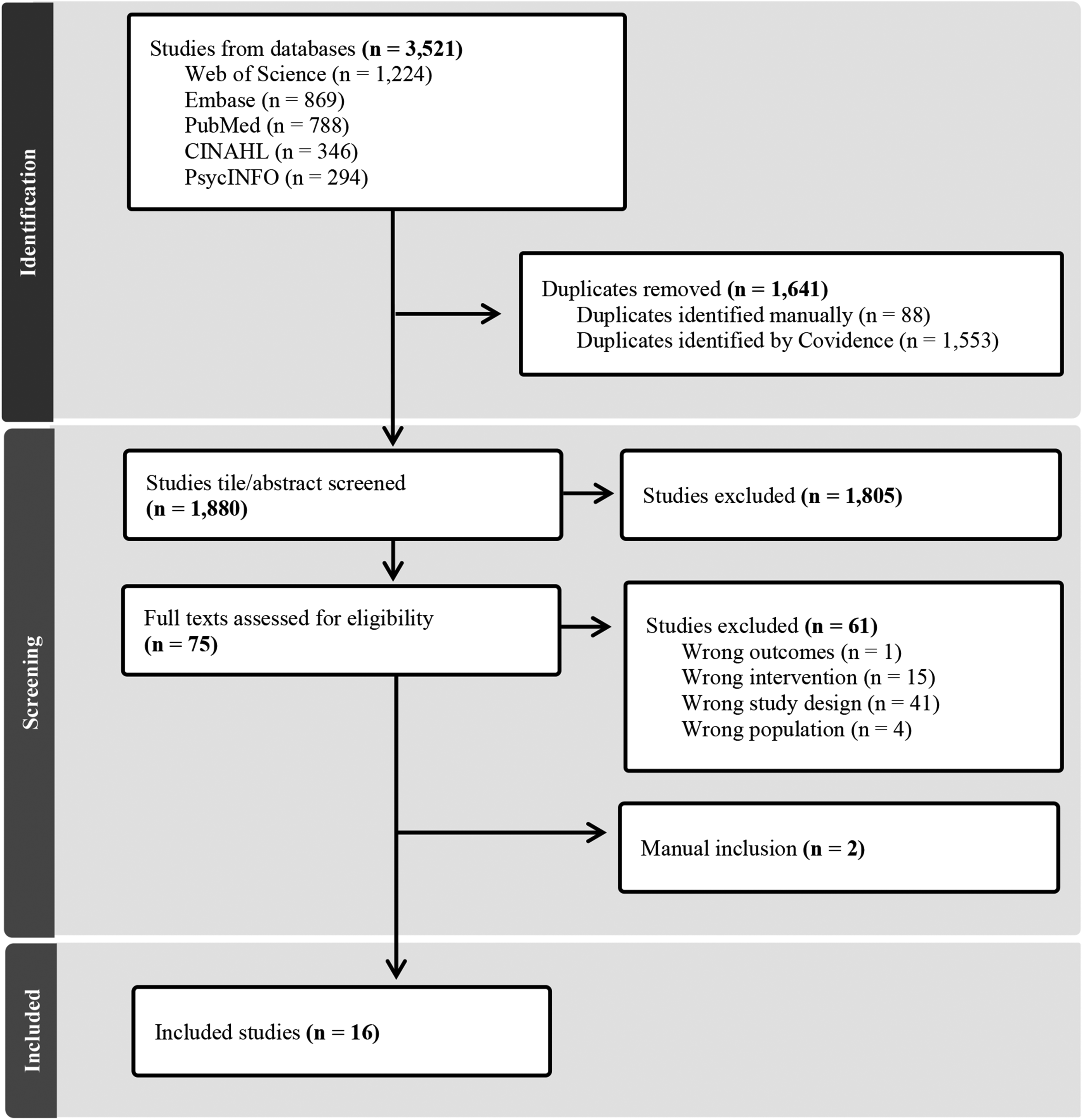
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart diagram of identification, screening and inclusion process.
Study quality
Assessment of the studies using SQUIRE 2.0 22 has revealed a mean score of 16.94 out of 18. Ten studies (62.5%) scored 18, three (18.7%) 17 and the remaining three (18.7%) between 13 and 14. The most common reason for lower scores was unclear disclosure of ethical considerations (31.25%).
Study characteristics
Included studies have primarily focused on mental health (depression, anxiety, psychosis, behavioural change and general mental health),23–30 HIV,31–33 gerontology,34,35 type 2 diabetes,16,29 cardiovascular 36 and oncology care. 37 One study (6.2%) was conducted in Canada, whereas the remaining 15 (93.8%) were from the USA. Most studies (81.2%) were published after 2020. A summary of included studies is shown in Table 2.
Summary of included studies (n = 16).
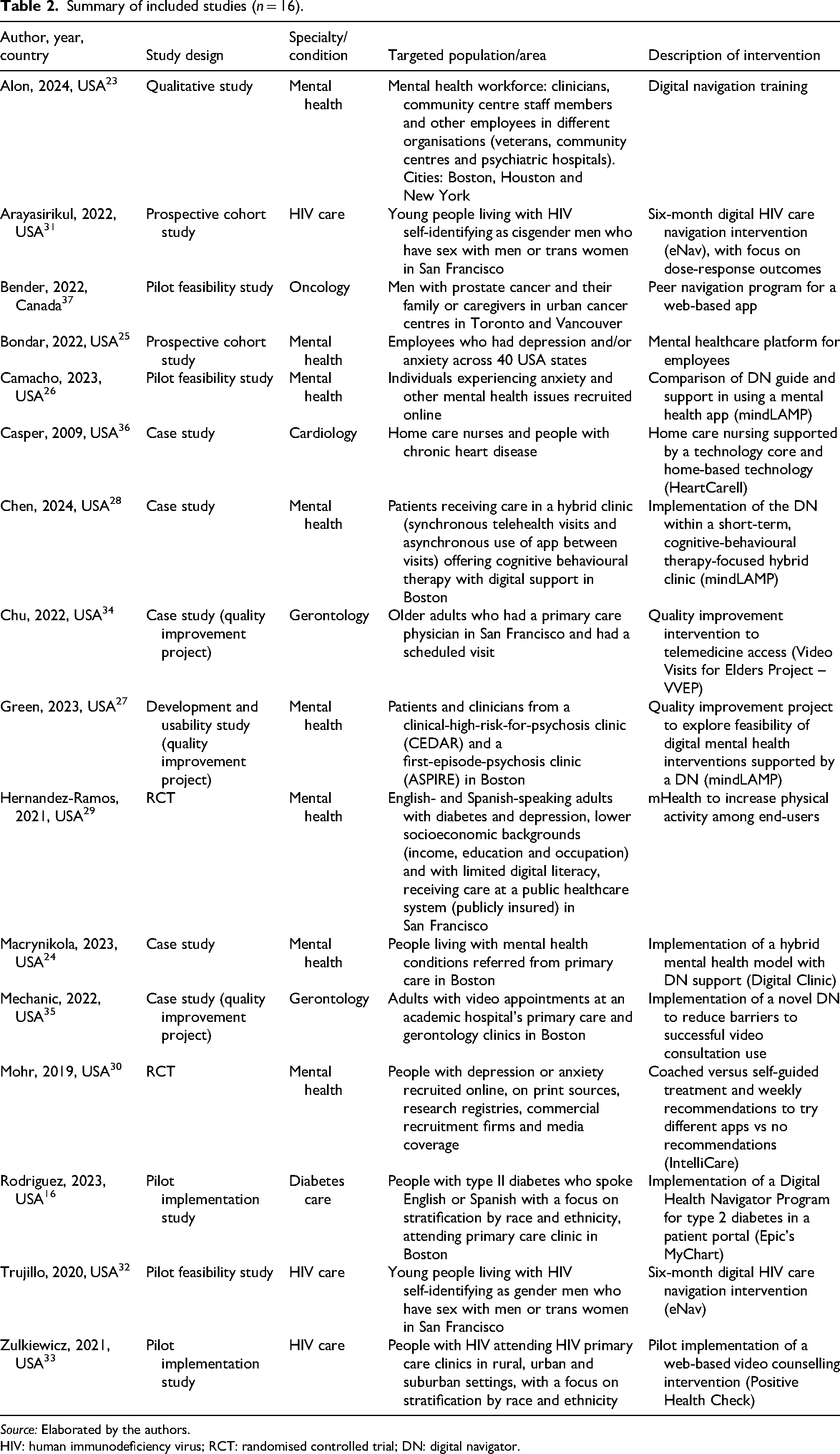
Source: Elaborated by the authors.
HIV: human immunodeficiency virus; RCT: randomised controlled trial; DN: digital navigator.
Eight studies (50.0%) used either the term digital navigator,23,24,26–28 digital care navigator31,32 or digital health navigator 16 to refer to the team member supporting technology implementation for patient care. Seven (43.7%) studies have used a variety of terminologies: some more specific to the technology or intervention (technical assistance,33,36 telehealth patient navigator 35 or VVEP team 34 ), others related to the navigation (peer navigator 37 or care navigator 25 ) and others more broad (coach 30 ). One study did not assign a specific name to refer to DN. 29
Training was mentioned in half of the studies (50.0%), with the duration varying from 6 35 to 10 h,24,26,28 1 day 23 or 6 weeks. 37 Training content covered basic technology, digital literacy (62.5%),16,23,24,26,27 specific skills of the tool used (87.5%)16,23,24,26–28,35 and DN-specific competencies and techniques (87.5%),16,23,24,26–28,37 such as outreach ability and organisational awareness. Two studies (25.0%)24,28 have described training based on the simulation or observation of DN in practice.
Modalities of digital healthcare included mobile apps (43.7%),24,26–30,36 web or online programs (25.0%),16,25,33,37 telehealth (12.5%),34,35 SMS text-messages (12.5%)31,32 and one study (6.2%) described DN training without specifying the modality. 23 Communication between digital navigators and end-users included text-messages,16,26,29–32,37 phone16,25,29,30,35 and video calls,25,29,34 e-mail, 37 pager, 16 letters 16 and in-person.16,33 Five studies23,24,27,28,36 did not specify any means of communication. DN roles were performed by research assistants16,23,26 or coordinators, 34 clinicians,25,27 community healthcare workers, 23 other health staff,23,24,27 medical students, 34 volunteers,23,28 peers 23 or tech-smart individuals. 24 Eight studies29–33,35–37 did not specify the professional background of navigators.
Table 3 summarises the main aspects of the DN that could be quantified as either present or not (DN terminology, DN role, DN-related outcomes and DN training) or details of how they were described (mean of communication and DN professional background or job title).
Summary of quantifiable digital navigator (DN) aspects included in the original articles (n = 16).
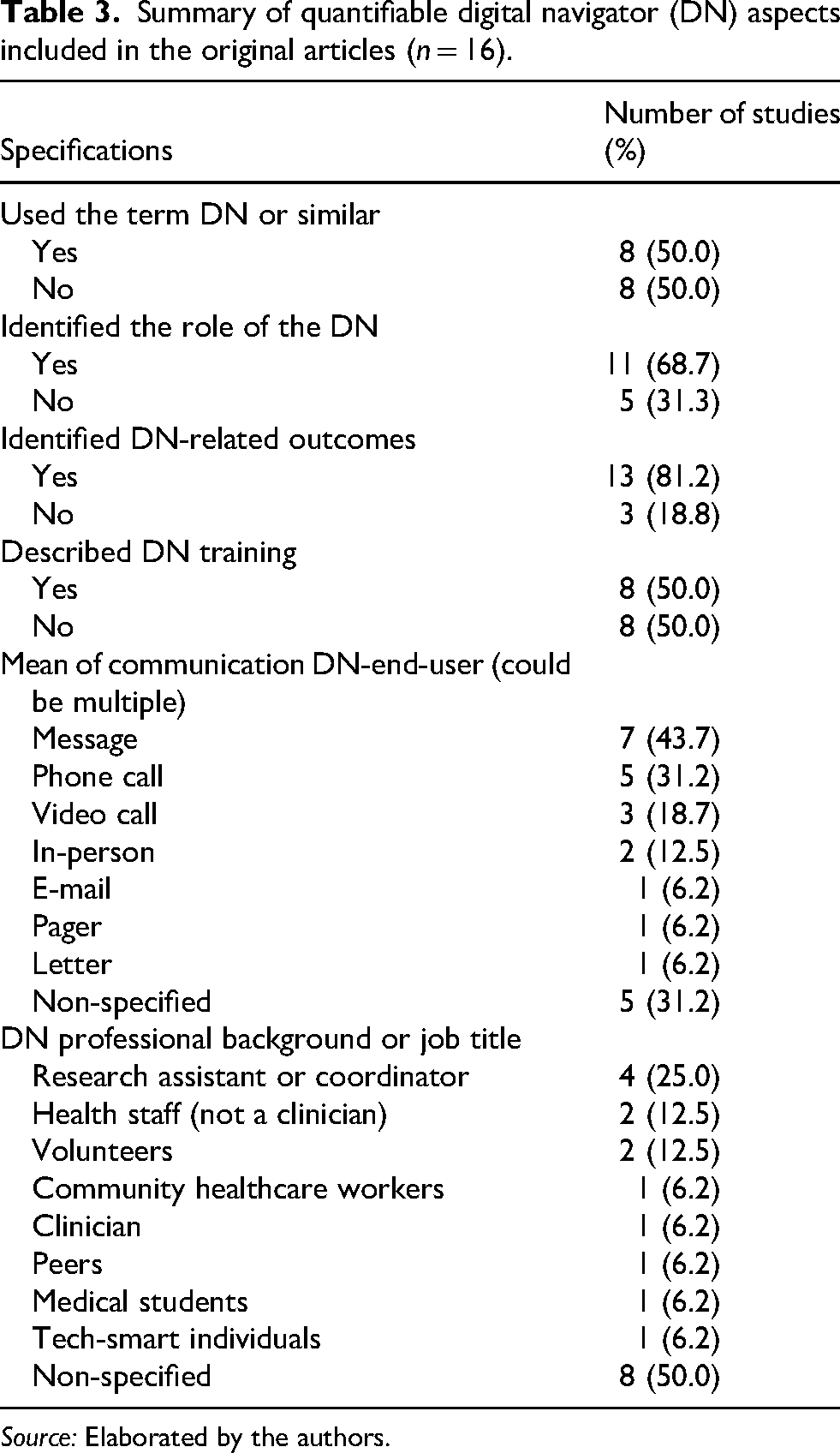
Source: Elaborated by the authors.
The roles described in 11 studies (68.7%),16,23–28,31,32,34,37 as well as the techniques described in 12 (75.0%),16,24,26,28–35,37 and equity outcomes reported as directly related to DN’ practice in 13 (81.2%),16,23,26–35,37 were organised in Table 4, following categories created in Table 1.
Summary of DN roles, applied techniques and skills, and equity-expected outcomes extracted from included studies (n = 16) and classified according to categories from Table 1, including the number of articles reporting each category.
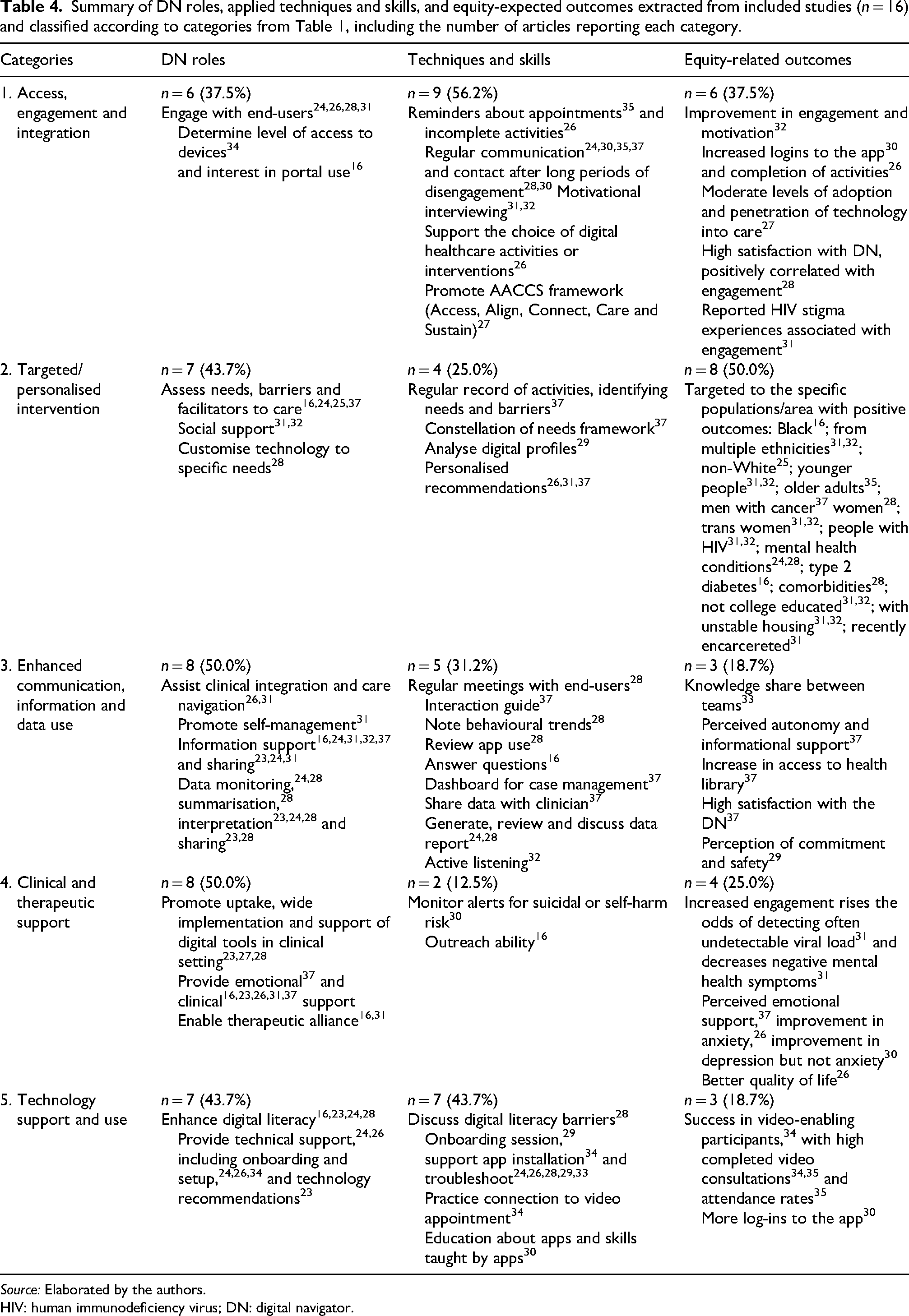
Source: Elaborated by the authors.
HIV: human immunodeficiency virus; DN: digital navigator.
Is the DN contributing to reduce health inequities?
DN roles in the included studies focused primarily on providing technical and clinical support, utilising data to leverage clinical practice, promoting intervention engagement and assessing individual health and digital needs. When comparing this review's results (Table 4) to potential expectations of a DN described in existing non-empirical (theoretical) literature (Table 1), contributions exceeded expectations, particularly under ‘Clinical and therapeutic support’, presenting roles beyond technology incorporation to treatment, such as emotional 37 /clinical16,23,26,31,37 support and therapeutic alliance.16,31 Both social31,32 and tailored technology support 28 were roles described in included studies under ‘Targeted and customised intervention’ not described in the literature. Under ‘Enhanced communication, information, and data use’, included studies failed to mention DN role in ensuring data privacy, but highlighted DN's performance in promoting data use for self-management. 31 Regarding ‘Technology support and use’, one important addition was the role of DN in improving end-users’ digital literacy.16,23,24,28
Techniques and skills used by DN had gaps and additions in all categories when comparing the methods – Table 1 and results – Table 4. Some gaps were therapeutic and clinical knowledge, documentation and policies compliance, personalised toolkits and encouragement towards goals. However, some techniques not mentioned in the literature, such as discussing digital literacy barriers, 28 outreach ability, 16 active listening, 32 regular meetings with end-users, 28 recording activities, 37 and identifying needs, 37 barriers28,37 and digital profiles 29 were reported as techniques and skills used by DN in the included studies. When relating these techniques to Behaviour Change Techniques (BCTs), they mostly fall under the ‘goals and planning’ and ‘feedback and monitoring’ categories – problem solving, goal setting and monitoring of behaviour. BCTs are components of an intervention that are designed to alter behaviour by targeting its underlying determinants, allowing interventions to be clearly specified, replicated and evaluated.38
For equity-expected outcomes, ‘Clinical and therapeutic support’ mostly described mental health outcomes while ‘Access, engagement and integration’ mostly described engagement-related outcomes. There were insufficient outcomes in included studies when comparing methods – Table 1 with what was achieved by DN (results – Table 4). For instance, no studies evaluated DN's performance in optimising shared-decision making, data quality, self-management, workflow integration or care delivery in underserved areas. However, a few outcomes not listed in the literature (emotional 37 and informational 37 support, access to health library 37 and satisfaction with DN 37 ) were identified in the included studies. Figure 2 synthesises the DN roles, techniques and skills associated with positive outcomes in the included studies.
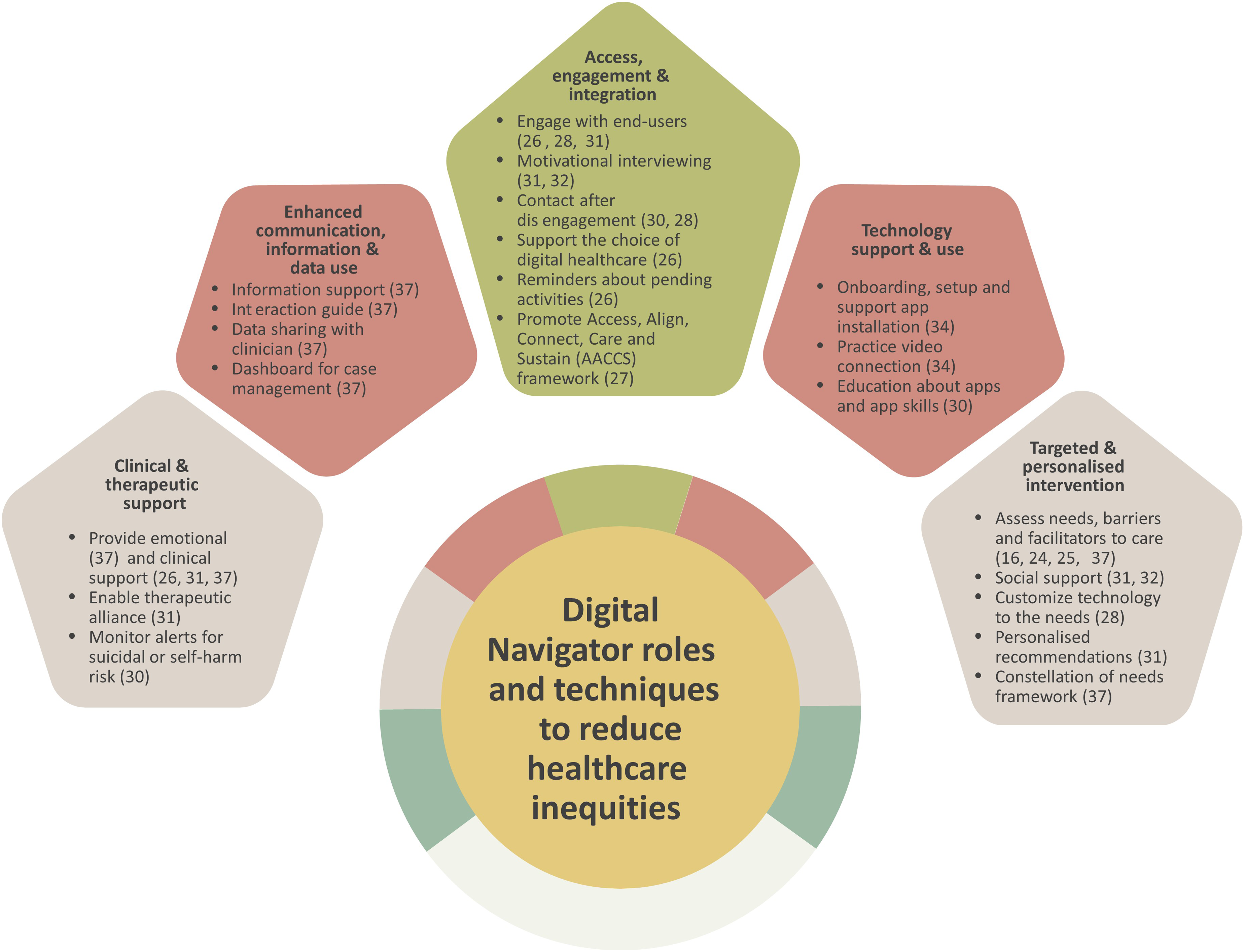
DN roles, techniques, and skills associated with positive outcomes in included studies.
Perceptions from targeted populations described in the studies were also not listed in Table 1. A few end-users receiving cognitive behavioural therapy in a hybrid clinic (i.e. synchronous telehealth and asynchronous mobile app) felt supported, and reported positive experiences and new skills gained. 28 They also viewed the digital intervention as a good way to access care. 28 End-users receiving digital HIV care navigation described a community sense, better medication tracking, less missed appointments and support to talk to clinicians. 32 Despite having DN available, challenges with the technology were still mentioned. 27
Discussion
Our results suggest that DN has the potential to reduce healthcare inequities. Most studies analysed have primarily examined their role in supporting technology use, increased communication and clinical integration, often neglecting how social factors impact integration of care across the health system. These were expectations described in literature, which demonstrates a gap in studies that tested DN role in overcoming socioeconomic barriers to promote integrated care, highly relevant when attempting to reduce healthcare inequities.
Our findings also demonstrate a gap in DN scope of practice, including clear roles and competencies. Heterogeneity in DN characteristics was found across studies, including training, background, qualifications and terminology adopted. Eight different names were reported across included studies. Other terms to describe similar interventions such as phone navigator, 39 human support 40 or technology specialist 41 are reported, with differences. For example, when compared to a coach, DN has been described as ‘more engaged approach, […] which seeks to integrate more aspects of care’. 42 Inconsistent terminology makes the search for relevant studies a challenge, and hinders the development of a consistent scope of practice, with appropriate roles and training.
Other reviews of DN in mental health focused on motivation, engagement, treatment adherence, technical and clinical support, access and feedback,40,42,43 aligned with our study findings. Including DN as a part of the staff has also been described as improving telehealth adoption, adaptation, effectiveness and satisfaction.44 When tracing back to the origins of PN (bridge gaps in cancer prevention and treatment) 1 and care navigation (guiding individuals in the health continuum beyond healthcare),45,46 essential components, such as providing service information 39 to support care journeys appear to be missing. Many techniques depicted aimed mostly to engage end-user's with the intervention or technology, particularly troubleshooting, similar to what has been reported previously.39,40,42,43 At this point, it remains unclear whether the primary purpose of DN is to bridge the gap between end-users and health services using digital health tools or, alternatively, and not additionally, to focus on bridging the gap between end-users and digital healthcare tools themselves, increasing digital health use and adoption.
Besides, a core DN skill when the goal is to reduce inequities, is cultural competence, 39 widely neglected in the included studies. Cultural competence is essential to ensure improved outcomes, enhance communication, increase satisfaction, 47 provide appropriate quality care to different groups and reduce health inequities. 48 Study findings show a cultural competency training is perceived as beneficial by participants. 44
Training programs for DN in our findings focused solely on technical, operational and clinical skills, offering no attention to the social dimensions of the role. Basic smartphone use and troubleshooting, mobile app assessment tools, clinical terminology, data knowledge and engagement techniques13,14 were mostly outlined, but rarely detailed. There was insufficient description of the essential skills for DN, despite the existence of evidence-based manuals14,49 outlining a curriculum for effective DN training.
Eight studies targeted DN interventions to specific populations, focusing on equity-related outcomes, 16 such as workflow integration, 13 care delivery in underserved areas 13 and integration of DN into systems. 12 Again, care navigation appears overlooked, with limited attention to care integration, social and cultural factors impacting health equity and access.
Other findings referring to DN's reach, beyond closing access disparities and promoting digital literacy and integrated care, highlight the temporary or transitional role of DN in supporting the uptake of digital technologies. 26 Once individuals become proficient in using digital health tools, they tend to rely less on DN. In contrast, some authors present DN as a figure who can become a permanent point of reference for end-users. 37 While additional strategies in DN practice may help mitigate digital barriers, they are unlikely to eliminate those entirely. 29 In this sense, having DN scope of practice aligned with healthcare equity goals 16 seems reasonable to sustain positive impact and better outcomes.
Nearly all studies reported DN interventions developed in the USA, where access challenges and healthcare fragmentation persist 50 despite advanced technology and substantial investments. If DN is widely developed in this context, it becomes critical to prioritise equity over technical support to promote healthcare integration. Besides, included studies hardly presented population size, socioeconomic status and availability of local health services, essential characteristics to fully understand healthcare inequities. Most included studies focused on metropolitan areas,16,23,27–29,31,34,35,37 while others did not specify the location, relying on virtual recruitment.26,30 Considering the incipient nature of DN, these initiatives may not yet have been extended to more marginalised populations or rural and remote regions. Our findings suggest that it may be particularly worthwhile to explore the development of DN initiatives in countries or regions with fragmented systems or limited access to healthcare.
Studies using virtual recruitment should also outline geographical coverage, not only to provide an overview of the population and needs, but also to allow identification of appropriate referral destinations. There is no one-size-fits-all approach for DN interventions and, despite the need for clarity in their scope of practice and training, adapting it to individual and local needs which vary geographically, culturally and regionally, is also in its core competencies.
The rapid development of digital health has evidenced and reinforced persistent health inequities, underscoring the importance of investing in integrated health systems and careful designing digital healthcare with strong focus on equity.8,51 Multilevel efforts should be coordinated to address health inequity, especially regarding digital disparities, with involvement from government, industry and, the entire healthcare team including DN. An intersectoral approach, such as providing digital health education and facilitate access to devices and internet connection, can foster greater digital inclusion. 16
Strengths and limitations
This study summarises latest findings on DN roles and characteristics without restricting the analysis to a specialty or health condition, an approach not previously undertaken. The focus of DN in addressing health inequities remains underexplored, and this article may open pathways for future research, which may include other related aspects such as digital engagement and motivation.
Some limitations should be acknowledged. Terms such as ‘coach’ and ‘human support’ were not part of the initial search and were instead identified during screening, which could have resulted in the exclusion of some relevant studies; with manual inclusions adopted to mitigate this. Additionally, the emerging nature of the topic limits the number of available studies, evidencing inconsistent terminology, which poses challenges for comprehensive search and synthesis. Consequently, the findings contribute to addressing the main research question, although inconclusively, which leaves room for further investigation.
Conclusion
This review found a gap in the literature when it comes to the role of DNs to reduce healthcare inequities, an emerging topic. Despite the promising potential of DN, studies describing DN interventions with focus on reducing inequities were incipient. Having an individual or a group supporting the integration of digital healthcare modalities and system navigation is particularly relevant when fragmented care is in place and in countries or locations marked by deep or growing social and health inequities. The literature supports the relevance of DN, which appears diverse and multifaceted, with heterogeneous professional practice, training, techniques, skills and outcomes. However, current implementation remains strongly focused on technological aspects, with less attention to social support and healthcare integration. Our findings suggest that although DN holds promise, there is still a lot to be developed and investigated to fully understand its potential, sustainability and limitations. Focusing on social and cultural factors to reduce barriers to care seems to be the best approach to optimise DN applications and benefits.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X261457758 - Supplemental material for Can digital navigators help reduce inequities in healthcare? A systematic review
Supplemental material, sj-docx-1-jtt-10.1177_1357633X261457758 for Can digital navigators help reduce inequities in healthcare? A systematic review by Giulianna Ornellas, Mariana Vercesi de Albuquerque and Soraia de Camargo Catapan in Journal of Telemedicine and Telecare
Supplemental Material
sj-docx-2-jtt-10.1177_1357633X261457758 - Supplemental material for Can digital navigators help reduce inequities in healthcare? A systematic review
Supplemental material, sj-docx-2-jtt-10.1177_1357633X261457758 for Can digital navigators help reduce inequities in healthcare? A systematic review by Giulianna Ornellas, Mariana Vercesi de Albuquerque and Soraia de Camargo Catapan in Journal of Telemedicine and Telecare
Footnotes
Ethical considerations
This article does not contain any primary data with human or animal participants, and informed consent is not required.
Funding
The authors disclosed receipt of the following financial support for the research and authorship of this article: This work was supported by the Coordination for the Improvement of Higher Education Personnel – Brazil (CAPES) [Funding Code 001].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.