
Abstract
Background
Emergency department (ED)-based teletrauma service may improve access to trauma expertise, especially in rural areas. However, its impact on patient outcomes remains unclear due to limited understanding of how and what type of care is delivered. The objective of this study was to characterize how EDs in the United States (US) use teletrauma services in clinical practice.
Methods
Non-federal/non-specialty EDs, that previously reported using teletrauma, were surveyed in the 2023 National Emergency Department Inventory Teletrauma Survey. The survey was developed and mailed/emailed to ED directors up to two times; nonresponders were contacted via telephone. Survey assessed structural and process measures including staffing, workflows, clinical care, and resource availability. Descriptive statistics were used.
Results
Among 378 EDs that reported using teletrauma in 2022, 310 responded (82%). Only 68% (211/310) reported using teletrauma in 2023. Most teletrauma-using EDs (TT-EDs) used the service once a month or less (58%), were staffed by non-emergency medicine (EM)-trained providers for in-person care (69%) and EM-trained physicians for remote care (72%). Consults were usually initiated at the discretion of the in-person provider (80%) and often after the patient's arrival to the ED (46%). Clinical applications included decision-support for interfacility transfers (78%), resuscitation-support (71%), documentation (69%) and remote procedural-support (64%) for patients of all ages. Some TT-EDs received trauma education from teletrauma-providing sites (30%), but few reported receiving resources, such as blood products (4%).
Conclusion
Teletrauma is not widely used in US EDs. Even when capabilities exist, teletrauma use remains limited and insufficiently adapted to rural trauma care.
Introduction
Trauma centers are specialized hospital units with comprehensive resources and expertise to treat injured patients. 1 Timely treatment at a trauma center reduces risk of death by 25%. 2 Yet nearly 30 million, mostly rural patients, lack timely access to a trauma center, necessitating treatment at local hospitals without this level of trauma expertise.3,4 Prior research shows that lack of trauma center access results in higher mortality among severely injured rural patients compared to their urban counterparts and potentially avoidable interfacility transfers of patients with minor injuries, wasting already scarce rural healthcare resources.5–16 The traditional solution of establishing new trauma centers is slow, costly, and often impractical in rural areas. Consequently, there have been no improvements in outcomes or access to expert trauma care for over a decade. 17
In recent years, telehealth has matured as a viable alternative to in-person healthcare delivery, especially among underserved rural communities. 18 Remote trauma care experts can connect via real-time, two-way, audio-visual communications with injured patients and their local healthcare teams (teletrauma) at rural emergency departments (EDs). 19 Provider-to-provider telehealth is well-established for other acute time-sensitive conditions, such as telestroke, to remotely deliver clinical expertise at the point-of-care, resulting in timely access and improved patient outcomes.18,20–23 Telehealth has been used in several ways to deliver trauma care in the ED, ranging from acute resuscitation support and procedural proctoring to knowledge-transfer and decision making regarding the need for patient transfer to a trauma center.24,25 Injury populations served through telehealth have also ranged from undifferentiated trauma patients to specific injuries such as burns, traumatic brain injury, and hand-trauma.26–29 While limited-scale use of teletrauma shows promising results, it is difficult to evaluate its impact on patient outcomes given the heterogeneity in how teletrauma has been used and the trauma populations it has served.26,29–32
A recent report by the Agency for Healthcare Research and Quality (AHRQ) highlights that “within each use of telehealth there are wide range of models” and the “lack of information about the specifics of telehealth interventions make it difficult to synthesize results across studies.” 18 The report recommends including “more complete descriptions of both the content of telehealth and comparator interventions” in future research. 18 For teletrauma, a more complete description of teletrauma use in EDs is needed to begin understanding its impact on trauma care. Furthermore, the American College of Surgeons Committee on Trauma (ACS COT) recently described two main goals for teletrauma programs—to reduce potentially preventable early deaths and to reduce potentially avoidable interfacility transfers. 33 How teletrauma-using EDs (TT-EDs) align with these goals remains unclear, especially in rural areas. Therefore, the objective of this study is to characterize how US EDs are using teletrauma services in their clinical practice to care for injured patients.
Methods
Study design and sample
The National ED Inventory (NEDI)-USA is a nationwide survey of all non-federal, non-specialty US EDs coordinated by the Emergency Medicine Network; detailed NEDI-USA methodology has previously been described.34,35 ED directors at EDs reporting teletrauma use in NEDI-USA 2022 were surveyed in the NEDI Teletrauma Survey 2023. This study was approved by an institutional review board at a large academic health system in the United States and was determined to be exempt human subjects research and follows American Association for Public Opinion Research (AAPOR) guidelines.
Survey development and pretesting
A draft survey was created by the study team following a literature review, including a consideration of limitations of prior work, as highlighted in a recent AHRQ report. 18 The survey questions covered structural and process measures pertinent to delivery of remote trauma care at TT-EDs. Pilot surveys were conducted with eight ED directors, randomly selected from the target population, to assess survey clarity, completion times and need for assistance to inform refinements.
Survey administration
Surveys were sent to ED directors by mail up to two times over a 2-month period; a link to an online version of the survey was also included. Nonresponding EDs or EDs with incomplete surveys were further contacted via telephone. Survey data were recorded and managed using REDCap.36,37 The survey was administered between November 2024 and March 2025.
Measurements
The full survey was administered to EDs that confirmed the receipt of teletrauma services in 2023 (Supplemental material). The survey asked questions pertaining to teletrauma program structure and processes-of-care in 2023. Structural questions explored hub–spoke relationships, healthcare provider qualifications, teletrauma equipment/infrastructure, funding/payment model, frequency of teletrauma use, resource availability/sharing, and education/knowledge transfer. Processes-of-care questions explored teletrauma workflow (criteria and timing of teletrauma consult initiation), content of teletrauma engagement (acute trauma resuscitation support, remote procedural proctoring, decision making for interfacility transfers, and review of imaging) and types of injured patients (age and injury patterns) served via teletrauma.
Other variables of interest
ED characteristics were obtained from the NEDI-USA 2022 database including total ED visits in 2022, geographic location (region/state), urban/rural (defined using Urban Influence Codes), critical access hospital (CAH), Council of Teaching Hospitals (COTH) member, stroke center level, and adult/pediatric trauma center level. Basic and advanced trauma centers were classified based on prior work that unified American College of Surgeons (ACS) verified and state designated trauma center levels. 38 ACS-similar levels 1 and 2 trauma centers were classified as advanced and ACS-similar level 3 trauma centers were classified as basic trauma centers.
Data analysis
Data analysis was performed at the level of each individual ED. Descriptive statistics were used to quantitatively report numbers and percentages of responses to discrete survey items. Chi-square or Fisher's exact tests were used, as appropriate, to compare general ED characteristics among: (1) survey responders versus nonresponders and (2) EDs confirming using or not using teletrauma in 2023. All analyses were performed with Stata version 18.0 (Stata Corp, College Station, Texas, USA).
Results
In 2022, 378 EDs reported using teletrauma and 310 responded to the NEDI Teletrauma Survey 2023 (82% response rate) (Figure 1). There were no statistically significant differences between survey responders versus nonresponders except that responders were less likely to be in urban areas (20% urban location among responders vs. 34% among nonresponders, p = 0.02) (Supplemental Table 1). Among the responding EDs, only 68% (n = 211/310) confirmed using teletrauma in 2023. Of the 99 EDs that did not use teletrauma in 2023, 22% (22/99) stated that prior response was misreported, and they did not use teletrauma in 2022; 68% (69/99) did not specify a reason for the change.
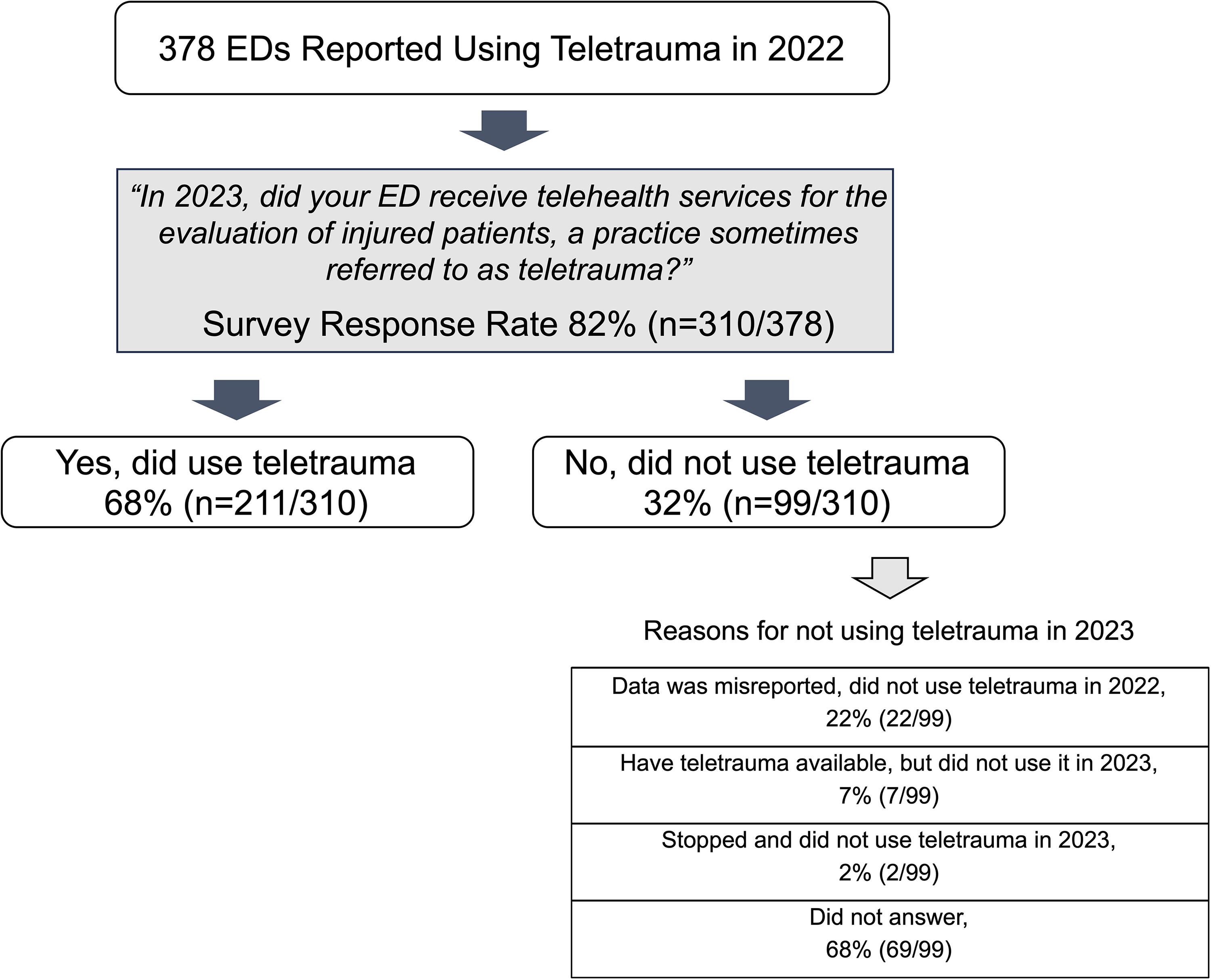
Flowchart of teletrauma using emergency departments (EDs) included in the survey.
General ED characteristics
Compared to non-TT-EDs, TT-EDs had lower annual ED visit volumes, were more likely to be in the Midwest region and in rural areas (Table 1).
Characteristics of emergency departments responding to the NEDI teletrauma survey, n = 310.
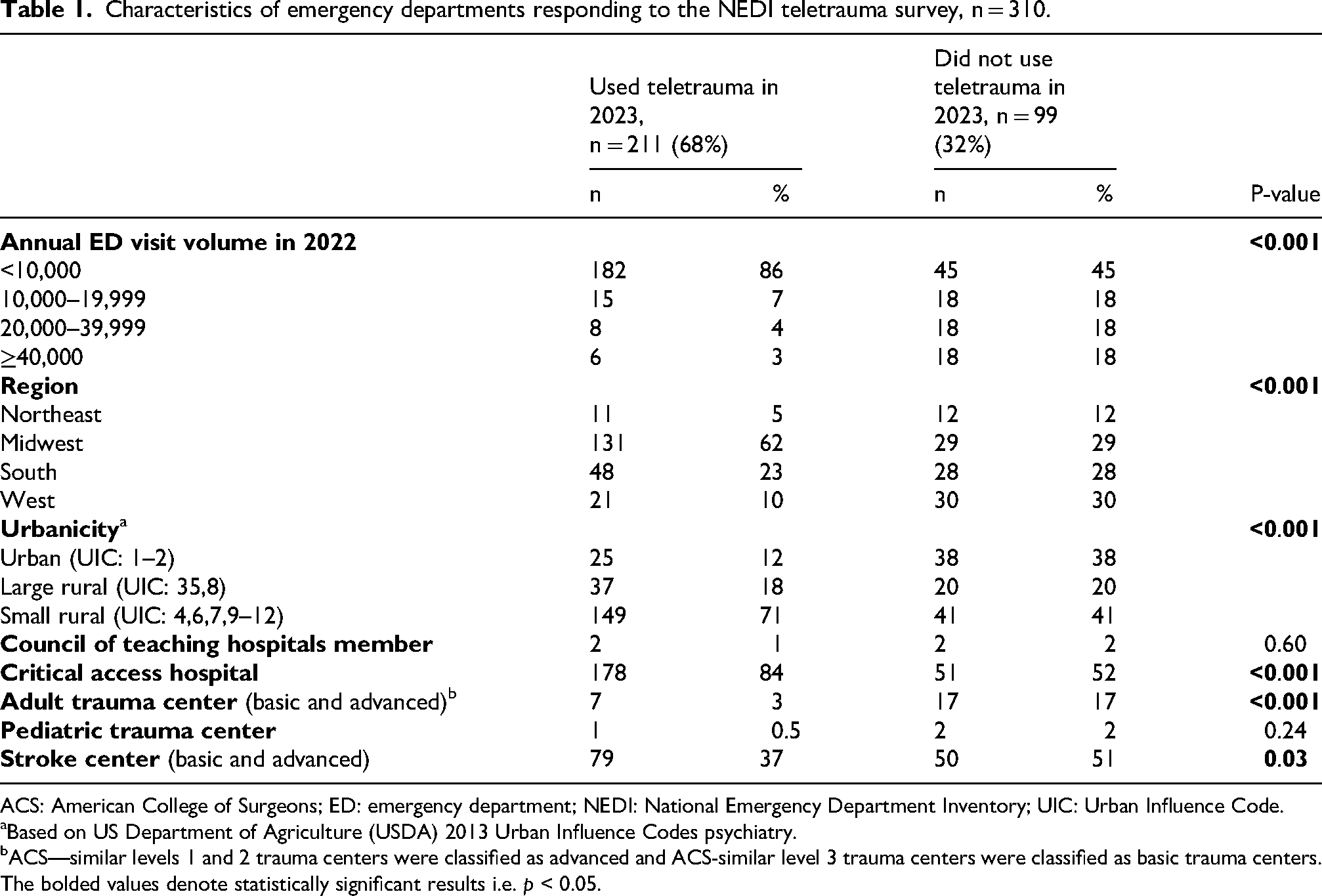
ACS: American College of Surgeons; ED: emergency department; NEDI: National Emergency Department Inventory; UIC: Urban Influence Code.
Based on US Department of Agriculture (USDA) 2013 Urban Influence Codes psychiatry.
ACS—similar levels 1 and 2 trauma centers were classified as advanced and ACS-similar level 3 trauma centers were classified as basic trauma centers.The bolded values denote statistically significant results i.e. p < 0.05.
Survey responses related to teletrauma program structure
Table 2 describes teletrauma program structure. Most TT-EDs (60%, 126/210) reported evaluating ≥1 injured patients per week yet most (58%, 123/211) used teletrauma services once every 3 to 4 weeks or less often to care for injured patients. In most TT-EDs, a nonphysician provider (nurse practitioner or physician assistant) led in-person care (47%, 100/211) while emergency medicine (EM)-trained physicians provided remote injury care in most instances (72%, 150/209). Third-party and nonhospital-based entities (e.g. private organizations, state trauma systems, and regional trauma care collaboratives) provided teletrauma in most EDs (54%, 113/210). Programs were primarily funded through direct contractual agreements between EDs and facilities providing the teletrauma service (75%, 157/208). While some EDs reported receiving formal trauma care education from the hub site (30%, 62/210), very few TT-EDs reported receiving trauma care resources, such as blood products or medicines, from the hub sites (4%, 9/207).
Survey responses related to the teletrauma-using ED's structure reported to the NEDI teletrauma survey 2023, n = 211.
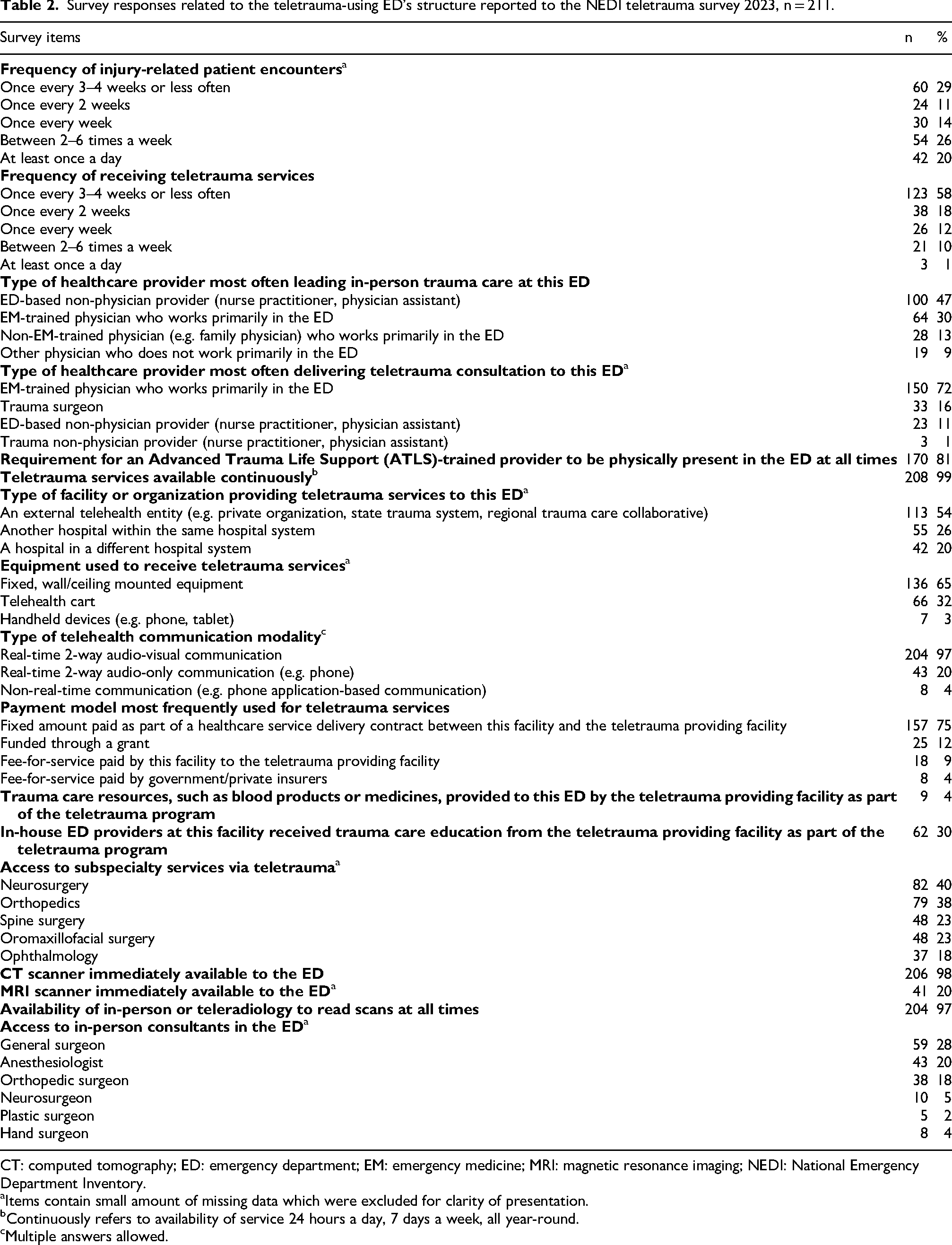
CT: computed tomography; ED: emergency department; EM: emergency medicine; MRI: magnetic resonance imaging; NEDI: National Emergency Department Inventory.
Items contain small amount of missing data which were excluded for clarity of presentation.
Continuously refers to availability of service 24 hours a day, 7 days a week, all year-round.
Multiple answers allowed.
Survey responses related to teletrauma program processes-of-care
Table 3 describes teletrauma program processes-of-care. Most TT-EDs reported teletrauma consult initiation at the discretion of the spoke provider (80%, 165/205) and most often after the arrival of the injured patient to the ED (46%, 96/207). TT-EDs reported using teletrauma services for a range of clinical applications including clinical decision making for interfacility transfers (78%, 165/211), for initial evaluation and acute resuscitation (71%, 149/211), to help with medical documentation (69%, 146/211) and to provide remote procedural support for interventions such as central venous catheter placement, chest tube placement, endotracheal intubation, or cricothyroidotomy (64%, 136/201). Additionally, 68% (143/211) reported using teletrauma for three or more of these services. Most TT-EDs used teletrauma services for all ages (95%, 136/211) and any type of injury (≥86% of EDs). Among TT-EDs that reported using teletrauma for only specific types of injuries, most reported using teletrauma for burn care. Relevant to care of the severely injured patients, 74% (153/208) of TT-EDs had capability to obtain type O negative blood for emergent transfusion in less than 15 minutes but only 11% (23/207) had emergent access to operating room within 30 minutes.
Survey responses related to the teletrauma-using ED's processes-of-care reported to the NEDI teletrauma survey 2023, n = 211.
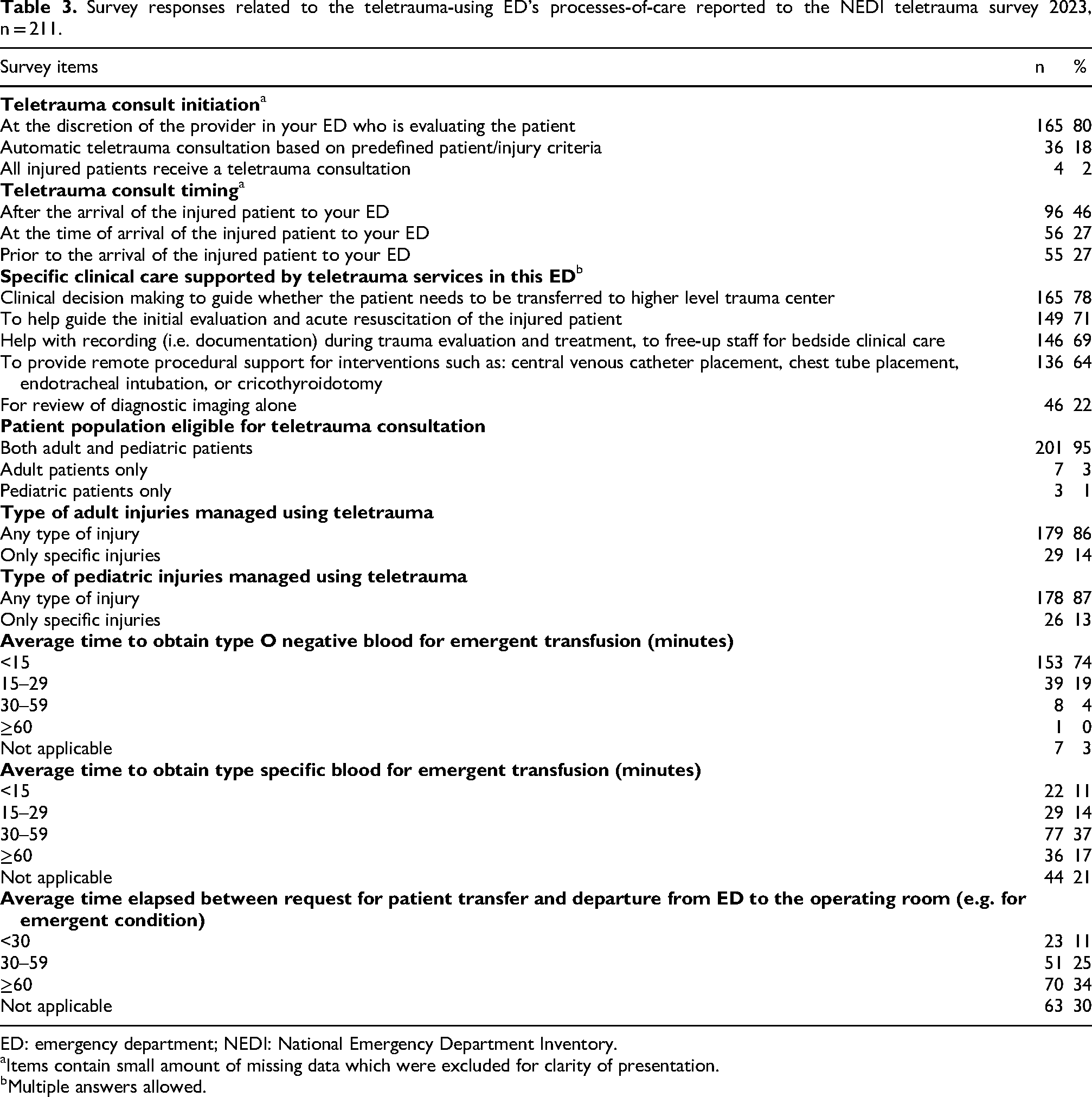
ED: emergency department; NEDI: National Emergency Department Inventory.
Items contain small amount of missing data which were excluded for clarity of presentation.
Multiple answers allowed.
Discussion
This national survey reports the first comprehensive description of teletrauma use in US EDs. Fewer EDs used teletrauma in the United States than previously reported. 39 Survey responses on teletrauma program structure and processes-of-care offer key insights into the: (1) provider types and workflows enabling teletrauma care, (2) clinical care delivered via teletrauma, and (3) dynamics of hub-and-spoke relationships. At TT-EDs, in-person care was typically provided by non-EM-trained staff, while remote care was provided by EM-trained physicians. Teletrauma use was infrequent, discretionary, and lacked standardization. Clinical applications were broad, but specialist access and resource sharing were limited. Cumulatively, these results suggest that while telehealth-enabling capabilities exist in these EDs, the current approach to teletrauma care delivery lacks intentionality and alignment with ACS COT goals of reducing potentially preventable early deaths and potentially avoidable interfacility transfers. Overall, this study lays the groundwork for future efforts aimed at optimizing the integration of telehealth into trauma care systems.
Provider types and workflows enabling teletrauma care
Our study demonstrates a trauma care model at TT-EDs where in-person trauma care is predominantly delivered by either nonphysician providers or non-EM trained physicians, while teletrauma care is primarily provided by nonhospital-based, EM-trained physicians. This reflects the reality of diminishing EM physician presence at small, rural, and CAH facilities where telehealth is increasingly being leveraged to remotely deliver EM physician expertise for many conditions through partnerships with private telehealth entities.40–43 In this context, the provision of teletrauma appears to be a byproduct of the expansion of tele-emergency medicine (tele-EM) rather than an intentional approach to improve access to or quality of trauma care. Our results demonstrating infrequent and discretionary use of teletrauma services at TT-EDs further support this notion. More than half of TT-EDs reported using teletrauma once every 3 to 4 weeks or less often, despite the majority seeing at least one injured patient per week. Additionally, most teletrauma consultations were initiated at the discretion of the in-person provider, rather than using predefined criteria, and typically occurred after the patient's arrival to the ED. Although the impact on patient outcomes is not yet determined, this approach is a departure from trauma activation guidelines developed to identify patients in need of urgent care while balancing under and over-triage. 44 Therefore, the current discretionary use of teletrauma raises concerns regarding appropriateness, quality, and timeliness of trauma care. Overall, these data suggest that while certain capabilities exist, teletrauma use is currently reactive, driven by individual provider decisions, and is not used systematically to deliver remote trauma care.
Clinical care delivered via teletrauma
We found that teletrauma services were available to manage any type of injury among all age groups. These results confirm previously reported findings from pilot teletrauma programs.26,31,45–47 The undifferentiated use of teletrauma likely stems from the fact that remote trauma care was most frequently delivered by EM physicians whose scope of practice includes care of all patients. Additionally, given overall low patient volumes, it may be impractical to further restrict care to specific injury patterns, especially outside of intentionally implemented teletrauma programs. Among the few EDs using teletrauma for specific injuries, burns were the most commonly cited indication. This finding is expected as burn care requires expertise that is only available at a few trauma centers nationwide and relies heavily on visual assessment of the wound. Both these factors make burn care amenable to telehealth. 48
Survey results demonstrated that teletrauma services were used for many clinical applications. The most common uses, including clinical decision making for interfacility transfers, acute resuscitative phase care support and remote procedural support for urgent bedside interventions, encompass all aspects of acute injury evaluation and management, and corroborates previous reports of teletrauma use in pilot programs. Although most TT-EDs required in-person providers to be Advanced Trauma Life Support (ATLS)-trained, the use of telehealth, especially for acute resuscitation and procedural proctoring, suggests that ATLS training alone may not be enough to maintain a trauma readiness posture at these facilities. This need for additional cognitive and technical support likely reflects the lack of experience and expertise of in-person providers, yet it also appears to be driven by a shortage of bedside staff. Our finding of a previously unreported use of TT, that 69% of the TT-EDs reported using teletrauma to document clinical care as way to free up staff for bedside clinical care, supports this view. Recent developments in ambient artificial intelligence (AI)-based medical transcription may alleviate the burden of medical documentation in the near future and should be considered as an adjunct in the provision of teletrauma care.49–51
Dynamics of hub-and-spoke relationships
Reimbursement for telehealth services is a key determinant of program sustainability. Most TT-EDs reported paying a fixed amount as part of a negotiated healthcare service delivery contract between the hub-and-spoke sites. This model encompasses flat-rate per consultation, irrespective of patient acuity and actual care delivered, with allowance for on-call pay and is considered distinct from traditional fee-for-service and value-based care models.52,53 This finding is novel but expected as flat-rate models simplify reimbursement, and are generally considered favorable for providers predominantly managing low-acuity cases, as is likely the case with teletrauma. 53 This model may also be influenced by private entities providing the majority of the remote care and utilizing nontraditional payment models versus hospital-based practices. A significant downside of using this model is the absence of incentives to pursue quality improvement initiatives and curtail costs of care. A significant proportion of TT-EDs reported being funded through a grant, which is understandable, given the pilot implementation of teletrauma in many instances. Only a few facilities reported receiving reimbursement from commercial and government insurers. Taken together these findings highlight that although individual hub-and-spoke sites see certain value in investing in a teletrauma service, most insurers currently lack a compelling value proposition to support reimbursement.
Despite the formal financial relationships, we found that resource sharing between hub-and-spoke sites to enhance trauma care was limited. Only 4% of TT-EDs reported receiving trauma care resources, such as blood products or medicines (e.g. prothrombin complex concentrate for anticoagulant reversal), and only 30% received formal trauma education from the hub site. Additionally, there was limited access to subspecialty services, such as neurosurgery, to offer remote expertise on management of specific injury patterns. Overall, the transactional nature of financial arrangements and limited resource sharing suggests that TT-EDs are yet to function as fully integrated extensions of the trauma system.
Alignment with goals set by the American College of Surgeons Committee on Trauma
In a recent white paper on teletrauma, the ACS COT described two main programmatic goals—to reduce potentially preventable early deaths, and to reduce potentially avoidable interfacility transfers. 33 Our findings suggest that while several telehealth-enabling capabilities exist at TT-EDs, such as established financial relationships to ensure sustainability, presence of telehealth equipment, and access to telehealth providers, there appears to be an overall lack of intentionality and specificity to deliver trauma care. This suggests a potential for misalignment with goals described by the ASC COT. For example, the lack of access to specialists via teletrauma can adversely affect efforts to reduce potentially avoidable interfacility transfers. Similarly, while 64% of TT-EDs reported using teletrauma for procedural support, only 30% reported receiving formal trauma care education to build requisite knowledge and skills to enable resuscitation of the critically injured patient. However, there exists an opportunity at the early stages of teletrauma development to undertake course correction. Clearly defining roles and responsibilities, standardizing workflows and care pathways, engaging the broader trauma care community, including trauma surgeons and subspecialists, and building knowledge and resource sharing capacities can all contribute positively towards mission realignment.
Limitations
We acknowledge potential limitations of this study. First, survey responses were self-reported with the potential for information bias. However, the survey was completed by ED leaders who likely had the correct information regarding operational aspects of teletrauma care delivery. Second, while the original NEDI-USA 2022 survey asked about teletrauma use, this was part of a broader survey that was not intentionally designed to investigate the specifics of teletrauma use. It is possible that the NEDI-USA 2022 survey misidentified teletrauma-using EDs who were subsequently invited to complete the NEDI Teletrauma Survey 2023. We acknowledge this limitation, however, given that the both surveys were completed by the ED directors, we believe that the NEDI-USA 2022 survey likely overcalled rather than undercalled this misidentification, that is, more false-positives than false-negatives were reported. To mitigate these false-positives, the opening question of the NEDI Teletrauma Survey 2023 specifically asked to confirm whether NEDI-USA 2022-identified EDs actually did use teletrauma in 2023 before proceeding to ask about additional details. Additionally, both NEDI-USA 2022 and NEDI Teletrauma Survey 2023 achieved high response rates (>80%) thus minimizing the effects of any residual misclassification. Third, while this survey was designed to understand specifics of ED teletrauma use, details of certain aspects of program structure and processes require further inquiry. For example, additional clarification is needed in topic areas such as reimbursement, program motivators, barrier/facilitators of using teletrauma, and elements to assess program performance. However, we intentionally designed the survey to balance the depth of content assessment with the feasibility of completion, which contributed to achieving a national response rate of 82%. Lastly, this survey was exclusively administered to the spoke sites. Although input from hub sites is important to gain a more comprehensive understanding, our initial focus was intentionally placed on end-users at each individual teletrauma-using ED. Insights obtained from this survey will help inform the design of future evaluations to include perspectives from hub sites.
Implications for rural trauma care, teletrauma research and policy
The study results have important implications for rural trauma care, teletrauma research and policy. They lay the foundation for future research aimed at understanding program motivators, barriers and facilitators as well as patient outcomes. This information is important to understand where and how teletrauma can be used to successfully enhance rural trauma care. Clinically, this study highlights persistent gaps in rural trauma care, illustrates how teletrauma is being used to, albeit incompletely, address some of these challenges and where opportunities exist to optimize rural trauma care. From a policy perspective, our findings highlight the need for establishing teletrauma standards, potentially modeled on trauma center standards and verification, to address variability and ensure alignment with goals described by the ACS COT for teletrauma programs.1,33
Conclusions
This nationwide study provides the first comprehensive evaluation of teletrauma program structures and processes in US EDs. Our study confirms that teletrauma is not being widely used. Even when capabilities exist, the actual use of teletrauma remains infrequent, lacks intentionality and specificity to fully address challenges of rural trauma care in line with programmatic goals described by the ACS COT.
Supplemental Material
sj-pdf-1-jtt-10.1177_1357633X261462011 - Supplemental material for National study to characterize teletrauma use in United States emergency departments
Supplemental material, sj-pdf-1-jtt-10.1177_1357633X261462011 for National study to characterize teletrauma use in United States emergency departments by Zain G Hashmi, Janice A Espinola, Ashley F Sullivan, Krislyn M Boggs, Maeve Swanton, Russell Griffin, Jan O Jansen, Jeffrey D Kerby and Carlos A Camargo Jr in Journal of Telemedicine and Telecare
Footnotes
Acknowledgements
The authors thank Anurag Pratap and Malavika Pillai (full-time paid employees) for their efforts contacting survey respondents; and to the NEDI-USA survey respondents.
Author contribution
Ethical consideration
This study was approved by the Mass General Brigham Human Research Committee (Protocol #: 2005P000015, 11/13/2023, exempt) and follows American Association for Public Opinion Research (AAPOR) guidelines.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by The Gillian Reny Stepping Strong Center for Trauma Innovation 2024 Innovator Award (co-principal investigators Dr. Hashmi and Dr. Camargo). Funders were not involved in the design or conduct of the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.