
Abstract
Virtual urgent care (VUC) has become an increasingly utilized resource for acute care delivery. Frequent utilization of VUC may reflect unmet longitudinal care needs and contribute to fragmented care. While high-utilizer patterns are well described in emergency departments, they have not been systematically characterized in telemedicine. We evaluated a clinical decision support (CDS) nudge designed to identify and address high utilizers of VUC at a large academic health system. An electronic health record alert triggered when patients met predefined high-utilizer criteria (>3 visits in 30 days, >12 in six months, or >20 in 12 months) and prompted providers to document a structured follow-up plan using a SmartPhrase. Among 473 eligible patients, 162 (34%) received the SmartPhrase. After adjustment for baseline utilization using negative binomial regression, SmartPhrase use was associated with a 22% relative reduction in VUC visits over the subsequent 30 days (incidence rate ratio 0.78, p = .03). Bootstrapped analyses confirmed a significant reduction in the SmartPhrase group (−1.47 visits; 95% CI [−2.19 to −0.62]), while no significant change occurred in the comparison group. These findings suggest that a low-cost, workflow-integrated CDS nudge may reduce short-term telehealth overutilization by prompting structured follow-up discussions and encouraging longitudinal care planning.
Plain language summary
Virtual urgent care (VUC) allows patients to see a healthcare provider online for urgent concerns. It has become a common and convenient way to receive medical care. However, some patients use VUC repeatedly for ongoing issues that may be better managed through regular primary care. This repeated use can lead to fragmented care, higher healthcare costs, and unresolved health problems.
In our health system, we noticed that a small group of patients accounted for a large number of virtual urgent care (VUC) visits. To better support these patients, we created a simple electronic alert in the medical record. When a patient met certain “high-use” criteria, the system nudged the provider to discuss follow-up care and document a plan in the visit note.
We studied whether this nudge made a difference. Among patients whose providers used the follow-up discussion prompt, VUC visits decreased by about 22% over the next 30 days. In contrast, patients whose providers did not use the prompt did not experience a decrease in visits. This suggests that a brief, structured conversation about ongoing care may help reduce repeated urgent visits.
Importantly, this intervention was low-cost and easy to implement. Rather than limiting access to care, it encouraged providers and patients to think about longer-term solutions. As virtual care continues to expand, simple nudges like this may help ensure that patients receive the right care in the right setting.
Keywords
Introduction
Frequent utilization of telemedicine for recurring concerns can lead to fragmented care 1 and increased healthcare costs. 2 Although VUC services are ideally positioned to reduce unnecessary emergency department (ED) visits—especially given that an estimated 3–10% of ED visits could be conducted via telehealth 3 —a separate challenge persists: patients may turn to VUC repeatedly for ongoing issues that could be more appropriately managed through longitudinal primary care. 4
High-utilizer patterns are well described in EDs, 5 where a small proportion of patients account for a disproportionate share of visits, often driven by unmet longitudinal care needs. However, this behavioral pattern has not been systematically characterized in VUC—a rapidly expanding and now ubiquitous modality of healthcare delivery. 6 With over 400,000 VUC encounters across five years on our platform, we observed a similar high-utilizer phenomenon emerging in the telemedicine setting. Identifying and addressing this pattern is essential as health systems increasingly rely on telehealth as a front door to care.
To our knowledge, this is the first study to formally describe high-utilizer behavior within a VUC platform and to evaluate a targeted intervention to address it. We present a novel, low-cost, high-impact clinical decision support (CDS) approach designed to prompt structured provider intervention at the point of care. At NYU Langone Health, a CDS nudge was developed to identify high utilizers, encourage providers to review prior visits/treatment failures and initiate discussions with these patients regarding appropriate follow-up care for their subacute concerns, and promote the documentation of this plan in the visit note. This study evaluated provider response to the CDS alert and the associated change in VUC utilization.
Methods
In our Electronic Health Record (Epic Systems, Verona, WI), an OurPractice Advisory (OPA) alert was developed to appear to VUC providers when a patient met high-utilizer criteria: more than three VUC visits in 30 days, more than 12 VUC visits in six months, or more than 20 VUC visits in the past year (Figure 1). The high-utilizer criteria were determined pragmatically based on clinical judgment, internal consensus, and experiential knowledge of the VUC leadership team derived from over 400,000 visits across five years of VUC platform operations, aiming to capture patterns of frequent use that raised concern among frontline providers. The OPA alert directed providers to use the .VUCHIGHUTILIZER SmartPhrase, which included a prompt for discussing a follow-up plan with the patient and documenting specific discussion details. Data were collected on patient demographics, the frequency of OPA firings, and SmartPhrase use from 12 November 2024, when the OPA was initiated, to 14 February 2025. To evaluate the 30-day period before and after the OPA triggered, patient VUC utilization rate data was collected from 14 October 2024 to 15 March 2025.
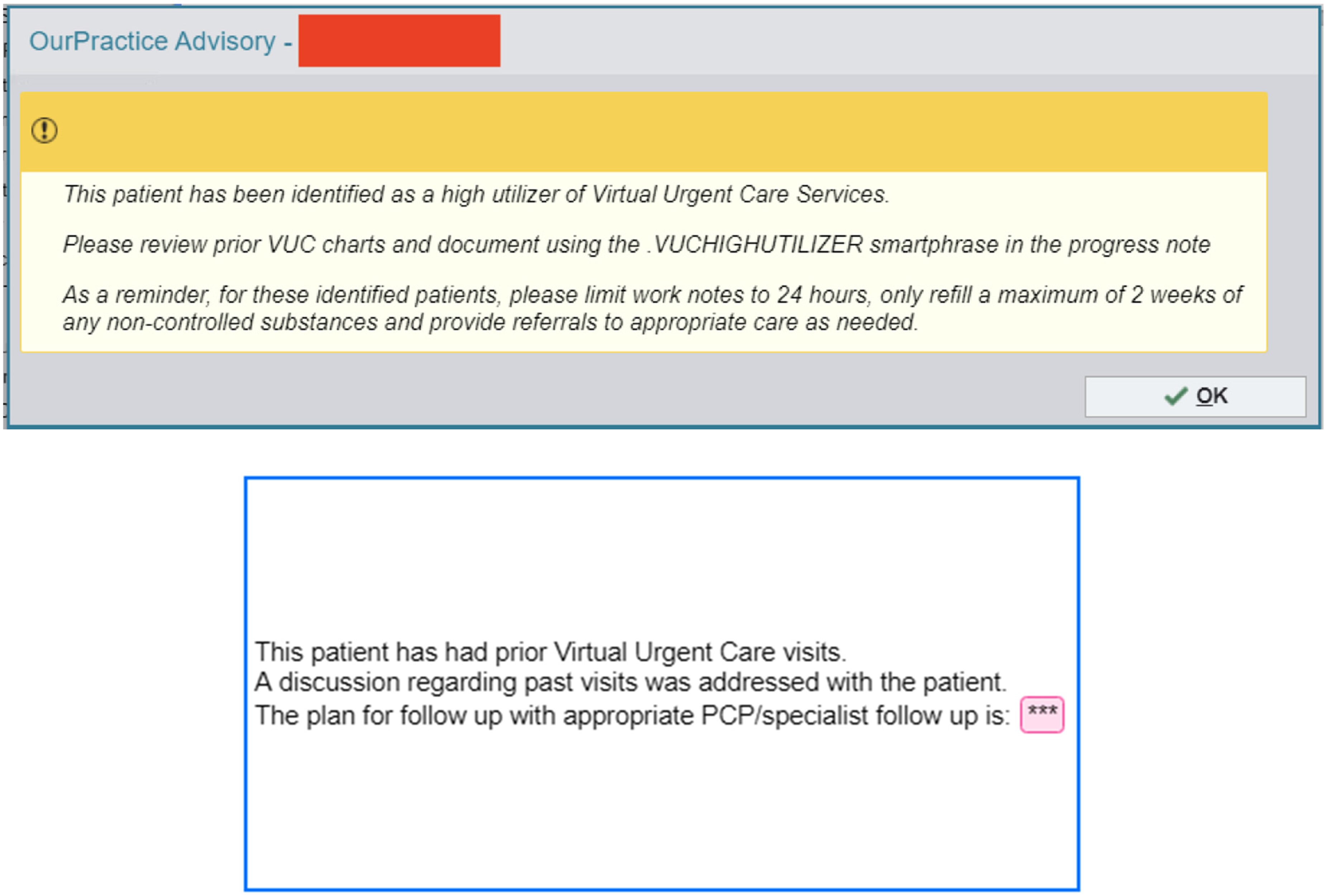
Virtual urgent care high utilizer alert and associated SmartPhrase, © 2025 Epic Systems Corporation.
Patients were categorized into two groups based on provider response to the OPA alert: (1) SmartPhrase used and (2) SmartPhrase not used despite the OPA alert firing. Baseline demographic characteristics were compared between groups using chi-square tests. For each patient, VUC visit counts were calculated for the 30-day periods preceding and following the index OPA trigger. The primary outcome was the change in VUC visits (post − pre). The primary analysis used a negative binomial regression model with postindex visit count as the dependent variable, adjusting for baseline utilization. Results are reported as incidence rate ratios (IRRs) with 95% confidence intervals. Sensitivity analysis was completed using bootstrapping with 10,000 resamples. All tests were two-sided with α = 0.05. Additionally, encounter-level data were extracted to assess downstream clinical actions, including prescriptions issued, laboratory orders, and imaging studies. The proportions of encounters with these orders were compared between visits in which the SmartPhrase was used and those in which it was not. Data analysis was performed using Python version 3.10 (GCC).
Results
Between 12 November 2024 and 14 February 2025, the OPA alert fired across 1101 unique VUC encounters involving 473 patients who met high-utilizer criteria. Of these, providers used the .VUCHIGHUTILIZER SmartPhrase in 266 encounters (24.2% of encounters) involving 162 patients (34.2% of patients). The remaining 311 patients did not receive the SmartPhrase across 835 encounters. There were no statistically significant differences in age, sex, race, or ethnicity between patients whose providers used the SmartPhrase and those whose providers did not (Table 1).
Demographics of VUC patients who were smartphrase-eligible.
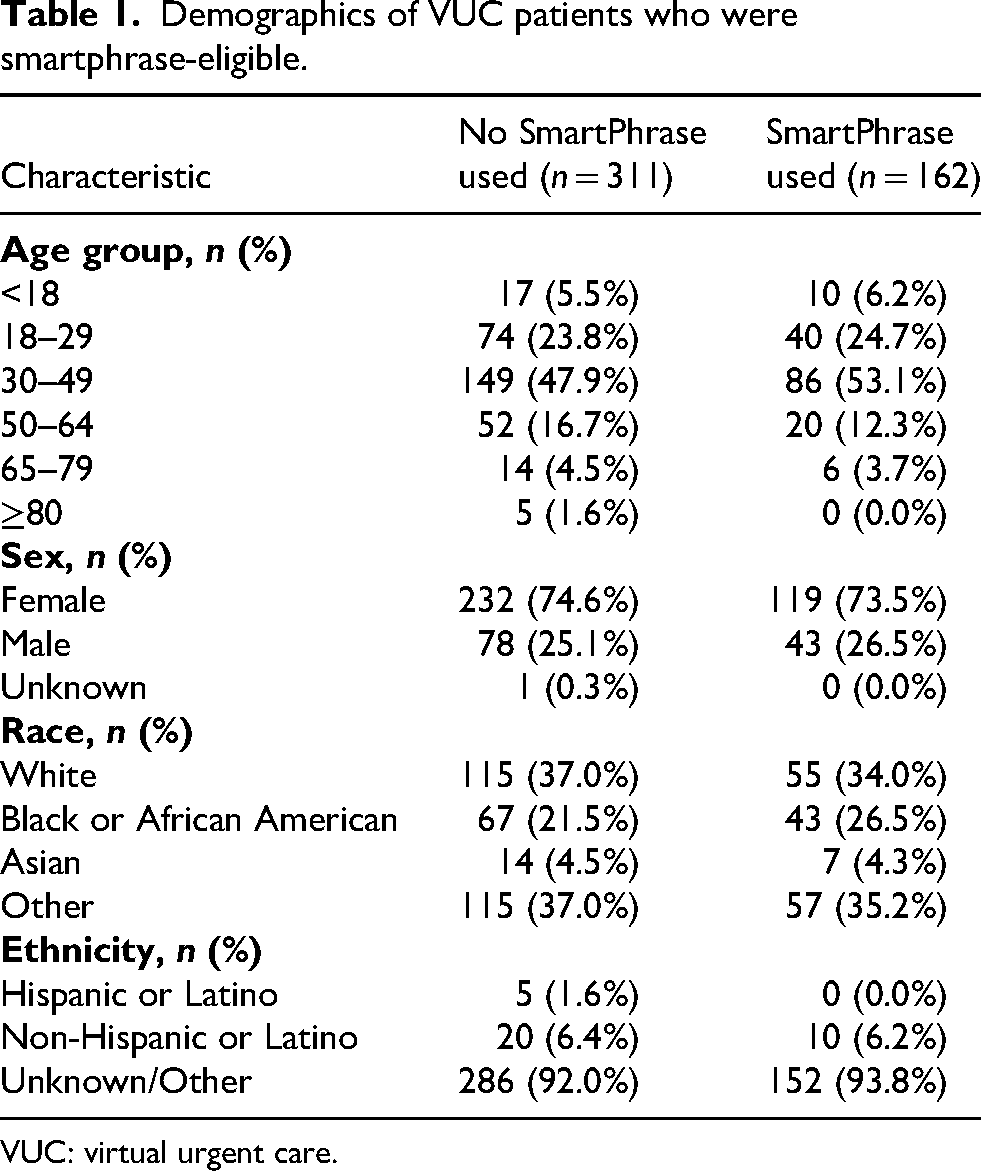
VUC: virtual urgent care.
Table 2 shows baseline and postindex VUC utilization by SmartPhrase use. At baseline, patients in the SmartPhrase group had higher mean VUC utilization (3.52 vs 2.83 visits). In the 30 days following the index trigger, mean utilization decreased to 2.16 in the SmartPhrase group and was 2.94 in the non-SmartPhrase group, yielding a mean change of −1.36 versus +0.11 visits. After adjustment for baseline utilization, SmartPhrase use was associated with a 22% relative reduction in 30-day VUC visits (IRR 0.78, 95% CI [0.62–0.97]; p = .030). Bootstrapped analysis with 10,000 resamples demonstrated a mean reduction of 1.47 visits (95% CI [−2.19 to −0.62]) in the SmartPhrase group, whereas the comparison group showed no significant change (+0.11 visits; 95% CI [−0.19 to +0.42]).
Change in virtual urgent care visits comparing patients who received .VUCHIGHUTILIZER SmartPhrase to patients who did not.
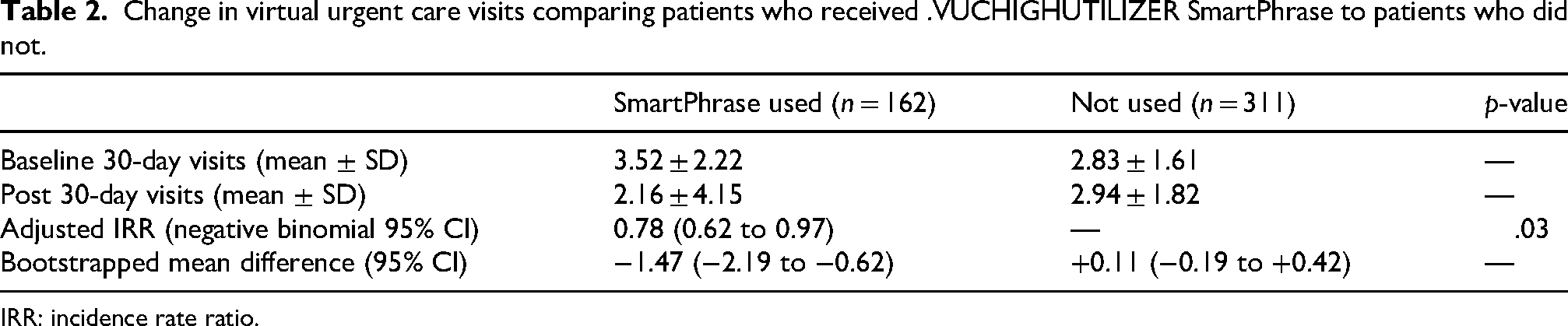
IRR: incidence rate ratio.
Additionally, among encounters in which the .VUCHIGHUTILIZER SmartPhrase was used, 54% resulted in a prescription being issued, 9% included laboratory testing, and 3% included imaging orders. By comparison, among encounters where the SmartPhrase was not used, prescriptions were issued in 27% of visits, labs were ordered in 4%, and imaging studies were ordered in 1%.
Discussion
High-utilizer behavior is well described in ED literature, where a small subset of patients account for a disproportionate number of visits. Our findings suggest that a similar utilization dynamic observed in ED settings is now emerging in VUC, an increasingly common entry point into healthcare systems. In our cohort, high utilizers represented a diverse and often younger population repeatedly seeking episodic virtual care. This pattern may suggest that a new generation of patients 50 years and younger are increasingly relying on convenient, on-demand care, perhaps in lieu of longitudinal management. Frequent VUC use is concerning because it may reflect unmet primary care needs, fragmented care delivery, and inefficient allocation of healthcare resources. For this reason, targeted interventions aimed at modifying high-utilizer behavior warrant careful evaluation.
After adjustment for baseline VUC utilization among our cohort, SmartPhrase use was associated with a 22% relative reduction in VUC visits over the subsequent 30 days. The intervention itself was modest—an alert paired with a documentation prompt—but may have been effective by making overutilization visible to providers and prompting a structured conversation about follow-up care. Faculty were explicitly encouraged to engage patients in substantive discussions regarding longitudinal management. We postulate that providers who utilized the SmartPhrase were more likely to reframe the encounter from an isolated urgent visit to part of a broader care plan, potentially facilitating transition to more appropriate longitudinal care. Because patients in the SmartPhrase group had higher baseline utilization, regression to the mean is a consideration. However, the absence of a parallel decline in the comparison group and the persistence of the association after adjusting for baseline utilization suggest that the observed reduction was unlikely to be explained solely by natural fluctuation. This baseline imbalance may also indicate that clinicians preferentially used the SmartPhrase for patients they recognized as being at especially high risk for recurrent VUC use, reflecting real-world clinical judgment but also introducing potential selection bias. Importantly, in this cohort, high utilization did not appear to self-correct. Patients for whom the SmartPhrase was not used experienced no reduction—and in fact a slight increase—in subsequent visits, suggesting that without targeted intervention, frequent VUC use may persist or worsen.
Only 24% of eligible encounters resulted in SmartPhrase use despite OPA alert firing, underscoring important implementation challenges. The intervention relied on a two-step workflow: an interruptive alert followed by manual entry of a specific dot phrase. This design introduces friction, requiring both cognitive recall and additional typing during time-constrained visits. The modest uptake suggests that alert-based CDS coupled with recall-dependent documentation may be suboptimal for sustained behavior change. Embedding structured prompts directly within note templates may reduce workflow burden and improve adherence. Future iterations should prioritize lower-friction CDS architectures, like inline disappearing text, 7 that can integrate seamlessly into documentation workflows.
Interestingly, SmartPhrase encounters were associated with higher rates of prescriptions, laboratory testing, and imaging compared with encounters in which the SmartPhrase was not used. This may reflect more intensive clinical engagement during these visits—perhaps a more comprehensive attempt to address unresolved concerns—rather than simple reassurance. At the same time, downstream laboratory and imaging use remained relatively low overall, suggesting that the reduction in future visits was unlikely to be driven by indiscriminate escalation of testing. Together, these findings point toward a behavioral effect on physician practice rather than purely technical automation.
This study has limitations. It was conducted at a single site over a relatively short period, and unmeasured confounding remains possible. Providers who chose to use the SmartPhrase may differ systematically from those who did not, and the nonrandomized observational design limits causal inference. We did not evaluate longer-term outcomes, patient adherence to follow-up recommendations, or clinical endpoints beyond VUC visit frequency. We also did not assess subsequent emergency department utilization, which would be an important exploratory safety outcome in future evaluations. Additionally, high-utilizer criteria were pragmatically defined based on institutional experience and may not generalize across telehealth platforms.
Despite these limitations, this study represents an early evaluation of high-utilizer behavior in telemedicine and a pragmatic attempt to address it using workflow-integrated CDS nudges. As telehealth platforms continue to expand, scalable strategies that promote care continuity while preserving access will be increasingly important. Lightweight, behaviorally informed CDS interventions may offer one such approach to optimizing virtual care delivery.
Footnotes
Acknowledgments
We gratefully acknowledge contributions to this project from the Ronald O. Perelman Department of Emergency Medicine at NYU Langone Health and Sheila Keatinge from NYU Langone MCIT.
Ethical approval and informed consent statements
Deemed quality improvement work without requirement for informed consent at our institution.
Author contributions
All authors contributed to the conception and design of the work and final drafting of the document.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data to be made available upon reasonable request.