
Abstract
Introduction
Effective communication between family members, intensive care unit (ICU) patients, and healthcare providers is essential for easing family member's distress. We sought to understand how virtual communication patterns between family members, ICU patients, and healthcare providers are related to the mental health outcomes of family members.
Methods
We systematically searched CINAHL and PubMed for peer-reviewed studies published between January 2015 and August 2024 that documented virtual communication with the family member of an adult ICU patient (e.g., phone calls, video calls) and used the family member's mental health as an outcome. Guided by the adapted Source, Channel, Message, Receiver, Outcome Model of Communication, quantitative mental health outcomes were categorized as “improved, neutral, or negative,” and qualitative study findings were synthesized into themes.
Results
Among 2,573 articles initially identified, 21 were selected for review. Phone and video calls were the most common communication modalities, and text messages were uncommon. Measured mental health outcomes included anxiety, depression, post-traumatic stress disorder, and stress or distress. Virtual communication was associated with either improved or no difference in measured mental health outcomes. However, meta-synthesis revealed two themes that suggest ways virtual communication can negatively influence emotions: (1) anxiety with variations in communication source, message, and frequency and (2) reassurance versus distress with communication modality.
Discussion
Promoting communication through virtual communication strategies may improve mental health outcomes or emotions experienced among family members of ICU patients. ICU healthcare providers should consider tailoring virtual communication modality and frequency to family members’ preferences.
Plain language summary
When a person is in the intensive care unit (ICU), it can be very stressful for family members—especially when they cannot visit or talk to the patient, doctors, or nurses in person. This study looked at how virtual communication, like phone calls, video calls, and text messages between families, patients, and ICU doctors and nurses, is related to the mental health of family members.
We reviewed 21 studies published between 2015 and 2024. These studies measured how virtual communication is related to family members’ mental health and emotional well-being. Most studies focused on anxiety, depression, post-traumatic stress disorder, or stress. For the studies that directly measured mental health, we found that virtual communication usually helped family members feel better or made no difference—none of the studies showed that virtual communication made mental health worse. However, some studies that interviewed family members showed that video calls could either reassure families or make them have negative emotions, such as feeling worried.
It is important for ICU doctors and nurses to ask families about their communication preferences. This way, they can adjust the type and frequency of virtual communication to support the mental health of family members of ICU patients.
Keywords
Introduction
Being the family member of a person hospitalized in the intensive care unit (ICU) is associated with adverse mental health outcomes including increased rates of anxiety, depression, and post-traumatic stress disorder (PTSD).1–3 Effective communication between family members and ICU healthcare providers is known to ease family members’ stress, anxiety, and comfort with decisions.4–6 Traditionally, most communication between ICU healthcare providers and family members occurs in-person, but can also occur via phone calls. A 2017 study of 14 Canadian ICUs found that 71.3% of families communicated with healthcare providers in-person, 15.4% of families communicated by phone, and 13.3% of families did not receive communication on the day the survey was administered. 7
Virtual communication (VC) is any information exchange that occurs between two parties using communication technology, including but not limited to audio communication (e.g., phone calls), video communication (e.g., video calls), and text-based communication (e.g., text messages, emails, messages via healthcare portals). Family members may rely on VC when they are unable to visit the patient's bedside due to geographic distance, limited time off from work, other family duties, or limited transportation access. 8 Limited ICU visiting hours were compounded during the COVID-19 pandemic by extensive visitor restrictions in hospitals,9,10 broadly shifting in-person communication patterns to VC between in-hospital healthcare providers and out-of-hospital family members.10,11
Three recent scoping reviews12–14 and one integrative review 15 examined altered family communication practices in the ICU during the COVID-19 pandemic. Common findings among these reviews were that phone calls and video calls were used to communicate with out-of-hospital family members.12–15 All reviews noted that the mental health of family members was impacted by restricted visitation and altered communication practices12–15; however, these reviews did not examine how specific aspects of VC, such as modality or frequency, impacted mental health outcomes of family members of ICU patients.
Given the body of evidence supporting communication as key in mitigating poor mental health outcomes among family members of ICU patients, and the continued reliance on VC modalities in the post-COVID-19 pandemic world, this review examines how aspects of VC between family members, ICU patients, and healthcare providers relate to family member' mental health outcomes.
Methods
Search strategy
The search strategy was developed in consultation with a library informaticist. We searched CINAHL and PubMed databases without restrictions to population or level of evidence. We limited to studies published between January 2015 and August 2024 to account for contemporary VC practices occurring 5 years before, during, and 1 year after the COVID-19 pandemic, which was declared over by the World Health Organization in May 2023. Our comprehensive search strategy used a combination of MeSH keywords and synonyms for ICU, family members, and VC (Table 1).
Search terms used.
Inclusion and exclusion criteria
Peer-reviewed quantitative, qualitative, and mixed methods studies were included if they (1) included adult family members of adult ICU patients, (2) reported at least one occurrence of VC with the family member (e.g., phone or video call, text-based messaging including email or patient portal messages), and (3) used family member's mental health as an outcome (e.g., anxiety, depression, PTSD, stress, distress).
Exclusion criteria included (1) non-English languages due to resource limitations, (2) non-peer-reviewed literature, and (3) simulated family-communication scenarios used to train healthcare providers. The main focus of this systematic review is VC; however, studies that included some in-person visitation (e.g., in-person updates, family meetings, or rounds) were not excluded if VC modalities were the primary communication strategy reported.
Article extraction and synthesis
All titles, abstracts, and full-text papers were reviewed independently by two reviewers (CMP, EP, MF, SK); disagreements were resolved by consensus among the reviewers. 16 Results are reported according to the Preferred-Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram. 17
The adapted Source, Message, Channel, Receiver, Outcome (SMCRO) Model of Communication (Figure 2) guided extraction. In the context of this review, the “source” is a communication partner in the ICU (e.g., healthcare provider or patient). The “message” is the words or information shared (e.g., updates on patient clinical status, test results). The “channel” includes communication frequency, duration, and modality (e.g., phone call, video call, text-based messaging, or in-person communication). The “receiver” is the family member of the critically ill patient (e.g., surrogate decision maker or other family member). Our adaptation adds a communication “outcome,” which is the family member's mental health. Communication broadly affects the emotions and mental well-being of a person,4–6 meaning it is important to consider as a key outcome to study.
We extracted descriptive study data and summarized study findings 18 relating to the Source, Message, Channel, and Outcome components of the SMCRO Model of Communication, as outlined above. For quantitative studies, we coded mental health outcomes resulting from communication as positive (indicating improved or positive association in mental health outcome), neutral (indicating no difference or change in mental health outcome), or negative (indicating worsened or negative association in mental health outcome). We used meta-synthesis 19 of qualitative studies to identify themes related to family members’ mental health and emotional responses to using VC technologies in the ICU, and subsequently integrated these themes with each component of the SMCRO Model of Communication.
Results
The initial search resulted in 2,573 articles; 21 were extracted for this review (Figure 1).
Prisma flow diagram.
Modified SMCRO model of communication.
Study characteristics
Table 2 reports overall study characteristics. These articles included 10 quantitative studies (Table 3),20–29 9 qualitative studies (Table 4),30–38 and 2 mixed-methods studies (Table 5).39,40 Quantitative studies included experimental (randomized controlled trials,21,23,29 a quasi-experimental pilot study, 20 and an interventional study 22 ) and non-experimental methods (cross-sectional observational24,25 and prospective observational studies26,27). All qualitative studies were cross-sectional; the majority utilized semi-structured individual interviews for data collection (n = 6/9, 67%)30,34–38 and used thematic analysis to describe findings (n = 7/9, 78%).31–37
Study characteristics.
Communication findings—quantitative studies (n = 10).
Communication findings—qualitative studies (n = 9).
Communication findings—mixed methods studies (n = 2).
All included studies were published after 2020; studies before 2020 did not meet the inclusion criteria because they did not specifically report use of VC modalities (e.g., phone calls, video calls, text messaging, patient portal messages) in their title or abstract. Most included studies (n = 12/21, 57%) began data collection within the first 6 months of the COVID-19 pandemic or the subsequent 6 months of the pandemic (n = 8/21, 38%).
Half of the studies were conducted in multiple ICUs (n = 11/21, 52%). Most studies (n = 17/21, 81%) did not specify the type of ICU. Geographically, most studies were conducted in Europe (n = 9/21, 43%) or North America (n = 6/21, 29%).
SMCRO result: Communication source
The communication source was most commonly the ICU nurse (n = 19/21, 90%). However, ICU physicians (n = 13/21, 62%) and ICU patients (n = 12/21, 57%) were other reported communication sources.
SMCRO result: Communication message
In general, most studies did not report details about the communication message. For studies that did discuss message content, healthcare providers typically discussed routine updates or non-routine significant events such as worsening clinical status or death. Qualitative studies revealed that the clarity of the message was important to family members. Family members reported feeling frustrated and disappointed when communication from healthcare providers was unclear, contained medical jargon, or if they received insufficient information or were misinformed on the patient's status.32,36 No studies reported the communication message between the patient and the family member.
SMCRO result: Communication channel
Modality
Most studies used one or two communication modalities (n = 17/21, 81%); few studies used three or more modalities (n = 4/21, 19%).21,25,36,37 Phone calls, video calls, or a combination of both were used in nearly every study (n = 20/21, 95%). One study examined the use of text messages, 26 and three studies reported rare opportunities for in-person communication amidst visitor restrictions during the COVID-19 pandemic, such as visitation at end of life.25,40
Frequency
Approximately half of the studies (n = 9/21, 43%) reported “daily” communication frequency. Other studies described communication frequency with vague terms, including “sporadic,”24,31 “arbitrary,” 30 or “intermittent.” 34 Two studies described communication frequency as being based on specific events, such as obtaining procedural consent, 34 or ICU admission/discharge. 26 Three studies did not report communication frequency.22,32,38
Duration
Approximately one-third of studies (n = 6/21, 29%) reported communication duration, with a range from 5 min24,27,29 to 30 min.20,29,38 In one qualitative study, some surrogate decision-makers felt communication on goals of care was “rushed.” 35
SMCRO result: Communication outcome
Measurement of mental health outcomes:
Quantitative and one mixed methods study used validated measures of mental health outcomes, including anxiety (n = 6/11, 55%), depression (n = 5/11, 46%), stress or distress (n = 4/11, 36%), and PTSD (2/11, 18%). Studies that used combined anxiety and depression scales, such as the Hospital Anxiety and Depression Scale (HADS)20,21,27 or the Depression Anxiety and Stress Scale-21 (DASS-21), 28 typically did not report subscales to understand anxiety and depression separately. Mental health outcomes were almost always measured during ICU hospitalization, with only one study including additional data collection after discharge. 27
Qualitative studies and two mixed methods studies reported emotions, experiences, and perceptions of family members using VC. Nearly all qualitative results (n = 10/11, 91%) found that some family members experienced negative emotional responses to the communication message and channel of VC, including feelings of anxiety, stress, psychological distress, worry, panic, fear, frustration, sadness, hopelessness, powerlessness, discomfort, and distrust.30–32,34–37,39,40 Fewer studies reported positive emotional responses to using VC, which included feelings of reassurance, involvement, togetherness, and appreciation,31,35,36,39,40 or reductions in anxiety and stress.31,34,35,40
How does virtual communication relate to the mental health of family members of intensive care unit patients?
Among the quantitative results, all demonstrated that mental health outcomes either improved or did not worsen with use of VC (Table 6). Improvements were found in anxiety, depression, stress, and distress after interventions testing the use of video calls,22–24,27,28 and one study found that video calls were superior to phone calls in terms of reducing anxiety. 23 The use of text messages was rare but appeared to be helpful, with family members from one study indicating that text messages providing routine updates on patient status changes (e.g., extubation, ICU discharge) made them feel “reassured” and did not make them feel anxious. 26
Quantitative results that found no change in mental health outcomes used mixed anxiety-depression scales20,21,28 or evaluated for changes in PTSD. Of note, all studies that measured PTSD used multiple communication modalities and described in-person visitation to the ICU for special circumstances, such as when the patient was approaching the end of life.21,25,40 It is unclear how these visitations or the patient being near the end of life might have changed mental health outcomes of participants in these studies.
Meta-synthesis of qualitative results revealed two themes relating to the emotions of family members using VC: anxiety with communication uncertainty, and reassurance versus distress with phone calls.
Theme 1. Anxiety with variations in communication source, message, and frequency
Family member' anxiety was related to variations in communication source, message, and frequency. Family members expressed negative emotions if there was no clear communication source for them to call as a point of contact, or if they perceived that calling placed an excessive burden on busy healthcare providers to give an update.31,34,36 Additionally, family members reported feeling worried about the communication message, fearing the information they may receive.30,31,41 If information provided contradicted prior updates, family members could develop distrust or doubt the message and the messenger. One family member in Lopez-Soto's study shared their confusion, “They kept telling us he was stable … then they called us to tell us he was dead … how is this possible?” 38
Family members expressed both positive and negative emotional responses to communication frequency. It was difficult for family members to wait for a phone call, particularly if they did not know when to expect a call, if calls were inconsistent, or if an expected call was delayed.31,34–37 Family members strongly desired regular, predictable updates.32,36 Family members felt reassured when they were told to call any time, 36 with one study recommending daily email updates on the patient's condition to ease family anxieties. Studies that reported daily phone or video call updates demonstrated reductions in feelings of anxiety as well as feelings of involvement in care and appreciation.31,35,36
Theme 2. Reassurance versus distress with communication modality
Communication modality affected the anxiety of family members. A combination of visitor restrictions and use of phone calls did not allow family members to directly see the patient or healthcare team; this led to worry and distress about the patient's condition,31,34,36,39 feelings of distrust with the patient's providers, 35 and a lack of reassurance that the patient received appropriate end-of-life care.37,39
Video call modalities resulted in mixed emotions. Family members appreciated video calls, which let them see the patient, 36 helped them feel connected to the patient and the healthcare team,32,35,39,40 and provided reassurance regarding the care that the patient received, 35 which subsequently alleviated stress34,35 and feelings of helplessness. 40 However, family members also reported negative emotional responses from video calls, such as stress, sadness, worry, and discomfort when seeing the environment of the ICU and that the patient was in poor health, intubated, on life support, and/or connected to medical equipment.32,35,36,40
Discussion
This systematic review with meta-synthesis examines how aspects of VC used between adult ICU patients, healthcare providers, and family members of ICU patients relate to mental health outcomes among these family members. We found that VC with family members typically occurs daily and that the communication sources were usually ICU healthcare providers, often nurses or less commonly physicians or the ICU patient. Phone and video calls were the most common modalities. The most notable finding of this review is that virtual communication was associated with either a positive or neutral effect on mental health outcomes measured with validated scales; however, meta-synthesis revealed that virtual communication may increase negative emotions experienced by family members of ICU patients.
All but one of the studies collected data during the first year of the COVID-19 pandemic. This timing suggests academic interest in the effects of VC, likely in reaction to the limited in-person visitation that occurred during the COVID-19 pandemic. Moreover, increased comparative research may have occurred because the pandemic offered a natural experiment for examining VC compared to in-person and phone communication prior to the pandemic.
Our findings of daily communication between ICU healthcare providers and family members reflect ICU communication practices and guidelines from before the pandemic. 42 However, in agreement with the findings of Meiers et al. (2024), 13 this review found that communication shifted to predominantly virtual instead of in-person modalities, reflecting a significant change from typical ICU communication practices. Text messages with family members were less frequently used, which was surprising given the increased acceptance and use of secure text-messaging between healthcare providers.41,43 Text messages offer the benefit of asynchronous communication, which may be more convenient for healthcare providers 41 ; however, this modality lacks audio and visual input, which family members found very reassuring in many of the qualitative studies included in this review. Another consideration is access to VC technologies—some studies excluded family members from study participation due to limited technology access, such as not having a smartphone or computer,23,27,29,31 not having internet access, 27 or not having specific smartphone applications such as WhatsApp.23,28,29 This discrepancy in access to VC technologies represents an additional area to consider for equitable study design, and an additional area to consider by clinicians communicating with family members of ICU patients.
There were mixed results determining the relationship between VC and the mental health of family members of ICU patients, reflecting similar incidental findings from a scoping review by Solomon et al. (2024). 14 We found that VC resulted in either improved or resulted in no difference in measured mental health outcomes, with no studies demonstrating worsened mental health outcomes from VC. The strength of these correlations varied across studies, but comparison was limited due to a lack of measures or scales of VC patterns. Additionally, the lack of studies reporting worsened mental health outcomes may not reflect a true lack of negative emotional consequences of VC, since qualitative evidence connected VC with both positive and negative feelings of family members. Family members reported that VC was both a “lifeline” to the patient and healthcare providers and simultaneously distressing in that they were limited to “visiting” the critically ill patient through a video screen. Family members may experience negative emotions resulting from the communication message shared about the critically ill patient; however, our findings suggest that the communication channel may also be associated with negative emotions in the context of limited in-person visitation. So, while VC may not change or worsen a person's measured mental health (e.g., symptoms of anxiety measured on a validated scale), VC may affect emotions (e.g., feelings of anxiety or worry). This is important, as repeated negative emotions (e.g., persistent worry) may signal risk for a future mental health outcome (e.g., generalized anxiety disorder).
Clinical, policy, and research recommendations
Our results suggest that healthcare providers can do more to ease the stress of family members. We found evidence of family members’ strong preference for daily updates at a predictable time, with a clear point-of-contact in the ICU for communication, and a clear message without medical jargon or vague information. Specific clinical policy recommendations are listed in Table 7.
Summary of communication modality and positive, neutral, or negative mental health outcomes from the quantitative studies.
Clinical policy recommendations to improve communication.
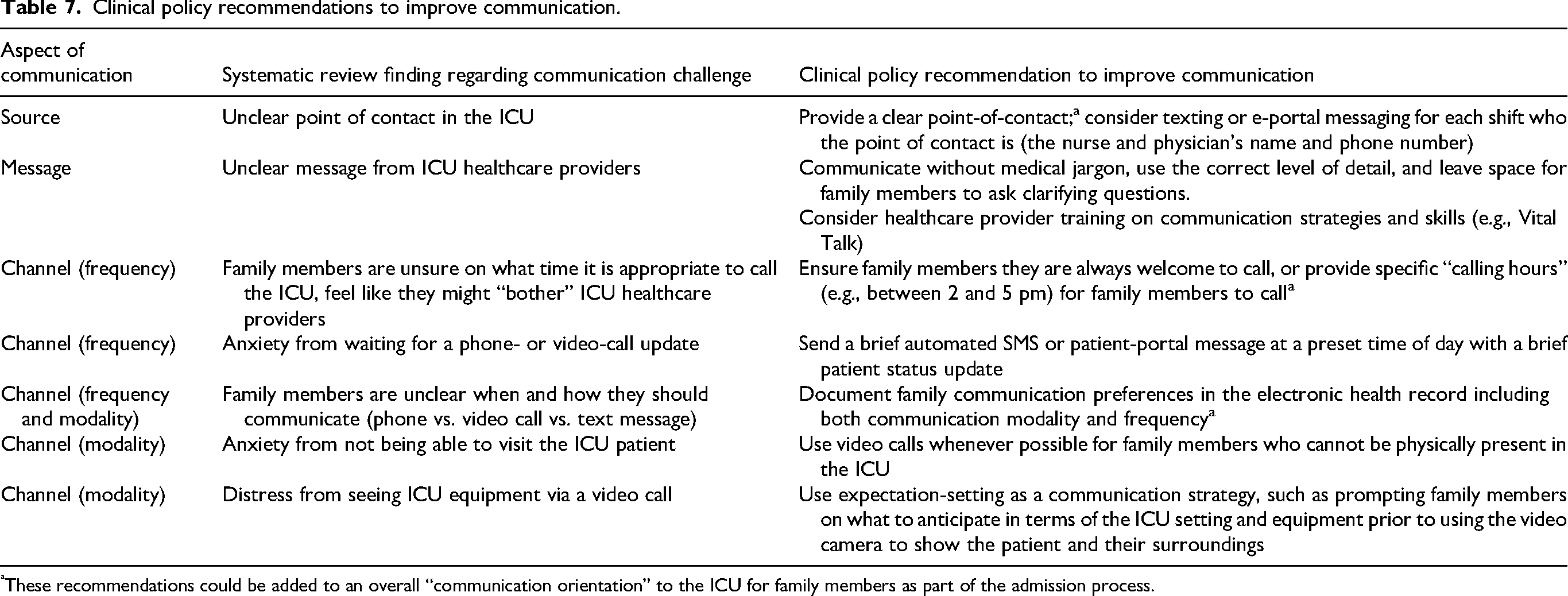
These recommendations could be added to an overall “communication orientation” to the ICU for family members as part of the admission process.
Future research should consider testing VC strategies individually and bundled together to address common communication challenges in ICU settings. For example, Gorman et al. (2020) received positive feedback from families receiving brief text messages as a communication strategy; however, more research may be necessary to determine the practicability of this solution across care settings and illness scenarios. We found limited data exploring VC between families and the ICU patient, which may have additional implications in the mental health of family members, and is another area to explore in future research.
Limitations and strengths
There were few papers to review, perhaps due to not including databases such as EMBASE or PsycINFO, or perhaps due to this topic being under-researched. We excluded any non-English language articles due to resource limitations, and therefore may have missed data from studies published in other languages—we identified one study from a South American country, and no studies from African countries, so information from these regions is lacking. Our study is strengthened by meta-synthesis, which is helpful for collating qualitative findings, but some richness of the qualitative data is lost in deriving themes. Additional strengths of our systematic review with meta-synthesis include the focus on understanding how VC was related to mental health outcomes of family members and the use of a communication theory-based approach. Using the adapted SMCRO Model of Communication provides a strong foundation for addressing our research question and future communication science.
Conclusion
A recent increase in the use of VC between family members, ICU patients, and healthcare providers necessitates understanding how VC might affect the mental health of family members. Although it is not possible to change the communication “message,” findings from this review suggest that modifications in communication frequency, duration, and modality could lead to better mental health outcomes among family members of ICU patients.
Footnotes
Acknowledgments
The authors would like to acknowledge Ms. Ja’Lynn Gray for helping to review titles and abstracts for this manuscript.
ORCID iDs
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
No new data were created in this study. Data sharing is not applicable to this article.